Easy bullet points on gastrulation and neurulation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here are easy bullet points on both topics, sourced from The Developing Human: Clinically Oriented Embryology:
Gastrulation
What it is: The process that converts the bilaminar disc (2 layers) into a trilaminar disc (3 layers) - the three germ layers.
When: Week 3 (the embryo is called a "gastrula" this week)
Key steps:
- The primitive streak appears first - a thickened band of epiblast cells at the caudal midline of the embryonic disc
- The primitive streak cranial end enlarges to form the primitive node
- Epiblast cells migrate inward (ingress) through the primitive streak - this process is called ingression
- Ingressing cells displace the hypoblast to form endoderm (the deepest layer)
- Other ingressing cells spread out between ectoderm and endoderm to form mesoderm (the middle layer)
- Cells remaining in the epiblast become ectoderm (the top layer)
- So all 3 germ layers arise from epiblast cells
The 3 germ layers and what they make:
- Ectoderm - skin, brain, spinal cord, peripheral nerves, eyes, inner ear, neural crest cells
- Mesoderm - muscles, bones, cartilage, blood vessels, kidneys, gonads, heart
- Endoderm - lining of gut, respiratory tract, liver, pancreas, thyroid
Key signals: FGFs, Wnt3a, Wnt5a, nodal (TGF-β family), Sonic hedgehog (Shh)
Fate of primitive streak: Regresses by end of week 4. If it persists, it can form a sacrococcygeal teratoma.
Neurulation
What it is: The formation of the neural tube - the precursor of the brain and spinal cord.
When: Weeks 3-4 (completed by end of week 4)
Key steps:
- The notochord forms from cells of the primitive node and induces the overlying ectoderm to thicken
- This thickening becomes the neural plate (neuroectoderm)
- Around day 18, the neural plate folds inward along its midline, creating a neural groove with neural folds on either side
- The neural folds are most prominent at the cranial end - these are the first signs of brain development
- The neural folds elevate, come together, and fuse - converting the groove into a closed neural tube
- Fusion starts in the middle and zippers both cranially and caudally
- The openings at each end are called neuropores:
- Anterior (cranial) neuropore closes ~day 25
- Posterior (caudal) neuropore closes ~day 27-28
- The neural tube then separates from the overlying surface ectoderm (which becomes skin)
Neural crest cells:
- As the neural folds fuse, cells at the junction break away = neural crest cells
- They undergo epithelial-to-mesenchymal transition and migrate widely
- Give rise to: dorsal root ganglia, autonomic ganglia, cranial nerve ganglia (V, VII, IX, X), Schwann cells, melanocytes, adrenal medulla, meninges (arachnoid + pia mater), facial bones
Clinical relevance - Neural Tube Defects (NTDs):
- Failure of neural tube closure = NTDs
- Anencephaly - failure of cranial neuropore to close (brain fails to develop)
- Spina bifida - failure of caudal neuropore to close
- Folic acid supplementation before/during pregnancy significantly reduces NTD risk
Easy memory trick:
- Gastrulation = "getting layers" (3 germ layers form)
- Neurulation = "neural tube" forms (brain + spinal cord precursor)
- The Developing Human: Clinically Oriented Embryology, pp. 188-210
What neural tube defects result from failed closure, and how does folic acid prevent them?
Finding Sources
Searching PubMed
folic acid neural tube defects prevention mechanism
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a thorough breakdown of NTDs and the folic acid story:
Neural Tube Defects (NTDs) from Failed Closure
NTDs are midline malformations involving neural tissue, meninges, and/or overlying bone. They are among the most common congenital CNS anomalies, occurring at ~1-10 per 1,000 live births worldwide (~3,500 births/year in the US). The specific defect depends on which neuropore fails to close and when.
Defects by Location
Cranial Neuropore Failure (anterior, ~day 25)
-
Anencephaly
- Most severe - the entire forebrain fails to develop
- Forebrain disruption at ~day 28 of gestation
- Brain is replaced by the area cerebrovasculosa - a disorganized remnant of neural tissue mixed with ependyma, choroid plexus, and meningothelial cells
- Calvarium (skull vault) is absent
- Posterior fossa structures may be partially spared depending on the extent of the defect
- Lethal - incompatible with life
- Associated with polyhydramnios (fetus cannot swallow properly)
-
Encephalocele
- Brain tissue herniates through a midline bony defect in the skull
- Most common at the occiput (back of skull)
- Nasofrontal variants (involving orbit, ethmoid, cribriform plate) also occur
- Severity varies from small meningeal sac to large brain herniation
Caudal Neuropore Failure (posterior, ~day 27-28)
These fall under the umbrella of spina bifida - a spectrum from trivial to severe:
| Type | What herniates | Neurologic deficit? |
|---|---|---|
| Spina bifida occulta | Nothing - just a bony defect in the vertebral arch | No (asymptomatic, found incidentally) |
| Meningocele | Meninges + CSF only (no cord tissue) | Usually none |
| Myelocele | Spinal cord exposed, flush with skin surface | Significant motor/sensory loss |
| Myelomeningocele | Spinal cord + meninges herniate through defect | Motor + sensory deficits below the level, bowel/bladder dysfunction |
- Myelomeningocele is the most clinically significant form
- Most common in the lumbosacral region
- Causes motor/sensory deficits in lower limbs, loss of bowel and bladder control
- Often complicated by infection (skin over the sac is thin and defective)
- Associated with Chiari II malformation (cerebellar herniation through foramen magnum) and hydrocephalus
- Risk of recurrence in subsequent pregnancies: ~4-5%
MRI of myelocele (A) vs. myelomeningocele (B):
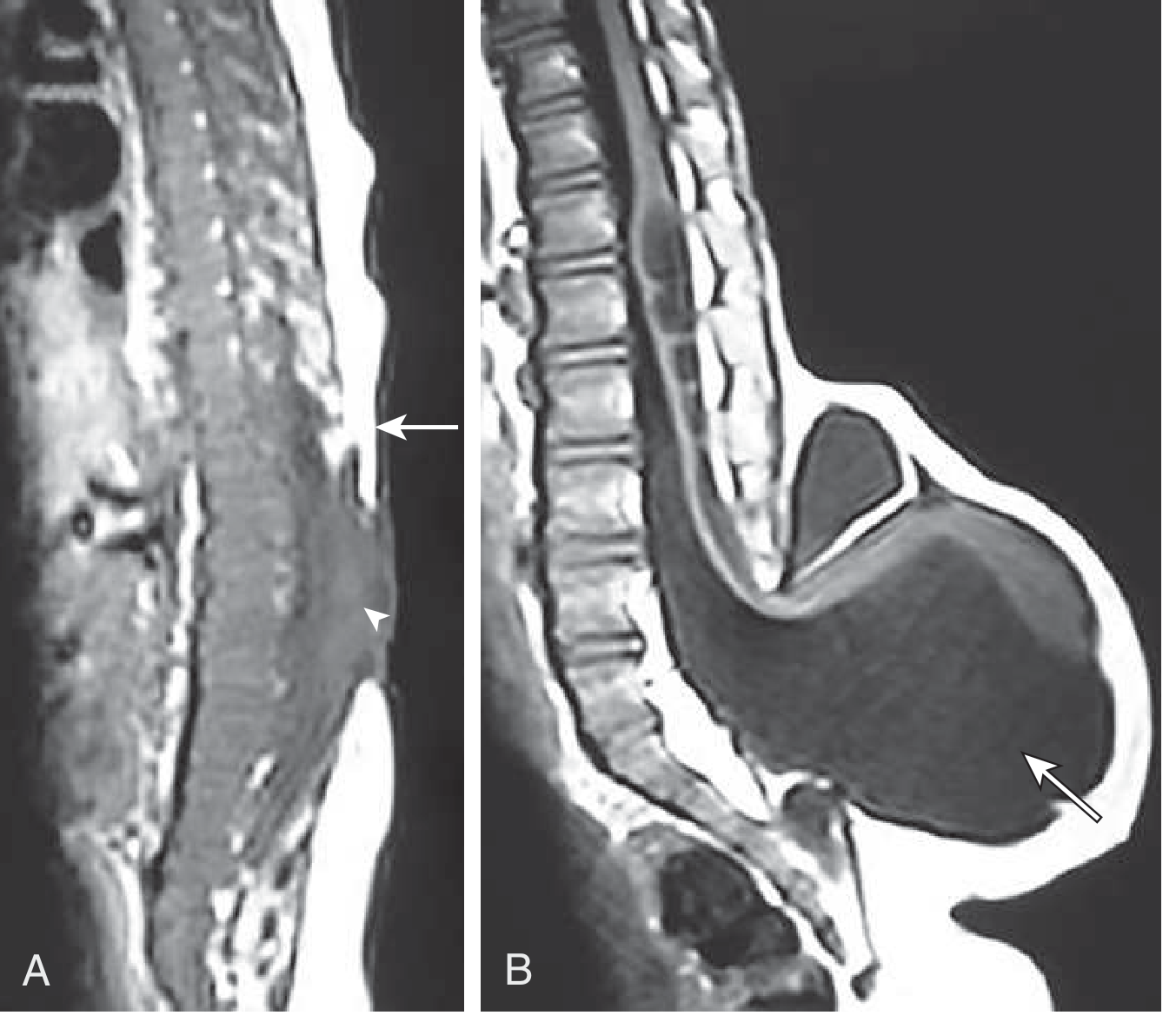
In myelocele (A), neural tissue (arrowhead) is flush with the skin surface. In myelomeningocele (B), the sac containing nerve tissue and CSF bulges well beyond the skin surface (arrow). - Goldman-Cecil Medicine
Risk Factors for NTDs
- Folate deficiency (most important modifiable factor)
- Teratogenic drugs - especially valproic acid (anticonvulsant) and carbamazepine
- Chromosomal anomalies
- Maternal diabetes
- Hyperthermia in early pregnancy
- Genetic polymorphisms in folate metabolism enzymes (see below)
How Folic Acid Prevents NTDs
The biochemical mechanism
Folic acid (vitamin B9) is central to one-carbon metabolism - the transfer of single carbon units needed for:
-
DNA synthesis - folate (as 5,10-methyleneTHF) is required to convert dUMP to dTMP (thymidylate synthesis). Without enough thymidine, rapidly dividing cells cannot replicate DNA properly. Neurulation is a period of intense cell proliferation - any impairment causes failure of neural fold fusion.
-
DNA methylation - folate (as 5-methylTHF) donates a methyl group to homocysteine via methionine synthase, regenerating methionine. Methionine is then converted to SAM (S-adenosylmethionine), the universal methyl donor for CpG island methylation. Impaired methylation disrupts epigenetic gene regulation during neural tube closure.
-
Homocysteine metabolism - folate deficiency impairs the enzyme methylenetetrahydrofolate reductase (MTHFR), which converts 5,10-methyleneTHF to 5-methylTHF. This causes homocysteine to accumulate. Elevated homocysteine is independently toxic to developing cells.
- A common genetic polymorphism in MTHFR (affecting 5-10% of the population) reduces enzyme efficiency. These individuals are at higher NTD risk but are partially protected by higher folate intake.
Why timing matters
- Neural tube closure is complete by day 28 of embryonic development
- Most women do not know they are pregnant until after week 4-6
- This means supplementation must begin before conception to be effective for neurulation
Dosing and efficacy
- 400 mcg/day begun before conception significantly reduces NTD incidence - Harper's Illustrated Biochemistry
- Folate supplementation (doses up to 6 mg/day used in high-risk cases) reduces NTD risk by approximately 50-60% - Goldman-Cecil Medicine
- Because of this, mandatory flour fortification with folic acid has been implemented in many countries (including the US since 1998), which has reduced NTD rates substantially
- The incidence of myelomeningocele in the US has fallen from ~1/1,000 to ~0.6/1,000 births, partly attributed to folate fortification and periconceptional supplementation
Important caveat about folic acid supplementation
- High-dose folic acid can mask vitamin B12 deficiency (corrects megaloblastic anemia but not the irreversible neurologic damage), which is why some countries have been cautious about mandatory fortification
- There is also some concern about folic acid supplementation increasing transformation of preneoplastic colorectal polyps into cancers - a consideration at population level
Summary table:
| NTD | Neuropore | Severity | Key features |
|---|---|---|---|
| Anencephaly | Cranial | Lethal | No brain/skull vault |
| Encephalocele | Cranial | Variable | Brain herniates through skull |
| Spina bifida occulta | Caudal | Asymptomatic | Bony defect only |
| Meningocele | Caudal | Mild | Meninges + CSF herniation |
| Myelomeningocele | Caudal | Severe | Cord herniates, motor/sensory/bowel/bladder loss |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1150; Goldman-Cecil Medicine, p. 4043; Harper's Illustrated Biochemistry, p. 558; The Developing Human: Clinically Oriented Embryology, p. 211
A recent umbrella review (PMID 39074459) confirms preconception folic acid and multivitamin supplementation meaningfully reduces NTD incidence, consistent with the textbook data above.
Fate of notochord
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
All the key content is in. Here's a clean summary:
Fate of the Notochord
What the notochord is
- A transient midline cellular rod formed in week 3 from cells migrating cranially from the primitive node
- It extends from the oropharyngeal membrane to the primitive node, defining the craniocaudal axis of the embryo
- It is not a permanent structure - its main job is to act as a signaling center during development
Functions while present
- Defines the longitudinal axis of the embryo and gives it rigidity
- Induces the overlying ectoderm to thicken and form the neural plate (primary inductor of CNS development)
- Provides signals for axial musculoskeletal patterning (via Sonic hedgehog/Shh signaling from the notochord and floor plate)
What happens to it
As the vertebral column develops around the notochord:
- Within vertebral bodies: The notochord is compressed and squeezed out - it degenerates and completely disappears where it is surrounded by the developing vertebral body
- Between vertebral bodies: The notochord persists and expands to form the nucleus pulposus - the gelatinous, water-rich center of each intervertebral disc
So the final adult remnant of the notochord = nucleus pulposus of every intervertebral disc.
Structure of the intervertebral disc (adult remnant)
| Part | Origin | Composition |
|---|---|---|
| Nucleus pulposus | Notochord remnant | Gelatinous matrix with scattered notochordal cells, high proteoglycan + water content |
| Annulus fibrosus | Mesoderm (sclerotome) | Concentric layers of fibrocartilage surrounding the nucleus |
- The nucleus pulposus has a high concentration of proteoglycans (mainly aggrecan), which attract water and give it its shock-absorbing properties
- In young people, notochordal cells are still identifiable in the nucleus pulposus; they are gradually replaced by chondrocyte-like cells with age
Clinical relevance - what goes wrong
1. Disc herniation ("slipped disc")
- With age or injury, the annulus fibrosus tears
- The nucleus pulposus herniates (bulges) posterolaterally, compressing nerve roots
- Most common at L4/L5 and L5/S1
2. Chordoma
- A rare, slow-growing malignant tumor arising from vestigial notochordal remnants that failed to fully degenerate
- ~1/3 occur at the base of the cranium (clivus), extending to the nasopharynx
- ~1/3 occur in the lumbosacral/sacrococcygeal region (the other end of the notochord's original extent)
- Infiltrates bone, difficult to fully resect surgically, but resection provides long-term disease-free survival in many cases
Easy memory summary
Notochord forms (week 3)
↓
Induces neural plate → CNS develops
↓
Vertebrae form around it
↓
Notochord squeezed within vertebrae → degenerates
Notochord between vertebrae → expands → NUCLEUS PULPOSUS
↓
Any leftover notochordal cells → potential CHORDOMA
Sources: The Developing Human: Clinically Oriented Embryology, pp. 202-203, 918; Junqueira's Basic Histology, 17e; Miller's Review of Orthopaedics, 9th Ed
This is a shared conversation. Sign in to Orris to start your own chat.