Differentiate between macular edema and central serous retinopathy
Macular Edema vs. Central Serous Retinopathy (CSCR)
1. Definition and Pathogenesis
| Feature | Macular Edema (ME) | Central Serous Chorioretinopathy (CSCR) |
|---|---|---|
| Core mechanism | Breakdown of the inner or outer blood-retinal barrier (BRB) causing fluid to accumulate within the retinal layers (intraretinal) | Focal dysfunction of the RPE allows fluid from the hyperpermeable choriocapillaris to leak beneath the neurosensory retina (subretinal) |
| Fluid location | Intraretinal (enlarges cystic spaces between retinal layers) | Subretinal space (between neurosensory retina and RPE) |
| Layer primarily affected | Muller cells and retinal capillary endothelium | Retinal pigment epithelium (RPE) and choriocapillaris |
| Classification | A symptom/finding with many underlying causes (diabetic, venous occlusion, post-surgical, uveitic, etc.) | An idiopathic disease entity; part of the "pachychoroid" disease spectrum |
2. Epidemiology and Risk Factors
| Feature | Macular Edema | CSCR |
|---|---|---|
| Typical patient | Variable - any age depending on cause | Young to middle-aged White male (M:F = 3:1) |
| Key associations | Diabetes mellitus (most common), retinal vein occlusion (CRVO/BRVO), post-cataract surgery (Irvine-Gass syndrome), uveitis, retinitis pigmentosa, epiretinal membrane, topical prostaglandins/epinephrine | Corticosteroid use (any route including intranasal/topical), psychological stress, Type A personality, Helicobacter pylori, systemic hypertension, pregnancy, Cushing syndrome, sleep apnea, renal dialysis |
| Laterality | Often bilateral (e.g., diabetic) or unilateral (vein occlusion) | Typically unilateral; bilateral in ~30% (often subclinical in fellow eye) |
| Steroid relationship | Steroids are a treatment (intravitreal dexamethasone, fluocinolone) | Steroids are a major precipitant - must be discontinued |
3. Clinical Features and Symptoms
| Symptom/Sign | Macular Edema | CSCR |
|---|---|---|
| Vision loss | Blurred, often gradual (depending on cause) | Blurred, acute to subacute onset |
| Metamorphopsia | Present | Prominent |
| Micropsia | Rare | Characteristic - fluid dome elevates retina causing minification |
| Dyschromatopsia | Rare | Mild color desaturation |
| Acquired hyperopia | Absent | Present - low-power convex lens may improve VA (retinal elevation) |
| VA range | Variable; can be severe | Typically 6/9 to 6/18 (20/30 to 20/60); rarely below 20/200 |
| Fundus exam | Loss of foveal reflex, retinal thickening, cystic spaces; may see hard exudates, hemorrhages, or disc swelling depending on cause | Round or oval dome-shaped elevation at macula; clear or slightly turbid subretinal fluid; no hard exudates; no hemorrhage |
| Hard exudates | Present (especially diabetic ME) | Absent |
| Hemorrhage | May be present (especially vein occlusion) | Absent |
4. Imaging - The Key Differentiator
OCT (Optical Coherence Tomography)
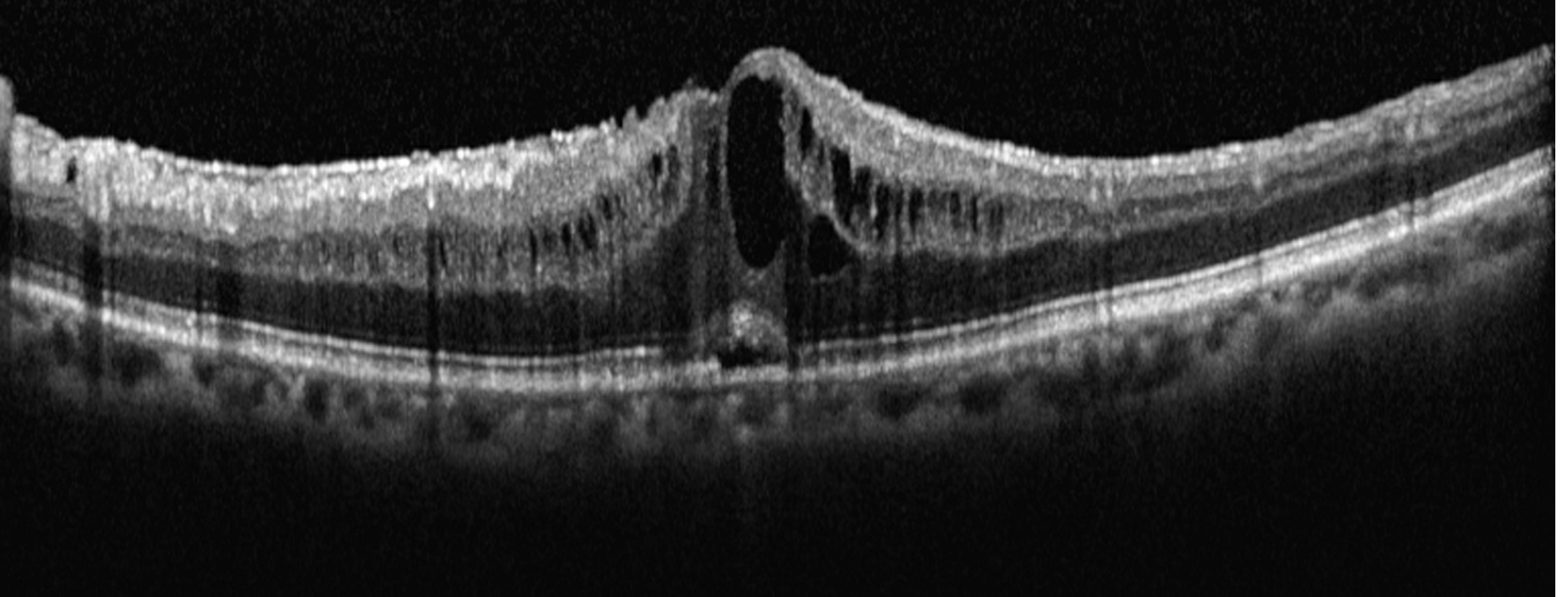
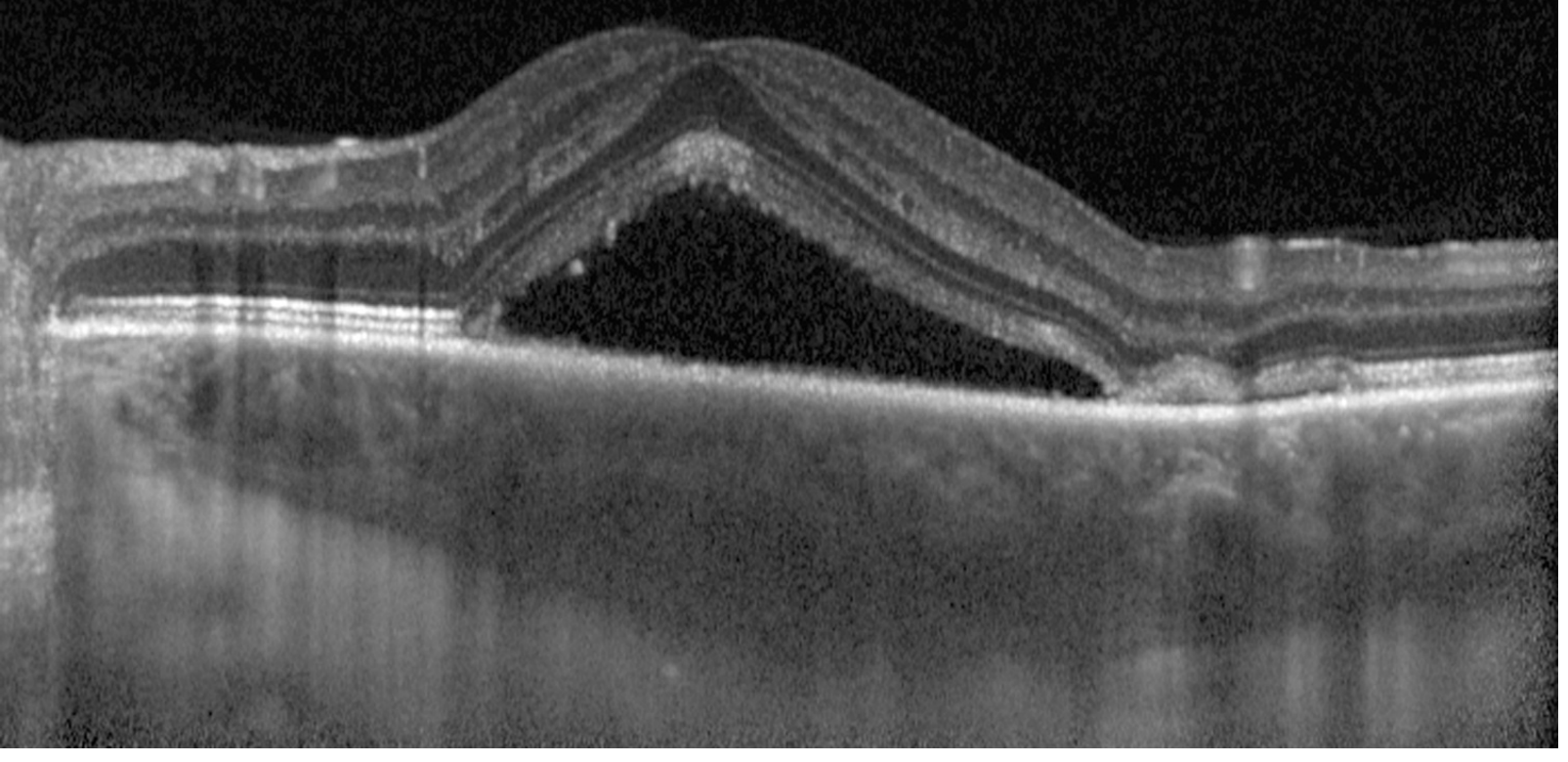
| OCT Finding | Macular Edema | CSCR |
|---|---|---|
| Fluid location | Intraretinal (within retinal layers as cystic spaces) | Subretinal (between retina and RPE) |
| Retinal layers | Disrupted, thickened | Intact, simply elevated |
| Foveal contour | Lost - replaced by cysts | Preserved but elevated |
| Choroid | Normal thickness | Thickened (pachychoroid) |
| RPE | Intact (or disrupted in severe diabetic) | Small PED (pigment epithelial detachment) often present at leak point |
| Hard exudate | May be visible | Absent |
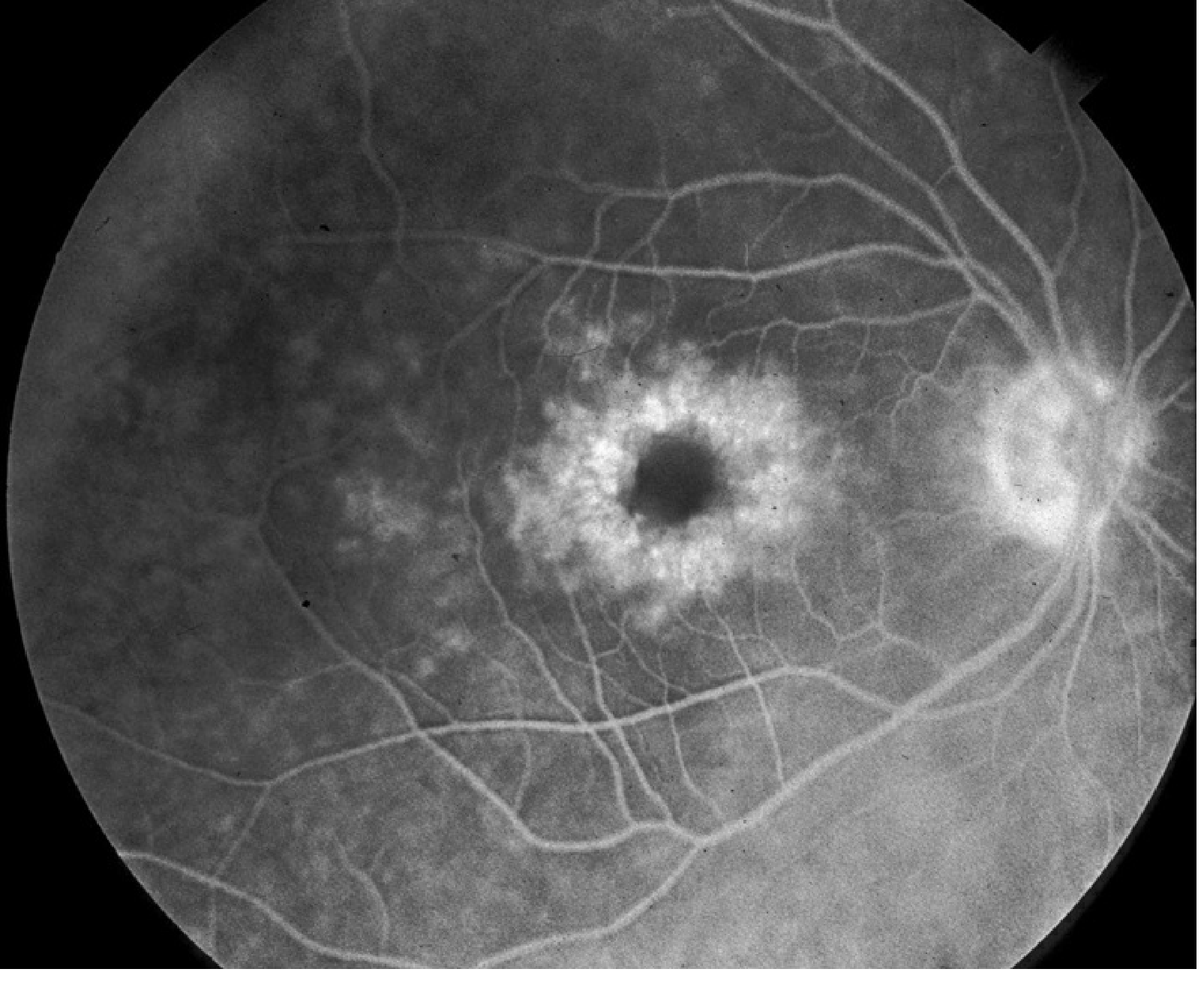
Fluorescein Angiography (IVFA)
| IVFA Finding | Macular Edema | CSCR |
|---|---|---|
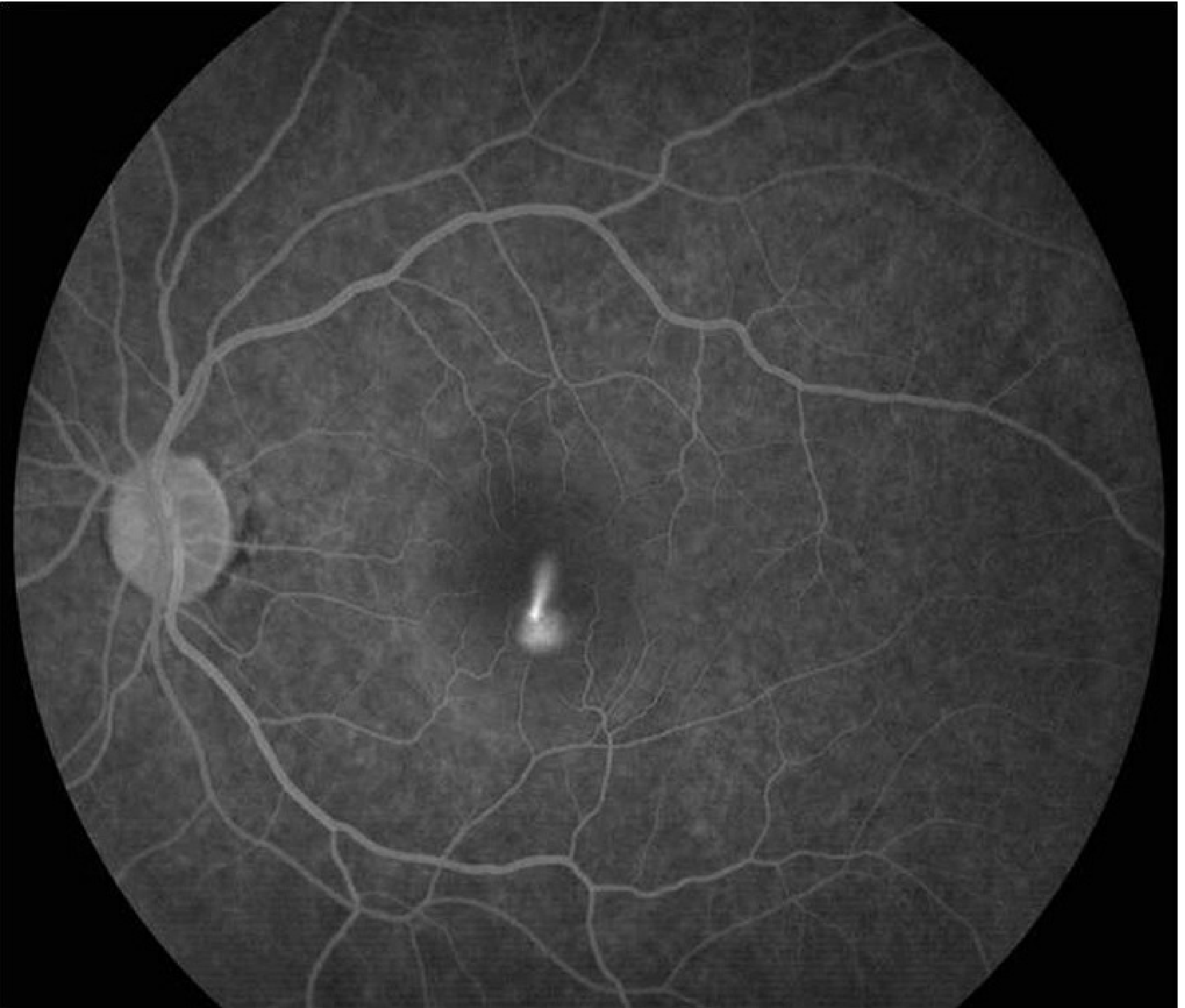
| Early phase | Perifoveal capillary leakage | Pinpoint hyperfluorescent RPE leak |
| Late phase | "Petaloid" or spoke-wheel pattern of pooling | "Smoke-stack" (10-20%) or "ink-blot" expansion |
| Site of leak | Perifoveal capillaries / capillary bed | RPE (single or few pinpoint sites) |
| Optic disc leakage | Possible (Irvine-Gass) | Not a feature |
ICGA (Indocyanine Green Angiography)
- ME: Not the primary test; used for underlying choroidal neovascularization
- CSCR: Shows choroidal artery and choriocapillaris filling delays, and characteristic multifocal hyperfluorescent patches in early phase - reflects underlying pachychoroid pathology
5. Course and Prognosis
| Feature | Macular Edema | CSCR |
|---|---|---|
| Natural course | Chronic without treatment; vision progressively worsens | Acute form: self-resolving in 3-6 months in ~80% |
| Chronicity | Persistent unless underlying cause treated | ~15% develop chronic CSCR (>12 months); recurrence in up to 50% |
| Visual prognosis | Depends entirely on underlying etiology and treatment response | Generally good for acute; chronic disease causes permanent photoreceptor/RPE degeneration and lasting vision loss |
| Complications | Photoreceptor damage, macular atrophy, lipid exudation | RPE atrophy, secondary CNV, bullous CSCR |
6. Treatment
| Treatment | Macular Edema | CSCR |
|---|---|---|
| First-line | Anti-VEGF (ranibizumab, aflibercept, bevacizumab) for diabetic ME and vein occlusion | Observation for acute CSCR (most resolve spontaneously) |
| Steroids | Intravitreal dexamethasone implant or fluocinolone acetonide (for refractory/steroid-responders) | Contraindicated - steroids precipitate and worsen CSCR; must be discontinued |
| Anti-VEGF | Mainstay for most secondary causes | Reserved for secondary CNV complication only |
| Laser | Focal/grid macular laser for extrafoveal microaneurysms (diabetic); avoided near fovea | Low-intensity laser photocoagulation to extrafoveal RPE leak point (accelerates recovery but long-term benefit uncertain; CNV risk) |
| Photodynamic therapy (PDT) | Not standard | Half-dose verteporfin PDT for chronic CSCR - can achieve rapid subretinal fluid resolution |
| Mineralocorticoid antagonists | Not used | Eplerenone or spironolactone - associated with improved anatomic and visual outcomes in chronic CSCR |
| Topical NSAIDs | Ketorolac, bromfenac, nepafenac (especially postoperative CME) | Not effective |
| Treat underlying cause | Optimize glycemic control, treat uveitis, stop offending drops | Stop corticosteroids (any formulation), address Cushing workup if needed |
7. Summary Comparison Table
| Parameter | Macular Edema (CME) | CSCR |
|---|---|---|
| Pathogenesis | BRB breakdown - intraretinal fluid accumulation | RPE dysfunction - subretinal fluid from choriocapillaris |
| Fluid location on OCT | Intraretinal cysts | Subretinal space (clean dome) |
| Typical patient | Diabetic, post-surgery, any age | Young-middle aged male, stressed/steroid-exposed |
| Hard exudates | Present | Absent |
| IVFA pattern | Petaloid / spoke-wheel | Smoke-stack or ink-blot |
| Choroidal thickness | Normal | Increased (pachychoroid) |
| Steroids | Used as treatment | Contraindicated (cause/worsen) |
| Primary treatment | Anti-VEGF, intravitreal steroids, NSAIDs | Observation, stop steroids, PDT (chronic), mineralocorticoid antagonists |
| Spontaneous resolution | No | Yes (acute form, ~80%) |
| Recurrence | Depends on underlying disease control | Up to 50% |
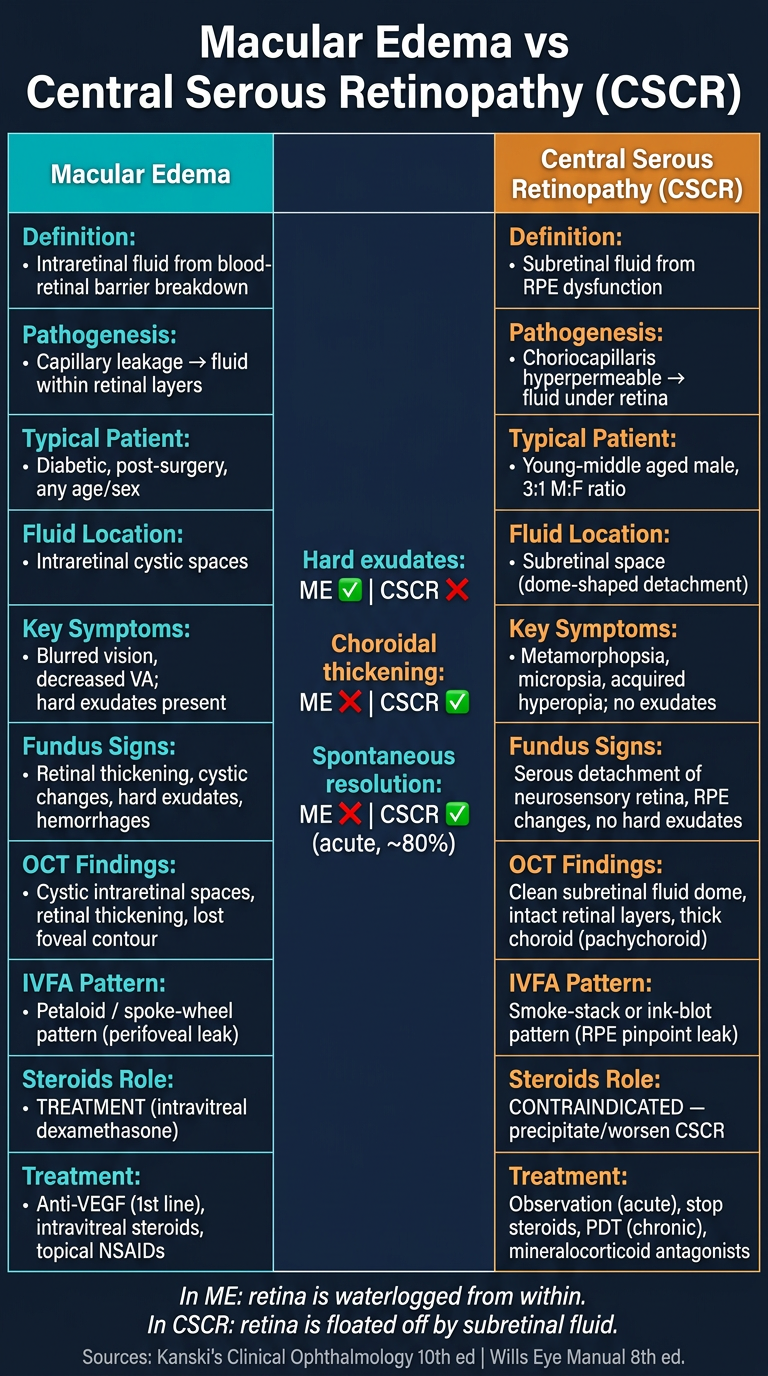
Make a poster from this
Medical education poster titled "Macular Edema vs Central Serous Retinopathy (CSCR)" with a clean clinical layout on a dark navy blue background. Two columns side by side comparing both conditions across these categories: Definition, Pathogenesis, Typical Patient, Fluid Location, Key Symptoms, Fundus Signs, OCT Findings, IVFA Pattern, Steroids Role, and Treatment. Left column (Macular Edema) in teal/cyan accent color: - Definition: Intraretinal fluid from blood-retinal barrier breakdown - Pathogenesis: Capillary leakage → fluid within retinal layers - Typical Patient: Diabetic, post-surgery, any age/sex - Fluid Location: Intraretinal cystic spaces - Key Symptoms: Blurred vision, decreased VA; hard exudates present - OCT: Cystic intraretinal spaces, retinal thickening, lost foveal contour - IVFA: Petaloid / spoke-wheel pattern (perifoveal leak) - Steroids: TREATMENT (intravitreal dexamethasone) - Treatment: Anti-VEGF (1st line), intravitreal steroids, topical NSAIDs Right column (CSCR) in orange/amber accent color: - Definition: Subretinal fluid from RPE dysfunction - Pathogenesis: Choriocapillaris hyperpermeable → fluid under retina - Typical Patient: Young-middle aged male, 3:1 M:F ratio - Fluid Location: Subretinal space (dome-shaped detachment) - Key Symptoms: Metamorphopsia, micropsia, acquired hyperopia; no exudates - OCT: Clean subretinal fluid dome, intact retinal layers, thick choroid (pachychoroid) - IVFA: Smoke-stack or ink-blot pattern (RPE pinpoint leak) - Steroids: CONTRAINDICATED — precipitate/worsen CSCR - Treatment: Observation (acute), stop steroids, PDT (chronic), mineralocorticoid antagonists Center dividing section with key differentiators highlighted: "Hard exudates: ME ✓ | CSCR ✗" "Choroidal thickening: ME ✗ | CSCR ✓" "Spontaneous resolution: ME ✗ | CSCR ✓ (acute, ~80%)" Bottom footer with memory hook in italic: "In ME: retina is waterlogged from within. In CSCR: retina is floated off by subretinal fluid." Sources: Kanski's Clinical Ophthalmology 10th ed | Wills Eye Manual 8th ed. Professional medical poster style, clear white text, well-organized table layout, readable fonts.