AUSCULTATION: lung with diagram
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching the Web
lung auscultation sites diagram anterior posterior stethoscope placement
Loading Image
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile everything.
Lung Auscultation
Technique
Listen at both apices and over upper and lower lobes, anteriorly and posteriorly, during both inspiration and expiration. Use the diaphragm of the stethoscope for higher-pitched sounds and the bell for lower-pitched sounds. Apply the stethoscope directly to skin (not through clothing) in a quiet room. Work from top to bottom, comparing sides symmetrically.
- Start at the apices (above the clavicles)
- Move systematically down: upper lobes, middle lobe/lingula, lower lobes
- Repeat on the posterior chest, starting at T3 level
Surface Projections of Lung Lobes (Auscultation Anatomy)
This is the key diagram for understanding where to place the stethoscope:
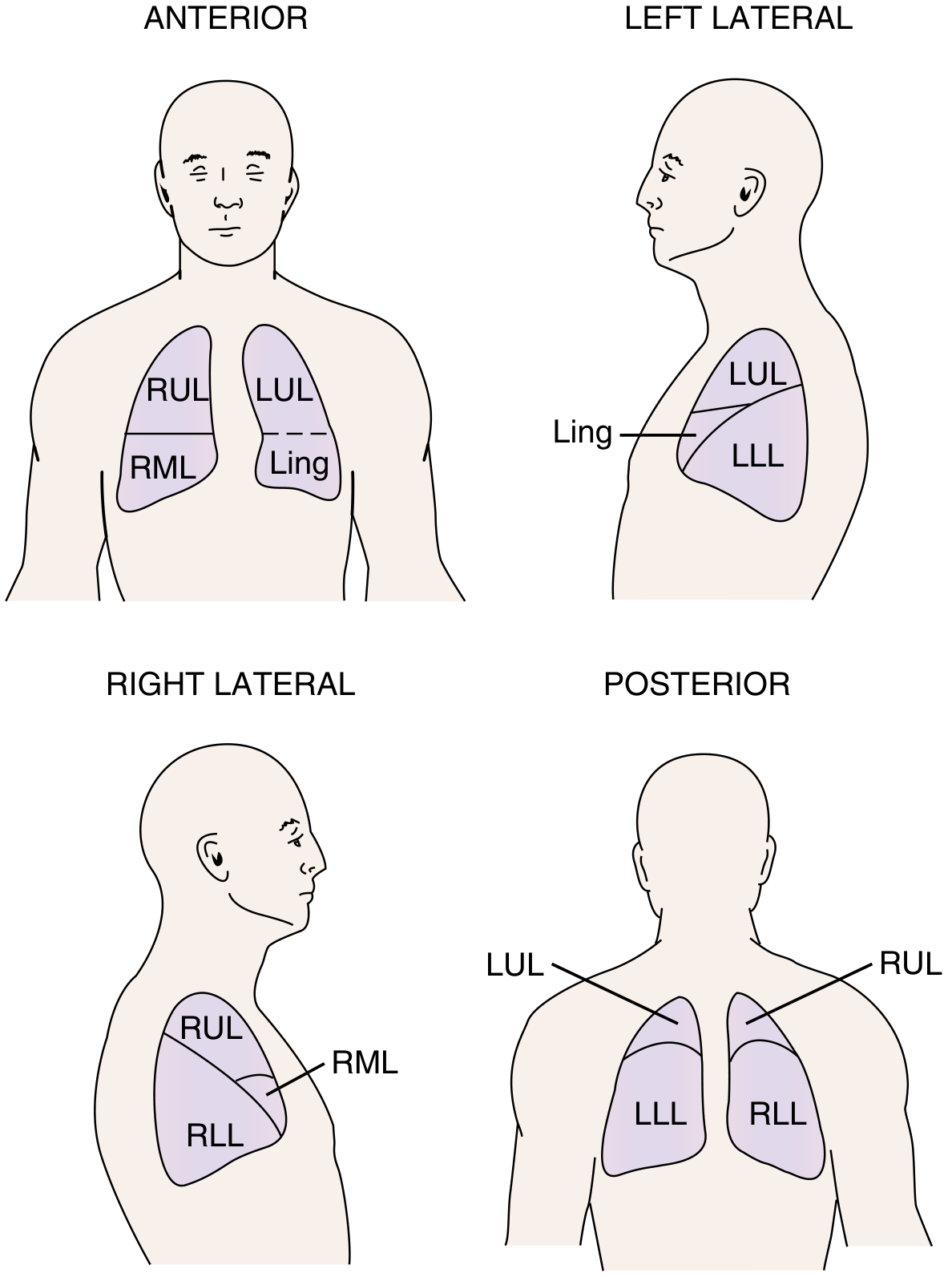
Figure 18.2 - Murray & Nadel's Textbook of Respiratory Medicine
Key anatomical landmarks:
- The oblique fissures (both lungs) run from the spinous process of T3 posteriorly to the 6th rib at the midclavicular line anteriorly
- The horizontal fissure (right lung only) lies at the 4th costal cartilage anteriorly, separating RUL from RML
- Posteriorly, nearly all of the visible lung surface is lower lobe - so posterior auscultation is mostly sampling the lower lobes
- Anteriorly, the upper and middle lobes predominate
Abbreviations: RUL = right upper lobe, RML = right middle lobe, RLL = right lower lobe, LUL = left upper lobe, Ling = lingula (left upper lobe), LLL = left lower lobe
Classification of Lung Sounds
(Based on ATS/Murray & Nadel's standardized nomenclature)
| Lung Sound | Acoustic Characteristics | Significance |
|---|---|---|
| Normal breath sounds | 200-600 Hz; soft, non-musical; louder on inspiration | Normal; arise from turbulent airflow in lobar/segmental bronchi |
| Tracheal breath sounds | 75-1600 Hz; hollow sound heard in both phases just below sternal notch | Normal over trachea |
| Bronchial breath sounds | Same as tracheal but heard in lung periphery; equal on inspiration & expiration | Consolidation, atelectasis - indicates airless air spaces around patent airway |
| Fine crackles | Discontinuous, soft, high-pitched, short; mid-to-late inspiratory | Opening of collapsed distal airways - fibrosis, atelectasis, heart failure, ILD |
| Coarse crackles | Discontinuous, loud, low-pitched; early inspiratory or expiratory; may clear with cough | Distal airway secretions - bronchitis, COPD |
| Wheezes | Continuous >250 ms; high-pitched (≥400 Hz); hissing quality; mainly expiratory | Airway narrowing - asthma/COPD (diffuse), focal lesion (if unilateral) |
| Rhonchi | Continuous >250 ms; low-pitched (<200 Hz); snoring quality; mainly expiratory | Large airway secretions - bronchitis, COPD; often clears with cough |
| Stridor | Continuous, high-pitched; mainly inspiratory; heard best over neck | Extrathoracic obstruction - anaphylaxis, epiglottitis, foreign body. Needs urgent attention |
| Pleural friction rub | Coarse, grating, creaking sound; heard in both phases | Pleural inflammation - pleuritis |
Important: The old term "rales" is no longer used - replaced by "crackles." The term "vesicular" is also inaccurate (normal breath sounds do not arise from alveoli).
Diagnostic Utility - Auscultatory Finding to Clinical Diagnosis
| Auscultatory Finding | Clinical Correlation |
|---|---|
| Bronchial breathing | Pneumonia, interstitial lung disease |
| Fine crackles | Heart failure, ILD, alveolar filling disorders |
| Coarse crackles | Bronchitis |
| Wheeze | Asthma, COPD, bronchomalacia |
| Rhonchus | Bronchitis, COPD |
| Stridor | Upper airway obstruction (laryngeal/tracheal inflammation, mass, external compression) |
| Absent breath sounds | Pleural effusion, pneumothorax, complete atelectasis |
Classic Findings in Common Pulmonary Disorders
| Disorder | Inspection | Palpation | Percussion | Auscultation |
|---|---|---|---|---|
| Asthma (acute) | Hyperinflation; accessory muscle use | Impaired excursion; decreased fremitus | Hyperresonance; low diaphragm | Prolonged expiration; inspiratory + expiratory wheezes |
| Pneumothorax (complete) | Lag on affected side; increased hemithorax size | Absent fremitus | Hyperresonant / tympanitic | Absent breath sounds |
| Pleural effusion (large) | Lag on affected side | Decreased fremitus; trachea shifted away | Dullness or flatness | Absent breath sounds |
| Atelectasis (lobar) | Lag on affected side | Decreased fremitus; trachea shifted toward affected side | Dullness or flatness | Absent breath sounds |
| Consolidation (pneumonia) | Possible lag/splinting | Increased fremitus on affected side | Dullness | Bronchial breath sounds; bronchophony; pectoriloquy; crackles |
Voice-Generated Sounds (Vocal Resonance)
Associated with consolidation (increased transmission) or effusion/pneumothorax (decreased transmission):
- Bronchophony - spoken "99" sounds clear and loud over consolidated lung (normally muffled)
- Egophony (E-to-A change) - spoken "E" sounds like "A" (nasal, bleating quality) over consolidated lung above a pleural effusion
- Whispered pectoriloquy - whispered words are clearly audible over consolidated lung (normally inaudible)
Sources: Murray & Nadel's Textbook of Respiratory Medicine, Chapter 18 | Goldman-Cecil Medicine, Chapter 71 (Table 7-1)
This is a shared conversation. Sign in to Orris to start your own chat.