CSF analysis and lumber puncture procedure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-organized answer.
Lumbar Puncture (LP) and CSF Analysis
1. Overview
Lumbar puncture (LP) is a procedure in which a spinal needle is inserted into the lumbar subarachnoid space to obtain cerebrospinal fluid (CSF). It is one of the most informative investigations in neurology and emergency medicine.
2. Indications
Urgent / Emergent:
- Suspected bacterial, viral, fungal, or tuberculous meningitis/encephalitis
- Suspected subarachnoid hemorrhage (SAH) when CT head is negative
- CNS infection in immunocompromised patients
Non-urgent / Elective:
- Demyelinating disease (multiple sclerosis - oligoclonal bands)
- Idiopathic intracranial hypertension (pseudotumor cerebri)
- Unexplained neurological disorders: altered consciousness, polyneuropathy, seizures
- Meningeal carcinomatosis / lymphomatous meningitis
- Neurosyphilis or other chronic CNS infections
- Normal pressure hydrocephalus evaluation
- Therapeutic: intrathecal chemotherapy, antibiotics, contrast (myelography)
(Pfenninger & Fowler's Procedures for Primary Care, p. 1438)
3. Contraindications
Absolute:
- Local skin infection at the puncture site
- Suspected or confirmed raised intracranial pressure (papilledema, focal neurological signs, deteriorating consciousness) - get CT head first
- Supratentorial mass lesion with midline shift
Relative:
- Severe coagulopathy (platelet count <20,000/mm³; INR >1.4) - most experienced clinician, smallest gauge needle
- Anticoagulated patient (see guidance below)
- Unstable patient (hypotension, shock, unstable airway) - defer until stable
- Uncooperative adult patient
CT Scan First (Box 206-1 - Indications): Age ≥60, altered consciousness, history of CNS disease, immunocompromised state, new-onset seizure within 1 week, focal neurological signs (arm drift, facial palsy, gaze palsy, leg drift, visual field defect, abnormal language), inability to answer two questions or follow two commands.
Important: Absence of papilledema does NOT reliably exclude raised ICP - papilledema may be absent in up to 15% of adults and 50% of children with early raised ICP. Do NOT delay antibiotics while awaiting CT when meningitis is strongly suspected.
4. Anticoagulation Considerations
| Agent | Guidance |
|---|---|
| Aspirin / NSAIDs alone | Safe to proceed; not a contraindication |
| Aspirin + heparin/LMWH (concurrent) | Avoid combination - higher SEH risk |
| IV Heparin | Discontinue ≥4 hours before |
| LMWH | Withhold; timing varies by agent |
| Warfarin | Reverse to INR <1.5 if thrombosis risk is low |
| Clopidogrel / Ticlopidine | Discontinue 7-10 days prior (ASRA recommendation) |
| Tirofiban / Eptifibatide | Normal platelet activity returns ~8 hours after stopping |
| Abciximab | 24-48 hours after stopping |
The most feared anticoagulation-related complication is spinal epidural hematoma (SEH) - rare but catastrophic; requires urgent MRI and laminectomy if suspected.
(Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 3950-3957)
5. Equipment
- Spinal tray containing:
- Povidone-iodine swabs and alcohol swab
- Fenestrated drape and sterile gloves
- Manometer with three-way stopcock
- 1% lidocaine + 3 mL syringe with 20-23 gauge needle
- 20-22 gauge spinal needle (Quincke or Sprotte/atraumatic pencil-point)
- Four numbered, capped sterile test tubes
- Sterile dressing
- Optional: pulse oximetry, EMLA cream (apply 30-60 min before), 1 mL syringe for dry taps, ultrasound guidance in obese patients
(Pfenninger & Fowler's, p. 1438-1439)
6. Procedure - Step by Step
Positioning
Two positions are used:
Lateral decubitus (fetal position) - preferred for pressure measurement:
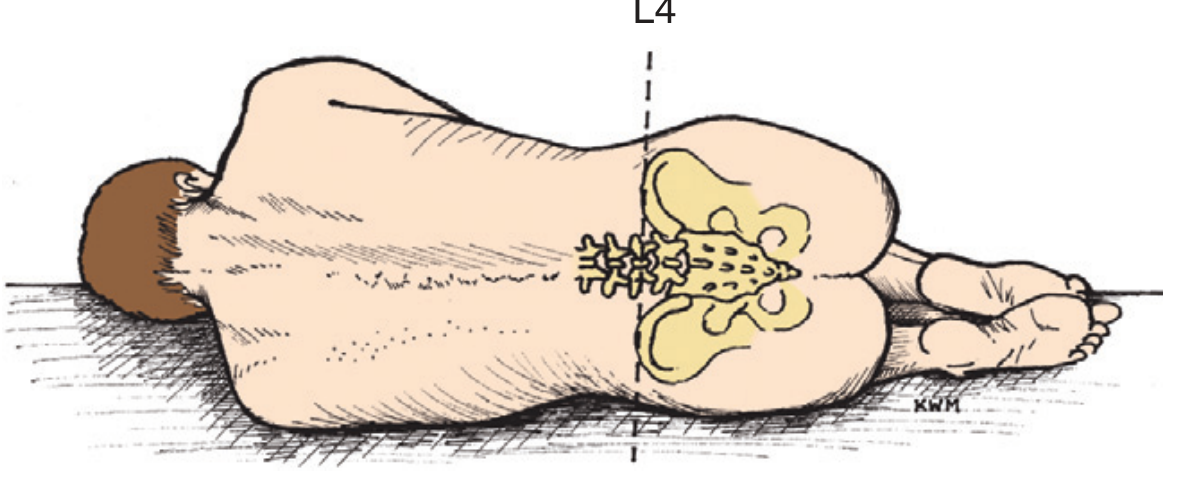
Patient lies on the side with knees drawn up to abdomen ("fetal position"), neck slightly flexed forward. Shoulders, back, and hips must be perpendicular to the bed - no forward or backward tilt.
Sitting upright position: More commonly used in adults; makes midline identification easier, especially in obese patients.
Anatomic Landmark
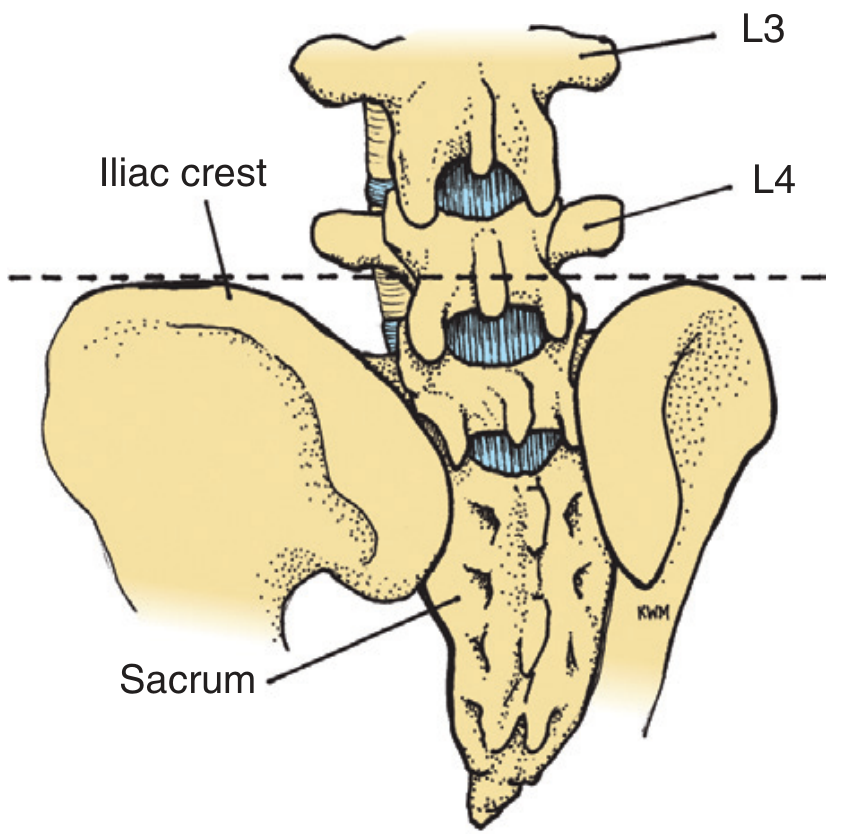
A horizontal line drawn between the superior aspects of both iliac crests intersects the body of L4. The L3-L4 interspace is the primary target; L2-L3 or L4-L5 may also be used. The spinal cord in adults ends at approximately L1-L2, so LP at L3-L4 or below safely enters the cauda equina region.
Step-by-Step Technique
- Consider CT head first in patients with focal neurological signs, altered mentation, immunocompromise, suspected SAH, or papilledema.
- Position the patient near the edge of the bed in lateral decubitus or sitting position. Identify the L3-L4 interspace using iliac crest landmarks.
- Prepare sterile field - open spinal tray, put on sterile gloves, pre-assemble manometer. Place numbered test tubes in order.
- Skin preparation - clean a ≥10 cm diameter area with povidone-iodine; apply fenestrated drape.
- Local anaesthesia - inject 3 mL of 1% lidocaine: raise a skin wheal in the midline at L3-L4, then infiltrate deeper into interspinous ligaments in the direction the spinal needle will travel. A field block can also be used.
- Insert the spinal needle - insert the 20-22 gauge needle through the skin in the midline, angled ~15 degrees cephalad toward the umbilicus, keeping the bevel parallel to the longitudinal axis of the spine (to split rather than cut dural fibres, reducing post-LP headache). Advance slowly.
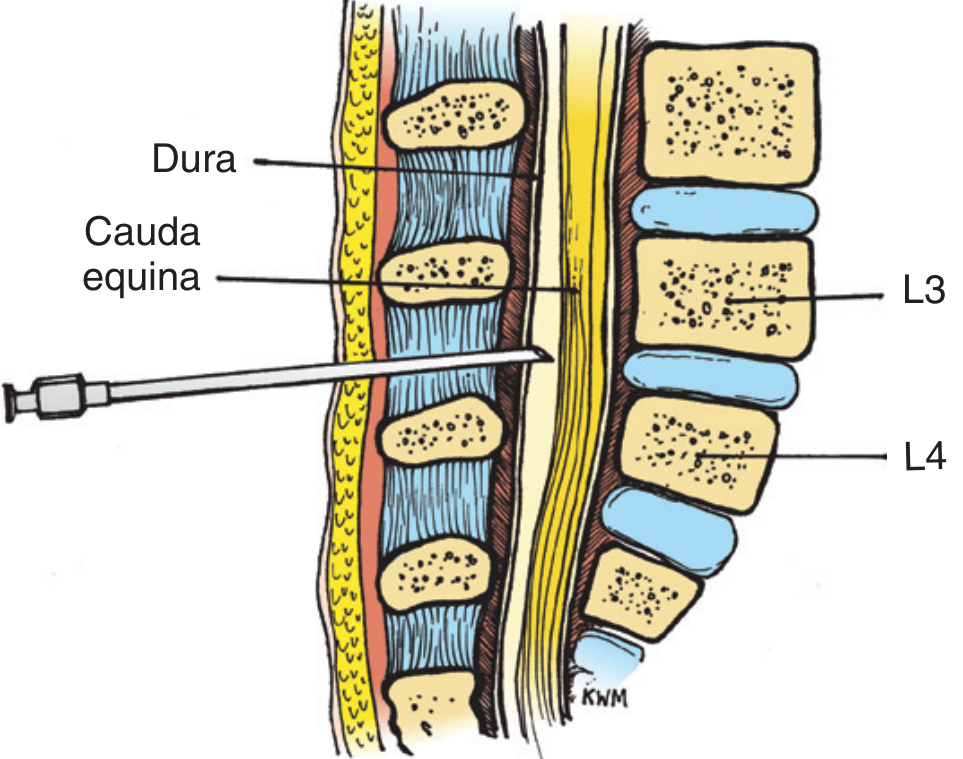
- Confirm position - a slight "pop" may be felt as the needle passes through the dura (may not be felt with Quincke needle). Withdraw the stylet every 3-4 mm and check for fluid at the hub. Rotate needle 90-180° if no fluid returns. If radicular pain (pain down one leg) occurs, the needle is too lateral - remove and reposition.
- Measure opening pressure - attach the three-way stopcock and manometer. Ask the patient to straighten their legs and relax. CSF will rise in the manometer. Note colour and pressure. CSF should oscillate slightly with respirations.
- Normal opening pressure: 50-170 mm H₂O in adults (70-180 mm H₂O by some references); 50-80 mm H₂O in infants and children
- Coughing, crying, shouting artificially elevates pressure
- Collect CSF - obtain 4 tubes (~1 mL each minimum; up to 8-40 mL total as needed). Standard tube assignment:
- Tube 1: Chemistry (protein, glucose)
- Tube 2: Gram stain and culture
- Tubes 3 & 4: Cell count + differential (compare tube 1 vs tube 4 for traumatic tap differentiation)
- Save a tube for additional tests (serology, PCR, cytology, India ink, etc.)
- Withdraw needle - replace stylet before removal. Apply sterile dressing. Advise the patient to lie flat for 1-2 hours to reduce post-LP headache risk.
(Pfenninger & Fowler's Procedures for Primary Care, p. 1438-1441; Tietz Textbook of Laboratory Medicine 7th Ed.; Tintinalli's Emergency Medicine)
7. CSF Analysis - Normal Values
| Parameter | Normal Value |
|---|---|
| Opening pressure | 50-170 mm H₂O (adults); 50-80 mm H₂O (children) |
| Appearance | Crystal clear and colourless |
| Xanthochromia | None |
| Red blood cells (RBCs) | ≤5/mm³ |
| White blood cells (WBCs) | ≤5/mm³; no PMNs (neutrophils) normally present |
| WBC (neonates) | Up to 22/mm³ (higher baseline) |
| Glucose | >40 mg/dL, or 60-70% of serum glucose |
| Protein | <50 mg/dL (higher in neonates) |
| Gram stain / Culture | Negative |
(Tintinalli's Emergency Medicine - Table 175-2; Pfenninger & Fowler's - Table 206-1)
8. CSF Findings in Disease States
| Condition | Opening Pressure | Appearance | WBCs (/mm³) | Cell Type | Glucose | Protein |
|---|---|---|---|---|---|---|
| Normal | 50-170 mm H₂O | Clear | ≤5 | Lymphocytes | Normal | <50 mg/dL |
| Bacterial meningitis | Elevated (>180) | Turbid/cloudy | 500-20,000 | Neutrophils | Low (<40 mg/dL) | High (100-700 mg/dL) |
| Viral (aseptic) meningitis | Normal/mildly elevated | Clear | 10-1,000 | Lymphocytes | Normal | Normal to mildly elevated |
| Tuberculous meningitis | Elevated | Cloudy/xanthochromic | 100-500 | Lymphocytes (early: PMNs) | Very low | High |
| Fungal meningitis (Cryptococcus) | Elevated | Clear to slightly turbid | Low (0-100) | Lymphocytes | Low | Elevated |
| Subarachnoid hemorrhage | Elevated | Bloody, then xanthochromic | Elevated (RBCs) | RBCs + RBC casts | Normal | Elevated |
| MS / Demyelinating disease | Normal | Clear | Normal or mildly elevated | Lymphocytes | Normal | Normal or mildly elevated; oligoclonal bands + |
| Guillain-Barre Syndrome | Normal | Clear | Normal | - | Normal | Elevated (albuminocytological dissociation) |
| Malignant/carcinomatous meningitis | Variable | Clear to xanthochromic | Elevated | Abnormal/malignant cells | Low | Elevated |
Key CSF Differentiators
Bacterial vs. Viral Meningitis:
- Bacterial: lower glucose, higher protein, higher WBC counts, neutrophilic predominance
- Viral: normal glucose, slightly elevated or normal protein, lymphocytic pleocytosis
- Early bacterial meningitis can occasionally show lymphocytes
Subarachnoid Hemorrhage vs. Traumatic Tap:
| Feature | SAH | Traumatic Tap |
|---|---|---|
| Blood in CSF | Present in all tubes equally | Clears from tube 1 to tube 4 |
| Xanthochromia | Present (develops 2-4 hrs after bleed) | Absent |
| Clotting | Does NOT clot | May clot |
| RBC count | High, uniform across tubes | Decreasing |
Xanthochromia (yellow or pink discoloration) after centrifugation is due to oxyhemoglobin and bilirubin from RBC breakdown - it indicates true hemorrhage, not traumatic tap. It persists for up to 2-3 weeks after SAH.
(Harrison's 22E; Frameworks for Internal Medicine; Goldman-Cecil Medicine)
9. Additional CSF Tests
- Gram stain - identifies bacteria in ~70-90% of bacterial meningitis; lower yield for Listeria (~30%)
- Culture - gold standard for bacterial/fungal/mycobacterial meningitis
- India ink preparation - for Cryptococcus neoformans
- Cryptococcal antigen - more sensitive than India ink
- VDRL - highly specific (but not sensitive) for neurosyphilis
- Oligoclonal bands - multiple sclerosis, CNS lupus
- PCR - HSV, CMV, EBV, JC virus, enterovirus, TB; particularly useful in partially treated meningitis
- 16S ribosomal RNA PCR - broad bacterial detection
- 18S/28S rRNA PCR - broad fungal detection
- Beta-glucan assay - adjunct for fungal infections
- Cytology + cell block - malignant meningitis; large volumes needed (40 mL); flow cytometry for lymphoma
- Metagenomic next-generation sequencing (mNGS) - unbiased pathogen identification in diagnostically challenging cases
(Harrison's Principles of Internal Medicine 22E, p. 1177)
10. Complications
| Complication | Details |
|---|---|
| Post-LP headache | Most common (3-36%); positional (worse upright, better supine); onset 24-48 hrs; due to CSF leak from dural puncture site; treat with caffeine, hydration, analgesics, or blood patch |
| Local discomfort | Expected; radicular pain (down one leg) indicates needle too lateral - reposition |
| Spinal epidural hematoma (SEH) | Rare but catastrophic; especially in anticoagulated patients or traumatic LP; presents with new severe back pain, radiculopathy, or sphincter disturbance after procedure; diagnose with urgent MRI spine; treat with emergency laminectomy |
| Infection / meningitis | Risk <0.01% with proper sterile technique |
| Herniation | Risk of cerebral herniation if LP done in setting of raised ICP with mass lesion - always check for contraindications first |
| Epidermoid tumour | Rare late complication if needle inserted without stylet - caused by implanted dermal cells |
To reduce post-LP headache risk:
- Use the smallest gauge needle available (22-25 gauge)
- Use an atraumatic (pencil-point) needle (Sprotte/Whitacre) rather than Quincke
- Orient the Quincke bevel parallel to longitudinal spine axis to split rather than cut dural fibres
- Replace stylet before removing the needle
(Tintinalli's Emergency Medicine; Pfenninger & Fowler's; Roberts & Hedges')
11. Special Considerations
- Paediatric patients: Higher baseline WBC and protein in neonates. Opening pressure <28 cm H₂O generally considered normal in children. Collect ~1 mL per tube.
- HIV/Immunocompromised: Normal CSF values may exist even with significant infection (especially cryptococcal meningitis). Always send India ink + cryptococcal antigen. CSF HIV PCR and antigen detection also available.
- Obese/Difficult anatomy: Ultrasound guidance to locate spinous processes; sitting position preferred; may need fluoroscopy after multiple failed attempts.
- Failed LP: Change patient position (lying to sitting or vice versa), try a different interspace, try lateral approach. A "dry tap" is usually due to poor patient positioning or misplaced needle rather than obliterated subarachnoid space.
Sources:
- Pfenninger & Fowler's Procedures for Primary Care, 3rd Ed., pp. 1438-1441
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, pp. 3950-3976
- Harrison's Principles of Internal Medicine, 22E (2025), p. 1177
- Tintinalli's Emergency Medicine: A Comprehensive Study, Table 175-2
- Tietz Textbook of Laboratory Medicine, 7th Ed., pp. 1628-1631
- Frameworks for Internal Medicine, pp. 992-1022
This is a shared conversation. Sign in to Orris to start your own chat.