So i will be asking a few doubts related to huaman body which includes anatomy, physiology and histology..... i just want you to give me right answers and give me simple explanation for the answers thats all like give me a simple way to remeber things.. coz i dont have time and my exams are coimg upp
N1. Which muscle from the following muscles is not extrinsic muscle of the tongue? Answer: Geniohyoid muscle
Why?
| Muscle | Action |
|---|---|
| Genioglossus | Protrudes tongue |
| Hyoglossus | Depresses tongue |
| Styloglossus | Retracts & elevates tongue |
| Palatoglossus | Elevates tongue back |
What is Geniohyoid then?
- It's a suprahyoid muscle (connects chin to hyoid bone)
- It elevates the hyoid and helps in swallowing
- It has nothing to do with moving the tongue directly
🧠 Memory Trick
"If it ends in -GLOSSUS, it moves the tongue"
what is extrinsic and intrinsic
Extrinsic Muscles
- Origin OUTSIDE the tongue, insertion INTO the tongue
- They move the tongue (side to side, in, out)
- Think: they come from somewhere else and pull the tongue around
Intrinsic Muscles
- Entirely WITHIN the tongue (both origin and insertion inside)
- They change the SHAPE of the tongue (make it flat, round, pointed)
- Think: they live inside and reshape it
🧠 One-line memory trick:
Extrinsic = Move it (they're outsiders pulling it) Intrinsic = Shape it (they're insiders molding it)
Quick Example:
- You stick your tongue out → Extrinsic (Genioglossus) doing the work
- You make your tongue pointed → Intrinsic muscles doing the work
N13 The mesentery is a double layer of peritoneum that supports which of thefollowing organs? Answer: Small intestine
What is the Mesentery?
- A double fold of peritoneum (like a fan-shaped sheet)
- It attaches the small intestine to the posterior abdominal wall
- It carries blood vessels, lymphatics, and nerves to the gut
Simple Picture in Your Head:
Imagine the small intestine is a kite and the mesentery is the string + frame holding it in place inside your belly.
Why not the other organs?
| Organ | Its Peritoneal Fold |
|---|---|
| Stomach | Greater & Lesser Omentum |
| Liver | Falciform ligament |
| Large intestine (most) | Retroperitoneal (no fold) |
| Small intestine | Mesentery ✅ |
🧠 Memory Trick:
"MESEN-tery = MESEN-teric = Small intestine"
Ascending colon under the liver bends to the left forming splenic flexure- false
The Two Mistakes:
| What the statement said | What is actually correct |
|---|---|
| "Ascending colon under the liver..." | ❌ It's the TRANSVERSE colon that passes under the liver |
| "...bends to form splenic flexure" | ❌ The bend under the liver is the HEPATIC flexure, not splenic |
The Correct Story of the Colon:
🧠 Memory Trick:
Hepatic flexure = under the Liver (both on the RIGHT) Splenic flexure = under the Spleen (both on the LEFT)
- Right side = Liver = Hepatic flexure
- Left side = Spleen = Splenic flexure
Question N23 A patient has adult-onset diabetes with glucosuria. The appearance of glucose in the urine is a consequence of which of the following processes in the proximal tubule? Answer: Saturation of the Na+-glucose cotransporter
The Normal Situation:
- Normally 100% of glucose is reabsorbed
- No glucose appears in urine
What Happens in Diabetes:
The Key Concept - Tm (Transport Maximum):
The cotransporter has a maximum capacity called Tm Normal Tm for glucose = ~180 mg/dL (renal threshold) In diabetes, blood glucose goes above 180 mg/dL → transporter is full → glucose escapes into urine
Simple Analogy:
Think of the cotransporter as a bucket. Normally it catches all the glucose. In diabetes, so much glucose is flooding in that the bucket overflows → glucosuria!
🧠 Memory Trick:
"180 = the magic number" Blood glucose above 180 mg/dL = transporter saturated = glucose in urine
Question N5 Which of the following is TRUE regarding gastric emptying? Answer: a. Decreased by CCK N24 Renin in the circulation originates from: Answer: Juxtaglomerular cells
N5 - Gastric Emptying Decreased by CCK ✅
What is CCK?
Why does CCK slow gastric emptying?
Duodenum says: "Hey! I already have fat/protein here, stop sending more from the stomach!" So CCK puts the brakes on the stomach
What CCK actually does:
- ⬇️ Slows gastric emptying
- Contracts gallbladder (releases bile)
- Stimulates pancreatic enzymes
- Increases satiety (feeling full)
🧠 Trick - Things that SLOW gastric emptying:
"Fat, Acid, CCK, and Stress slow the stomach"
- High fat meal
- Acidic contents in duodenum
- CCK
- Pain/stress
N24 - Renin from Juxtaglomerular (JG) Cells ✅
Where exactly?
What triggers renin release?
- ⬇️ Blood pressure
- ⬇️ Blood volume
- ⬇️ Na⁺ delivery to macula densa
- Sympathetic stimulation (β1)
What does renin do?
Renin → converts Angiotensinogen → Angiotensin I → (ACE) → Angiotensin II → raises BP
🧠 Memory Trick:
JG cells = the kidney's blood pressure sensor & alarm system Low pressure detected → JG cells release renin → BP goes back up
Question N6 The process of mastication is initiated by:
Mastication is initiated by: Relaxation of the jaw muscles (masseter)
How it works - The Chewing Reflex:
- Food placed in mouth → stretches the mouth/jaw muscles
- This reflexively inhibits the jaw closing muscles (masseter, temporalis)
- Jaw drops open (relaxation)
- Stretch receptors in jaw muscles then fire → jaw snaps back up
- This cycle repeats rhythmically = chewing!
It's a Reflex - not a conscious start:
The presence of food in the mouth automatically triggers the masticatory reflex It is controlled by rhythmic centers in the brainstem (You can also voluntarily chew - but the reflex initiates it)
Muscles of Mastication - Quick List:
| Muscle | Action |
|---|---|
| Masseter | Closes jaw (elevates mandible) |
| Temporalis | Closes + retracts jaw |
| Medial pterygoid | Closes jaw |
| Lateral pterygoid | Opens jaw (only one!) |
🧠 Memory Trick:
"3 close, 1 opens" - Three muscles close the jaw, only the Lateral pterygoid opens it"Lateral = Lowers the jaw"
Question N7 Which of the following physiological processes assists in clearing a large food bolus from the esophagus? Answer: D) Secondary peristalsis
Types of Peristalsis in the Esophagus:
| Type | Trigger | Purpose |
|---|---|---|
| Primary peristalsis | Voluntary swallowing | Moves food bolus from pharynx down to stomach |
| Secondary peristalsis | Distension/stretching of esophagus by remaining food | Clears leftover/stuck bolus |
| Tertiary peristalsis | Spontaneous, uncoordinated | Non-propulsive, abnormal (seen in elderly) |
Simple Story:
You swallow food → Primary peristalsis pushes it down But a large chunk gets stuck → esophagus wall gets stretched Stretching triggers Secondary peristalsis → extra wave pushes it down Think of it as the esophagus saying: "You're still here?! Let me push harder!"
Key Point:
- Secondary peristalsis does NOT need swallowing to be triggered
- It is triggered locally by esophageal distension
- This is also what clears refluxed acid back down from the esophagus
🧠 Memory Trick:
Primary = initiated by swallowing (voluntary) Secondary = initiated by stretch (automatic cleanup crew) Tertiary = uncoordinated, abnormal (trouble!)
Question N4 Parotid duct pass on the face horizontally, turns deeply and penetrates into --------------------- muscle Answer:
Answer: Buccinator muscle
The Path of the Parotid Duct (Stensen's Duct):
- Exits the parotid gland (in front of the ear)
- Runs horizontally across the face over the masseter muscle
- At the anterior border of masseter → turns sharply inward (medially)
- Pierces the Buccinator muscle
- Opens into the mouth at the upper 2nd molar (parotid papilla)
Simple Picture:
Parotid duct = a pipe running across your cheek It has to punch through the buccinator (your cheek muscle) to get inside your mouth
Key Landmarks:
| Structure | Relation |
|---|---|
| Masseter muscle | Duct runs over it |
| Buccinator muscle | Duct pierces through it |
| Upper 2nd molar tooth | Where duct opens in the mouth |
🧠 Memory Trick:
"Parotid duct Bucc-s its way into the mouth" (Bucc = Buccinator 😄)
Or remember: **"B"uccinator because saliva goes **"B"ack into the mouth through it
Bonus fact:
is the sodt palate behind hard palate
The Roof of Your Mouth - Front to Back:
FRONT (teeth)
↓
Hard Palate (bony, rigid - front 2/3)
↓
Soft Palate (muscular, flexible - back 1/3)
↓
Uvula (the dangly thing at the back)
↓
Throat (oropharynx)
Hard vs Soft Palate:
| Hard Palate | Soft Palate | |
|---|---|---|
| Position | Anterior (front) | Posterior (back) |
| Structure | Bone (palatine process of maxilla + palatine bone) | Muscle + mucosa (no bone) |
| Function | Rigid base for tongue to push food | Moves up to close off nasal cavity during swallowing |
Easy Way to Feel It:
Run your tongue along the roof of your mouth from front to back
- Hard part at front = hard palate
- Soft/fleshy part at back = soft palate
- Dangly bit = uvula
🧠 Memory Trick:
"Hard comes before Soft" - alphabetically AND anatomically (front to back)!
Question N8 In humans develop two successive sets of teeth ------------------ teeth and ------------------- teeth. Answer:
Answer: Deciduous (Milk) teeth and Permanent teeth
The Two Sets:
| Deciduous Teeth | Permanent Teeth | |
|---|---|---|
| Also called | Milk teeth, Baby teeth, Primary teeth | Adult teeth, Secondary teeth |
| When they appear | 6 months - 2 years of age | 6 - 12 years (replacing deciduous) |
| How many | 20 teeth | 32 teeth |
| Types | Incisors, Canines, Molars only | Incisors, Canines, Premolars, Molars |
Key Difference - What's missing in baby teeth?
Deciduous teeth have NO premolars! Permanent teeth add premolars + extra molars (wisdom teeth)
Dental Formula:
I 2/2 : C 1/1 : M 2/2 = 10 per jaw = 20 total
I 2/2 : C 1/1 : PM 2/2 : M 3/3 = 16 per jaw = 32 total
🧠 Memory Trick:
"Decide to leave at 6" - Deciduous teeth start falling out at age 6 "20 baby, 32 adult" - easy numbers to remember Baby teeth = no Premolars (P for Permanent only!)
Question N9 The surface of the crown is covered by a layer of -------------- the hardest substance in the body. Answer:
Answer: Enamel - the hardest substance in the human body
Structure of a Tooth - Layers:
CROWN (above gum)
├── Enamel ← outermost, hardest layer
├── Dentine ← bulk of the tooth (beneath enamel)
├── Pulp cavity ← nerves + blood vessels (feels pain!)
ROOT (below gum)
├── Cementum ← covers root (like enamel but softer)
├── Dentine ← continues from crown
└── Periodontal ligament ← anchors tooth to bone
Key Facts about Enamel:
| Feature | Detail |
|---|---|
| Hardest substance | In the entire human body |
| Made of | 96% hydroxyapatite (calcium phosphate crystals) |
| Produced by | Ameloblasts |
| Can it regenerate? | NO - once lost, gone forever |
| Covers | Only the crown (not the root) |
Root is covered by what?
Root = covered by Cementum (not enamel) This is a common trick question! ⚠️
🧠 Memory Trick:
"Enamel = A-MEL-oblasts make it" (AMELoblasts → AMEL → enAMEL) "Crown = Enamel, Root = Cementum" Hardest = Enamel > Dentine > Cementum > Bone
Question N10 Where is the pharyngeal opening of the pharyngotympanic tube? Answer:
Answer: Lateral wall of the Nasopharynx
What is the Pharyngotympanic Tube?
- Also called Eustachian tube / Auditory tube
- Connects the middle ear to the nasopharynx
- Function: equalizes pressure between middle ear and atmosphere
Its Two Openings:
| Opening | Location |
|---|---|
| Tympanic opening | Middle ear (tympanic cavity) |
| Pharyngeal opening | Lateral wall of nasopharynx (behind the inferior nasal concha) |
Exact Location of Pharyngeal Opening:
On the lateral wall of nasopharynx Just behind/posterior to the inferior nasal concha The opening has a raised ridge around it called the Torus tubarius
Why is this important clinically?
Infections from the throat/nose can travel up the tube → cause middle ear infections (Otitis media) This is why kids get ear infections after a cold! Children have a shorter, wider, more horizontal tube → more prone to ear infections
🧠 Memory Trick:
"Naso → tube → ear" Pharyngeal opening = NasoPHARYNX (it opens where its name says - PHARYNX!) Torus Tubarius = the little bump/cushion guarding the opening - "Torus = Tympanic tube's door"
Question N14 Which anatomical structure is not enclosed in the free edge of hepatoduodenal ligament? Answer: The aorta
Answer: The Aorta is NOT enclosed in the hepatoduodenal ligament ✅
What IS enclosed in the Hepatoduodenal Ligament?
| Structure | Position |
|---|---|
| Portal vein | Posterior |
| Hepatic artery proper | Left side (anterior) |
| Common bile duct (CBD) | Right side (anterior) |
🧠 Memory Trick - "VAN":
Vein (portal) - Artery (hepatic) - Nerve... wait, it's bile duct! Better trick: "Portal Triad = PHA" Portal vein + Hepatic artery + Aduct (bile duct)
Why NOT the Aorta?
The aorta runs behind the peritoneum (retroperitoneal) It is nowhere near the hepatoduodenal ligament The portal vein carries blood to liver - not the aorta!
Clinical Importance - Pringle's Manoeuvre:
Surgeons compress the hepatoduodenal ligament between fingers to stop liver bleeding This works because all 3 structures supplying/draining the liver pass through it! 🎯
Question N16 Spleen is connected to the left kidney by ------------------------------ ligament Answer: splenorenal ligament
Answer: Splenorenal ligament ✅
Simple Breakdown of the Name:
Spleno = Spleen + Renal = Kidney So splenorenal = spleen to kidney - the name tells you exactly what it connects!
All Ligaments of the Spleen:
| Ligament | Connects | Contains |
|---|---|---|
| Splenorenal (lienorenal) | Spleen → Left kidney | Splenic vessels + tail of pancreas |
| Gastrosplenic (gastrolienal) | Spleen → Stomach | Short gastric vessels + left gastroepiploic vessels |
| Phrenicosplenic | Spleen → Diaphragm | Nothing major |
| Splenocolic | Spleen → Colon | Nothing major |
Most Important One to Remember:
Splenorenal ligament carries the splenic artery & vein + tail of pancreas This is why the tail of pancreas is the closest part of pancreas to the spleen!
🧠 Memory Trick:
"RENAL = Kidney" (think renal failure, renal artery - always means kidney) "Spleno + Renal = Spleen to Kidney"
For the contents: "Splenorenal has the Splenic vessels and the Tail" Splenorenal = Splenic vessels + Tail of pancreas 🎯
Question N17 Spleen is connected to the stomach by ---------------------------- ligament Answer: gastrosplenic ligament
Answer: Gastrosplenic ligament ✅
Simple Breakdown:
Gastro = Stomach + Splenic = Spleen Name literally tells you: Stomach → Spleen!
What does it contain?
Short gastric vessels (branches of splenic artery) Left gastroepiploic vessels
Quick Comparison - The Two Main Splenic Ligaments:
| Ligament | Connects | Contains |
|---|---|---|
| Gastrosplenic | Stomach ↔ Spleen | Short gastric vessels + Left gastroepiploic vessels |
| Splenorenal | Spleen ↔ Kidney | Splenic vessels + Tail of pancreas |
Where do these ligaments come from?
Gastrosplenic = anterior layer of greater omentum Splenorenal = posterior layer of greater omentum
🧠 Memory Trick - The Spleen's Neighbours:
"Spleen shakes hands with 4 friends"
- Stomach → Gastrosplenic ligament
- Kidney → Splenorenal ligament
- Diaphragm → Phrenicosplenic ligament
- Colon → Splenocolic ligament
Just remember: "G-R-P-C" = Gastrosplenic, Renal, Phrenico, Colic 🎯
Question N18 Arterial supply of the spleen is provided by ---------------- artery which arise from the --------------- ---------------. Answer:
Answer: Splenic artery which arises from the Coeliac trunk
Full Answer:
Arterial supply = Splenic artery Arises from = Coeliac trunk (Coeliac axis)
The Coeliac Trunk - 3 Branches:
Coeliac Trunk (T12 level)
|
_____|_____
| | |
Left Common Splenic
Gastric Hepatic Artery
Artery Artery ↓
→ Spleen
🧠 Memory Trick for Coeliac Trunk branches:
"Left Hand Side" = Left gastric, Hepatic (common), Splenic Or: "The Liver, Stomach and Spleen all eat from the same COELIAC trunk!"
Key Features of the Splenic Artery:
| Feature | Detail |
|---|---|
| Course | Runs along upper border of pancreas |
| Characteristic | Most tortuous (twisted) artery in the body |
| Travels through | Splenorenal ligament to reach spleen |
| Also supplies | Pancreas (via pancreatic branches) + Stomach (via short gastric & left gastroepiploic) |
🧠 Extra Trick:
"Splenic artery = most TORTUOUS artery" - common exam fact! It winds and twists along the pancreas like a snake 🐍 🎯
Question N22 Left gastro-omental (epiploic) artery is branch of ----------------------------- Answer: splenic artery
Answer: Splenic artery ✅
The Gastro-omental (Gastroepiploic) Arteries - Both of them:
| Artery | Branch of | Runs along |
|---|---|---|
| Left gastro-omental | Splenic artery | Left side of greater curvature of stomach |
| Right gastro-omental | Gastroduodenal artery | Right side of greater curvature of stomach |
They meet and form an anastomosis:
Both arteries run along the greater curvature of stomach They meet in the middle and anastomose with each other This forms a vascular arcade along the greater curvature
🧠 Memory Trick:
"LEFT goes with LEFT" Left gastro-omental → Left side → comes from Splenic (which is on the left!)
"RIGHT goes with RIGHT" Right gastro-omental → Right side → comes from Gastroduodenal (which is on the right!)
Quick Recap of Splenic Artery Branches:
- Pancreatic branches (supplies pancreas)
- Short gastric arteries (supplies fundus of stomach)
- Left gastro-omental artery (supplies greater curvature)
- Terminal splenic branches (supplies spleen)
Common Exam Trick ⚠️:
Don't confuse Left gastro-omental (splenic) with Right gastro-omental (gastroduodenal) Just remember Left = Splenic always! 🎯
then where is the lesser curvature of stomach
Lesser Curvature = the shorter, right/upper border of the stomach
Picture the Stomach:
Fundus (top)
/
/ ← Lesser Curvature (short, concave, RIGHT side)
Esophagus → [ STOMACH ] → Duodenum
\ ← Greater Curvature (long, convex, LEFT side)
\
(bulges to the left)
Simple Way to Remember:
| Lesser Curvature | Greater Curvature | |
|---|---|---|
| Side | Right/medial | Left/lateral |
| Length | Shorter (concave) | Longer (convex) |
| Blood supply | Left & Right gastric arteries | Left & Right gastro-omental arteries |
| Covered by | Lesser omentum | Greater omentum |
Blood Supply Summary - Easy Table:
| Artery | Supplies | Branch of |
|---|---|---|
| Left gastric | Lesser curvature (left) | Coeliac trunk directly |
| Right gastric | Lesser curvature (right) | Hepatic artery |
| Left gastro-omental | Greater curvature (left) | Splenic artery |
| Right gastro-omental | Greater curvature (right) | Gastroduodenal artery |
🧠 One Rule to Remember:
Lesser curvature = Gastric arteries Greater curvature = Gastro-omental arteries
can u give me an image showing right and left greater curvature along with lesser curvature
Anatomical diagram of the stomach showing blood supply, with labels for: Lesser Curvature (right/medial side), Greater Curvature (left/lateral side), Left Gastric Artery along lesser curvature, Right Gastric Artery along lesser curvature, Left Gastro-omental Artery along greater curvature, Right Gastro-omental Artery along greater curvature, Fundus at top, Pylorus connecting to Duodenum on right, Esophagus entering on left top, Lesser Omentum covering lesser curvature, Greater Omentum hanging from greater curvature, Coeliac Trunk branching into Splenic Artery and Common Hepatic Artery, clean medical education style with color coded arteries
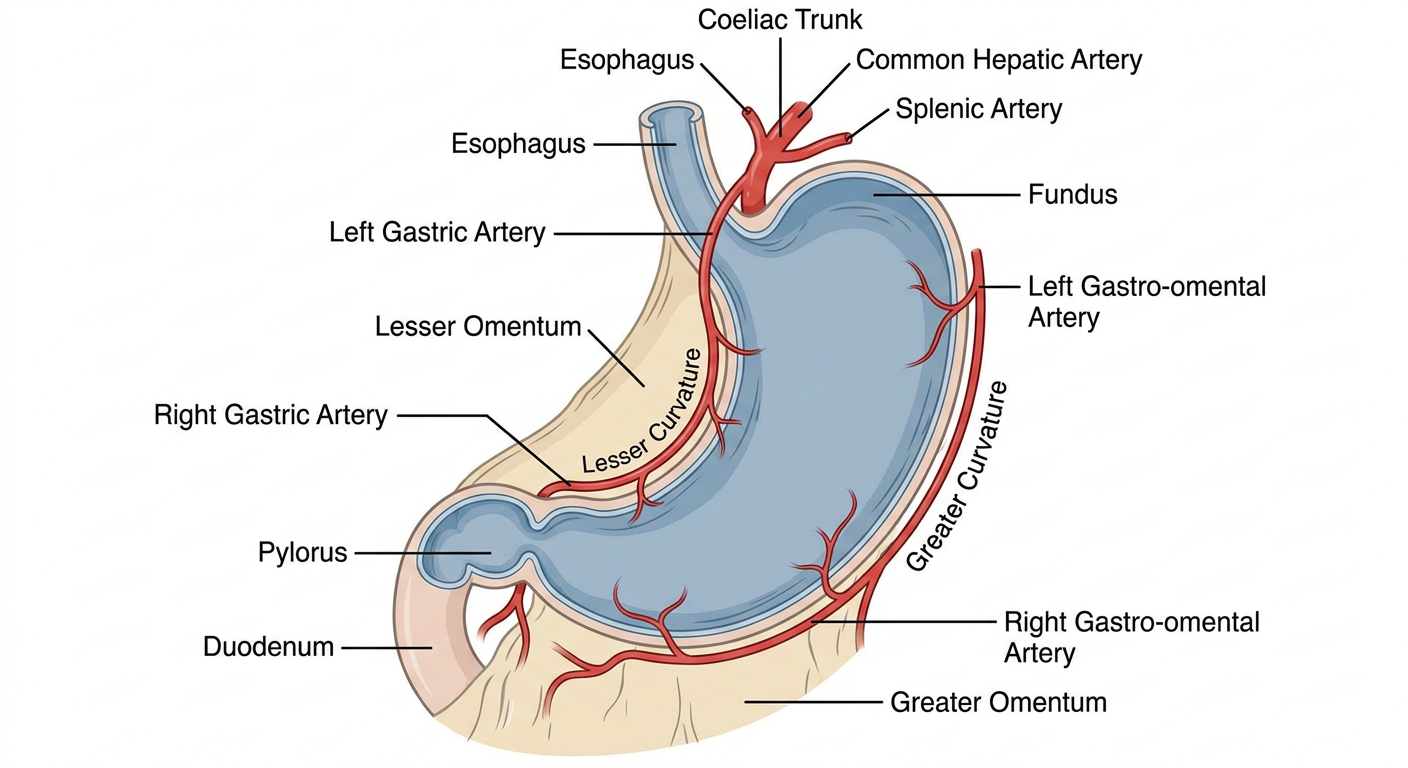
Quick Reference from the image:
- Lesser Curvature (right/concave side) → supplied by Left + Right Gastric arteries
- Greater Curvature (left/convex side) → supplied by Left + Right Gastro-omental arteries
🧠 Recap:
| Artery | From | Where |
|---|---|---|
| Left Gastric | Coeliac trunk | Lesser curvature (left part) |
| Right Gastric | Hepatic artery | Lesser curvature (right part) |
| Left Gastro-omental | Splenic artery | Greater curvature (left part) |
| Right Gastro-omental | Gastroduodenal artery | Greater curvature (right part) |
what is cecum
Cecum = the beginning of the large intestine
Simple Definition:
The cecum is a blind-ended pouch (dead-end sac) that forms the first part of the large intestine "Cecum" = Latin for "blind" - because it's closed at one end
Where is it?
Right iliac fossa (lower right region of abdomen) Just below where the small intestine joins the large intestine
Picture it:
Small intestine (ileum)
↓
[ILEOCECAL VALVE]
↓
┌─────────┐
│ CECUM │ ← blind pouch (right iliac fossa)
└────┬────┘
|
Appendix ← hangs from the bottom of cecum
|
Ascending colon → goes upward
Key Facts:
| Feature | Detail |
|---|---|
| Position | Right iliac fossa |
| Part of | Large intestine (first part) |
| Connected to | Ileum (via ileocecal valve) above, Ascending colon below |
| Attached to | Appendix hangs from its posteromedial wall |
| Covered by | Peritoneum (intraperitoneal) |
Ileocecal Valve:
The valve between ileum and cecum Prevents backflow of large intestinal contents into small intestine
🧠 Memory Trick:
"C for Cecum = C for Commencement" - it's where the large intestine STARTS "Cecum = blind bag with a tail (appendix)" Location: "Right iliac fossa" = same side as appendix (that's why appendix pain is in the right lower abdomen!) 🎯
Question N32 Left renal artery is longer and passes posterior to the inferior vena cava Answer: 0 0.25 (Question Point) Points Received: 0.25
Answer: FALSE - This statement is WRONG ❌
What's Wrong With the Statement?
| Left Renal Artery | Right Renal Artery | |
|---|---|---|
| Length | SHORTER | LONGER |
| Passes posterior to IVC? | NO | YES ✅ |
The Correct Facts:
RIGHT renal artery = longer + passes posterior to the IVC LEFT renal artery = shorter (aorta is closer to left kidney)
Why?
Aorta IVC
| |
Left | | Right
Kidney | | Kidney
|←short→|←——long——→|
Left RA Right RA
(must cross
behind IVC)
- The aorta sits slightly to the LEFT of midline
- So the left renal artery is SHORT (kidney is right next to aorta)
- The right renal artery is LONGER because it has to travel across to reach the right kidney AND pass behind the IVC
🧠 Memory Trick:
"Right is LONG and goes BEHIND the IVC" "Left is SHORT because aorta is on the LEFT"
Think: Right renal artery = the long way around (has to sneak behind the IVC!) 🎯
Similarly for Renal VEINS (opposite rule!):
Left renal vein = LONGER (has to travel across to reach IVC) Right renal vein = SHORTER (IVC is right next to right kidney)
⚠️ Arteries and veins are opposite - common exam trick!
Question N33 The left renal artery usually arises a little higher than the right renal artery Answer:
Answer: TRUE ✅
Why does the Left arise higher?
Both renal arteries arise from the aorta at L1-L2 level But the left renal artery arises slightly HIGHER than the right
Reason - Position of the Kidneys:
| Kidney | Position | Why |
|---|---|---|
| Right kidney | Sits LOWER | Pushed down by the liver above it |
| Left kidney | Sits HIGHER | Spleen is lighter, doesn't push it down as much |
Since the left kidney sits higher → its artery also arises at a slightly higher level from the aorta
Summary of Left vs Right Renal Artery:
| Feature | Left Renal Artery | Right Renal Artery |
|---|---|---|
| Length | Shorter | Longer |
| Level of origin | Slightly higher ✅ | Slightly lower |
| Passes behind IVC? | No | Yes |
🧠 Memory Trick:
"Left kidney is the higher kidney" (liver pushes right one down) "Higher kidney = Higher artery origin"
Easy way to remember kidney levels: "Liver is heavy = pushes RIGHT kidney DOWN" So Right kidney is lower, Left kidney is higher! 🎯
Connects to previous question:
Right artery = longer + lower origin + passes behind IVC Left artery = shorter + higher origin + no IVC crossing
what does rises above mean?
Simple Picture:
AORTA (going downward)
|
L1 ——→ [Left renal artery] ← branches off HERE (higher up)
|
L2 ——→ [Right renal artery] ← branches off HERE (lower down)
|
↓
Think of it like floors in a building:
Aorta = a tall building with pipes branching off at different floors Left renal artery = branches off at floor 1 (higher) Right renal artery = branches off at floor 2 (lower)
In anatomy "higher" = closer to the head:
| Term | Meaning |
|---|---|
| Higher / Superior | Closer to the head |
| Lower / Inferior | Closer to the feet |
The left renal artery leaves the aorta at a point closer to the head compared to where the right renal artery leaves
🧠 One line summary:
"Higher = more towards the head = higher vertebral level (L1 vs L2)"
Question N34 The psoas major, quadratus lumborium and transversus abdominis muscles are posterior relations of the the right and left kidneys. Answer:
Answer: TRUE ✅
The 3 Posterior Relations of Both Kidneys:
| Muscle | Position relative to kidney |
|---|---|
| Psoas major | Medial (inner) part of posterior surface |
| Quadratus lumborum | Middle/lateral part of posterior surface |
| Transversus abdominis | Lateral (outer) part of posterior surface |
Picture it:
KIDNEY (viewed from behind)
___________________________
| | | |
| Psoas | Quadratus| Trans-|
| Major | Lumborum |versus |
| (medial)| (middle) |(lat.) |
|________|__________|_______|
The kidney rests on these 3 muscles like sitting on a 3-seater sofa!
🧠 Memory Trick:
"PQT" = Psoas, Quadratus, Transversus From medial to lateral: P → Q → T
"Pretty Queen Travels" = Psoas, Quadratus, Transversus 😄
Additional Posterior Relations (nerves passing through):
- Subcostal nerve (T12)
- Iliohypogastric nerve (L1)
- Ilioinguinal nerve (L1)
Key point ⚠️:
These are posterior relations of BOTH right and left kidneys - same for both sides! ✅ 🎯
cranial nerve 5?
CN V = Trigeminal Nerve - the largest cranial nerve
3 Divisions - "TRI = 3":
| Division | Name | Area it supplies | Foramen |
|---|---|---|---|
| V1 | Ophthalmic | Forehead, eye, nose tip | Superior orbital fissure |
| V2 | Maxillary | Cheek, upper lip, upper teeth | Foramen rotundum |
| V3 | Mandibular | Lower lip, lower teeth, chin, tongue, ear | Foramen ovale |
🧠 Memory Trick for Foramina:
"Standing Room Only" Superior orbital fissure → Rotundum → Ovale V1 → V2 → V3
What does CN V do?
| Function | Which division |
|---|---|
| Sensation of face | ALL three (V1, V2, V3) |
| Motor (chewing muscles) | V3 ONLY |
V1 and V2 = purely sensory V3 = sensory + motor
Motor muscles supplied by V3:
"My Teeth Masticate Very Little"
- Masseter
- Temporalis
- Medial pterygoid
- Lateral pterygoid
- Mylohyoid, Tensor tympani, Tensor veli palatini, Anterior belly of digastric
Ganglia associated with CN V:
| Ganglion | Associated with |
|---|---|
| Trigeminal (Gasserian) ganglion | Main sensory ganglion of CN V |
| Ciliary ganglion | V1 |
| Pterygopalatine ganglion | V2 |
| Otic ganglion | V3 |
| Submandibular ganglion | V3 |
Clinical Points:
Trigeminal neuralgia = sudden severe facial pain in CN V distribution Corneal reflex = afferent is CN V1, efferent is CN VII Dentist injections block V2 and V3 branches!
🧠 One Final Trick - Which division covers what:
V1 = above the eye (Very top) V2 = below eye, above mouth (middle) V3 = below mouth + jaw (bottom) + MOTOR
Think of the face divided into 3 horizontal strips top to bottom = V1, V2, V3! 🎯
soft palate muscles
Soft Palate has 5 muscles
🧠 Memory Trick to remember all 5:
"T-P-P-L-M" or say: "Tensor, Levator, Palatoglossus, Palatopharyngeus, Musculus Uvulae" = "Two Lovers Play Perfectly Music" 😄
The 5 Muscles - Simple Table:
| Muscle | Action | Nerve supply |
|---|---|---|
| Tensor veli palatini | Tenses (tightens) soft palate + opens Eustachian tube | CN V3 (only one NOT from CN X!) |
| Levator veli palatini | Elevates soft palate (closes off nasopharynx during swallowing) | CN X |
| Palatoglossus | Elevates tongue + closes off oropharynx | CN X |
| Palatopharyngeus | Pulls pharynx upward during swallowing | CN X |
| Musculus uvulae | Shortens + elevates uvula | CN X |
The BIG EXAM POINT ⚠️:
ALL soft palate muscles are supplied by CN X (Vagus) via pharyngeal plexus EXCEPT Tensor veli palatini = CN V3 (Trigeminal)
🧠 Trick for the Exception:
"TENSOR is the TENSE one - it goes its own way with V3!" All others follow CN X - only Tensor rebels!
Functions during Swallowing:
Levator lifts soft palate → seals off nose (so food doesn't go up your nose!) Tensor opens Eustachian tube → equalizes ear pressure during swallowing (That's why your ears "pop" when you swallow!)
Clinical Point:
If CN X is damaged → soft palate droops on that side Uvula deviates to the normal (unaffected) side Remember: "Uvula runs away from the damaged side" 🎯
The ceiling of nasopharynx is formed by the sloping base of the skull and consists of: Answer: The posterior part of the body of the sphenoid bone and the basal part of the occipital bone i wanna the anatomical positioning
Ceiling of Nasopharynx - Anatomical Position
Picture the Skull Base from the Side (Sagittal view):
FRONT BACK
| |
| Cribriform Sphenoid Occipital |
| plate bone bone |
| (ethmoid) | | |
| ↓ ↓ |
| [Body of [Basal part |
| Sphenoid] of Occiput] |
| \ / |
| \ / |
| SLOPING ROOF |
| ↓ |
| NASOPHARYNX CEILING |
The Two Bones forming the Ceiling:
| Bone | Part involved | Position |
|---|---|---|
| Sphenoid bone | Posterior part of its body | ANTERIOR part of the ceiling |
| Occipital bone | Basal part (basilar part) | POSTERIOR part of the ceiling |
Where exactly are these bones?
Sits in the middle of the skull base Think of it as the "keystone" of the skull Its posterior part slopes downward → forms front of nasopharynx roof
The part of occipital bone that is in front of the foramen magnum Slopes downward and forward Forms the back of nasopharynx roof
They meet at:
Spheno-occipital synchondrosis (a cartilaginous joint) This fuses around age 20-25
Simple Diagram - Front to Back:
Nose → Sphenoid body → Spheno-occipital junction → Basal Occipital → Foramen magnum
↑ ↑ ↑
(anterior (where they (posterior
ceiling) meet) ceiling)
\__________________________________/
NASOPHARYNX ROOF
(slopes downward
like a slide)
🧠 Memory Trick:
"S before O" = Sphenoid is anterior, Occipital is posterior (Alphabetical order = front to back!)
The roof slopes because: Sphenoid is higher up → Occipital slopes down toward foramen magnum Like a slide going backward and downward 🎯
Clinical Relevance:
Nasopharyngeal carcinoma grows right at this roof It can erode into the sphenoid/occipital bones That's why it can damage CN VI (abducens) early - the nerve runs nearby!
can u show me via diagrams and images
Detailed sagittal cross-section anatomical diagram of the human head showing the nasopharynx and skull base, with clear labels for: Sphenoid bone body (anterior part of nasopharynx roof), Basal/Basilar part of Occipital bone (posterior part of nasopharynx roof), Spheno-occipital synchondrosis (junction between the two bones), Foramen magnum, Nasopharynx cavity below the sloping roof, Hard palate below nasopharynx, Soft palate, Nasal cavity in front, the sloping angle of the roof clearly shown, arrows indicating anterior and posterior directions, clean medical education style with color coding for sphenoid bone in blue and occipital bone in orange
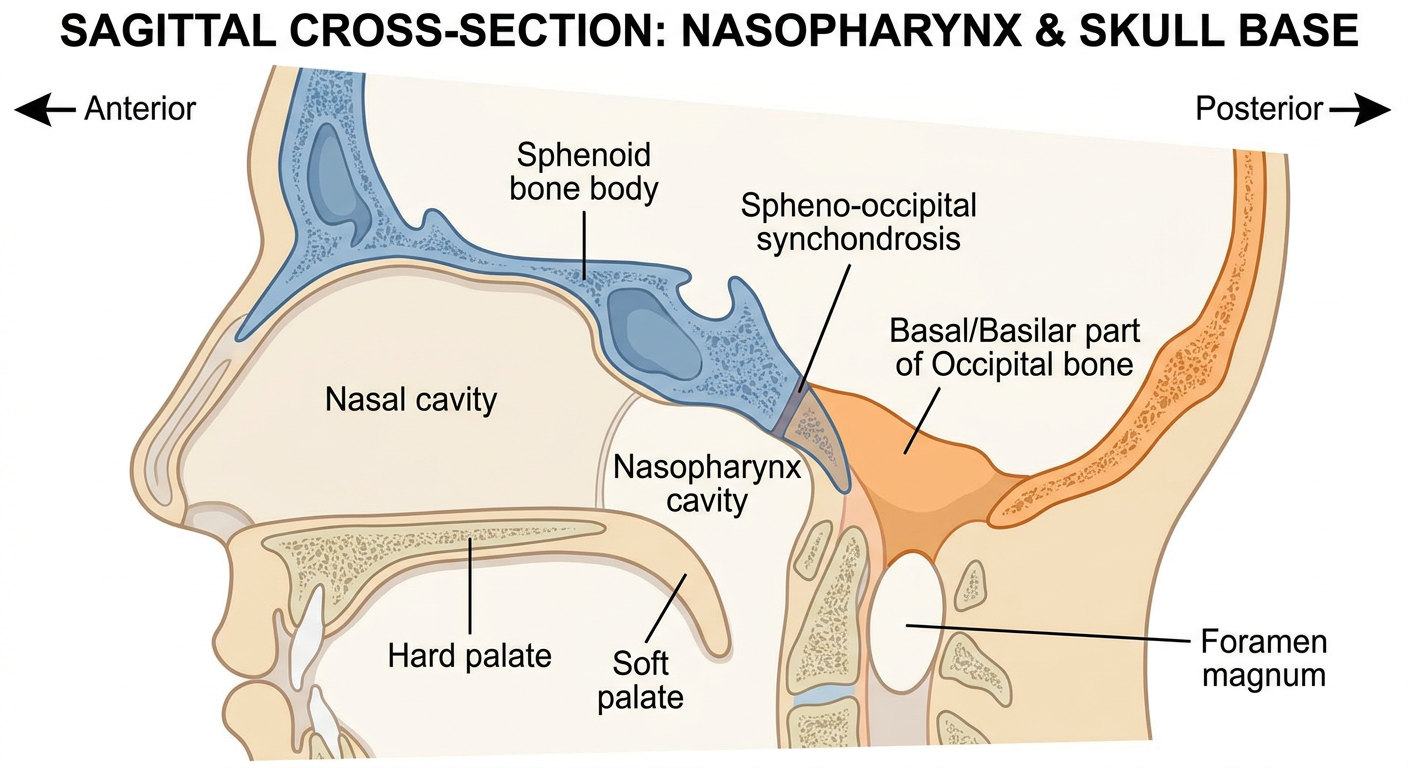
Reading the Diagram:
FRONT (nose side) →→→ BACK (throat side)
↓ ↓
SPHENOID BODY BASAL OCCIPITAL
(blue - anterior) (orange - posterior)
\ /
\__________________________________/
↑ SPHENO-OCCIPITAL JUNCTION
(fuses at age 20-25)
↓
NASOPHARYNX CAVITY
↓
Hard palate → Soft palate
Key Points from the image:
| Structure | Color | Position |
|---|---|---|
| Sphenoid body | 🔵 Blue | Anterior roof |
| Basal Occipital | 🟠 Orange | Posterior roof |
| Their junction | Middle | Spheno-occipital synchondrosis |
| Foramen magnum | Behind occipital | Where spinal cord exits |
🧠 Final Trick:
The roof SLOPES like a slide - higher at front (sphenoid), lower at back (occipital) "S before O" = Sphenoid (front) → Occipital (back) 🎯
what is hypochondrium?
Hypochondrium = the upper side regions of the abdomen, just below the ribs
The 9 Regions of the Abdomen:
RIGHT CENTRE LEFT
┌─────────────┬──────────────┬─────────────┐
│ RIGHT │ EPIGASTRIC │ LEFT │ ← TOP ROW
│HYPOCHONDRIUM│ REGION │HYPOCHONDRIUM│
├─────────────┼──────────────┼─────────────┤
│ RIGHT │ UMBILICAL │ LEFT │ ← MIDDLE ROW
│ LUMBAR │ REGION │ LUMBAR │
├─────────────┼──────────────┼─────────────┤
│ RIGHT │ HYPOGASTRIC│ LEFT │ ← BOTTOM ROW
│ ILIAC FOSSA│ (PUBIC) │ ILIAC FOSSA│
└─────────────┴──────────────┴─────────────┘
What's in each Hypochondrium?
| Region | Main Organs |
|---|---|
| Right Hypochondrium | Liver (right lobe), Gallbladder, Right kidney (upper), Hepatic flexure of colon |
| Left Hypochondrium | Spleen, Stomach (fundus), Left kidney (upper), Splenic flexure of colon, Tail of pancreas |
What does "Hypochondrium" mean?
"Hypo" = below "Chondrium" = cartilage (costal cartilage/ribs) So literally = "below the ribs/cartilage"
🧠 Memory Trick:
Right Hypo = LIVER + GALLBLADDER (that's why liver pain/gallstones = right upper quadrant pain) Left Hypo = SPLEEN (that's why spleen pain = left upper quadrant pain)
"Right Hypo = Liver's home" "Left Hypo = Spleen's home" 🎯
Also know the word "Hypochondriac":
A person who always thinks they're sick! Originally meant someone who always complained of pain in the hypochondrium region 😄
Question N16 The ------------------- is large, fan-shaped double-layered fold of peritoneum that connects the jejunum and ileum to the posterior abdominal wall
Answer: Mesentery
Full Definition:
The mesentery is a large, fan-shaped, double-layered fold of peritoneum that connects the jejunum and ileum to the posterior abdominal wall
Key Features:
| Feature | Detail |
|---|---|
| Shape | Fan-shaped (wide at intestinal end, narrow at root) |
| Layers | Double layer of peritoneum |
| Connects | Jejunum + Ileum → Posterior abdominal wall |
| Root of mesentery | Runs from L2 vertebra (left side) to right sacroiliac joint |
| Length of root | About 15 cm long |
| Length of intestinal border | About 6 metres long (length of small intestine!) |
What travels inside the mesentery?
Between the two layers of peritoneum:
- Superior mesenteric artery & vein
- Lymphatics
- Autonomic nerves
- Fat
Picture it:
Posterior abdominal wall
|
[ROOT - 15cm]
|
\\\\\|///// ← fan shaped, spreading out
\\\\|////
\\\|///
Jejunum + Ileum (6 metres!)
🧠 Memory Trick:
"Mesentery = the small intestine's FAN" Short root (15cm) holds a very long intestine (6m) - like a fan!
"Mesen-tery = Middle-territory" - it's in the middle of the abdomen holding the middle part of the gut (jejunum + ileum) 🎯
Don't confuse with:
| Structure | Connects |
|---|---|
| Mesentery | Jejunum + Ileum → posterior wall |
| Transverse mesocolon | Transverse colon → posterior wall |
| Sigmoid mesocolon | Sigmoid colon → posterior wall |
Question N17 The spleen is surrounded by visceral peritoneum except in the area -------------------- of the spleen
Answer: Hilum (Hilus) of the spleen
Why is the Hilum not covered by peritoneum?
The hilum is where all the vessels enter and exit the spleen Blood vessels, lymphatics and nerves need a "doorway" to get in Peritoneum cannot cover this opening - it would block the vessels!
What passes through the Hilum?
| Structure | Direction |
|---|---|
| Splenic artery | Enters spleen |
| Splenic vein | Exits spleen |
| Lymphatic vessels | Exit spleen |
| Nerve fibers | Enter spleen |
| Tail of pancreas | Reaches up to (but doesn't enter) hilum |
Location of the Hilum:
On the medial (visceral) surface of the spleen Faces toward the stomach Connected to stomach via gastrosplenic ligament Connected to kidney via splenorenal ligament
Simple Analogy:
Spleen = an orange Peritoneum = the peel covering it Hilum = the belly button of the orange where the stalk was The peel (peritoneum) has a gap at the belly button (hilum)! 🍊
🧠 Memory Trick:
"HILUM = HOLE" - it's the hole/gap in the peritoneum Same rule applies to ALL organs: Kidney hilum, Lung hilum, Liver porta hepatis - all are gaps where vessels enter/exit = no peritoneum there! 🎯
Question N27 The descending part (second part) of the duodenum is just to the right of midline and extends Answer: From the neck of the gallbladder to the lower border of vertebra LIII can u please xeplain this via images
Detailed anatomical diagram showing the 4 parts of the duodenum in C-shape with vertebral levels labeled on the right side, showing: First part (superior) at L1 level near neck of gallbladder, Second part (descending) running vertically from L1 to L3 level just to the right of midline, Third part (horizontal/inferior) crossing at L3 level, Fourth part (ascending) going up to L2 level at duodenojejunal flexure, gallbladder and its neck shown above connected to the start of second part, bile duct and pancreatic duct entering the second part at major duodenal papilla (ampulla of Vater), head of pancreas sitting inside the C-curve, vertebral column shown on the left with L1 L2 L3 L4 levels clearly labeled, midline indicated with dotted line, second part highlighted in different color to emphasize it, clean medical education anatomical style
Medical anatomy diagram of the duodenum showing C-shaped loop with 4 parts labeled. The second part descends vertically on the right side of spine from upper L1 to lower L3 vertebral level. Gallbladder neck shown at the top near where second part begins. Vertebral levels L1, L2, L3 marked. Head of pancreas sits inside the C-curve. Bile duct enters the second part. Simple clean educational medical illustration with colored labels.
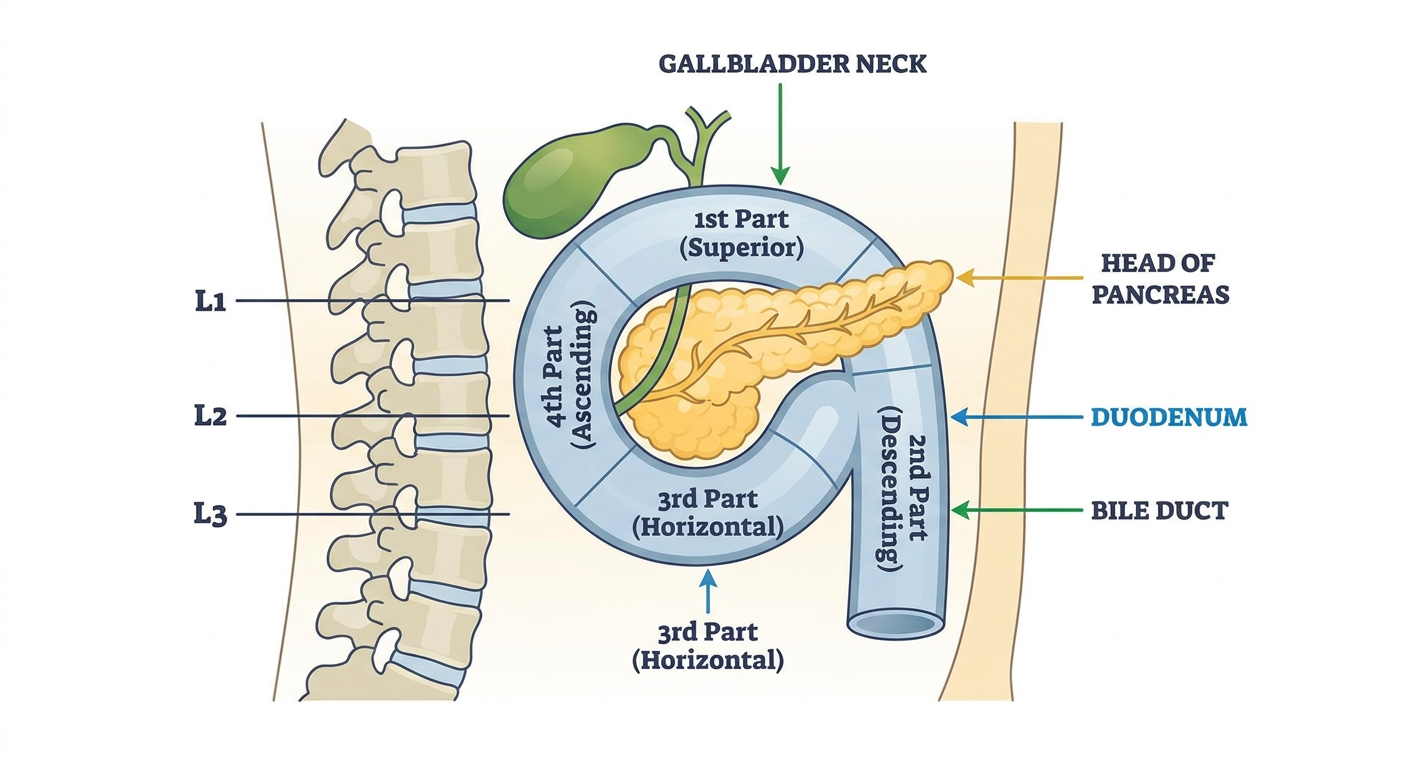
All 4 Parts of the Duodenum - With Levels:
| Part | Name | Vertebral Level | Direction |
|---|---|---|---|
| 1st part | Superior | L1 | Horizontal (goes right) |
| 2nd part | Descending ⭐ | L1 to L3 | Goes DOWN (vertical) |
| 3rd part | Horizontal/Inferior | L3 | Horizontal (goes left) |
| 4th part | Ascending | L3 to L2 | Goes UP then left |
Focus on 2nd Part (Descending):
Neck of Gallbladder (L1 level)
↓
┌──────────────┐
│ 2nd part │ ← RIGHT of midline
│ DESCENDING │ ← Bile duct + Pancreatic duct open here
│ (vertical) │ ← Major duodenal papilla (Ampulla of Vater)
└──────────────┘
↓
Lower border of L3
Key contents of 2nd part:
Major duodenal papilla (Ampulla of Vater) - where bile + pancreatic juice enter Minor duodenal papilla - where accessory pancreatic duct opens
🧠 Memory Trick:
"2nd part = DOWN from gallbladder neck to L3" "Bile meets gut at the 2nd part" - most important part clinically! Pancreatic head hugs the inside of the C-curve 🎯
Question N29 The omental appendices, taeniae coli and haustra coli is observed in the rectum and anal canal Answer:
Answer: FALSE ❌
Why FALSE?
The 3 Special Features of the Colon:
| Feature | What it is | Present in Rectum? |
|---|---|---|
| Taeniae coli | 3 thickened bands of longitudinal muscle running along colon | ❌ NO |
| Haustra coli | Pouches/sacculations of the colon wall | ❌ NO |
| Omental appendices (appendices epiploicae) | Small fat-filled pouches hanging off colon | ❌ NO |
What happens at the Rectum?
At the rectosigmoid junction, all 3 features disappear:
- Taeniae coli spread out to form a complete longitudinal muscle layer
- Haustra disappear (rectum is smooth)
- Omental appendices disappear
Simple Picture:
COLON RECTUM
─────────────────────────────────────────
Has taeniae coli → Spreads into full muscle coat
Has haustra → Smooth wall (no pouches)
Has omental app. → No fat tags
🧠 Memory Trick:
"The 3 H-T-O features = COLON only!" Haustra + Taeniae + Omental appendices = HTO = Hold The Order (they stop at rectum!)
Or simply: "Rectum is SMOOTH - it lost all 3 decorations of the colon" 🎯
Why does this matter clinically?
On X-ray/colonoscopy:
- Colon = haustral markings visible
- Rectum = smooth, no markings This helps identify which part of bowel you're looking at! ✅
Question N30 The left colic flexure is higher than right colic flexure what is colic flexure and why so
Answer: TRUE ✅ - Left colic flexure IS higher than right
First - What is a Colic Flexure?
A colic flexure = a bend/turn in the colon "Colic" = related to colon "Flexure" = a bend or curve
| Flexure | Also called | Location | Side |
|---|---|---|---|
| Right colic flexure | Hepatic flexure | Under the liver | Right side |
| Left colic flexure | Splenic flexure | Under the spleen | Left side |
Why is the Left (Splenic) Flexure HIGHER?
LEFT SIDE RIGHT SIDE
─────────────────────────────────────────
Spleen sits HIGH Liver sits LOWER
(light organ, (heavy organ,
not pushed down) pushes things down)
↓ ↓
Left flexure Right flexure
sits HIGHER sits LOWER
(under spleen) (under liver)
Simple Comparison:
| Left (Splenic) Flexure | Right (Hepatic) Flexure | |
|---|---|---|
| Height | HIGHER | Lower |
| Neighbour | Spleen (light) | Liver (heavy) |
| Angle | More acute (sharp bend) | Less acute |
| Clinical note | Harder to reach in colonoscopy | Easier to reach |
The Full Colon Path:
Cecum (low, right)
↓
Ascending colon (goes UP)
↓
RIGHT (Hepatic) flexure ← lower, under liver
↓
Transverse colon (crosses left to right)
↓
LEFT (Splenic) flexure ← HIGHER, under spleen
↓
Descending colon (goes DOWN)
↓
Sigmoid colon
↓
Rectum
🧠 Memory Trick:
"Left is loftier" = Left flexure is Higher "Liver is heavy = pulls right flexure DOWN" "Spleen is lighter = left flexure stays UP HIGH"
Also: Left splenic flexure is more acute (sharper angle) - that's why it's harder to pass a colonoscope through it! 🎯
Question N31 All parts of the large intestine considered as intraperitoneal. Answer: (false)
Answer: FALSE ❌
First - What do these terms mean?
| Term | Meaning |
|---|---|
| Intraperitoneal | Covered by peritoneum on ALL sides, has a mesentery, can move freely |
| Retroperitoneal | Behind the peritoneum, covered only on front, fixed to posterior wall |
| Extraperitoneal | Completely outside peritoneum |
Large Intestine - Peritoneal Status:
| Part | Peritoneal Status |
|---|---|
| Cecum | Intraperitoneal ✅ |
| Appendix | Intraperitoneal ✅ |
| Ascending colon | Retroperitoneal ❌ |
| Right colic flexure | Retroperitoneal ❌ |
| Transverse colon | Intraperitoneal ✅ (has transverse mesocolon) |
| Left colic flexure | Retroperitoneal ❌ |
| Descending colon | Retroperitoneal ❌ |
| Sigmoid colon | Intraperitoneal ✅ (has sigmoid mesocolon) |
| Rectum | Retroperitoneal ❌ |
| Anal canal | Extraperitoneal ❌ |
🧠 Memory Trick:
Intraperitoneal parts = "CATS" Cecum, Appendix, Transverse colon, Sigmoid colon
Everything else = Retroperitoneal/Extraperitoneal!
Simple Pattern:
FIXED parts (retro) = Ascending, Descending, Flexures, Rectum
MOBILE parts (intra) = Cecum, Appendix, Transverse, Sigmoid
Mobile parts have MESENTERIES - that's what makes them intraperitoneal!
- Transverse colon → transverse mesocolon
- Sigmoid colon → sigmoid mesocolon
- Appendix → mesoappendix 🎯
Question N8 The lips are encircled by -------------- ---------------- muscle, which acts as a spinchter. Answer: orbicularis oris
Answer: Orbicularis Oris ✅
What is Orbicularis Oris?
A circular muscle that surrounds the mouth/lips Works like a sphincter - it encircles and closes the opening "Orbicularis" = circular/ring-shaped "Oris" = of the mouth
Key Facts:
| Feature | Detail |
|---|---|
| Shape | Circular (sphincter-like) |
| Location | Surrounds the lips |
| Nerve supply | CN VII (Facial nerve) |
| Action | Closes lips, purses lips, protrudes lips |
What it does:
- Closes the mouth (sphincter action)
- Whistling 🎵
- Kissing 💋
- Sucking (important in babies for breastfeeding)
- Helps in speech
The "Orbicularis" Family - 2 members:
| Muscle | Location | Action |
|---|---|---|
| Orbicularis Oris | Around mouth | Closes lips |
| Orbicularis Oculi | Around eye | Closes eyelids |
🧠 Memory Trick:
"Orbicularis = Circular" (like an orbit/circle) "Oris = Oral = Mouth" "Oculi = Ocular = Eye"
Both are supplied by CN VII (Facial nerve) If CN VII is damaged (Bell's palsy) → can't close mouth or eye properly! 🎯
Greater curvature of the stomach is supplied by ------------------------ and -------------------------- arteries. Answer: right and left gastro omental arteries which arrive from splenic artery
Answer: Partially correct - needs a small correction! ⚠️
Correct Answer:
- Left gastro-omental artery - branch of Splenic artery ✅
- Right gastro-omental artery - branch of Gastroduodenal artery ❌ (NOT splenic!)
The Correction:
| Artery | Branch of | Side of Greater Curvature |
|---|---|---|
| Left gastro-omental | Splenic artery | Left side |
| Right gastro-omental | Gastroduodenal artery | Right side |
Only the LEFT one comes from splenic artery The RIGHT one comes from gastroduodenal artery (which is a branch of common hepatic artery → coeliac trunk)
Full Stomach Blood Supply - Master Table:
| Curvature | Artery | Branch of |
|---|---|---|
| Lesser (left) | Left gastric | Coeliac trunk directly |
| Lesser (right) | Right gastric | Hepatic artery proper |
| Greater (left) | Left gastro-omental | Splenic artery |
| Greater (right) | Right gastro-omental | Gastroduodenal artery |
| Fundus | Short gastric arteries | Splenic artery |
🧠 Memory Trick:
"LEFT side = SPLENIC" (both on left side of body) "RIGHT side = HEPATIC/GASTRODUODENAL" (both on right side)
Lesser curvature = GASTRIC arteries Greater curvature = GASTRO-OMENTAL arteries
Think: "Greater needs MORE arteries from DIFFERENT sources" - that's why it gets supply from both splenic AND gastroduodenal! 🎯
Question N32 Several minor calices of the kidneys unite to form renal pelvis Answer:
Answer: FALSE ❌
Why FALSE?
The Correct Order - Urine drainage pathway:
Renal Papilla (tip of renal pyramid)
↓ drains into
Minor Calyx (plural = calices)
↓ 2-3 minor calices unite to form
Major Calyx
↓ 2-3 major calices unite to form
Renal Pelvis
↓
Ureter
↓
Urinary Bladder
The Correct Statement Should Be:
Several minor calices unite to form major calices Several major calices unite to form the renal pelvis
Numbers to Remember:
| Structure | Number |
|---|---|
| Minor calices | 7-14 per kidney |
| Major calices | 2-3 per kidney |
| Renal pelvis | 1 per kidney |
Simple Analogy:
Think of it like a tree:
- Minor calices = small branches
- Major calices = big branches
- Renal pelvis = trunk
- Ureter = root going down
🧠 Memory Trick:
"Minor → Major → Pelvis → Ureter" "Small cups → Big cups → Funnel → Pipe"
Minor calices are like small cups catching urine from each papilla They pour into bigger cups (major calices) Which pour into the funnel (renal pelvis) Which drains into the pipe (ureter)! 🎯
Question N4 Parotid duct opens into the oral cavity near the ---------------- ------------------- ------------------- ------------------
Answer: Crown of the upper second molar tooth
Full Answer (4 blanks):
Parotid duct opens into the oral cavity near the crown of the upper second molar tooth
The Complete Path of Parotid Duct (Stensen's Duct):
Parotid gland (in front of ear)
↓
Runs horizontally over MASSETER muscle
↓
Turns sharply inward (medially)
↓
Pierces BUCCINATOR muscle
↓
Opens at PAROTID PAPILLA
(opposite the crown of upper 2nd molar tooth)
Key Landmarks:
| Landmark | Detail |
|---|---|
| Opens opposite | Upper 2nd molar tooth |
| Opening called | Parotid papilla (small raised bump) |
| Muscle it pierces | Buccinator |
| Muscle it runs over | Masseter |
Why upper 2nd molar specifically?
It is the largest upper molar Its crown is at the exact level where the duct enters the cheek You can feel the parotid papilla with your tongue on your inner cheek!
🧠 Memory Trick:
"Parotid opens near the 2nd upper molar" "2nd molar = 2nd salivary gland opening" (parotid is the 2nd largest salivary gland... well actually largest - but the trick helps!)
Better trick: "P2 = Parotid → 2nd molar" 🎯
All 3 Salivary Gland Openings - Bonus:
| Gland | Opens at |
|---|---|
| Parotid | Opposite upper 2nd molar (parotid papilla) |
| Submandibular | Sublingual papilla (beside frenulum of tongue) |
| Sublingual | Sublingual fold (floor of mouth) via multiple openings |
Question N32 Several minor calices of the kidneys unite to form renal pelvis
the jejunum mostly occupies which quadrant of abdomen