Pain gate theory
Reading File
Searching the Web
gate control theory of pain Melzack Wall mechanism
Finding Sources
Searching PubMed
"gate control theory" pain
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich, authoritative textbook content and two excellent diagrams. Here is the full answer:
Gate Control Theory of Pain
Origin
Proposed in 1965 by Ronald Melzack and Patrick Wall in their landmark paper "Pain Mechanisms: A New Theory" (Science, 150:971). It was the first model to show that pain is not a simple one-way transmission from periphery to brain - rather, pain signals are actively modulated before they reach consciousness.
Core Circuit
The gate operates in the dorsal horn of the spinal cord (particularly the substantia gelatinosa, laminae I and II). Three neuronal players are involved:
| Cell | Role |
|---|---|
| C fibers (small, unmyelinated) | Nociceptive - carry pain signals, "open the gate" |
| A-beta (Aβ) fibers (large, myelinated) | Non-nociceptive - carry touch/pressure/vibration, "close the gate" |
| Inhibitory interneuron (substantia gelatinosa) | The gate keeper |
| Projection neuron (T-cell) | Transmits signal up the anterolateral tract to the brain |
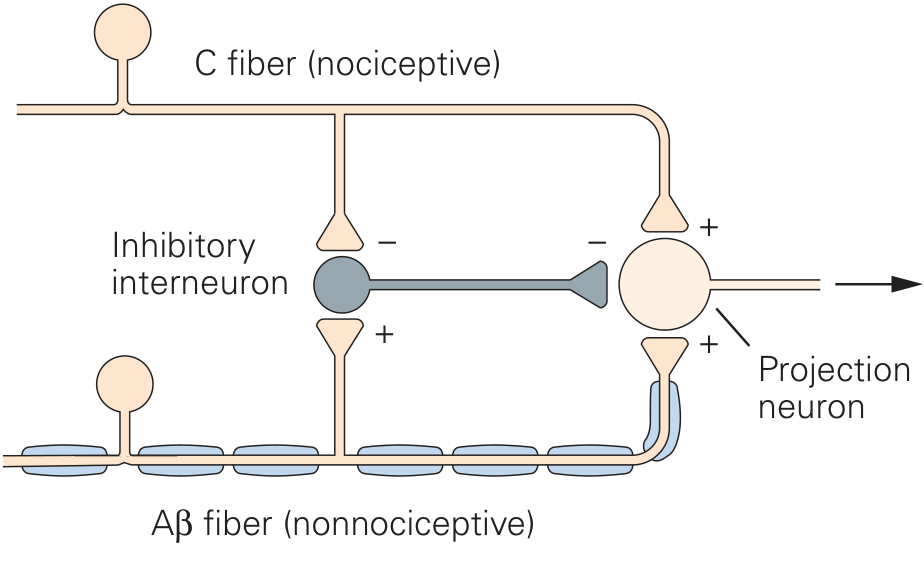
Figure: The gate control circuit. C fiber (nociceptive) activity inhibits the inhibitory interneuron (opening the gate). A-beta fiber activity excites the inhibitory interneuron (closing the gate), suppressing the projection neuron's output.
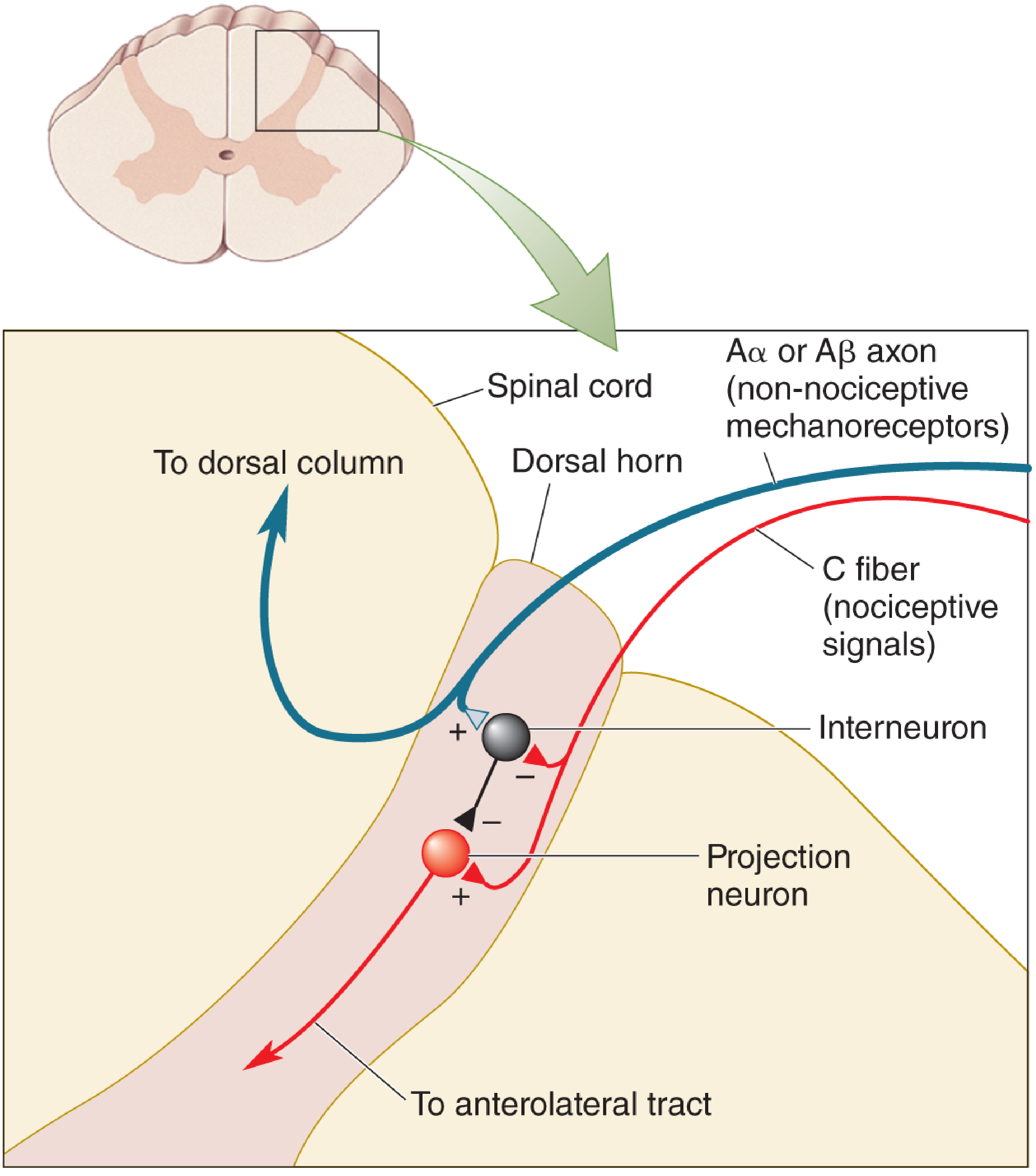
Figure: Spinal cord cross-section showing the dorsal horn gate. A-alpha/A-beta non-nociceptive inputs excite the inhibitory interneuron (+), which inhibits (-) the projection neuron. C-fiber nociceptive input activates the projection neuron (+) and inhibits (-) the interneuron, keeping the gate open.
How the Gate Works
Gate OPEN (pain felt):
- C fibers fire at high rates (injury, noxious stimulus)
- C fibers inhibit the inhibitory interneuron (disinhibition)
- Projection neuron fires freely → pain signal ascends to the brain
Gate CLOSED (pain reduced):
- A-beta fibers are active (rubbing, vibration, touch)
- A-beta fibers excite the inhibitory interneuron
- Inhibitory interneuron suppresses projection neuron firing → pain reduced
As Kandel's Principles of Neural Science explains: "The C fibers indirectly inhibit the interneurons, thus increasing the activity of the projection neurons (thereby 'opening the gate'), whereas the Aβ fibers excite the interneurons, thus suppressing the output of the projection neurons (and 'closing the gate')."
Neurochemistry of the Gate
Gate-like regulation arises from GABA-mediated and glycine-mediated inhibitory circuits in the spinal cord dorsal horn. The inhibitory interneurons use these transmitters to suppress projection neuron activity. - Medical Physiology, p. 575
Two Levels of Control
The original model focused only on the spinal gate, but we now recognize two control inputs:
- Afferent (peripheral) control - Activity in large vs. small fibers from the periphery
- Descending (central/supraspinal) control - The brain itself can modulate the gate via descending pathways (e.g., periaqueductal gray, raphe nuclei, locus coeruleus releasing serotonin and norepinephrine). This explains why emotional state, attention, and stress alter pain perception.
Why It Matters Clinically
The gate control theory directly explains and underpins several therapies:
| Therapy | Mechanism |
|---|---|
| Rubbing an injury | Activates A-beta mechanoreceptors - closes the gate |
| TENS (Transcutaneous Electrical Nerve Stimulation) | Electrically activates large-diameter A-beta fibers to suppress nociceptive C-fiber transmission |
| Spinal Cord Stimulation (SCS) | Delivers electrical stimulation to dorsal columns, activating large fibers and gating pain at multiple spinal levels |
| Opioids | Act on opioid receptors in the dorsal horn (and supraspinally), reducing projection neuron output |
| CBT / distraction | Engage descending inhibitory pathways (supraspinal gate) |
As stated in Barash's Clinical Anesthesia: "The analgesic effect of SCS may involve the gate control theory, neurotransmitter modulation in the spinal cord affecting pain pathways, and suppression of sympathetic activity."
Limitations and Modern Updates
The original 1965 model has been refined substantially:
- Gate interactions also occur at supraspinal relay centers, not just the dorsal horn - Kandel, Principles of Neural Science, 6th ed.
- The theory did not fully account for central sensitization (wind-up via NMDA receptor activation, long-term potentiation at dorsal horn synapses), which underlies chronic pain states
- Wide dynamic range (WDR) neurons are now known to be more complex than the original T-cell concept
- Psychological and cognitive factors (attention, expectation, catastrophizing) powerfully modulate pain via descending systems - this was underweighted in the original model
- Despite revisions, the fundamental idea - "that pain-inducing signals are regulated by the balance of activity in convergent large and small sets of sensory axons has stood the tests of time" - Neuroscience: Exploring the Brain, 5th ed.
Summary mnemonic: Think of the gate as a seesaw in the dorsal horn:
- Small fibers (C, A-delta) tip it toward PAIN (gate open)
- Large fibers (A-beta) tip it toward NO PAIN (gate closed)
- The brain can also push the seesaw from above (descending modulation)
This is a shared conversation. Sign in to Orris to start your own chat.