Health education on geriatrics
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Searching PubMed
"falls"[MeSH Terms] AND "aged"[MeSH Terms] AND "prevention"[MeSH Terms]
Searching the Web
geriatric falls risk factors prevention guidelines 2024 2025 healthcare students
Finding Sources
Searching PubMed
"accidental falls"[MeSH Terms] AND "aged"[MeSH Terms]
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have rich material from the textbooks. Let me compile a comprehensive health education resource on falls and fall prevention in the elderly for healthcare students.
Health Education in Geriatrics: Falls & Fall Prevention
For Healthcare Students/Trainees | Sources: Textbook of Family Medicine 9e, Goldman-Cecil Medicine, and current clinical guidelines
1. Why Falls Matter - Epidemiology
Falls are one of the most consequential geriatric syndromes, and understanding their scope is the first step in clinical care:
- ~30% of adults over 65 fall at least once per year; incidence rises with age
- Up to 10% of falls result in serious injury (hip fractures, head trauma, lacerations)
- Falls are the leading cause of injury-related deaths in people over 65
- Hip fractures account for >300,000 hospitalizations per year in the US, with a 1-year mortality rate of up to 33%
- Direct medical costs exceed $19 billion annually (in the US alone)
- By 2050, worldwide hip fractures are projected to rise to 6.26 million per year
Falls also cause harm beyond physical injury: post-fall anxiety leads to loss of self-confidence, social isolation, depression, and further deconditioning - creating a vicious cycle that increases future fall risk.
- Textbook of Family Medicine 9e, p. 62
2. Risk Factors - Intrinsic vs. Extrinsic
The risk of falling is multiplicative with multiple risk factors. A patient with 1 risk factor has a ~19% annual fall risk; with 3 or more risk factors, the risk jumps to ~60%.
Intrinsic Risk Factors (Patient-Related)
| Category | Examples |
|---|---|
| Age-related physiology | Reduced proprioception, slower reflexes, sarcopenia, kyphosis |
| Sensory deficits | Visual impairment, hearing loss, peripheral neuropathy |
| Cardiovascular | Orthostatic hypotension (up to 30% of older adults), arrhythmias, aortic stenosis |
| Neurological | Cognitive impairment, Parkinson's disease, stroke, cerebellar dysfunction |
| Musculoskeletal | Arthritis, muscle weakness, foot deformities, gait abnormalities |
| Psychiatric | Depression, anxiety, poor judgment |
| Metabolic | Diabetes (neuropathy, hypoglycemia), anemia, dehydration |
Extrinsic Risk Factors (Environmental & Medication-Related)
Medications (high-risk classes):
- Benzodiazepines and sedative-hypnotics
- Tricyclic antidepressants and SSRIs
- Antihypertensives and diuretics
- Neuroleptics/antipsychotics
- Narcotic analgesics
- Antihistamines and anticonvulsants
- Class 1A antiarrhythmics
Key point: Taking 4 or more prescription drugs is itself an independent risk factor for falls.
Environmental hazards:
- Loose rugs, poor lighting, slippery floors
- Stairs without handrails
- Poorly fitting shoes or footwear
- Uneven pavements, low toilet seats, no grab bars
- Textbook of Family Medicine 9e, p. 62-63; Goldman-Cecil Medicine
3. Screening - Who Needs Assessment?
All older adults should be asked at least once yearly about falls (SOR: C).
Three Key Screening Questions (AGS/BGS Guidelines):
- Two or more falls in the prior 12 months?
- Presents with an acute fall?
- Difficulty with walking or balance?
The two strongest predictors of future falls are: (1) a history of previous falls, and (2) a reported abnormality in gait or balance.
4. Clinical Assessment - The Falls Workup
For any patient with a positive screen, perform a structured multifactorial assessment:
History
- Circumstances of fall(s): activity, time of day, symptoms beforehand
- Medication review (complete list including OTC and supplements)
- Medical history: cardiac, neurologic, musculoskeletal, psychiatric conditions
- Functional status and ADLs
- Home environment assessment
Physical Examination
| Component | What to Assess |
|---|---|
| Postural blood pressure & pulse | Orthostatic hypotension (drop ≥20 mmHg systolic on standing) |
| Musculoskeletal | ROM in legs, arthritis, foot abnormalities, kyphosis |
| Neurological | Proprioception, coordination, muscle strength, cognition |
| Cardiovascular | Arrhythmias, murmurs (aortic stenosis) |
| Sensory | Visual acuity, hearing |
| Gait & Balance | Timed Up and Go (TUG) test |
The "Get Up and Go" Test (TUG)
A quick, validated office-based assessment of mobility:
- Patient stands from a seated chair, walks ~10 feet (3 m), turns around, walks back, sits down
- Normal: completed within 10 seconds
- Watch for: pushing off chair to rise (weak legs), shuffling gait, poor step height, decreased stride length, wide-based stance, slow multi-point turning
- Textbook of Family Medicine 9e, p. 63; Cummings Otolaryngology
Investigations (when clinically indicated)
- Labs: CBC, BMP, glucose (if metabolic cause suspected)
- Cardiac: Holter monitor or event monitor if syncope suspected; echo if murmur present
- Neuroimaging (MRI/CT): Only if focal neurological signs are present
5. The Falls Prevention Guideline - A Clinical Algorithm
The American Geriatrics Society (AGS) / British Geriatrics Society (BGS) guideline provides a structured approach:
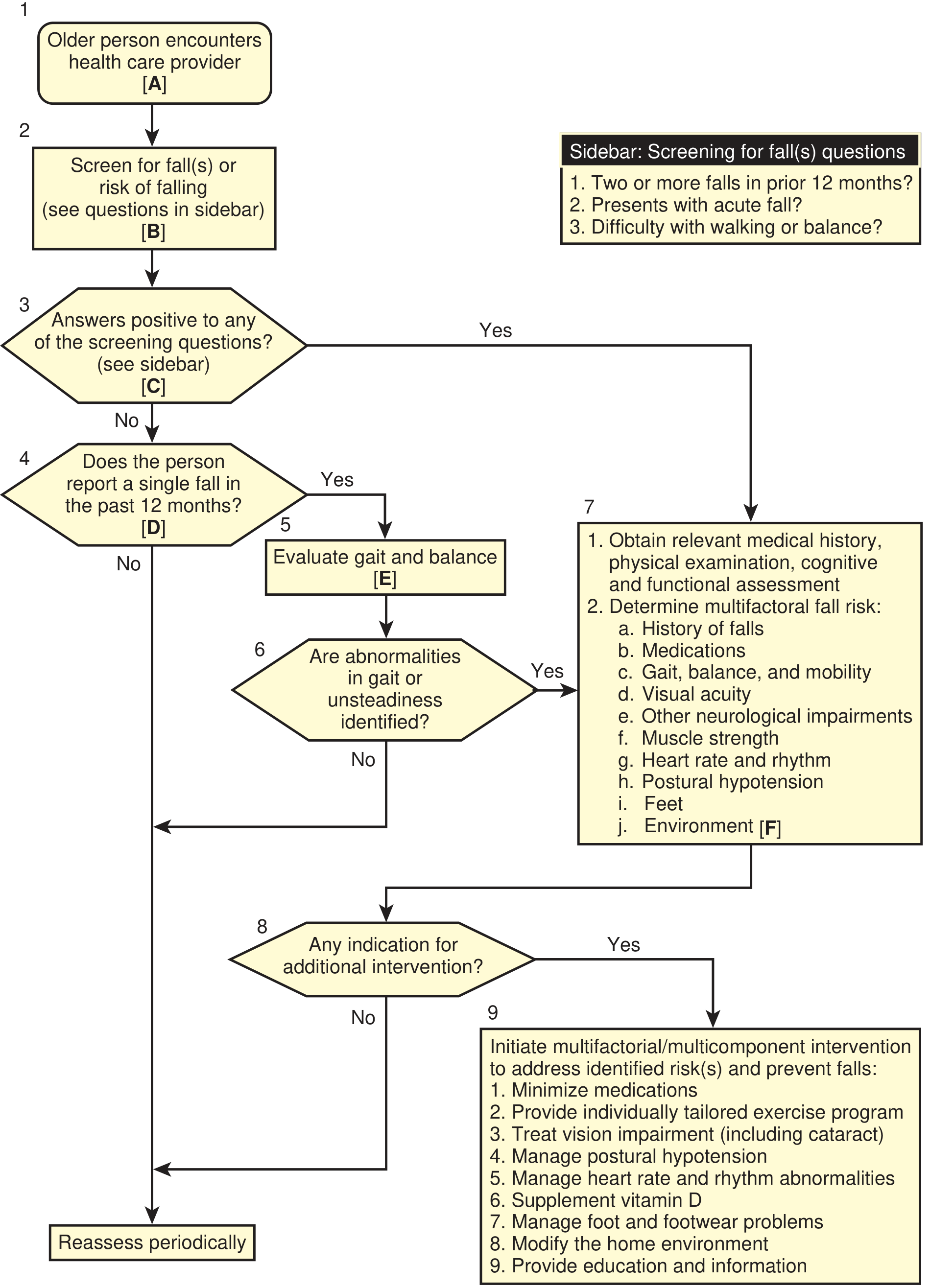
Figure: Practice guideline for the prevention of falls in older persons - AGS/BGS Panel on Falls Prevention
6. Management - Multifactorial Interventions
Evidence consistently shows a multifactorial approach is most effective - no single intervention alone is sufficient (SOR: A).
A. Medication Review (First Priority)
- Reduce the total number of medications when possible
- Taper or discontinue sedating drugs (benzodiazepines, sleep aids, opioids)
- Adjust antihypertensives/diuretics if orthostatic hypotension is present
- Review each medication's fall-risk profile
B. Exercise Programs (Strongest Evidence)
- Programs targeting at least 2 of 3 components for a minimum of 12 weeks show the most benefit (SOR: A):
- Strengthening (resistance training)
- Balance training (Tai Chi is particularly effective)
- Aerobic/endurance training
- The 2025 APTA Geriatrics Clinical Practice Guideline gives multicomponent exercise a strong recommendation (Level I evidence) as the most important intervention
C. Environmental Modification
- Home safety assessment by an occupational therapist (SOR: A for community-dwelling elderly)
- Install grab bars in bathrooms, handrails on stairs
- Remove loose rugs and clutter
- Improve lighting
- Encourage appropriate footwear
D. Sensory Corrections
- Treat vision impairment (including cataracts)
- Hearing aids where applicable
- Correct peripheral neuropathy causes where possible
E. Manage Specific Conditions
- Treat orthostatic hypotension
- Manage cardiac arrhythmias
- Manage foot and footwear problems
- Manage Parkinson's disease, osteoporosis, and other contributing conditions
F. Vitamin D
- Routine vitamin D supplementation to reduce falls has inconclusive evidence and recent trials show no benefit in vitamin D-replete individuals
- Still recommended if the patient has osteopenia or osteoporosis, or documented vitamin D deficiency
G. Physical Restraints - Do NOT Use
- Physical restraints do not reduce fall risk and are associated with increased injury risk - their use has been appropriately and dramatically reduced since the 1980s
- Textbook of Family Medicine 9e, p. 64; Goldman-Cecil Medicine; World Falls Guidelines 2022
7. Post-Fall Syndrome - The Psychological Dimension
A point often overlooked in clinical training:
- Post-fall anxiety syndrome develops in many elderly patients after a fall - even without injury
- Patients restrict their own activity out of fear of falling again
- This leads to: deconditioning → muscle weakness → worse balance → increased fall risk
- Can progress to depression and social isolation
- Management includes psychological support, graded return to activity, and balance retraining
8. Key Clinical Pearls for Students
| Point | Clinical Takeaway |
|---|---|
| Ask every year | "Have you had any falls in the past year?" at every annual visit |
| Falls = frailty marker | A fall is never "just a fall" - it signals underlying vulnerability |
| Medication is the most modifiable risk | Always reconcile the medication list |
| No single intervention works alone | Always use multifactorial, multicomponent strategies |
| Don't restrain | Physical restraints increase, not decrease, injury risk |
| Fear of falling is itself dangerous | Address psychological consequences proactively |
| Exercise is the strongest intervention | Balance + strength training, minimum 12 weeks |
| Home hazards matter | Environmental assessment by OT is Grade A evidence |
9. Recent Evidence Update (PubMed, 2023-2026)
A 2026 systematic review and meta-analysis (PMID: 41318106) identified that older adults with diabetes have significantly elevated fall prevalence and distinct risk factors (neuropathy, hypoglycemia, vision impairment), warranting targeted fall screening in this population.
A 2026 review of age-friendly geriatric assessment (PMID: 41544278) reinforces that falls screening should be embedded in every geriatric encounter as part of a standardized "4Ms" framework (What Matters, Medication, Mentation, Mobility).
Summary Table: Falls in the Elderly
| Domain | Key Content |
|---|---|
| Incidence | 30% of adults >65 fall annually |
| Serious injury | ~10% of falls |
| Leading cause of | Injury-related death in >65s |
| Strongest predictors | History of fall + gait/balance abnormality |
| Top modifiable risk | Polypharmacy (especially sedatives, antihypertensives) |
| Best assessment tool | Timed Up and Go (TUG) test |
| Most effective intervention | Multicomponent exercise (balance + strength, ≥12 weeks) |
| Environmental intervention | OT home assessment (Grade A) |
| What NOT to do | Physical restraints |
| Screen frequency | At least once yearly for all patients >65 |
This is a shared conversation. Sign in to Orris to start your own chat.