I am intern doctor, please show list of all dermatology and venereology illnesses along with clinical pictures and also mention their classification, management, diagnosis, laboratory analysis and treatment
dermatology venereology complete list of diseases classification diagnosis treatment 2024
dermatology skin diseases clinical pictures atlas
psoriasis eczema acne rosacea clinical photos dermatology
syphilis gonorrhea STI sexually transmitted infection clinical pictures venereology
melanoma basal cell carcinoma squamous cell carcinoma skin cancer
tinea fungal infection dermatophyte ringworm athlete foot clinical
urticaria herpes zoster chickenpox viral skin infection scabies lice
vitiligo alopecia hair loss nail disorders pemphigus bullous dermatitis
Dermatology & Venereology: Complete Clinical Reference for Intern Doctors
CLASSIFICATION FRAMEWORK
- Inflammatory (infectious / non-infectious)
- Neoplastic (benign / malignant)
PART I — INFLAMMATORY DERMATOSES (Non-infectious)
1. ECZEMA / ATOPIC DERMATITIS
- Atopic dermatitis (endogenous)
- Contact dermatitis: Allergic vs Irritant
- Seborrhoeic dermatitis
- Discoid (nummular) eczema
- Dyshidrotic eczema (pompholyx)
- Stasis/gravitational eczema
- Pruritus, erythema, papules, vesicles, lichenification
- Distribution: flexural creases (antecubital, popliteal) in atopic; coin-shaped plaques in nummular; greasy scales on scalp/nasolabial folds in seborrhoeic

- Clinical (Hanifin-Rajka criteria for atopic dermatitis)
- Patch testing for allergic contact dermatitis
- Serum IgE elevated (atopic)
- Eosinophilia
- RAST/specific IgE for allergens
- KOH prep to exclude tinea (especially in hand eczema)
- Trigger avoidance, emollients (cornerstone)
- Topical corticosteroids (mild-to-moderate: hydrocortisone 1%; moderate-to-potent: betamethasone valerate, mometasone)
- Topical calcineurin inhibitors: tacrolimus 0.03–0.1%, pimecrolimus (steroid-sparing)
- Antihistamines (sedating: chlorphenamine; non-sedating: cetirizine) for itch
- Severe/refractory: dupilumab (anti-IL-4Rα), ciclosporin, methotrexate, azathioprine
- Seborrhoeic: antifungal shampoos/creams (ketoconazole 2%), low-potency steroids
2. PSORIASIS
- Plaque psoriasis (psoriasis vulgaris) — 80–90%
- Guttate psoriasis
- Pustular psoriasis (generalised/palmoplantar)
- Erythrodermic psoriasis
- Inverse (flexural) psoriasis
- Nail psoriasis
- Psoriatic arthritis
- Well-demarcated, salmon-pink plaques with silvery-white scale
- Auspitz sign (pinpoint bleeding on scale removal)
- Koebner phenomenon
- Nail: pitting, onycholysis, oil-drop sign

- Clinical; biopsy if uncertain
- Psoriasis Area Severity Index (PASI), Dermatology Life Quality Index (DLQI)
- Skin biopsy: parakeratosis, Munro microabscesses, acanthosis, elongated rete ridges
- ASO titre (guttate — streptococcal trigger)
- HLA-Cw6 association
- Metabolic screen (psoriasis associates with metabolic syndrome, CVD)
| Severity | Treatment |
|---|---|
| Mild | Topical corticosteroids, vitamin D analogues (calcipotriol), combination (Daivobet) |
| Moderate | Phototherapy: NB-UVB, PUVA |
| Severe | Methotrexate, ciclosporin, acitretin; Biologics: TNF-α inhibitors (etanercept, adalimumab, infliximab), IL-17 inhibitors (secukinumab, ixekizumab), IL-23 inhibitors (guselkumab, risankizumab) |
3. ACNE VULGARIS
- Comedonal (non-inflammatory)
- Inflammatory: papulopustular
- Nodulocystic/conglobate (severe)
- Acne fulminans (most severe)
- Acne rosacea (separate entity — see below)
- Comedones (open=blackheads, closed=whiteheads), papules, pustules, nodules, cysts
- Face, chest, upper back
- Post-inflammatory hyperpigmentation, scarring
- Clinical; grading by IGA (Investigator Global Assessment) or Leeds scale
- Androgen profile (if features of PCOS/virilisation)
- Bacterial culture if resistant (rule out Gram-negative folliculitis)
- If on isotretinoin: LFTs, fasting lipids, FBC, urine pregnancy test
| Grade | Treatment |
|---|---|
| Mild | Benzoyl peroxide, topical retinoids (adapalene, tretinoin), topical antibiotics (clindamycin) |
| Moderate | Oral antibiotics: doxycycline 100 mg OD (first-line), lymecycline |
| Severe | Oral isotretinoin 0.5–1 mg/kg/day (highly teratogenic — contraception mandatory); spironolactone (females) |
| Hormonal | Combined OCP (e.g. co-cyprindiol/Dianette) |
4. ROSACEA
- I: Erythematotelangiectatic (ETR)
- II: Papulopustular
- III: Phymatous (rhinophyma — sebaceous hyperplasia)
- IV: Ocular rosacea
- Central facial erythema, flushing, telangiectasias
- Papules/pustules without comedones (distinguishes from acne)
- Triggers: sun, heat, spicy food, alcohol, stress


- Clinical (National Rosacea Society diagnostic criteria)
- Demodex folliculorum overcolonisation may be relevant
- Dermoscopy: branching telangiectasias, follicular plugging
- Skin biopsy if uncertain
- Sun protection (SPF 50+), avoid triggers
- Topical: metronidazole 0.75%, azelaic acid 15–20%, ivermectin 1% cream (anti-Demodex)
- Oral: doxycycline 40 mg modified-release (low-dose anti-inflammatory, not antibiotic dose)
- Vascular lasers/IPL for telangiectasias
- Rhinophyma: CO₂ laser, surgical debulking
5. URTICARIA (HIVES)
- Acute (<6 weeks): usually allergic/infective
- Chronic (>6 weeks): spontaneous (CSU) or inducible (dermographism, cold, cholinergic, solar, pressure)
- Urticarial vasculitis
- Transient wheals (pruritic, oedematous, centrifugal spread) lasting <24 h
- Angioedema: deep dermal/subcutaneous swelling
- Clinical; trigger identification
- FBC, ESR, CRP, LFTs, TFTs, ANA, complement (C3/C4)
- Chronic: autologous serum skin test (ASST), anti-FcεRI/anti-IgE antibodies
- Inducible: cold stimulation test, dermographometer
- Acute: antihistamines (cetirizine, loratadine); severe/anaphylaxis: IM adrenaline 0.5 mg (1:1000)
- Chronic spontaneous urticaria:
- Step 1: Non-sedating H1-antihistamine (cetirizine 10 mg OD)
- Step 2: Up to 4× licensed dose
- Step 3: Add omalizumab (anti-IgE, 300 mg SC every 4 weeks) — highly effective
- Step 4: Ciclosporin
PART II — BULLOUS (BLISTERING) DISEASES
6. PEMPHIGUS VULGARIS
- Pemphigus vulgaris (most common, life-threatening)
- Pemphigus foliaceus
- Paraneoplastic pemphigus
- IgA pemphigus
- Fragile, flaccid blisters → painful erosions
- Oral mucosa often first affected (50–70%)
- Nikolsky sign positive (skin slips with lateral pressure)
- Asboe-Hansen sign positive

- Skin biopsy: intraepidermal acantholysis (suprabasal split)
- Direct immunofluorescence (DIF): intercellular IgG/C3 "chicken-wire" pattern
- Indirect IF: anti-desmoglein (Dsg3 > Dsg1) antibodies
- ELISA: anti-Dsg3, anti-Dsg1
- Anti-Dsg3 ELISA (mucosal disease), anti-Dsg1 (skin disease)
- Baseline FBC, LFTs, U&E, glucose (before immunosuppression)
- High-dose systemic prednisolone 1 mg/kg/day initially
- Steroid-sparing agents: azathioprine, mycophenolate mofetil
- Rituximab (anti-CD20): now first-line in moderate-to-severe disease
- Wound care for erosions; IVIG in refractory cases
7. BULLOUS PEMPHIGOID
- Bullous pemphigoid (most common autoimmune blistering disease in elderly)
- Mucous membrane pemphigoid
- Pemphigoid gestationis (pregnancy)
- Lichen planus pemphigoides
- Tense bullae on urticarial/erythematous base
- Elderly patients (>70 years); trunk, flexures
- Pruritus often precedes blistering
- Nikolsky sign negative
- Biopsy: subepidermal blister, eosinophil-rich infiltrate
- DIF: linear IgG/C3 at dermoepidermal junction (DEJ)
- Anti-BP180 (BPAG2), anti-BP230 antibodies by ELISA
- Potent topical corticosteroids (clobetasol propionate 0.05%) — preferred over systemic
- Oral prednisolone (0.5 mg/kg/day) for extensive disease
- Doxycycline + niacinamide (milder disease)
- Azathioprine, methotrexate, mycophenolate as steroid-sparing
PART III — PAPULOSQUAMOUS DISORDERS
8. LICHEN PLANUS
- Cutaneous LP
- Oral LP (reticular, erosive, bullous)
- Genital LP
- Lichen planopilaris (scarring alopecia)
- Nail LP
- LP pigmentosus
- 4 P's: Pruritic, Purple, Polygonal, Papules
- Wickham's striae (lacy white lines on surface)
- Koebner phenomenon
- Wrists, forearms, ankles, mucous membranes
- Clinical; biopsy if uncertain
- Skin biopsy: band-like lichenoid infiltrate at DEJ, basal cell damage, colloid bodies (Civatte bodies)
- Hepatitis C serology (associated in some populations)
- Oral LP: exclude lichenoid drug reaction (check medication history)
- Topical corticosteroids (moderate to potent)
- Oral: prednisolone for severe/widespread; acitretin
- Topical tacrolimus (oral LP)
- Phototherapy (NB-UVB, PUVA)
9. PITYRIASIS ROSEA
- Herald patch (2–5 cm oval scaly plaque) → generalized eruption 1–2 weeks later
- "Christmas tree" distribution on trunk
- Self-limiting (6–8 weeks)
- HHV-6/7 association
- Reassurance; topical emollients
- Antihistamines for itch
- Aciclovir (early use may shorten duration)
- NB-UVB (second line)
PART IV — INFECTIOUS DERMATOSES
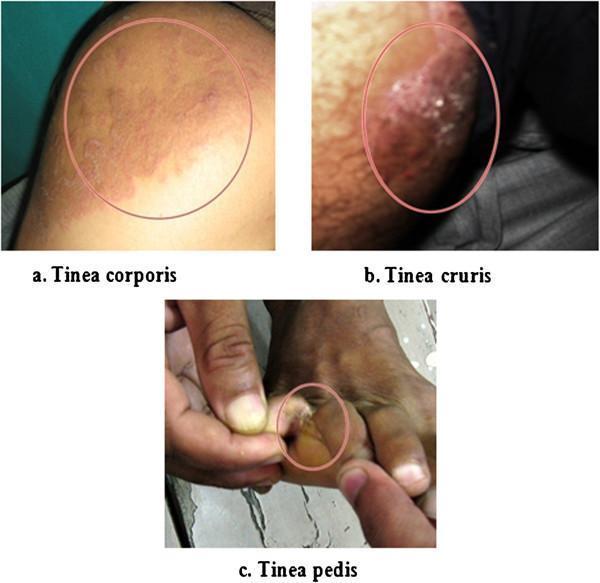
10. FUNGAL INFECTIONS (DERMATOPHYTOSES)
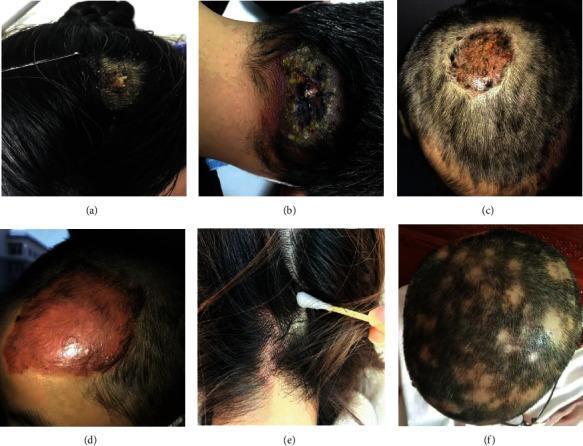
- Tinea capitis (scalp)
- Tinea corporis (body/ringworm)
- Tinea cruris (groin — "jock itch")
- Tinea pedis (foot — "athlete's foot")
- Tinea unguium/Onychomycosis (nails)
- Tinea versicolor/pityriasis versicolor (Malassezia — not a dermatophyte)
- Cutaneous candidiasis
- Annular, scaly plaques with active advancing edge and central clearing
- Tinea pedis: interdigital maceration, scaling, fissuring
- Onychomycosis: nail thickening, yellowing, subungual debris

- KOH microscopy: septate hyphae (dermatophytes), pseudohyphae (Candida), spaghetti and meatballs (Malassezia)
- Wood's lamp: Microsporum → green fluorescence; Pityrosporum → yellow-green
- Fungal culture on Sabouraud's dextrose agar
- Skin scrapings, nail clippings, or hair stubs for KOH/culture
- PCR (increasingly used for species identification)
- Tinea corporis/cruris/pedis: topical terbinafine 1%, clotrimazole 1% (4 weeks)
- Tinea capitis (requires oral): griseofulvin 10–20 mg/kg/day × 6–8 wk; terbinafine 125–250 mg/day × 4 wk
- Onychomycosis: oral terbinafine 250 mg/day × 12 wk (fingernails 6 wk) or itraconazole pulse
- Pityriasis versicolor: selenium sulphide shampoo, topical azoles; oral itraconazole/fluconazole for extensive disease
11. BACTERIAL SKIN INFECTIONS
- Impetigo (Staph. aureus / Group A Strep)
- Ecthyma (deep impetigo)
- Erysipelas (Group A Strep, dermis/superficial)
- Cellulitis (deep dermis/subcutaneous)
- Folliculitis, furuncle (boil), carbuncle
- Hidradenitis suppurativa (apocrine)
- Erythrasma (Corynebacterium minutissimum)
- Impetigo: golden-crusted lesions, honey-coloured exudate, perioral/nasal
- Erysipelas: bright red, sharply demarcated, raised plaque; fever/systemic upset
- Cellulitis: poorly defined erythema, warmth, tenderness, fever
- Swabs for MCS; blood cultures if systemic sepsis
- Erythrasma: coral-red fluorescence under Wood's lamp
- FBC (neutrophilia), CRP/ESR, blood cultures
- ASO titre (streptococcal)
- MRSA swab if risk factors
- Impetigo: topical mupirocin 2% or fusidic acid; oral flucloxacillin/cefalexin if widespread
- Erysipelas/cellulitis: IV benzylpenicillin + flucloxacillin (or IV co-amoxiclav); MRSA — vancomycin/daptomycin
- Folliculitis: topical antiseptics; recurrent — oral antibiotics, decolonisation
- Hidradenitis suppurativa:
- Hurley I: topical clindamycin, antiseptics
- Hurley II-III: oral tetracyclines, rifampicin + clindamycin
- Biologic: adalimumab (only licensed biologic for HS), secukinumab
- Surgery: wide local excision

12. VIRAL SKIN INFECTIONS
- Pruritic vesicular exanthem in crops ("dewdrop on a rose petal")
- Centripetal distribution; lesions at different stages simultaneously
- Fever, malaise

- Dermatomal pain/burning → unilateral vesicular eruption
- Thoracic > trigeminal distribution
- Ramsay Hunt syndrome (geniculate ganglion: ear vesicles + facial palsy + hearing loss)
- Post-herpetic neuralgia (PHN) — major complication
- Grouped vesicles on erythematous base; lips (orolabial) or genitalia
- Primary vs recurrent
- Eczema herpeticum (Kaposi's varicelliform eruption) in atopic patients
- Skin-coloured, umbilicated dome-shaped papules 2–5 mm
- Children (trunk), adults (genital area in sexually active)
- Self-limiting; HIV: extensive/giant lesions

- Common warts (verruca vulgaris): rough, papillomatous, any site
- Plantar warts (verruca plantaris): endophytic, painful
- Flat warts (verruca plana): flat-topped papules, face/limbs
- Genital warts (condylomata acuminata): HPV 6, 11
13. PARASITIC INFESTATIONS
- Intense nocturnal pruritus
- Burrows (pathognomonic) in finger webs, wrists, genitalia
- Widespread papular eruption; secondary eczematisation
- Crusted scabies: thick hyperkeratotic plaques, mild itch but highly contagious
- Clinical + dermoscopy ("delta-wing jet with contrail" sign of mite)
- Skin scraping + microscopy (mites, eggs, faecal pellets)
- Permethrin 5% cream: whole body (neck down), leave 8–12 h, repeat 1 week
- Alternative: malathion 0.5%, benzyl benzoate 25%
- Oral ivermectin 200 µg/kg × 2 doses (crusted scabies — first-line; classical — second-line)
- Treat all household contacts simultaneously; wash clothing/bedding at 60°C
- Antihistamines + topical steroids for post-scabetic itch
- Pediculus humanus capitis (head lice): nits (egg cases) on hair shafts, pruritic scalp
- Pediculus humanus corporis (body lice): vector for typhus, trench fever, relapsing fever
- Phthirus pubis (pubic/crab lice): STI
PART V — PIGMENTARY DISORDERS
14. VITILIGO
- Segmental (unilateral, dermatomal)
- Non-segmental/generalised: vitiligo vulgaris, acrofacial, universal
- Well-demarcated depigmented macules/patches
- Wood's lamp: chalk-white fluorescence
- Association with autoimmune conditions (thyroid disease, T1DM, Addison's, pernicious anaemia)

- Clinical; Wood's lamp examination
- Autoantibody screen: anti-thyroid, anti-nuclear, ANA
- TFTs + anti-TPO, anti-thyroglobulin antibodies
- Fasting glucose/HbA1c
- FBC (pernicious anaemia screen)
- Topical corticosteroids (class III), topical calcineurin inhibitors
- NB-UVB phototherapy (best evidence for repigmentation)
- Excimer laser
- Oral/topical ruxolitinib (JAK 1/2 inhibitor — approved 2022)
- Surgical (melanocyte transfer, split-thickness skin grafts) for stable segmental vitiligo
- Sunscreen to protect depigmented areas
15. MELASMA
PART VI — HAIR & NAIL DISORDERS
16. ALOPECIA
| Type | Cause | Scarring? |
|---|---|---|
| Androgenetic alopecia | DHT-mediated, genetic | No |
| Alopecia areata (AA) | Autoimmune | No |
| Tinea capitis | Dermatophyte | No (kerion can scar) |
| Lichen planopilaris | Lichen planus | Yes |
| Discoid lupus | Autoimmune | Yes |
| Traction/traumatic | Physical | No (can become scarring) |

- Clinical (smooth, non-scarring patches; exclamation mark hairs at periphery)
- Dermoscopy: yellow dots, black dots, broken hairs
- Scalp biopsy if uncertain (peribulbar lymphocytic infiltrate — "swarm of bees")
- TFTs, FBC, ferritin, serum zinc
- Intralesional triamcinolone acetonide 5–10 mg/mL (patches)
- Topical minoxidil 5%, topical DPCP immunotherapy
- Oral JAK inhibitors: baricitinib, ritlecitinib (approved for severe AA)
- Systemic steroids for rapidly progressive disease
- Topical minoxidil 2–5% (men and women)
- Oral finasteride 1 mg/day (men only — blocks 5α-reductase); dutasteride
- Hair transplant (FUE/FUT)
PART VII — SKIN TUMOURS & NEOPLASMS
17. MELANOMA
- Superficial spreading melanoma (SSM) — most common, 70%
- Nodular melanoma (most aggressive)
- Lentigo maligna melanoma (sun-damaged skin, elderly)
- Acral lentiginous melanoma (palms, soles, nails — commonest in darker skin)
- Amelanotic melanoma
- Asymmetry
- Border irregularity
- Colour variegation (tan, brown, black, red, white, blue)
- Diameter >6 mm
- Evolution (change over time)

- Dermoscopy (increase diagnostic accuracy by 30%)
- Excision biopsy (do not incise or shave)
- Sentinel lymph node biopsy for Breslow >0.8 mm or ulceration
- Histopathology with Breslow thickness (depth in mm), Clark level, ulceration, mitotic rate
- BRAF V600E mutation testing (present in ~50% — guides targeted therapy)
- Staging CT (chest, abdomen, pelvis), MRI brain
- LDH (elevated in metastatic disease — poor prognosis)
- Wide local excision (margins determined by Breslow thickness: 0–1 mm → 1 cm margin; 1–2 mm → 1–2 cm; >2 mm → 2 cm)
- Immunotherapy: pembrolizumab, nivolumab (anti-PD-1)
- Targeted therapy: BRAF inhibitors (vemurafenib, dabrafenib) + MEK inhibitors (trametinib, cobimetinib)
- Radiation for unresectable/metastatic
18. BASAL CELL CARCINOMA (BCC)
- Nodular (most common): pearly papule/nodule with rolled border and telangiectasias
- Superficial: erythematous scaly plaque (multiple lesions)
- Morphoeic/infiltrative: scar-like, ill-defined (most aggressive local growth)
- Pigmented BCC
- Basosquamous
- Clinical + dermoscopy (arborising telangiectasias, blue-grey ovoid nests)
- Punch/shave biopsy
- Histopathology: basaloid nests with peripheral palisading and retraction artefact
- Surgical excision (gold standard): 3–5 mm margins
- Mohs micrographic surgery: highest cure rates for high-risk/facial BCC
- Cryotherapy (superficial, small)
- Topical imiquimod 5%/PDT (superficial BCC)
- Curettage and cautery
- Advanced/inoperable: vismodegib (Hedgehog pathway inhibitor), sonidegib
19. SQUAMOUS CELL CARCINOMA (SCC)
- In situ (Bowen's disease — full-thickness epidermal dysplasia)
- Invasive SCC
- Verrucous carcinoma
- Keratoacanthoma (controversial — may be variant)
- Hyperkeratotic, indurated nodule with ulceration
- Actinic keratosis (AK) → SCC in situ (Bowen's) → invasive SCC (progression)
- High risk: immunosuppressed patients (organ transplant recipients)
- Histopathology: keratin pearls, disordered epidermal proliferation, dermal invasion
- Excision with 4–6 mm margins (standard); Mohs for high-risk sites
- Radiotherapy (adjuvant or inoperable)
- Cemiplimab (anti-PD-1) for advanced/metastatic SCC
- Actinic keratoses: topical 5-FU 5%, imiquimod 5%, diclofenac 3%, PDT, cryotherapy

20. OTHER BENIGN TUMOURS
| Lesion | Features | Treatment |
|---|---|---|
| Seborrhoeic keratosis | "Stuck-on" waxy papule; older adults | Cryotherapy, curettage |
| Dermatofibroma | Firm, tan/brown papule; legs; dimple sign | Excision if symptomatic |
| Epidermoid cyst | Punctum, cheesy contents | Excision |
| Lipoma | Soft, mobile, subcutaneous | Excision |
| Pyogenic granuloma | Rapidly growing red papule; bleeds easily | Curettage, excision |
| Haemangioma | Bright red vascular papule | Often involutes; propranolol for infantile |
| Keloid/hypertrophic scar | Excess collagen; extends beyond wound (keloid) | Intralesional triamcinolone, silicone, CO₂ laser |
PART VIII — AUTOIMMUNE/CONNECTIVE TISSUE DISEASES
21. LUPUS ERYTHEMATOSUS (Cutaneous)
- Discoid LE (DLE): chronic, scarring
- Subacute cutaneous LE (SCLE)
- Acute cutaneous LE (malar "butterfly" rash = SLE)
- Neonatal LE
- ANA, anti-dsDNA (SLE), anti-Ro/SSA, anti-La/SSB (SCLE)
- DIF (biopsy): lupus band (IgG, IgM, C3 at DEJ)
- Sunscreen (critical)
- Topical/intralesional steroids; hydroxychloroquine (mainstay for cutaneous LE, 200–400 mg/day)
- Severe SLE: systemic immunosuppression (azathioprine, mycophenolate, belimumab)
22. SYSTEMIC SCLEROSIS (SCLERODERMA)
- Skin thickening (sclerosis): fingers → hands → trunk
- Raynaud's phenomenon (often first sign)
- Telangiectasias, calcinosis, fingertip ulcers
- CREST syndrome: Calcinosis, Raynaud's, oEsophageal dysmotility, Sclerodactyly, Telangiectasias
- Anti-centromere antibody (limited), anti-topoisomerase I (anti-Scl-70) (diffuse)
PART IX — VENEREOLOGY (SEXUALLY TRANSMITTED INFECTIONS)
23. SYPHILIS (Treponema pallidum)
| Stage | Features |
|---|---|
| Primary | Painless, indurated genital ulcer (chancre); painless inguinal lymphadenopathy; heals spontaneously in 3–6 wk |
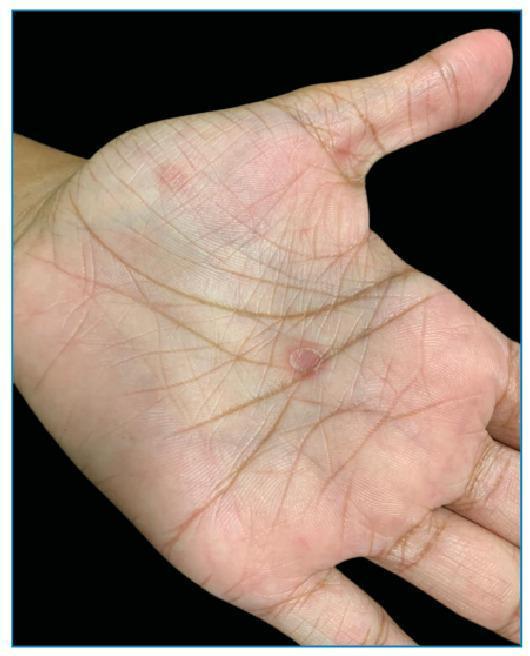
| Secondary | 4–8 wk after chancre: systemic illness, maculopapular rash (palms and soles — pathognomonic), condylomata lata, mucous patches, generalised lymphadenopathy, alopecia |
| Latent | Early (<1 yr) vs late (>1 yr): asymptomatic |
| Tertiary | Gummas (granulomatous), neurosyphilis, cardiovascular (aortitis) |
| Congenital | Early/late; Hutchinson's triad: interstitial keratitis, notched incisors, SNHL |

- Dark-field microscopy (primary chancre — gold standard for primary)
- Non-treponemal tests: VDRL, RPR (titre reflects disease activity; becomes negative with treatment)
- Treponemal tests: TPHA, FTA-ABS, TPPA, CLIA (remain positive for life — confirm diagnosis, cannot monitor treatment)
- PCR (chancre swab, CSF)
- Primary, secondary, early latent (<1 yr): Benzathine penicillin G 2.4 MU IM stat (single dose)
- Late latent/tertiary: Benzathine penicillin G 2.4 MU IM weekly × 3 doses
- Neurosyphilis: IV benzylpenicillin G 18–24 MU/day × 10–14 days
- Penicillin allergy: doxycycline 100 mg BD × 14 days (not congenital/neurosyphilis — desensitise)
- Jarisch-Herxheimer reaction: fever/chills/headache 2–8 h post-treatment; manage with paracetamol
24. GONORRHOEA (Neisseria gonorrhoeae)
- Males: urethral discharge (yellow-green, purulent), dysuria
- Females: often asymptomatic; cervicitis, pelvic inflammatory disease (PID)
- Pharyngeal, anorectal, ocular (neonatal ophthalmia)
- Disseminated gonococcal infection (DGI): arthritis-dermatitis syndrome — migratory polyarthralgia, tenosynovitis, pustular/haemorrhagic skin lesions
- NAAT (nucleic acid amplification test) — gold standard (urine, urethral/cervical/rectal/pharyngeal swab)
- Culture + sensitivity (essential before treatment if resistance suspected)
- Gram stain: intracellular Gram-negative diplococci (good sensitivity in males; poor in females)
- Uncomplicated: ceftriaxone 1 g IM single dose (IM is preferred; oral cefixime 400 mg no longer recommended due to resistance in many regions)
- Pharyngeal gonorrhoea: ceftriaxone 1 g IM (oral agents unreliable)
- PID: ceftriaxone + doxycycline + metronidazole
- Penicillinase-producing strains (PPNG): ceftriaxone remains effective; spectinomycin (alternate)
- Partner notification mandatory; test for concurrent STIs
25. CHLAMYDIA (Chlamydia trachomatis)
- Genital chlamydia (serovars D–K): most common bacterial STI
- Lymphogranuloma venereum (LGV, serovars L1–L3): invasive
- Trachoma (serovars A–C): eye disease (not STI in usual sense)
- Often asymptomatic; urethritis, mucopurulent cervicitis
- LGV: transient painless genital ulcer → painful inguinal buboes → ano-rectal syndrome (proctitis, strictures in MSM)

- NAAT (urine, self-taken vulvovaginal swab — most sensitive)
- LGV: NAAT with genotyping; serology (complement fixation titre >1:64)
- Uncomplicated genital chlamydia: doxycycline 100 mg BD × 7 days (first-line) or azithromycin 1 g stat
- LGV: doxycycline 100 mg BD × 21 days
- Pregnancy: azithromycin 1 g stat or amoxicillin 500 mg TDS × 7 days
26. GENITAL HERPES (HSV-1/HSV-2)
- Primary episode: painful grouped vesicles/ulcers on genitalia, perianal area; fever, inguinal lymphadenopathy, dysuria; more severe than recurrences
- Recurrences: shorter, less severe; prodrome of tingling/burning
- Neonatal herpes: vertical transmission (peripartum contact)
- PCR swab from lesion (gold standard)
- Viral culture; type-specific serology (HSV-2 IgG seroprevalence)
- First episode: aciclovir 400 mg TDS × 5 days or valaciclovir 1000 mg BD × 5 days
- Recurrent: aciclovir 800 mg TDS × 2 days or valaciclovir 500 mg BD × 3 days
- Suppressive therapy: aciclovir 400 mg BD (reduces recurrences and transmission)
27. HUMAN PAPILLOMAVIRUS (HPV) — ANOGENITAL WARTS
- Condylomata acuminata (soft, fleshy warts): HPV 6, 11 (low risk)
- Flat/papular warts: HPV 16, 18, 31, 33 (high-risk — associated with cervical/anal cancer)
- Bowenoid papulosis, Buschke-Löwenstein tumour (giant condyloma)
- Soft, flesh-coloured cauliflower-like papules in anogenital region
- Often asymptomatic; may itch or bleed
- Clinical; biopsy if uncertain or atypical
- Acetic acid 5% test (acetowhitening — not specific)
- Cervical cytology, colposcopy, anal cytology (high-risk patients)
- Patient-applied: imiquimod 5% cream × 16 wk; podophyllotoxin 0.5% solution/gel × 4 cycles
- Clinician-applied: cryotherapy, trichloroacetic acid 80–90% (TCA), electrosurgery, CO₂ laser
- HPV vaccination (Gardasil-9 — 9 strains): primary prevention (boys and girls 11–13 years)
28. TRICHOMONAS VAGINALIS
- Women: frothy yellow-green vaginal discharge, "strawberry cervix," pruritus vulvae, dysuria
- Men: often asymptomatic; urethritis
- NAAT (most sensitive)
- Wet mount microscopy: motile trichomonads (immediate; 60–70% sensitivity)
- Culture on Diamond's medium
- Metronidazole 2 g oral stat (or 400 mg BD × 5–7 days)
- Treat partners simultaneously; avoid alcohol during/48 h after metronidazole
29. CHANCROID (Haemophilus ducreyi)
- Painful genital ulcer (contrast with painless syphilis chancre)
- Ragged undermined edges; dirty grey/yellow necrotic base
- Tender inguinal lymphadenopathy (bubo) — may suppurate
- Clinical; culture on selective medium (low sensitivity)
- Exclusion of syphilis and herpes
- PCR (when available)
- Azithromycin 1 g stat, or ceftriaxone 250 mg IM stat
- Fluctuant buboes: aspiration or incision (prevent rupture)
30. HIV-RELATED DERMATOSES
| CD4 Count | Common Skin Manifestations |
|---|---|
| Any | Seborrhoeic dermatitis (severe), oral candidiasis, hairy leukoplakia |
| <200 | Kaposi's sarcoma, molluscum contagiosum (extensive/giant), herpes zoster (multidermatomal), chronic herpes simplex |
| <50 | Disseminated MAC, CMV retinitis (periorbital skin changes), bacillary angiomatosis |

SUMMARY: KEY LABORATORY INVESTIGATIONS IN DERMATOLOGY & VENEREOLOGY
| Test | Indication |
|---|---|
| KOH microscopy | Fungal infection |
| Tzanck smear | HSV/VZV (not specific) |
| Wood's lamp | Tinea, erythrasma, vitiligo, pityriasis versicolor |
| Patch test | Allergic contact dermatitis |
| Prick test/RAST | Urticaria, atopic dermatitis |
| Skin biopsy + H&E | Bullous diseases, tumours, inflammatory dermatoses |
| DIF | Pemphigus, bullous pemphigoid, DLE |
| Anti-Dsg1/3 ELISA | Pemphigus |
| Anti-BP180/BP230 | Bullous pemphigoid |
| ANA, anti-dsDNA | Lupus |
| RPR/VDRL + TPHA | Syphilis |
| NAAT | Gonorrhoea, chlamydia, herpes, trichomonas |
| Dark-field microscopy | Primary syphilis chancre |
| Wet mount | Trichomonas, Candida |
| FBC, CRP | Cellulitis, systemic infection |
| CD4 count/HIV VL | HIV-related dermatoses |
| BRAF mutation | Melanoma (targeted therapy selection) |
SUMMARY: COMMONLY USED DRUGS IN DERMATOLOGY
| Drug Class | Examples | Key Use |
|---|---|---|
| Topical corticosteroids | Hydrocortisone (mild), betamethasone, clobetasol (potent) | Eczema, psoriasis, lichen planus |
| Topical calcineurin inhibitors | Tacrolimus, pimecrolimus | Eczema (face), oral LP |
| Topical retinoids | Tretinoin, adapalene | Acne, photo-ageing |
| Systemic retinoids | Isotretinoin, acitretin | Severe acne, psoriasis |
| Antifungals | Terbinafine, itraconazole, fluconazole | Dermatophytoses |
| Antivirals | Aciclovir, valaciclovir, famciclovir | HSV, VZV |
| Biologics | Dupilumab (IL-4Rα), secukinumab (IL-17), adalimumab (TNF-α), omalizumab (IgE) | Severe eczema, psoriasis, urticaria, HS |
| JAK inhibitors | Baricitinib, ruxolitinib, ritlecitinib | Alopecia areata, vitiligo, atopic dermatitis |
| Penicillin | Benzathine pen G | Syphilis |
| Ceftriaxone | Ceftriaxone 1 g IM | Gonorrhoea |
| Doxycycline | 100 mg BD × 7 d | Chlamydia, LGV, rosacea |
| Metronidazole | 2 g stat | Trichomonas; topical for rosacea |
| Ivermectin | Oral 200 µg/kg | Scabies (crusted/systemic); topical 1% for rosacea |
I am disappointed as you haven't shown all list dermatology/ venereology illnesses
Generate a comprehensive dermatology diseases reference PDF
I am intern doctor, please show list of all dermatology and venereology illnesses along with clinical pictures and also mention their clinical classification, management, diagnosis, laboratory analysis and treatment
acne vulgaris comedones papules pustules nodules face
psoriasis plaque silvery scales erythematous Auspitz sign elbows knees
eczema atopic dermatitis flexural lichenification itching child adult
herpes zoster shingles dermatomal vesicular rash unilateral
urticaria wheals angioedema hives skin swelling
scabies burrows interdigital web spaces prurigo nodularis
melanoma ABCDE asymmetry border color diameter evolution pigmented lesion
contact dermatitis allergic patch test erythema vesicles
vitiligo depigmented patches well-demarcated white macules