Anterior spinothalamic tract Lateral spinothalamic tract Corticospinal tract Diagrams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have all the content and diagrams needed. Here is a complete, well-structured answer:
Spinal Cord Tracts: Anterior Spinothalamic, Lateral Spinothalamic & Corticospinal
Quick Reference Table
| Tract | Type | Modality | Decussation | Location in Cord |
|---|---|---|---|---|
| Anterior (Ventral) Spinothalamic | Ascending (sensory) | Light/crude touch, pressure | Anterior commissure (spinal cord) | Anterior white column |
| Lateral Spinothalamic | Ascending (sensory) | Pain, temperature | Anterior commissure (spinal cord, 1-3 segments above entry) | Lateral white column |
| Lateral Corticospinal | Descending (motor) | Voluntary motor | Pyramidal decussation (cervicomedullary junction) | Lateral white column |
1. Anterior (Ventral) Spinothalamic Tract
Function: Carries light touch (crude/tactile) and pressure from the contralateral body.
Pathway (3-neuron arc):
- 1st-order neuron: Peripheral receptor → dorsal root ganglion → enters spinal cord via dorsal root, ascends 1-2 segments in Lissauer's tract → synapses in dorsal horn (laminae IV-V)
- 2nd-order neuron: Axon crosses in the anterior white commissure to the opposite side → ascends in the anterior funiculus as the anterior spinothalamic tract → travels through brainstem
- 3rd-order neuron: Relays in VPL (ventroposterolateral) nucleus of thalamus → somatosensory cortex (postcentral gyrus, areas 3, 1, 2)
Key points:
- Carries light touch, tickle, and crude pressure
- Crosses in the anterior commissure at or near the level of entry (same segment or just above)
- Less clinically significant than the lateral spinothalamic tract because light touch has redundant pathways (also via dorsal columns)
- Somatotopic organisation: sacral fibres lie most lateral, cervical most medial
Miller's Review of Orthopaedics, 9th Ed. - "Ventral (anterior) spinothalamic tract comprises ascending fibers that transmit light tactile sensation."
2. Lateral Spinothalamic Tract
Function: Carries pain and temperature from the contralateral body. The most clinically important sensory tract.
Pathway (3-neuron arc):
- 1st-order neuron: Nociceptors/thermoreceptors → dorsal root ganglion → enters via dorsal root → synapses in dorsal horn laminae I and V (also IV, VI, VIII); some axon collaterals travel in Lissauer's tract for 1-2 segments before synapsing
- 2nd-order neuron: Crosses in the anterior white commissure, ascending 1-3 segments above the entry level before crossing → then ascends in the lateral funiculus (anterolateral system) → through medulla (lateral, between inferior olive and inferior cerebellar peduncle) → through pons (just lateral to the medial lemniscus) → through midbrain tegmentum
- 3rd-order neuron: Relays in VPL nucleus of thalamus (discriminative pain) and intralaminar/medial nuclei (affective/arousal aspects) → postcentral gyrus (areas 3, 1, 2)
Key points:
- The 2-3 segment ascent before crossing explains why a unilateral cord lesion causes pain/temperature loss 2-3 dermatomes below the lesion level on the contralateral side
- Somatotopic arrangement: sacral/lumbar fibres lie most laterally (superficially); cervical fibres added medially as tract ascends - explains sacral sparing with central cord lesions
- The tract also contains the spinoreticular tract (mediates the affective/emotional pain component via reticular formation → intralaminar thalamus → limbic cortex) and spinomesencephalic tract
- Clinically tested by pin-prick and temperature
Neuroanatomy through Clinical Cases, 3rd Ed. - "it takes two to three spinal segments for the decussating fibers to reach the opposite side, so a lateral cord lesion will affect contralateral pain and temperature sensation beginning a few segments below the level of the lesion."
Adams & Victor's Principles of Neurology, 12th Ed. - "As the ascending fibers cross the cord, they are added to the medial side of the spinothalamic tract, so that the longest fibers from the sacral segments come to lie most superficially."
3. Corticospinal Tract (Lateral)
Function: Voluntary motor control of the limbs and fine skilled movements (the primary descending motor pathway).
Pathway (2-neuron arc: UMN → LMN):
Upper Motor Neuron (UMN):
- ~55% from primary motor cortex (precentral gyrus, Brodmann area 4)
- ~30% from premotor and supplementary motor areas (area 6)
- ~15% from parietal lobe (areas 3, 1, 2, 5, 7)
- Giant pyramidal cells (Betz cells) = ~3% of fibres; largest neurons in the human nervous system
- Cell bodies in cortical layer V
Course:
- Corona radiata (white matter fan)
- Posterior limb of internal capsule - somatotopic: face most anterior → arm → trunk → leg most posterior
- Basis pedunculi of midbrain - middle third; face medial → leg lateral
- Scattered fascicles in pons
- Medullary pyramids (ventral surface of medulla - hence "pyramidal tract")
- Pyramidal decussation at the cervicomedullary junction - ~85% of fibres cross → become the lateral corticospinal tract in the lateral white column
- Anterior corticospinal tract - remaining ~15% do NOT cross at the medulla; descend ipsilaterally in anterior funiculus and cross segmentally in the anterior commissure at each spinal level
Lower Motor Neuron (LMN):
- Lateral corticospinal fibres synapse on anterior horn cells (LMN) and spinal interneurons
- LMN axons exit via ventral roots → peripheral nerves → skeletal muscle
Somatotopic organisation in lateral corticospinal tract:
- Upper extremity fibres medial; lower extremity fibres lateral (sacral most lateral) - explains why central cord syndrome predominantly affects arms
Clinical correlations:
- Lesion above decussation → contralateral UMN weakness (spasticity, hyper-reflexia, Babinski sign)
- Lesion below decussation → ipsilateral UMN weakness
- UMN signs: spasticity, clonus, hyperreflexia, Babinski, no wasting
- LMN signs: flaccidity, hyporeflexia, wasting, fasciculations
Neuroanatomy through Clinical Cases, 3rd Ed. - "about 85% of pyramidal tract fibers cross over at the pyramidal decussation to form the lateral corticospinal tract, while the remaining fibers form the anterior corticospinal tract."
Diagrams
Figure 1 - Lateral Corticospinal Tract (full course from cortex to muscle)
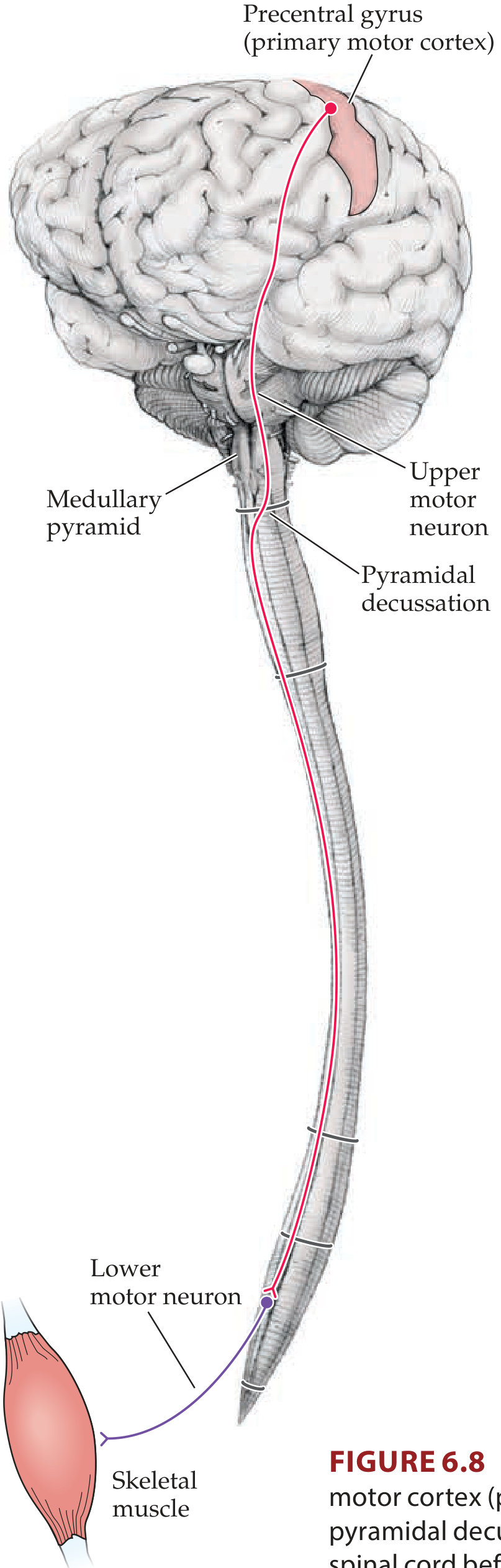
Neuroanatomy through Clinical Cases, 3rd Ed. - Fig 6.8: UMN in primary motor cortex sends axon to cross at pyramidal decussation, then descends to synapse on LMN in anterior horn.
Figure 2 - Lateral Corticospinal Tract (cross-sections at each level + rubrospinal tract)
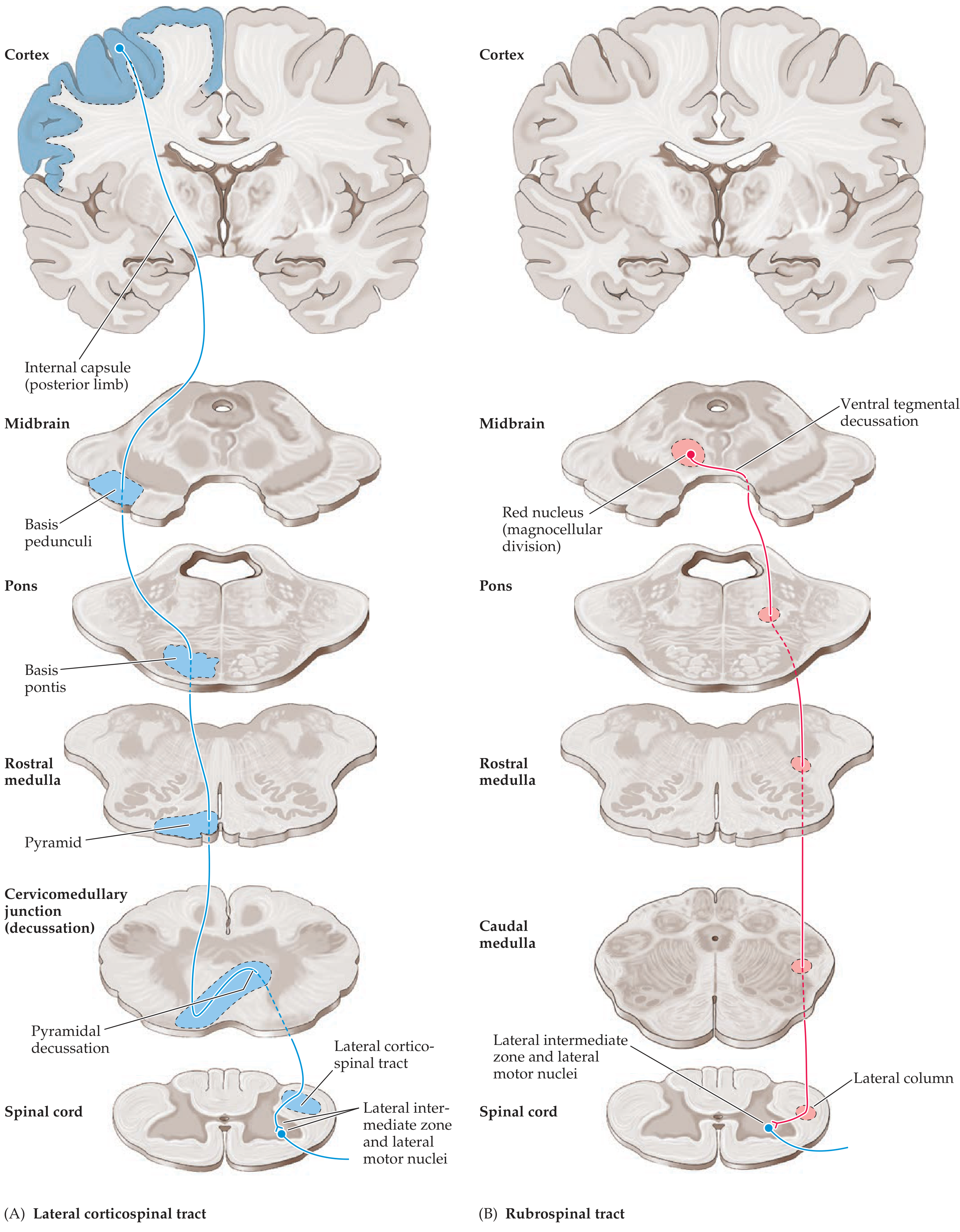
Fig 6.11A: Full course of the lateral corticospinal tract from cortex → internal capsule → basis pedunculi → basis pontis → pyramid → pyramidal decussation → lateral corticospinal tract in spinal cord.
Figure 3 - Somatotopic Organisation (internal capsule, midbrain, spinal cord)
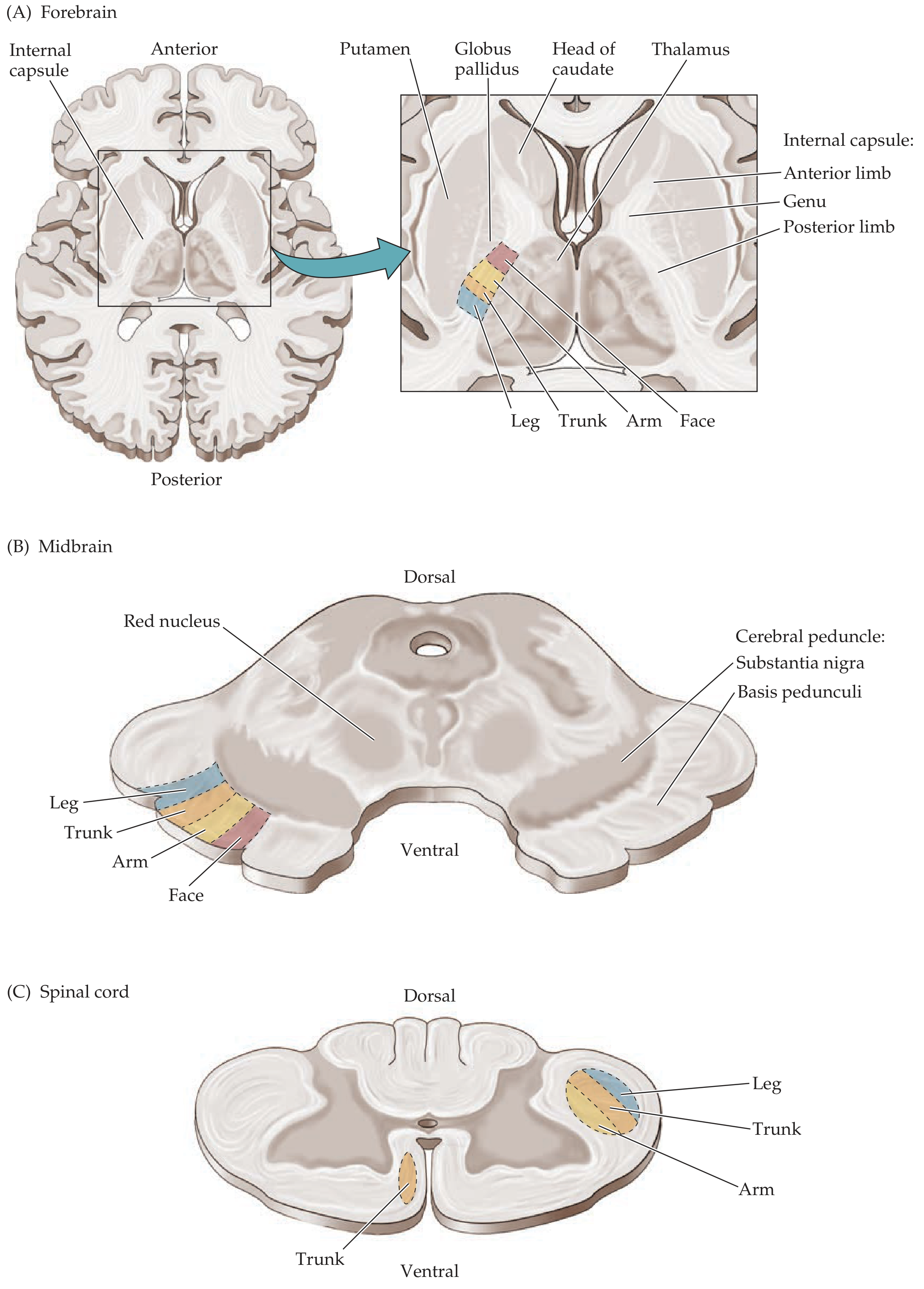
Fig 6.10: (A) Horizontal section through internal capsule - face anterior, leg most posterior in posterior limb. (B) Midbrain - face medial, leg lateral in basis pedunculi. (C) Spinal cord - arm medial, leg lateral in lateral column.
Figure 4 - Spinothalamic Tract (anterior and lateral divisions, full course)
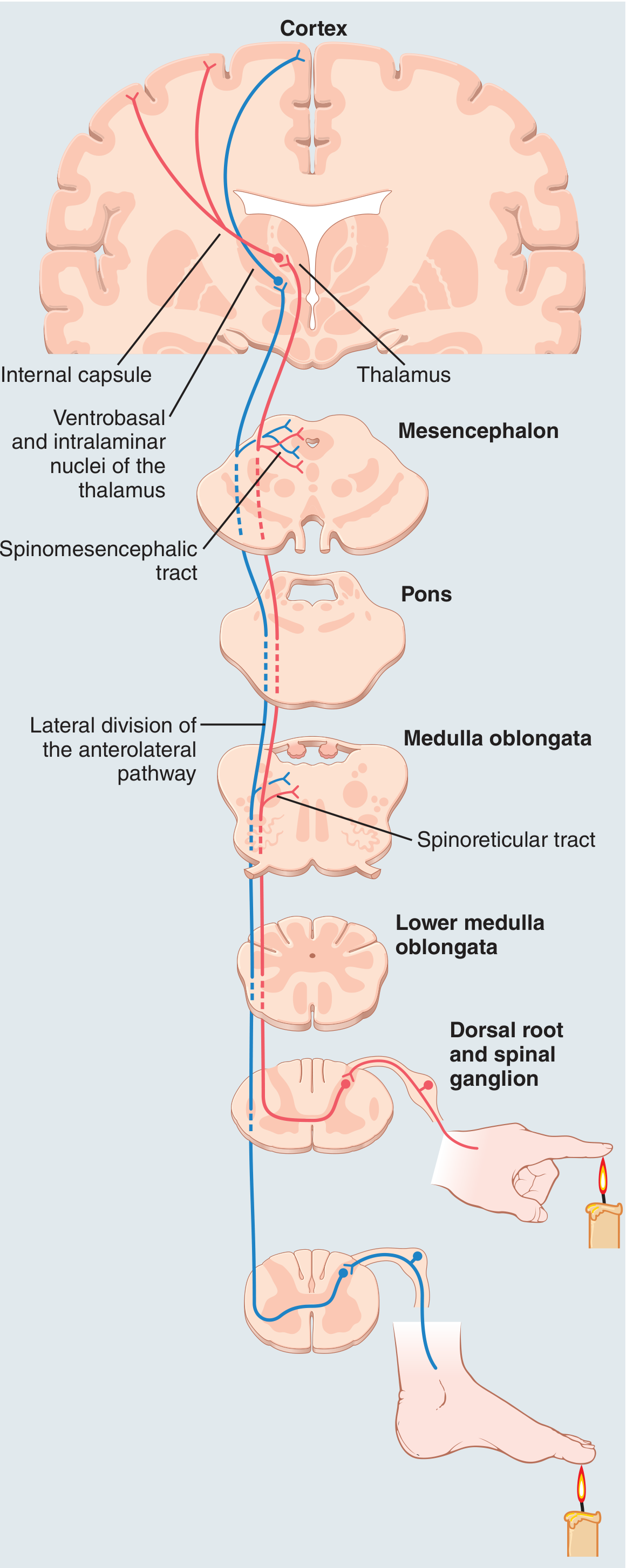
Guyton & Hall Medical Physiology - Fig 48.13: Anterolateral sensory pathway showing anterior and lateral spinothalamic tracts crossing in the anterior commissure, ascending through brainstem to VPL thalamus and cortex.
Figure 5 - Spinothalamic and Trigeminothalamic Tracts (Adams & Victor)
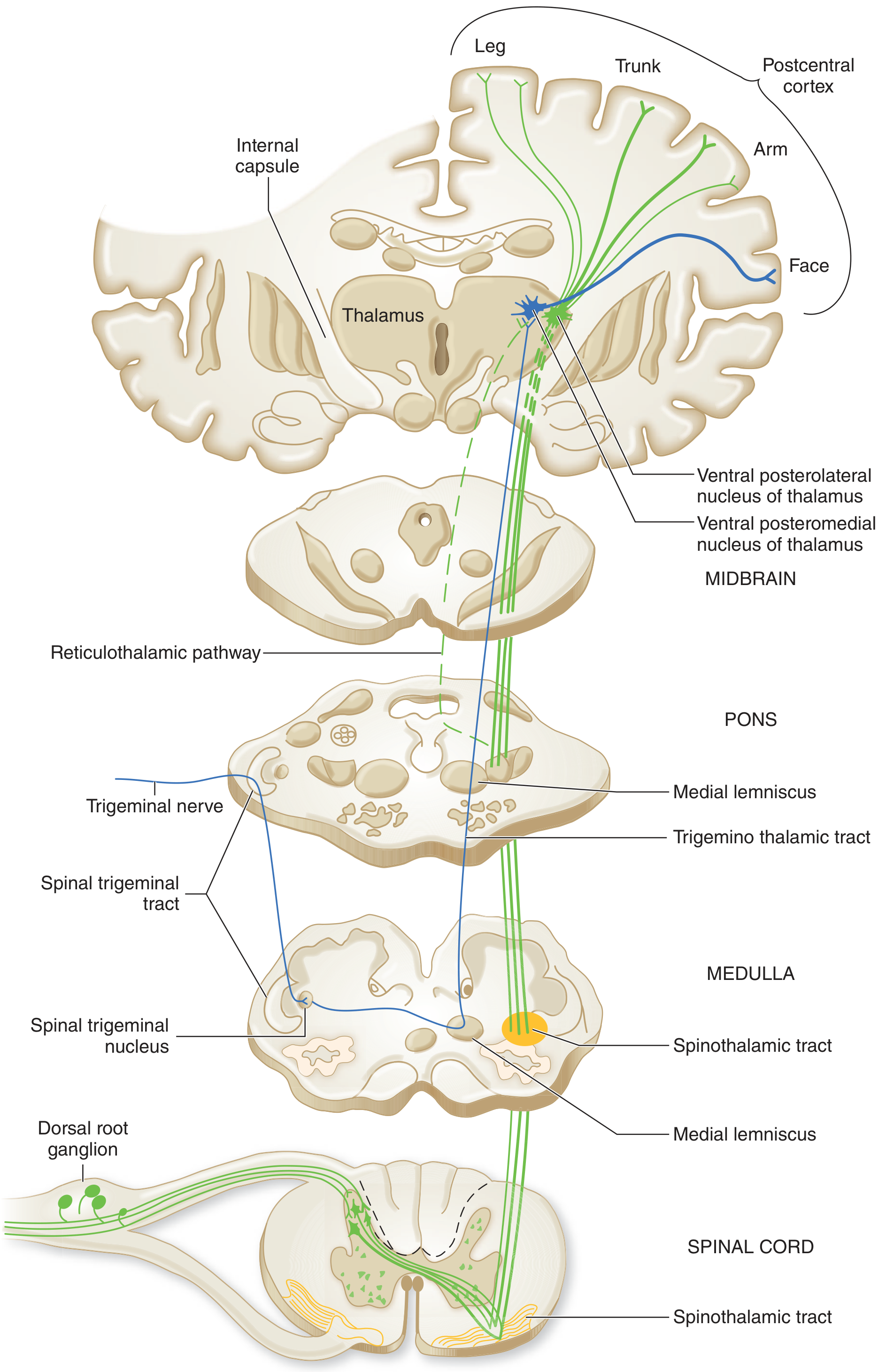
Adams & Victor's Principles of Neurology, 12th Ed. - Fig 7-2: Spinothalamic tract (green) and trigeminothalamic tract (blue) showing relay through VPL and VPM thalamus to postcentral cortex.
Figure 6 - Spinal Cord Cross-section Showing Tract Positions and Incomplete Spinal Cord Injury Syndromes
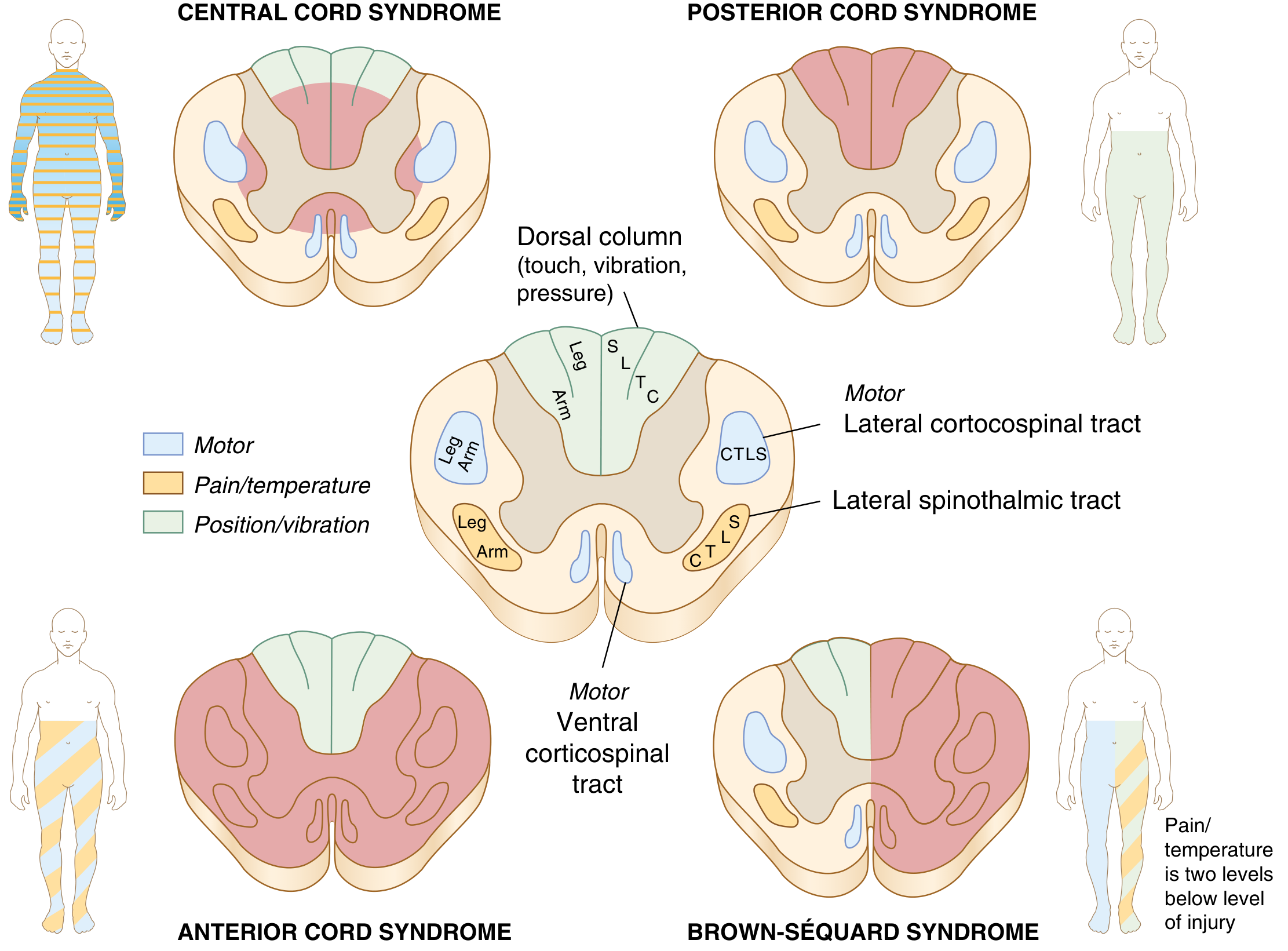
Miller's Review of Orthopaedics, 9th Ed. - Spinal cord tract positions and the four incomplete cord injury syndromes (Central, Posterior, Anterior, Brown-Séquard). Note: lateral spinothalamic tract and lateral corticospinal tract are positioned in the lateral column; ventral corticospinal tract in the ventral column.
Summary: Positional Guide in Spinal Cord Cross-section
DORSAL
┌──────────────────┐
│ Dorsal Columns │ ← proprioception, vibration, fine touch (ipsilateral)
│ (Post. funiculi)│
├────────┬─────────┤
│ Gray │ Lat. │ ← Lateral corticospinal (motor, ipsilateral after decussation)
│ matter │ White │ ← Lateral spinothalamic (pain/temp, contralateral)
│ │ Column │
├────────┴─────────┤
│ Ant. (Ventral) │ ← Anterior spinothalamic (light touch, contralateral)
│ White Column │ ← Anterior corticospinal (motor, uncrossed until cord level)
└──────────────────┘
VENTRAL
Clinical Correlation: Spinal Cord Injury Patterns
| Syndrome | Tracts Affected | Deficit |
|---|---|---|
| Brown-Séquard (hemi-cord) | Ipsilateral: lat. corticospinal + dorsal columns; Contralateral: lat. spinothalamic | Ipsilateral UMN motor + proprioception loss; Contralateral pain/temp loss 2-3 levels below |
| Anterior cord | Ant. + lat. spinothalamic + corticospinal | Bilateral motor + pain/temp loss; vibration/proprioception spared |
| Central cord | Central gray + inner lat. corticospinal (arm fibres) | Arm > leg weakness (arms most medial in tract) |
| Posterior cord | Dorsal columns | Loss of vibration, proprioception, fine touch; pain/temp intact |
Sources: Neuroanatomy through Clinical Cases 3rd Ed.; Adams & Victor's Principles of Neurology 12th Ed.; Guyton & Hall Medical Physiology; Miller's Review of Orthopaedics 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.