Dlc
It looks like your message got cut off. Could you clarify what you mean by "Dlc"?
- DLC (gaming) — downloadable content for a game?
- DLC (medical) — something clinical?
- DLC — an abbreviation for something else?
Let me know what you're looking for and I'll help right away.
Differential lucocyte count
Reading File
Finding Sources
Finding Sources
Searching the Web
differential leukocyte count normal values types WBC
Reading File
Searching Images
differential leukocyte count blood smear WBC types
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of the Differential Leukocyte Count (DLC):
Differential Leukocyte Count (DLC)
Definition
The DLC (also called the differential WBC count) is the percentage distribution of the different types of leukocytes in peripheral blood. It is performed on a Romanowsky-stained peripheral blood smear, scanning a defined counting area and classifying each leukocyte encountered until 100–1000 cells have been counted. The absolute concentration of each cell type = percentage × total leukocyte count.
"An increase in absolute concentration is an absolute increase; an increase in percentage only is a relative increase. Reference intervals are more useful if given as absolute concentrations rather than percentages." — Henry's Clinical Diagnosis and Management by Laboratory Methods
The Five Cell Types & Normal Values
| Cell Type | % of WBCs | Absolute Count (×10⁹/L) |
|---|---|---|
| Neutrophils (segmented + bands) | 50–70% | 1.8–7.7 |
| — Segmented | 40–60% | — |
| — Bands | 0–5% | — |
| Lymphocytes | 20–40% (avg ~34%) | 1.5–4.0 |
| Monocytes | 2–8% (avg ~4%) | 0–0.8 |
| Eosinophils | 1–5% | 0–0.45 |
| Basophils | 0–1% (avg ~0.5%) | 0–0.2 |
Individual Cell Morphology
1. Neutrophil (PMN — Polymorphonuclear Leukocyte)
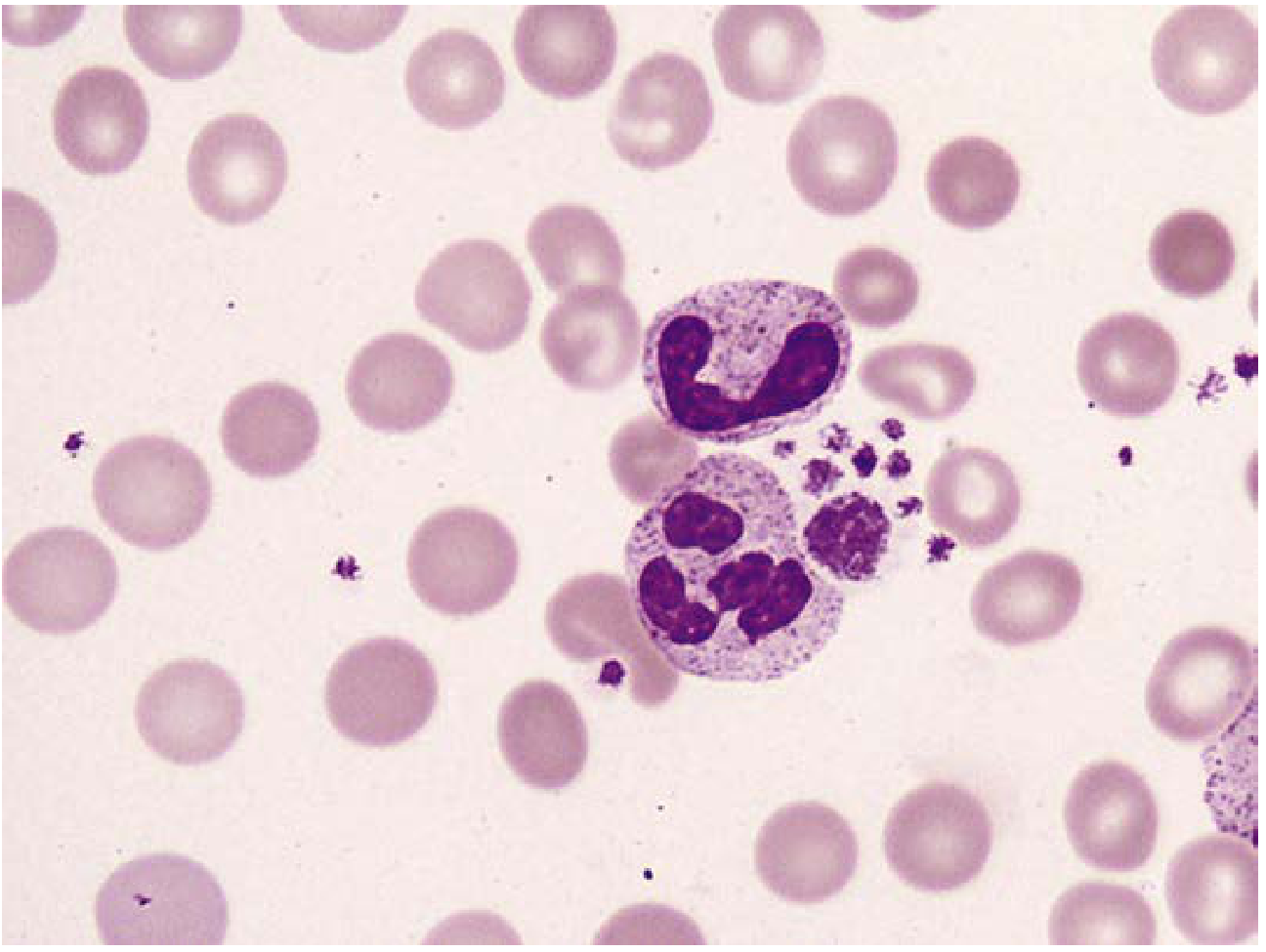
Figure: Mature neutrophil (multi-lobed nucleus with distinct filaments) alongside a band form (horseshoe-shaped nucleus). 1000×.
- Size: ~12 μm
- Nucleus: 2–5 lobes connected by thin filaments; coarse chromatin
- Lobe distribution: 10–30% have 2 lobes, 40–50% have 3 lobes, 10–20% have 4 lobes; ≤5% have 5 lobes
- Granules: Fine, pinkish-lilac (primary = azurophilic, secondary = specific)
- Shift to the left: ↑ bands and immature forms → suggests bacterial infection
- Hypersegmentation (>5 lobes): suggests megaloblastic anemia
2. Lymphocyte
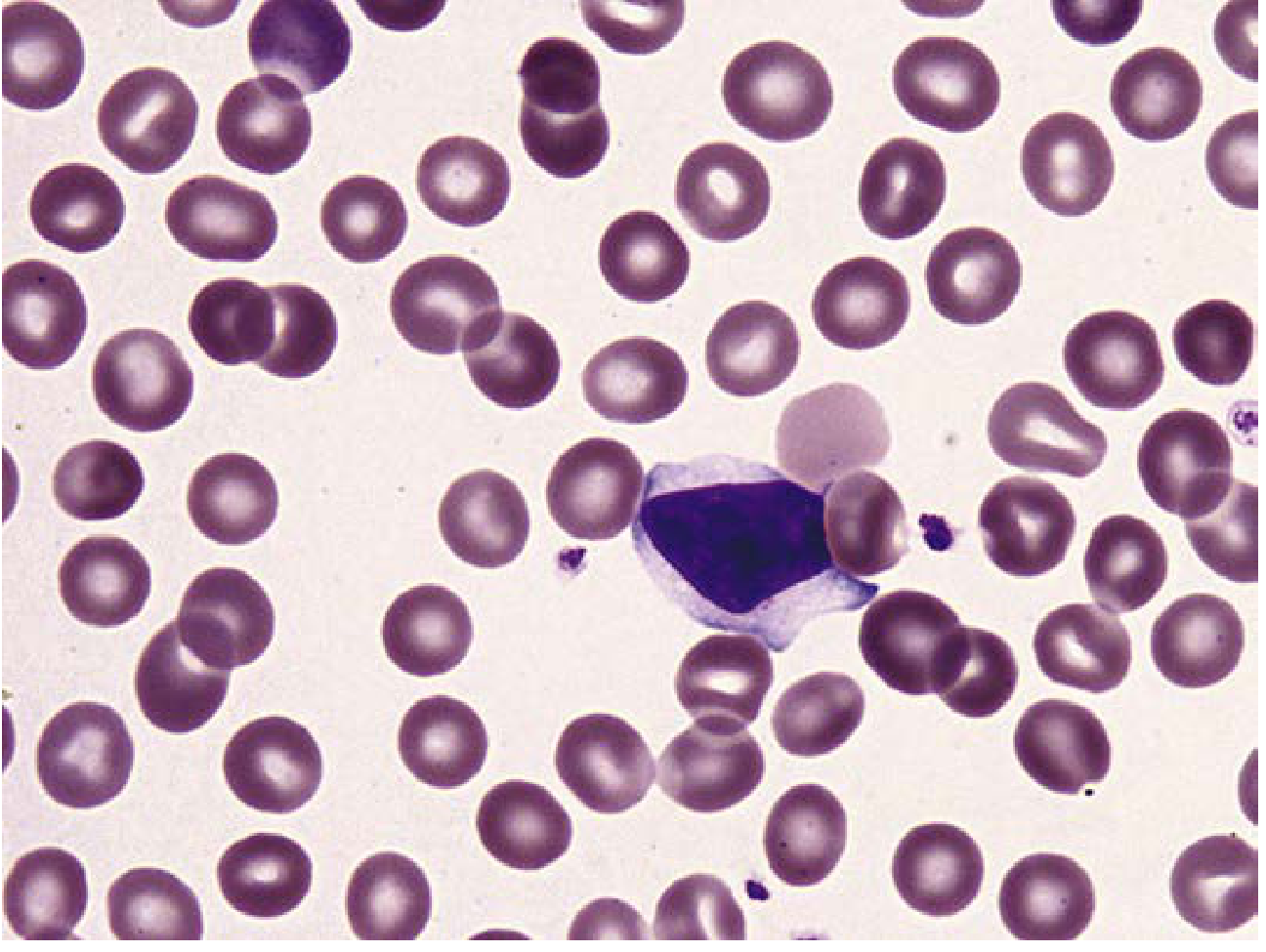
Figure: Reactive lymphocyte with abundant pale-gray cytoplasm and distinct chromatin/parachromatin separation. 1000×.
- Size: 6–15 μm (small to large)
- Nucleus: Round, heavily clumped dark-blue chromatin; may be indented
- Cytoplasm: Scant, pale blue; a clear perinuclear zone
- ~⅓ of large lymphocytes have red-purple azurophilic granules
- Atypical/reactive lymphocytes indicate antigenic stimulation (e.g., EBV)
- Plasma cells (not normally in blood): abundant blue cytoplasm, eccentric nucleus, clock-face chromatin
3. Monocyte
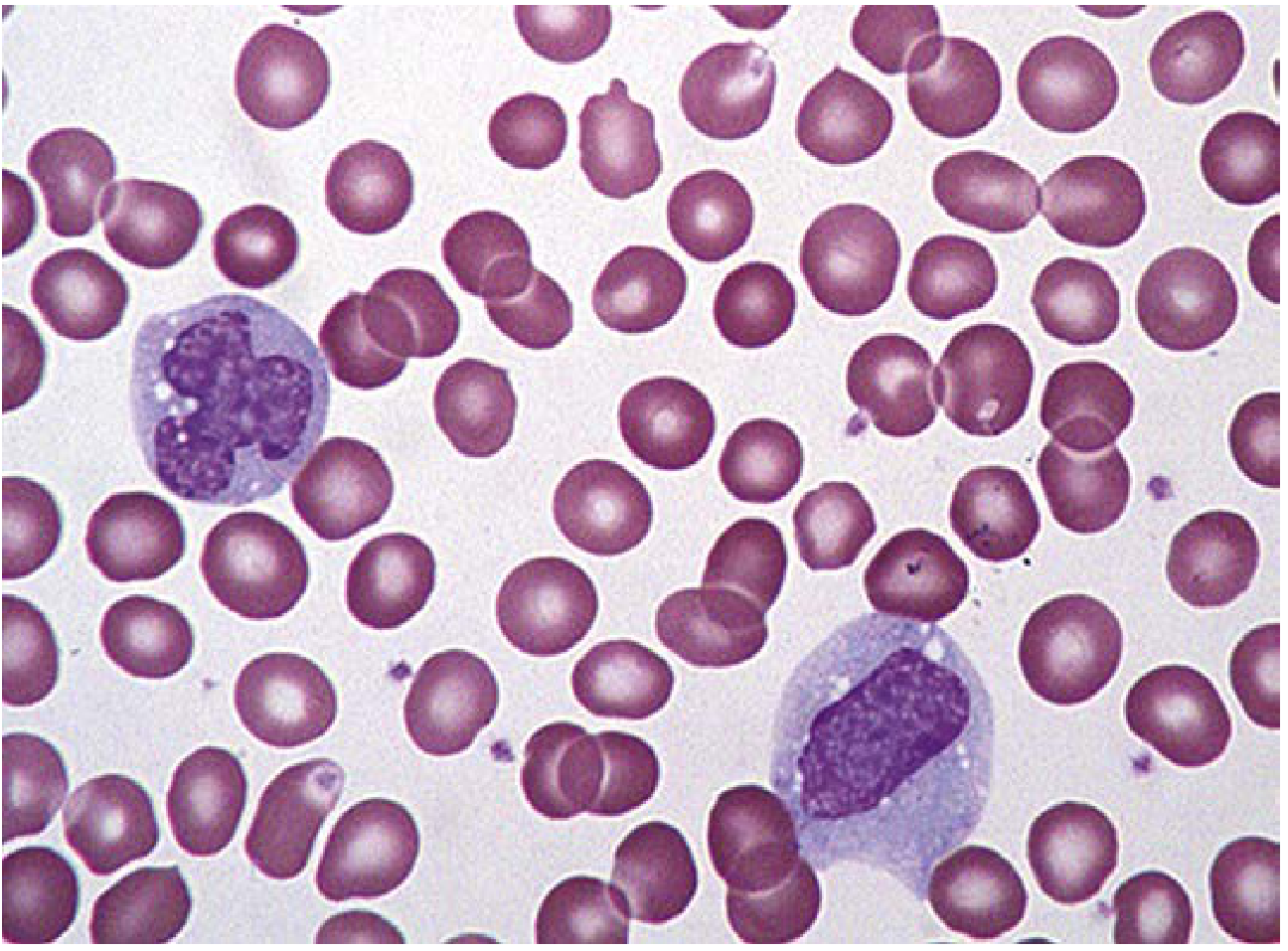
Figure: Two monocytes — the largest normal blood cells — with characteristic kidney/horseshoe-shaped nuclei and fine granular cytoplasm.
- Largest normal blood cell (14–20 μm; 2–3× diameter of RBC)
- Nucleus: Horseshoe/kidney-shaped or partially lobulated; fine parallel chromatin strands; stains less densely than other leukocytes
- Cytoplasm: Abundant, blue-gray, ground-glass appearance; fine red-purple granules; may have vacuoles
- Transforms into tissue macrophage
4. Eosinophil
- Size: Similar to neutrophil or slightly larger
- Nucleus: Usually bilobed
- Granules: Large, bright red-orange (eosinophilic) refractile granules filling the cytoplasm
-
2% in synovial fluid = eosinophilia (seen in Lyme disease, RA, parasites, allergic reactions)
- Peripheral blood eosinophilia >10% may suggest EGPA (Churg-Strauss)
5. Basophil
- Least numerous leukocyte (~0.5%; 95% reference: 0–0.2 × 10⁹/L)
- Nucleus: Less segmented than neutrophil (indented or partially lobulated), often obscured by granules
- Granules: Large, deep purple, water-soluble (may wash out leaving vacuoles); contain histamine and heparin
- May resemble Histoplasma capsulatum if granules are unevenly stained
Method of Performing DLC
- Prepare smear: Air-dried wedge smear or cytocentrifuge preparation, Romanowsky stain (Wright-Giemsa)
- Scan at 10×: Estimate WBC count; scan lateral and feather edges for monocytes and large cells
- Count at high power (100×): Use crenellation technique — move the field side-to-side across the counting area
- Count 100 cells routinely (200–1000 for greater precision)
- Record abnormal cells: NRBCs, blasts, immature granulocytes, reactive lymphocytes must be noted separately
- Automated differential: Hematology analyzers provide 5-part differential using impedance/light scatter; unreliable for abnormal/immature cells — flagged samples require manual review
Clinical Significance of Abnormal Findings
| Finding | Cause |
|---|---|
| Neutrophilia (↑ neutrophils) | Bacterial infection, inflammation, steroids, CML |
| Neutropenia (↓ neutrophils) | Viral infection, aplastic anemia, chemotherapy, drugs |
| Left shift (↑ bands/immature forms) | Acute bacterial infection, sepsis |
| Hypersegmentation | Megaloblastic anemia (B12/folate deficiency) |
| Lymphocytosis | Viral infections (EBV, CMV), CLL, pertussis |
| Lymphopenia | HIV, immunosuppression, steroids |
| Monocytosis | TB, subacute bacterial endocarditis, SLE |
| Eosinophilia | Allergy, asthma, parasites, EGPA, drug reactions |
| Basophilia | CML, allergic reactions, hypothyroidism |
| Blasts | Acute leukemia |
Absolute vs. Relative Count
The absolute count (% × total WBC) is clinically more meaningful than the percentage alone. For example, a patient with lymphopenia (total WBC 2.0 × 10⁹/L, 60% lymphocytes) has a relative lymphocytosis but a normal absolute lymphocyte count.
Source: Henry's Clinical Diagnosis and Management by Laboratory Methods (9780323673204)
This is a shared conversation. Sign in to Orris to start your own chat.