give me ultrasound picture of complete muscle tear of upper or lower limb
Ultrasound of Complete Muscle/Tendon Tear - Lower Limb
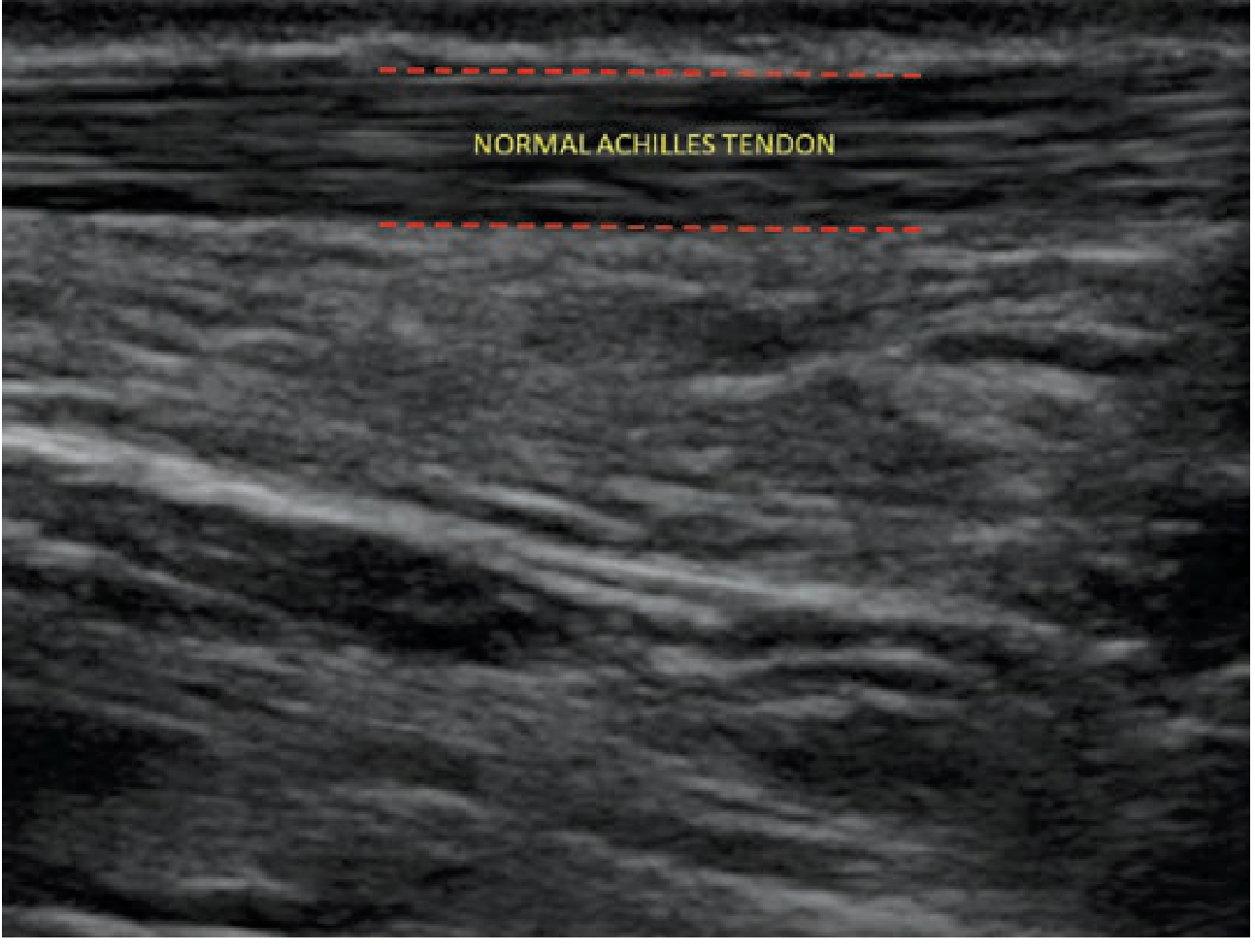
1. Normal Achilles Tendon (for comparison)
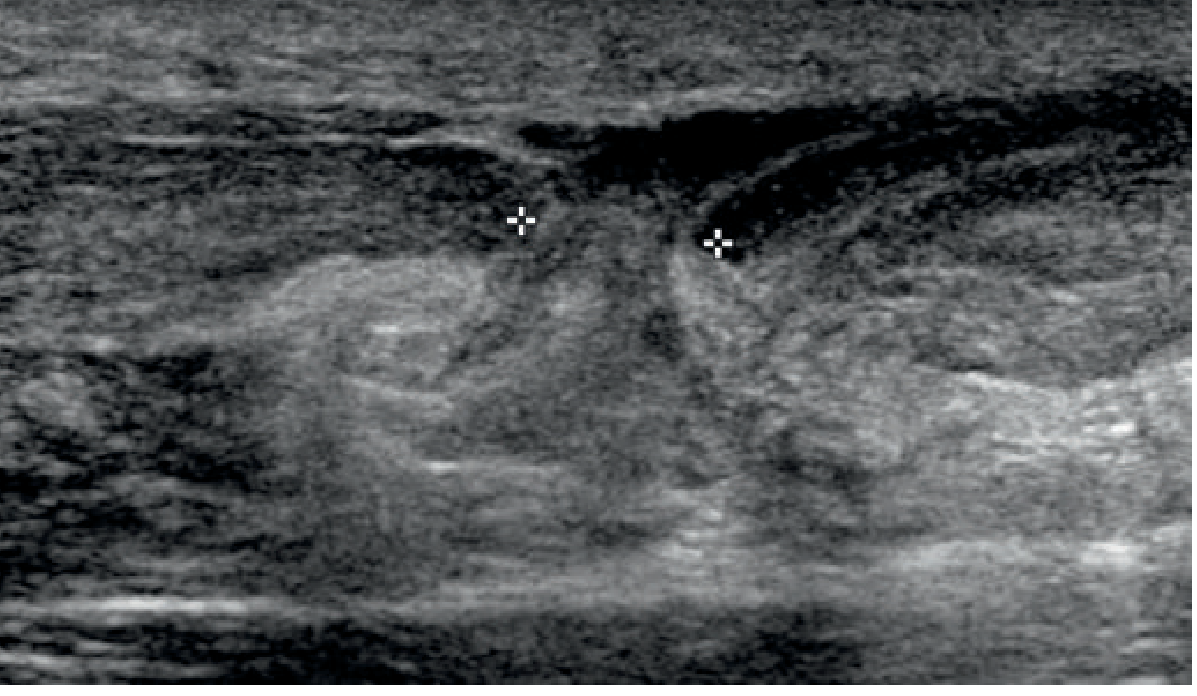
2. Complete Achilles Tendon Rupture
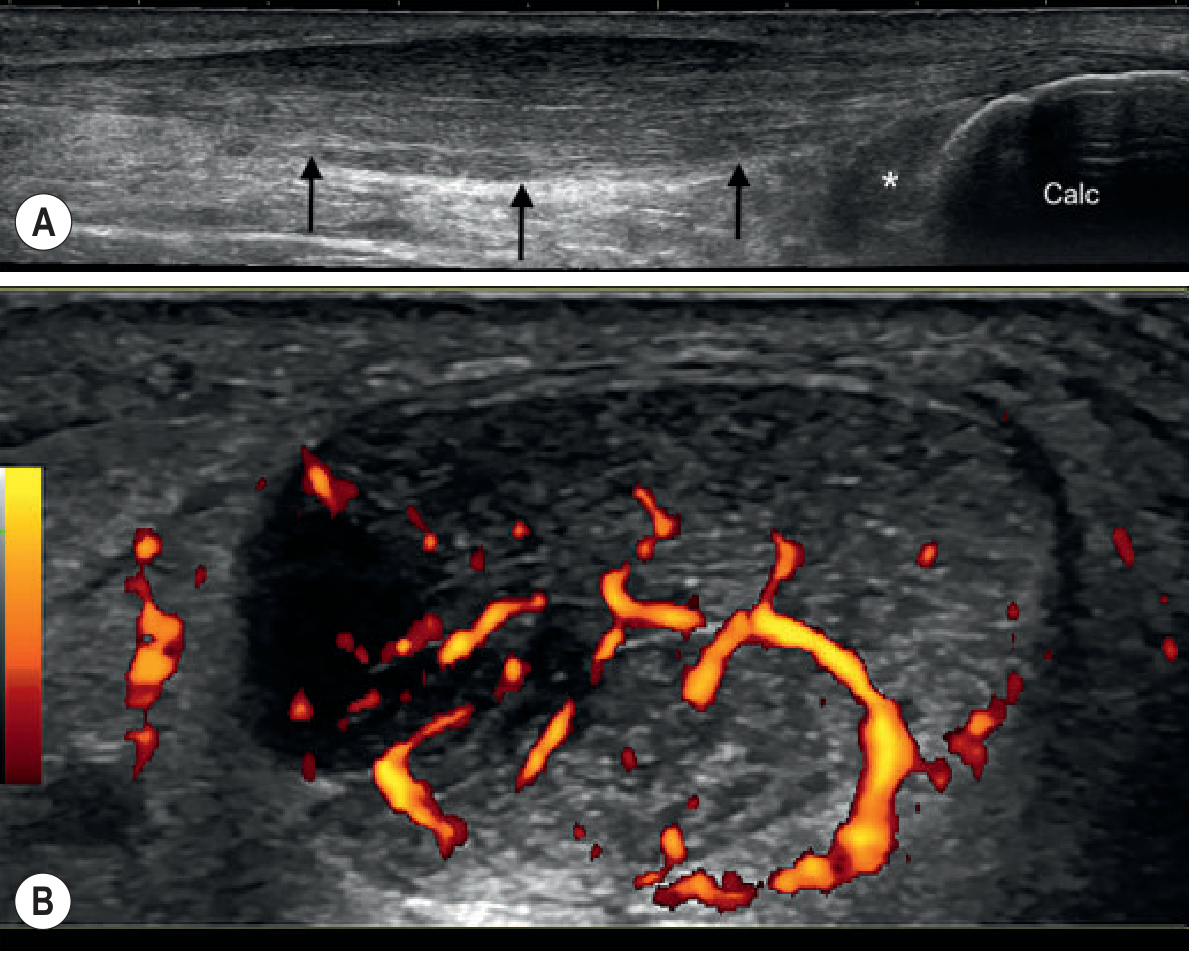
3. Achilles Tendinopathy with Power Doppler (pre-rupture stage for context)
How to Recognize a Complete Tear on Ultrasound
| Feature | Normal | Complete Tear |
|---|---|---|
| Fibrillar pattern | Continuous parallel echogenic fibers | Completely disrupted / absent |
| Tendon continuity | Intact end-to-end | Gap between retracted ends |
| Gap contents | None | Hypoechoic hematoma or echogenic fat (Kager's fat in Achilles) |
| Dynamic test | Tendon moves synchronously | No movement at tear site; ends move apart |
| Tendon thickness | Uniform | Proximal end may appear bulbous (retraction) |
- Discontinuity - complete loss of fibrillar echotexture across the full thickness
- Retraction - proximal tendon stump retracts, often visible as a curled-up echogenic mass
- Hematoma - anechoic or hypoechoic collection filling the gap
- Herniated fat - in Achilles tears, echogenic Kager's fat is seen interposed between the torn ends
- Quadriceps/patellar tendon: complete rupture shows hypoechogenicity over the entire length and thickness of the tendon, with a wedge-shaped separation
give me usg images of infective myositis
pyomyositis ultrasound sonography images muscle abscess findings
https://pmc.ncbi.nlm.nih.gov/articles/PMC7990081
pyomyositis ultrasound intramuscular abscess hypoechoic collection site:radiopaedia.org OR site:pmc.ncbi.nlm.nih.gov
Ultrasound of Infective Myositis (Pyomyositis)
Stage 1 - Invasive Stage: Early Muscle Edema
- Diffuse muscle swelling and enlargement
- Loss of normal striated muscle architecture (the usual parallel echogenic fibrillar pattern is disrupted)
- Mildly hypoechoic or heterogeneous muscle echotexture
- No discrete fluid collection yet
Stage 2 - Suppurative Stage: Intramuscular Abscess Formation



Ultrasound Features Summary by Stage
| Stage | Ultrasound Finding |
|---|---|
| Stage 1 (Invasive) | Diffuse muscle enlargement; loss of normal striated echo pattern; mild hypoechogenicity; no fluid pocket; hyperemia on Doppler |
| Stage 2 (Suppurative) | Discrete intramuscular hypoechoic/anechoic fluid collection; internal echoes/debris; posterior acoustic enhancement; surrounding echogenic edematous muscle; peripheral Doppler flow (hyperemia) |
| Stage 3 (Late/Septic) | Extension beyond single muscle; multi-compartment spread; gas echoes (bright foci with dirty shadowing) if gas-forming organisms |
Key Technical Points
- Probe: High-frequency linear array (7.5-15 MHz) for superficial muscles; lower frequency curvilinear (3-5 MHz) for deep muscles (iliopsoas, gluteus)
- Doppler: Power Doppler shows peripheral hyperemia around the abscess wall - distinguishes active infection from old hematoma
- Sonopalpation: Gentle probe compression over the collection reveals movement of pus/debris - confirms liquefaction
- Always compare with the contralateral normal side
- Limitation: Stage 1 (invasive) may be missed on ultrasound; MRI is the gold standard when clinical suspicion is high despite normal/equivocal ultrasound
myositis ossificans usg images
myositis ossificans ultrasound sonography images acoustic shadowing eggshell calcification
myositis ossificans ultrasound stages early late peripheral calcification acoustic shadow PMC site:pmc.ncbi.nlm.nih.gov
Ultrasound of Myositis Ossificans
Stage-by-Stage Ultrasound Appearances
Stage 1 (Early / Acute: 0-3 weeks) - Hematoma, No Calcification Yet

Stage 2 (Intermediate / Subacute: 3-8 weeks) - Peripheral Calcification

Stage 3 (Late / Mature: >8 weeks) - Complete "Eggshell" Calcification

Ultrasound Findings Summary by Stage
| Stage | Timing | Ultrasound Appearance |
|---|---|---|
| Acute | 0-3 weeks | Hypoechoic/anechoic intramuscular hematoma; muscle swelling; no calcification; hyperemia on Doppler |
| Intermediate | 3-8 weeks | Heterogeneous mass; peripheral hyperechoic foci begin to appear; partial posterior acoustic shadowing developing |
| Mature | >8 weeks | Complete hyperechoic peripheral "eggshell" rim; dense posterior acoustic shadowing; central area acoustically obscured; no Doppler flow |
Key Diagnostic Points on Ultrasound
- Zone phenomenon - peripheral calcification with a relatively lucent center is the hallmark; calcification always starts at the rim and moves inward (opposite to osteosarcoma)
- Posterior acoustic shadowing increases progressively as ossification matures - in late stages it can be so dense that the lesion interior is completely obscured
- No bone continuity - the lesion is separate from the adjacent cortex (important to confirm with orthogonal views); absence of a cleavage plane from bone suggests malignancy
- Doppler: Active hyperemia in early/intermediate stages; absent flow in mature calcified rim
- Probe: High-frequency linear 7.5-15 MHz; standoff pad may help for very superficial lesions
- US is very sensitive to calcific changes - it can detect ossification earlier than plain radiography in some cases
muscle sarcoma
soft tissue sarcoma muscle ultrasound sonography imaging findings
rhabdomyosarcoma synovial sarcoma undifferentiated pleomorphic sarcoma ultrasound images intramuscular
https://pmc.ncbi.nlm.nih.gov/articles/PMC8449057
soft tissue sarcoma ultrasound heterogeneous mass intramuscular thigh Doppler PMC open access image
Ultrasound Imaging of Muscle Sarcoma (Soft Tissue Sarcoma)
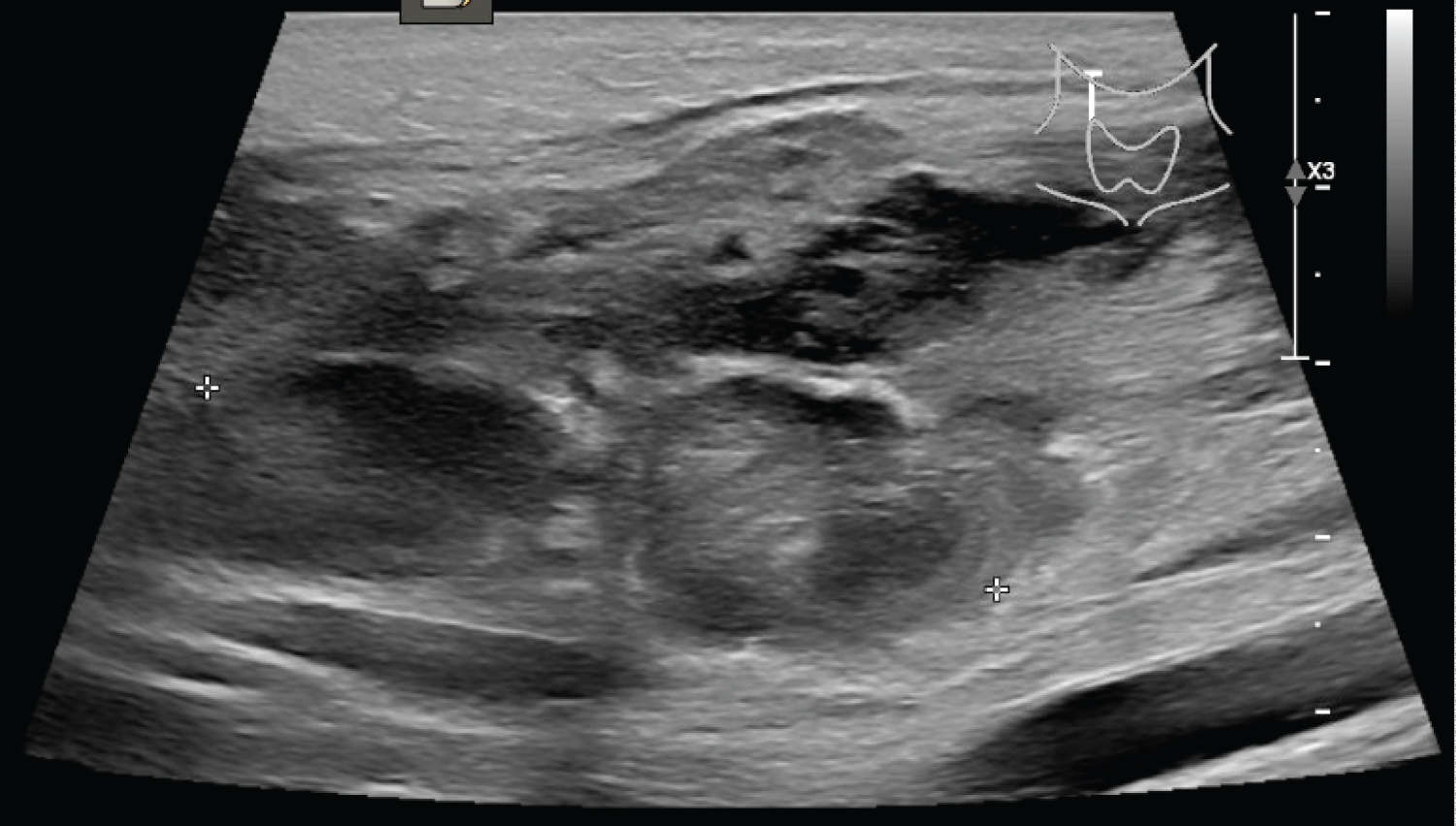
Image 1 - Undifferentiated Pleomorphic Sarcoma (UPS) / MFH - Thigh
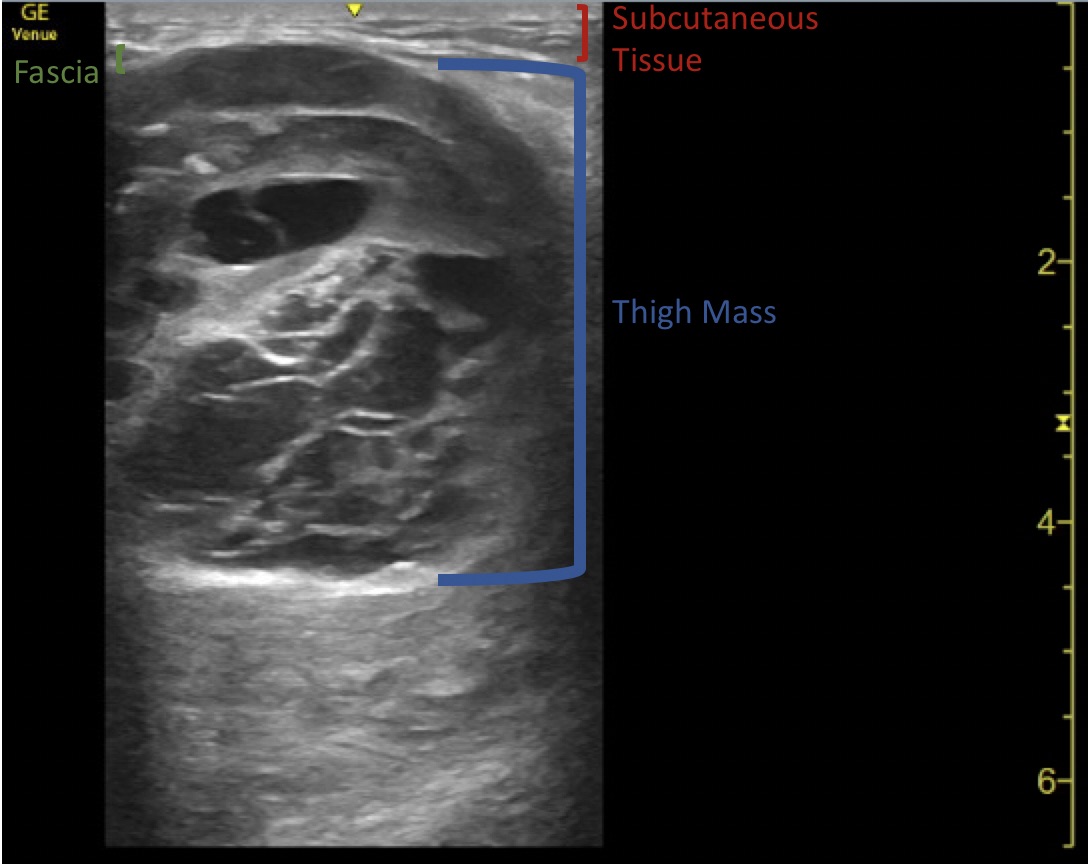
Image 2 - Soft Tissue Sarcoma, Forearm - Heterogeneous Mass with Marked Doppler Vascularity

Image 3 - Large Deep Sarcoma (Abdominal/Retroperitoneal Leiomyosarcoma) with Doppler

Image 4 - Synovial Sarcoma with Abnormal Doppler Flow
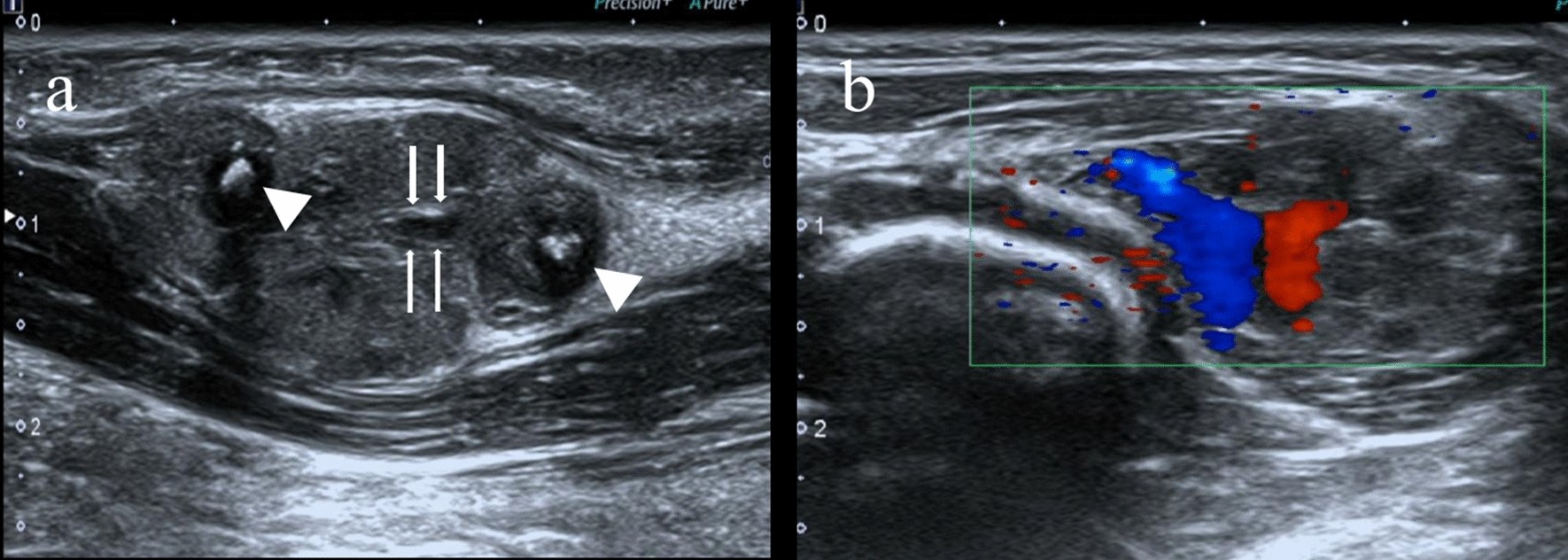
Image 5 - Radiopaedia Case: Intramuscular Sarcoma, Right Upper Thigh

Ultrasound Features: Benign vs. Sarcoma
| Feature | Benign | Sarcoma (Red Flags) |
|---|---|---|
| Size | <46 mm | >46 mm (>5 cm) |
| Location | Subcutaneous | Deep to fascia / intramuscular |
| Margins | Well-defined | Ill-defined, infiltrative |
| Echotexture | Homogeneous | Heterogeneous (mixed hypo/hyperechoic) |
| Necrosis | Absent | Anechoic areas (central necrosis) |
| Vascularity | Avascular or peripheral only | Marked internal, chaotic, disorganised Doppler |
| Vessel pattern | Organised/hierarchical | Anarchic - trifurcations, irregular calibre |
| Compression | May compress (lipoma) | Incompressible |
| Growth | Stable | Increasing in size |
Key Sarcoma Subtypes and USG Characteristics
| Subtype | Typical USG Appearance |
|---|---|
| Undifferentiated Pleomorphic Sarcoma (UPS/MFH) | Large, deep, markedly heterogeneous; mixed hypo/hyperechoic; necrosis common; high vascularity |
| Synovial Sarcoma | May appear deceptively well-defined and homogeneous; periarticular; calcifications in 30%; "triple sign" on MRI |
| Liposarcoma | Variable - myxoid type appears hypoechoic/pseudocystic; well-differentiated type echogenic like lipoma but large and deep |
| Rhabdomyosarcoma | Poorly defined, deeply invasive; heterogeneous; most common in children |
| Leiomyosarcoma | Hypoechoic mass, often with necrosis; high vascularity; retroperitoneal or extremity |
| Myxofibrosarcoma | Hypoechoic/pseudocystic due to myxoid matrix; may have "tail sign" infiltrating along fascia |
Role of Ultrasound in Sarcoma - Practical Points
- First-line triage: Ultrasound can definitively diagnose benign lesions (lipoma, ganglion, haematoma) and refer suspicious ones urgently
- Biopsy guidance: USG-guided core needle biopsy is the standard method - along the shortest path, avoiding neurovascular structures, with care to keep the biopsy tract within the eventual surgical resection field
- Always use Doppler: Vascularity pattern is the most discriminating feature
- Pitfall - myxoid tumors: Can mimic cysts on greyscale - increase the gain to reveal internal echoes indicating solid content (myxoid liposarcoma, intramuscular myxoma)
- If any doubt: Any mass >5 cm, deep to fascia, or with internal vascularity requires urgent MRI - do not attempt excisional biopsy without imaging staging
tennis leg usg images
tennis leg ultrasound sonography gastrocnemius medial head tear plantaris images
https://pmc.ncbi.nlm.nih.gov/articles/PMC3060433
tennis leg ultrasound images PMC3060433 gastrocnemius soleus hematoma tear site:pmc.ncbi.nlm.nih.gov
tennis leg ultrasound gastrocnemius medial head tear hematoma fluid between gastrocnemius soleus image open access
https://www.kjronline.org/DOIx.php?id=10.3348%2Fkjr.2006.7.3…
"tennis leg" ultrasound "gastrocnemius" "soleus" fluid collection hematoma image cdn.ncbi.nlm.nih.gov OR radiopaedia
Ultrasound of Tennis Leg
Anatomy Relevant to USG
- Skin / subcutaneous fat
- Gastrocnemius (hypoechoic with pennate fibrillar pattern)
- Echogenic fascia / aponeurosis (the triceps surae junction - the key interface)
- Soleus (deeper, also pennate)
Image 1 - Classic Tennis Leg: Fluid Between Gastrocnemius and Soleus (Labeled)

Image 2 - Extended Field-of-View: Aponeurotic Tear with Hematoma

Image 3 - Focal Disruption at the Musculotendinous Junction

Image 4 - Bilateral Comparison (Affected vs. Normal)

Image 5 - Large Hematoma Between Layers

USG Findings by Injury Grade
| Grade | Injury | Ultrasound Appearance |
|---|---|---|
| Grade 1 (Mild strain) | Microscopic tears; no macroscopic disruption | Near-normal; mild hypoechoic edema within MHG fibers; no fluid collection |
| Grade 2 (Partial tear) | Partial aponeurotic disruption | Disruption of pennate pattern; thin fluid collection (4-8 mm) between MHG and soleus; focal hypoechoic hematoma |
| Grade 3 (Complete tear) | Full-thickness aponeurotic rupture | Large fusiform hematoma (6-16 mm) filling gastrocnemius-soleus space; retraction of MHG; complete loss of fibrillar pattern at MTJ |
Classic USG Checklist for Tennis Leg
- Fluid between MHG and soleus - the hallmark sign; seen in 90.9% of cases
- Disruption of the pennate/fibrillar pattern of the distal MHG - loss of the normal echogenic septae
- Hematoma size - measure thickness; predicts severity and recovery time
- MHG retraction - retracted proximal stump visible as a hypoechoic bulge
- Fluid tracking distally along fascial planes - indicates large tear
- Always check for DVT - coexists in up to 10% of tennis leg cases; DVT appears as a non-compressible thrombosed vein
- Plantaris tendon - look for it as a separate thin echogenic line between MHG and soleus; discontinuity = plantaris tear (only 1.4% of tennis leg cases)
- Doppler - hyperemia at the tear margins; helps guide aspiration
baker' cyst and ruptured baker's cyst usg images
Baker's cyst ruptured popliteal cyst ultrasound sonography images findings
Baker's cyst ultrasound "neck sign" communication knee joint anechoic posterior acoustic enhancement radiopaedia open access
Ultrasound of Baker's Cyst and Ruptured Baker's Cyst
PART 1: Intact Baker's Cyst
Image 1 - Classic Simple Baker's Cyst: Transverse View with Measurements
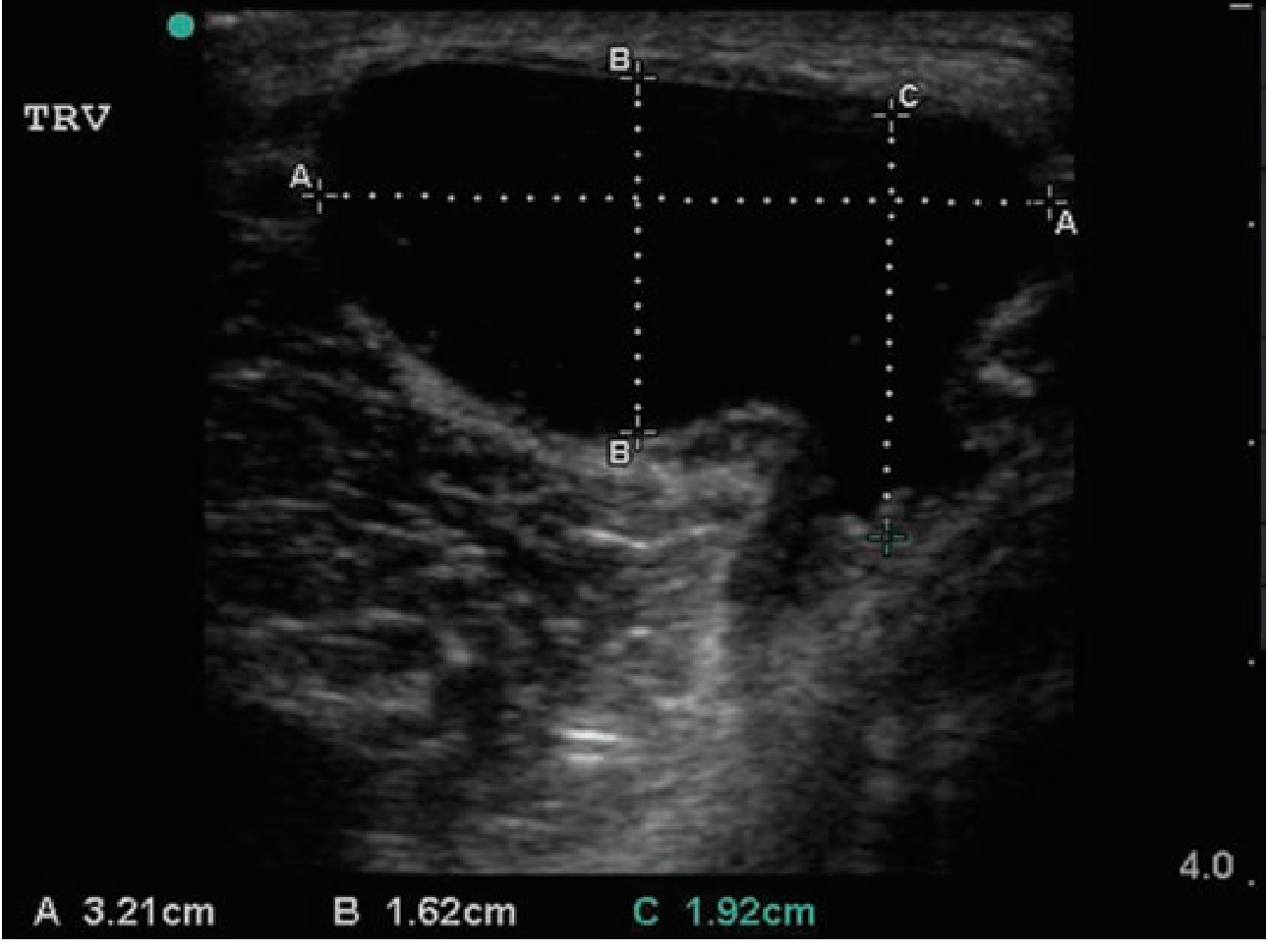
- Large anechoic (completely black/dark) fluid-filled cavity
- Sharply defined walls
- Posterior acoustic enhancement (the area deep to the cyst appears brighter than surrounding tissue - confirms fluid content)
- Well-encapsulated, oval/teardrop shape
Image 2 - Anatomical Position: Baker's Cyst between Semimembranosus and Medial Gastrocnemius (Labeled)

Image 3 - Baker's Cyst with Neck Communication to Knee Joint

- Panel A: Large cyst - yellow arrows show the "neck" communication connecting the cyst to the knee joint; white arrows show the cyst walls
- Panel B: Medium-sized cyst with clear neck visible between SM and MG
- Panel C: Small early cyst - subtle anechoic collection with the characteristic neck
Image 4 - Complex Baker's Cyst with Internal Debris (Thick-Walled)

- Internal echoes / debris (hyperechoic foci within the anechoic fluid)
- Wall thickening and irregularity
- Loss of clean posterior wall definition
Image 5 - Intact Baker's Cyst, Right Popliteal Fossa

PART 2: Ruptured Baker's Cyst
Image 6 - Ruptured Baker's Cyst: Pointed "Beak" Sign + Leaking Fluid Tracking into Calf

- The Baker's cyst body (dark anechoic area upper left)
- A pointed/beaked inferior margin (arrow) - this is the "beak sign" indicating the cyst has ruptured inferiorly
- Fluid tracking distally into the calf (dark hypoechoic fluid extending to the right along fascial planes)
Image 7 - Ruptured Baker's Cyst: Extended Field of View, Popliteal to Mid-Calf
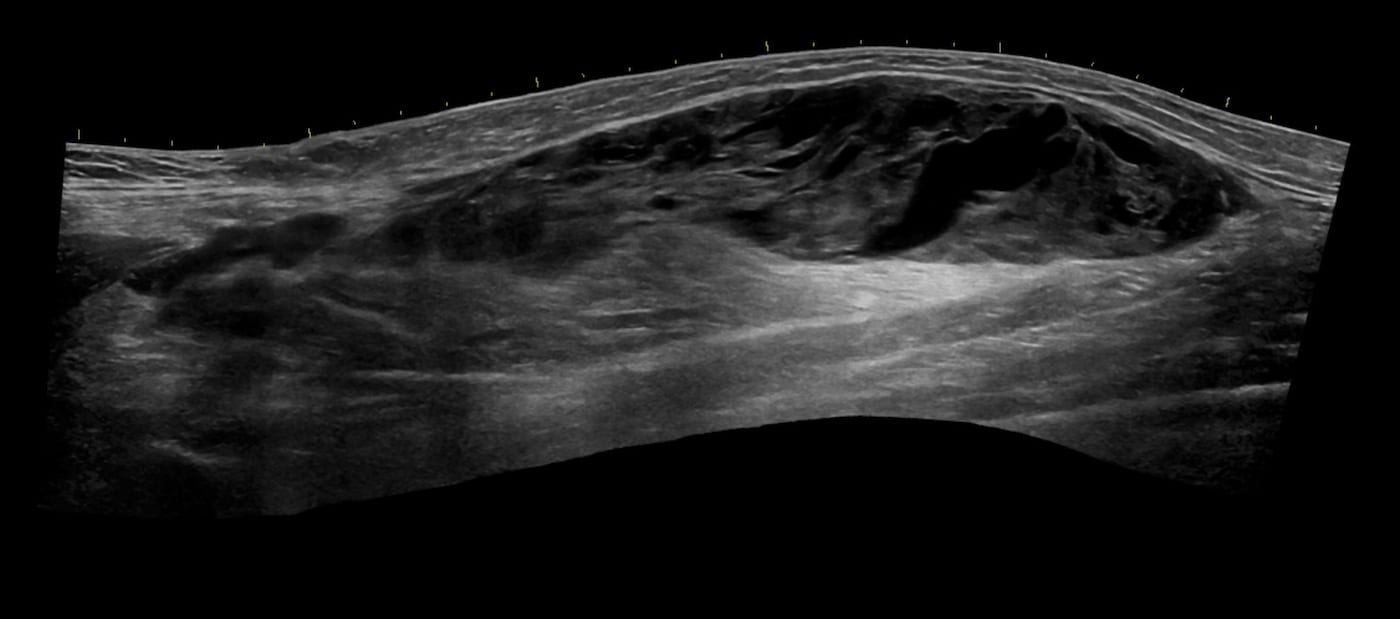
Image 8 - Right Popliteal Fossa: Intact Cyst at Popliteal Level

Image 9 - Complex Cyst: Bilateral Comparison, Right Knee

USG Comparison: Intact vs. Ruptured Baker's Cyst
| Feature | Intact Cyst | Ruptured Cyst |
|---|---|---|
| Shape | Round / oval, smooth walls | Irregular, pointed "beak" at inferior pole |
| Margins | Well-defined, sharp | Indistinct, collapsed, irregular |
| Fluid content | Anechoic (simple) or echogenic (complex) | Heterogeneous, mixed echogenicity |
| Location | Confined to popliteal fossa | Fluid tracks distally into calf between gastrocnemius and soleus |
| Posterior enhancement | Present (confirms cystic) | Variable - may be lost |
| Surrounding tissue | Normal | Edematous, hyperechoic subcutaneous fat |
| DVT exclusion | Add Doppler of popliteal vein | Always perform - DVT coexists in 10% |
Practical USG Protocol
- Probe: High-frequency linear (10-15 MHz)
- Position: Patient prone, knee extended; or lateral decubitus
- Start at: Popliteal fossa in transverse plane - look for cyst between SM tendon and MHG
- Identify the neck - trace the connection to the knee joint (goes anterosuperiorly)
- Scan distally if rupture suspected - follow fluid down the calf to the level of the soleus
- Always add Doppler of the popliteal and proximal calf veins to exclude DVT
- Dynamic compression - a simple cyst is compressible; a solid mass is not
KNEE JOINT EFFUSION,PREPATELLAR AND INFRAPATELLAR BURSITIS USG IMAGES
knee joint effusion prepatellar infrapatellar bursitis ultrasound sonography images suprapatellar recess
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.13.content.19.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.
KNEE JOINT EFFUSION,PREPATELLAR AND INFRAPATELLAR BURSITIS USG IMAGES
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.13.content.19.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.
pre and infrapatellar bursitis usg images
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.13.content.19.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.
prepatellar bursitis usg images
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.13.content.19.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.