Mamta divas, explain in detail for psm exam from park
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Mamta Diwas MCP day Park's PSM textbook details
Finding Sources
Finding Sources
Searching the Web
Mamta Diwas fixed day immunization session services beneficiaries PSM
Reading File
Reading Web Page
https://njcmindia.com/index.php/file/article/download/1464/1…
Reading File
Reading File
I now have enough information from Park's and supplementary sources. Let me compile the complete, exam-focused answer.
Mamta Diwas (Health and Nutrition Day / Village Health and Nutrition Day)
1. Definition
Mamta Diwas (also called Health and Nutrition Day or Village Health and Nutrition Day - VHND) is a fixed day, fixed site preventive and promotive health care service session organized once a month at the Anganwadi centre for mothers and children in a village or urban slum area.
- "Mamta" = mother's love/care in Hindi
- The concept evolved under the Reproductive and Child Health (RCH) Programme to strengthen outreach maternal and child health services
- In urban settings it is called "Mamta Day" or "Health and Nutrition Day" and is organized by Urban Health Centres (UHCs/UPHCs)
2. Under Which Programme?
Mamta Diwas operates under:
- National Health Mission (NHM) - specifically under Reproductive Maternal Newborn Child Health + Adolescent (RMNCH+A) strategy
- It is a key outreach activity under RCH-II / NHM
- Linked with ICDS (Integrated Child Development Services) through the Anganwadi centre
As per Park's (NHM chapter): "Village health and nutrition days in rural areas as an outreach activity, for provision of maternal and child health services."
3. Frequency and Site
| Feature | Detail |
|---|---|
| Frequency | Once a month (at least) per village |
| Site | Anganwadi centre |
| Day/Time | Fixed day, fixed time ("same day, same site, same time" policy) |
4. Beneficiaries
All three of the following are target beneficiaries:
- All pregnant women
- Breastfeeding/lactating women
- Under-5 children (especially infants and children up to 5 years)
In urban areas: also includes adolescents
5. Services Provided
A. Maternal Health Services
- Antenatal registration and antenatal check-up (ANC)
- Weight measurement of pregnant women
- Blood pressure measurement
- Haemoglobin estimation (detection of anaemia)
- Tetanus Toxoid (TT) injection
- Iron and Folic Acid (IFA) tablet distribution
- Identification of high-risk pregnancies and referral
- Abdominal examination
- Promotion of institutional delivery
- Post-partum/postnatal care
B. Child Health Services
- Immunization (BCG, OPV, Hepatitis B, DPT/pentavalent, measles, etc.)
- Growth monitoring (weight, height/length recording)
- Growth chart plotting in the Mother and Child Protection (MCP) Card
- Detection and grading of malnutrition
- Vitamin A supplementation
- Management/referral of sick children
C. Family Planning Services
- Counselling and provision of contraceptives
- Promotion of spacing and limiting methods
D. Nutrition Services
- Supplementary nutrition (through AWW/ICDS)
- Nutrition counselling
- Promotion of breastfeeding and complementary feeding (IYCF)
- Health and nutrition education (IEC)
E. Other Services
- ORS distribution for diarrhoea management
- Completion and maintenance of the Mother and Child Protection (MCP) Card
- Health education to community
- ASHA incentive disbursement for beneficiaries brought to session
6. Key Personnel Involved (Convergence)
A major feature of VHND/Mamta Diwas is multi-sectoral convergence:
| Personnel | Role |
|---|---|
| ANM (HWF) | Primary organizer; conducts immunization, ANC, recording |
| ASHA | Mobilizes beneficiaries; brings mothers and children |
| AWW (Anganwadi Worker) | Provides venue (Anganwadi centre); assists with nutrition |
| Medical Officer (PHC) | Supervision; provides support |
| LHV (Health Assistant Female) | Supervisory support |
| HWM (Health Worker Male) | Assists in outreach |
| PRI (Panchayati Raj Institution) | Community mobilization, coordination |
| Self Help Groups (SHGs) | Community level mobilization |
As per Park's: "VHND should be organized at least once in a month in each village with the help of Medical Officer, Health Assistant Female (LHV) of PHC, HWM, HWF, ASHA, AWW and their supervisory staff, PRI, self help groups etc."
7. Mother and Child Protection (MCP) Card
The MCP Card is a joint card developed in collaboration with the Ministry of Women and Child Development (MoWCD) and used at Mamta Diwas sessions. It contains:
- Family identification and registration number
- Identifying data of the mother and child
- Birth record
- Pregnancy and antenatal care records
- Immunization record of the child
- Growth chart (for monitoring child's growth)
- Details of services received at each session
Park's states: "A Mother and Child Protection Card should be duly completed for every woman registered."
The new ICDS MCP Card came into use in 2009 (introduced during Pandemic Influenza A H1N1 era).
8. Monitoring & Supervision
- Coverage Monitoring Chart / Dropout Chart maintained at PHC
- AEFI (Adverse Events Following Immunization) to be reported
- Vaccine Preventable Disease (VPD) reporting
- District-level supervisory visits to Mamta Diwas sessions
- Meetings with PRI and ICDS functionaries about Mamta Diwas sessions
- Beneficiaries to wait at least 30 minutes post-vaccination to observe for AEFI
9. Relation to RMNCH+A Strategy
Mamta Diwas is a platform for delivering RMNCH+A services in a single-window approach:
- R - Reproductive health (family planning)
- M - Maternal health (ANC, PNC, safe delivery promotion)
- N - Newborn care (HBNC, newborn immunization)
- C - Child health (immunization, growth monitoring, nutrition)
- H - Health education
- +A - Adolescent health (life skills, ARSH services at VHND)
10. Key Exam Points (Memory Pearls)
| Point | Fact |
|---|---|
| Full name | Village Health and Nutrition Day (VHND) / Mamta Diwas / Health and Nutrition Day |
| Frequency | Once a month per village |
| Site | Anganwadi centre |
| Key organizer | ANM, with ASHA and AWW |
| Beneficiaries | Pregnant women + Breastfeeding women + Under-5 children |
| Programme | NHM / RCH-II / RMNCH+A |
| MCP Card | Jointly developed with Ministry of Women and Child Development |
| Key services | ANC, immunization, growth monitoring, nutrition, FP |
| Convergence | ANM + ASHA + AWW + PHC MO + PRI + SHG |
Sources:
- Park's Textbook of Preventive and Social Medicine - Village Health and Nutrition Day section (Block 7); NHM/RCH-II chapter (Block 6); Sub-centre services chapter (Block 12); Maternal and child health chapter (Block 8)
- National Journal of Community Medicine - Process Evaluation of Mamta Diwas, Kheda District, Gujarat (2013)

IMG_20260616_014823.jpg
Give answer in full detailed manner for psm exam from park
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here are full, detailed answers for all 8 questions from your question paper, directly from Park's Textbook of Preventive and Social Medicine:
Q26. Define Elimination Criteria for Leprosy. Types. Bacillary Leprosy. (10 marks)
Definition of Leprosy
Leprosy (Hansen's disease) is a chronic infectious disease caused by Mycobacterium leprae. It affects mainly the peripheral nerves. It also affects the skin, muscles, eyes, bones, testes and internal organs.
Cardinal features (any one or more):
- Hypopigmented patches
- Partial or total loss of cutaneous sensation in affected areas (earliest: loss of light touch)
- Presence of thickened nerves
- Presence of acid-fast bacilli in skin or nasal smears
Elimination Criteria for Leprosy
Elimination is defined as: Reduction of prevalence rate of leprosy to less than 1 case per 10,000 population at the national or sub-national level.
This is not eradication - it is defined as a public health problem ceasing to exist, not complete absence of the disease.
Key milestones:
- 1991: WHO member states resolved to eliminate leprosy globally by 2000
- India achieved national elimination in December 2005 (PR fell below 1/10,000)
- The fall in prevalence is attributed to: improved case management, very low relapse rates, high cure rates, absence of drug resistance, and shorter treatment duration with MDT
Indicators used for monitoring (WHO):
- Prevalence Rate (PR) - cases registered per 10,000 population (key elimination indicator)
- New Case Detection Rate (NCDR) - now considered more important than PR for programme monitoring
- Treatment Completion Rate - calculated annually by states
- Grade 2 Disability Rate among new cases - reflects delay in diagnosis
- Proportion of child cases among new cases - reflects ongoing transmission
Classification / Types of Leprosy
A. Ridley-Jopling Classification (Immunological)
| Type | Abbreviation | Bacillary Load | CMI | Features |
|---|---|---|---|---|
| Tuberculoid | TT | Very few | High | 1-2 well-defined hypopigmented patches, loss of sensation, thickened nerve |
| Borderline Tuberculoid | BT | Few | Moderate-high | Few plaques, some loss of sensation |
| Mid-Borderline | BB | Moderate | Moderate | Multiple lesions, "swiss cheese" appearance |
| Borderline Lepromatous | BL | Many | Moderate-low | Many lesions, partial loss of sensation |
| Lepromatous | LL | Very many | Very low/absent | Diffuse infiltration, nodules, leonine facies |
- Indeterminate (I): Earliest form - single hypopigmented patch, mildly impaired sensation, no nerve thickening; may heal spontaneously or progress
B. WHO / Field Classification (for MDT purposes)
| Type | Criteria | Treatment |
|---|---|---|
| Paucibacillary (PB) | 1-5 skin patches; smear negative | 6-month MDT |
| Multibacillary (MB) | >5 skin patches; or smear positive | 12-month MDT |
Bacillary Leprosy (Multibacillary / Lepromatous Leprosy)
Multibacillary (MB) leprosy includes LL, BL, BB types (and any smear-positive case).
Features of Lepromatous (LL) Leprosy:
- Represents the anergic end of the spectrum - deficient Cell Mediated Immunity (CMI)
- Widespread, symmetrical skin lesions - macules, papules, nodules, plaques
- Leonine facies - thickening and nodulation of facial skin
- Madarosis - loss of eyebrows (superciliary) and eyelashes (ciliary)
- Nasal stuffiness, epistaxis, nasal collapse (saddle nose)
- Glove-and-stocking anaesthesia (late finding)
- Bacillary index (BI) very high (5+ or 6+)
- NOT a localized disease - systemic involvement (testes causing gynaecomastia, orchitis)
- High infectivity
Pathogenesis:
- Bacilli enter through respiratory route
- Migrate to neural tissue, enter Schwann cells and macrophages
- If CMI is deficient: uncontrolled spread → MB leprosy with multiple system involvement
- If CMI is strong: PB leprosy or spontaneous healing
Treatment - Multibacillary MDT Regimen (WHO):
| Drug | Adult Dose | Frequency |
|---|---|---|
| Rifampicin | 600 mg | Once monthly, supervised |
| Clofazimine | 300 mg | Once monthly, supervised |
| Clofazimine | 50 mg | Daily, self-administered |
| Dapsone | 100 mg | Daily, self-administered |
- Duration: 12 months
- Each monthly blister pack = 1 supervised dose + 27 daily doses
- On completing 12 blister packs within 18 months = treatment completed
Q27. Disability Limitation and Medical Rehabilitation in Leprosy (6 marks)
WHO Disability Grading in Leprosy
| Grade | Eyes | Hands | Feet |
|---|---|---|---|
| 0 | No impairment | No impairment | No impairment |
| 1 | Anaesthesia present; no visible impairment | Anaesthesia present; no visible impairment | Anaesthesia present; no visible impairment |
| 2 | Visible impairment (lagophthalmos, corneal ulcer, opacity) | Visible deformity/damage (claw hand, ulcer, absorption) | Visible deformity/damage (plantar ulcer, foot drop, absorption) |
- The highest grade in any part = Disability Grade for that patient
- Eye + Hand + Feet score (0-12) recorded at each examination
Deformities Occurring in Leprosy
| Site | Deformities |
|---|---|
| Face | Leonine facies, lagophthalmos, loss of eyebrows (madarosis), corneal ulcers, depressed/perforated nose, nodules on ears |
| Hands | Claw hand, wrist drop, plantar ulcers, absorption of digits, thumb-web contracture, hollowing of interosseous spaces |
| Feet | Plantar ulcers, foot drop, inversion of foot, clawing of toes, absorption of toes, collapsed foot |
| Others | Gynaecomastia, perforation of palate |
Prevention of Disability (POD)
Measures include:
- Care of dry, denervated skin of palms and soles
- Healing wounds, ulcers, skin cracks
- Preventing injuries to hands and feet by protective gloves and footwear
- Preventing joint stiffness in paralytic deformities
- Protecting eyes (lubricating drops, protective glasses)
- Periodic nerve function assessment (simple tests done in field)
- Improvement through prostheses, orthopaedic devices, corrective splints, corrective surgery
Medical Rehabilitation
WHO (Second Expert Committee) definition: "The physical and mental restoration, as far as possible, of all treated patients to normal activity, so that they may be able to resume their place in the home, society and industry."
Rehabilitation is an integral part of leprosy control. It must begin as soon as the disease is diagnosed.
Types of Rehabilitation:
- Preventive rehabilitation - early diagnosis and adequate treatment to prevent deformities; cheapest and surest form
- Medical rehabilitation - reconstructive surgery, physiotherapy, prostheses, splints
- Social rehabilitation - reintegration into family and society, combating stigma
- Vocational rehabilitation - training for alternative employment
Community-Based Rehabilitation (CBR):
WHO definition: "A strategy within general community development for the rehabilitation, equalization of opportunities and social inclusion of all people with disabilities, implemented through combined efforts of the people with disabilities themselves, their families, organizations and communities, and relevant governmental and non-governmental health, education, vocational, social and other services."
Key principle: "We should never allow dehabilitation to take place and afterwards take up the uphill task of rehabilitation" - Park's
Q28. CASE - Syndromic Approach in Sexually Transmitted Diseases (10 marks)
Definition of Syndromic Approach
The syndromic approach is a clinical management strategy where patients with STDs are diagnosed and treated on the basis of recognizable syndromes (a group of symptoms and clinical signs) rather than waiting for laboratory confirmation.
Rationale / Advantages
- Most STD patients present with symptoms that can be grouped into syndromes
- Lab facilities are often not available in peripheral areas
- Avoids delay in treatment
- Cost-effective
- Reduces transmission by immediate treatment
- Addresses the problem of co-infections (e.g., dual gonorrhoea + chlamydia)
Recognised STD Syndromes (NACO Guidelines)
- Urethral discharge (in males)
- Vaginal discharge (in females)
- Genital ulcer disease
- Inguinal bubo
- Scrotal swelling
- Lower abdominal pain (in females - Pelvic Inflammatory Disease/PID)
- Neonatal conjunctivitis
Flowcharts - Syndromic Management
1. Urethral Discharge (Males)
Causative organisms: Neisseria gonorrhoeae, Chlamydia trachomatis
Treatment (dual coverage):
- Tab. Cefixime 400 mg orally, single dose PLUS
- Tab. Azithromycin 1 g orally, single dose (supervised)
- If symptoms persist/recur after 7 days: add Secnidazole 2 g (for Trichomonas)
- If allergy to Azithromycin: Erythromycin 500 mg QID x 7 days
Partner management: Treat all recent female partners; advise abstinence; provide condoms; refer for VCT (HIV, syphilis, Hepatitis B); return visit at 7 days
2. Vaginal Discharge (Females)
Causative organisms: N. gonorrhoeae, C. trachomatis, T. vaginalis, Bacterial vaginosis (Gardnerella), Candida albicans
Treatment:
- Cover gonorrhoea + chlamydia + BV + trichomoniasis simultaneously
- Tab. Cefixime + Azithromycin + Secnidazole + Fluconazole (depending on risk assessment)
3. Genital Ulcer Disease
Causative organisms: Treponema pallidum (syphilis), Haemophilus ducreyi (chancroid), HSV
Treatment:
- Benzathine Penicillin 2.4 MU IM (syphilis) PLUS
- Azithromycin 1 g single dose / Ciprofloxacin 500 mg BD x 3 days (chancroid) PLUS
- Acyclovir 400 mg TDS x 7 days (herpes)
4. Lower Abdominal Pain / PID
- Covers gonorrhoea, chlamydia, anaerobes
- Cefixime + Doxycycline + Metronidazole
Components of Each Syndromic Management Visit (5 Cs)
- Compliance - ensure full treatment
- Counselling - risk reduction, behaviour change
- Condom promotion and provision
- Contact tracing - partner notification and treatment
- Check-up - follow-up visit
Q29. Prevention of STDs (10 marks)
Primary Prevention
A. Health Education and Behaviour Change
- Education about modes of transmission and risk behaviours
- Promotion of safer sexual practices: abstinence, mutual fidelity (being faithful to one uninfected partner - "ABC": Abstain, Be faithful, use Condom)
- Delay of sexual debut in adolescents
- Reduction in number of sexual partners
- Avoidance of high-risk sexual behaviours
B. Condom Promotion
- Correct and consistent use of male condoms provides highly effective protection
- Female condom - also effective
- Social marketing of condoms
- Free distribution through health facilities, NGOs
C. Treatment of Existing STDs
- Treating STDs reduces HIV transmission (STIs increase HIV susceptibility 3-fold or more)
- Early and complete treatment of all STDs
D. Targeted Interventions for High-Risk Groups
- Sex workers, long-distance truck drivers, intravenous drug users (IDUs), MSM (men who have sex with men), migrants
- Peer-led outreach, frequent STD screening, condom promotion
E. Blood Safety
- Screening of all blood and blood products for HIV, HBV, HCV, syphilis
- Avoidance of unnecessary transfusions
F. Safe Injection Practices
- Use of sterile/disposable needles and syringes
- Needle exchange programmes for IDUs
G. Prevention of Mother-to-Child Transmission (PMTCT)
- Antenatal screening for syphilis, HIV, HBV
- Treatment of infected pregnant women
- Safe delivery practices
H. Male Circumcision
- Reduces risk of HIV acquisition in men by ~60%
I. Vaccines
- Hepatitis B vaccine - highly effective, included in UIP
- HPV vaccine - against HPV types 16, 18 (causes 70% of cervical cancers) and types 6, 11 (genital warts)
Secondary Prevention
- Early case detection through screening programmes
- Prompt and complete treatment
- Partner notification and treatment (contact tracing)
- Syndromic management at peripheral level
Tertiary Prevention
- Prevention of complications (PID, infertility, cervical cancer)
- Rehabilitation of patients with severe STD complications
Q30. Prevention of HIV/AIDS (6 marks)
Prevention at Individual Level (Primary)
A. Behaviour Change (ABC Strategy)
- A - Abstinence from sex
- B - Be faithful to one uninfected partner
- C - Condom - correct and consistent use
B. Harm Reduction in IDUs
- Needle exchange / syringe exchange programmes
- Opioid substitution therapy (methadone, buprenorphine)
- Never share needles, syringes, drug paraphernalia
C. Pre-Exposure Prophylaxis (PrEP)
- Daily oral antiretroviral drugs (Tenofovir + Emtricitabine) in HIV-negative high-risk individuals
- Reduces HIV acquisition by >90%
D. Post-Exposure Prophylaxis (PEP) - see Q31
Prevention at Community/Programme Level
E. Blood Safety
- Mandatory screening of all blood/blood products for HIV
- Avoidance of unnecessary transfusions
- Promote voluntary blood donation
F. PMTCT (Prevention of Mother-to-Child Transmission)
- Universal HIV testing in ANC
- Option B+: All HIV+ pregnant women started on lifelong ART regardless of CD4 count
- Safe delivery (minimize obstetric trauma, avoid unnecessary episiotomy, avoid mixed feeding)
- Replacement feeding or exclusive breastfeeding (with ARV prophylaxis for the baby)
- ART for the infant (Nevirapine for 6 weeks)
G. Early Treatment = Prevention (Treatment as Prevention - TasP)
- ART reduces viral load to undetectable → Undetectable = Untransmittable (U=U)
- Universal Test and Treat (UTT) strategy
H. Targeted Interventions (TI)
- For high-risk groups: sex workers, truck drivers, IDUs, MSM
- Condom promotion, STI treatment, peer education
I. NACP (National AIDS Control Programme)
- Condom promotion and distribution
- Targeted interventions
- Blood safety programme
- ICTC (Integrated Counselling and Testing Centres)
- ART centres
Q31. Post-Exposure Prophylaxis (PEP) of HIV (6 marks)
Definition
PEP is the short-term use of antiretroviral drugs after a potential exposure to HIV to prevent infection.
When to Give PEP
Indications:
- Occupational exposure: needlestick injuries, cuts with sharp instruments, splashes to mucous membrane or broken skin with blood/body fluids of HIV+ or unknown status patient
- Non-occupational exposure: unprotected sexual intercourse (consensual or assault), sharing needles with HIV+ person
When NOT to give PEP
- Exposure more than 72 hours ago (ideally start within 2 hours; must start within 72 hours)
- Exposure to urine, saliva, tears, sweat (unless blood-stained)
- Source confirmed HIV-negative
Risk Assessment
| Type of Exposure | Approximate Risk per Exposure |
|---|---|
| Needlestick injury | 0.3% |
| Mucous membrane splash | 0.09% |
| Receptive anal intercourse | 0.1-3% |
| Receptive vaginal intercourse | 0.1-0.2% |
PEP Regimen (Preferred)
Tenofovir (TDF) 300 mg + Lamivudine (3TC) 300 mg + Dolutegravir (DTG) 50 mg once daily x 28 days
(Older regimens used Zidovudine + Lamivudine ± Lopinavir/ritonavir)
Duration
- 28 days (4 weeks)
Management Steps After Exposure
- Wound care - wash with soap and water; flush mucous membranes with water; do NOT squeeze wound
- Assess risk - type of exposure, source status
- Start PEP as soon as possible (within 2 hours, must be within 72 hours)
- Baseline testing - HIV ELISA, CBC, LFT, RFT, HBsAg, HCV
- Counselling - about PEP, side effects, adherence, safe sex during PEP
- Follow-up testing - HIV at 6 weeks, 3 months, 6 months
- Report exposure to infection control team
Q32. Emerging and Re-emerging Infectious Diseases (10 marks)
Definitions
Emerging infectious diseases (EIDs): Infections that have newly appeared in a population, or have existed but are rapidly increasing in incidence or geographic range.
Re-emerging infectious diseases: Previously known infections that have declined in the past but are now showing increasing incidence or have appeared in a new geographic location.
Examples
Emerging Infections
| Disease | Pathogen | Year/Period |
|---|---|---|
| HIV/AIDS | HIV | 1981 onwards |
| SARS | Coronavirus (SARS-CoV-1) | 2002-03 |
| MERS | MERS-CoV | 2012 onwards |
| COVID-19 | SARS-CoV-2 | 2019 onwards |
| Ebola | Ebola virus | 1976; major outbreak 2014-16 |
| Nipah virus | Nipah virus | 1999; India 2018 |
| Zika virus | Zika flavivirus | Major outbreak 2015-16 |
| Hendra virus | Hendra virus | 1994 |
| Avian Influenza | H5N1, H7N9 | 1997 onwards |
| Monkeypox (Mpox) | Monkeypox virus | Outbreak 2022 |
Re-emerging Infections
| Disease | Reason for Re-emergence |
|---|---|
| Tuberculosis | HIV co-infection, MDR/XDR-TB, population movement |
| Malaria | Drug resistance (chloroquine, artemisinin), insecticide resistance |
| Dengue | Urbanization, spread of Aedes aegypti, travel |
| Cholera | El Tor variant, conflict zones |
| Plague | Natural foci reactivation |
| Yellow fever | Decline in vaccination coverage |
| Diphtheria | Vaccine programme lapse |
| Measles | Anti-vaccine movements |
Factors Contributing to Emergence / Re-emergence
| Factor | Examples |
|---|---|
| Ecological changes | Deforestation, agricultural development, flooding |
| Human demographics | Urbanization, overcrowding, slums |
| International travel | Rapid global spread of pathogens |
| Technology and industry | Blood products (HIV), organ transplantation |
| Microbial adaptation | Antibiotic resistance, antigenic shift/drift |
| Breakdown of public health | Vaccine hesitancy, poor surveillance |
| Animal-human interface | Zoonotic spillover (wet markets, bushmeat) |
| Climate change | Altered vector distribution (dengue, malaria) |
| Immunosuppression | HIV, immunosuppressive therapy |
Control Measures
- Surveillance - robust global/national surveillance systems (IHR 2005 - International Health Regulations)
- Early detection and rapid response
- One Health approach - integrated human, animal, environmental health
- Vector control for vector-borne diseases
- Vaccine development - platform technologies (mRNA vaccines)
- Infection control in healthcare settings
- International cooperation - WHO, Global Health Security Agenda (GHSA)
- Risk communication and community engagement
Q33. Nosocomial Infections / Hospital-Acquired Infections (6/10 marks)
Definition
Nosocomial infection (Hospital-Acquired Infection / HAI): An infection occurring in a patient during the process of care in a hospital or other healthcare facility, that was not present or incubating at the time of admission.
- WHO definition: An infection acquired in hospital by a patient who was admitted for a reason other than that infection.
- Onset: usually after 48 hours of hospital admission (or after 30 days of a surgical procedure)
Magnitude
- Affects 5-15% of hospitalized patients globally
- One of the leading causes of morbidity and mortality in hospitals
- Common in ICUs, surgical wards, neonatal units
Types / Most Common Sites
| Type | Common pathogens |
|---|---|
| Urinary tract infections (UTIs) - most common (~40%) | E. coli, Klebsiella, Pseudomonas (mostly catheter-associated) |
| Surgical site infections (SSI) - 2nd most common | Staph. aureus, streptococci, E. coli |
| Pneumonia / Lower respiratory tract | Gram-negative rods, Staph. aureus (especially ventilator-associated) |
| Bloodstream infections (BSI/Septicaemia) | Staph. aureus (MRSA), Candida, Enterococcus |
| Gastrointestinal infections | C. difficile (post-antibiotic diarrhoea) |
Routes of Transmission
- Contact transmission (most common) - direct or indirect contact with infected patient or contaminated surfaces/instruments
- Droplet transmission - large droplets from coughing/sneezing
- Airborne transmission - TB, measles, chickenpox, Aspergillus
- Common vehicle - contaminated food, water, IV fluids, medications
- Vector-borne - mosquitoes (rare in hospital setting)
Risk Factors
Host factors:
- Extremes of age (very young/old)
- Immunosuppression (HIV, steroids, chemotherapy)
- Underlying chronic diseases (diabetes, CKD)
- Malnutrition
Procedure-related factors:
- Urinary catheterization (CAUTI)
- Intravenous lines/central catheters (CLABSI)
- Mechanical ventilation (VAP)
- Surgical procedures
- Organ transplantation
Environmental factors:
- Overcrowding
- Poor hand hygiene compliance
- Inadequate sterilization/disinfection
- Inappropriate antibiotic use → MRSA, VRE, carbapenem-resistant organisms
Prevention and Control (Bundle Approaches)
Standard Precautions (for all patients at all times):
- Hand hygiene - WHO 5 moments: before patient contact, before aseptic task, after body fluid exposure, after patient contact, after contact with patient surroundings
- PPE - gloves, gowns, mask, eye protection as required
- Safe handling of sharps (no recapping, puncture-resistant containers)
- Respiratory hygiene / cough etiquette
- Environmental cleaning and disinfection
- Proper waste management
- Safe injection practices
- Sterilization of patient-care equipment
Transmission-Based Precautions:
- Contact precautions - MRSA, VRE, C. difficile
- Droplet precautions - influenza, meningococcal disease
- Airborne precautions - TB (negative pressure rooms), measles
Specific Bundles:
| Bundle | Key components |
|---|---|
| CAUTI bundle | Avoid unnecessary catheter; use aseptic technique; use closed drainage system; maintain unobstructed flow; daily review for removal |
| CLABSI bundle | Hand hygiene; full barrier precautions during insertion; chlorhexidine skin antisepsis; optimal site selection; daily review for line removal |
| VAP bundle | Head-of-bed elevation 30-45°; daily sedation hold; DVT prophylaxis; oral care with chlorhexidine; weaning protocol |
| SSI bundle | Appropriate antibiotic prophylaxis; normothermia; glucose control; proper hair removal (clipping not shaving) |
Antimicrobial Stewardship:
- Rational antibiotic use to prevent emergence of MDR organisms
- De-escalation of antibiotics based on culture sensitivity
Surveillance:
- Regular monitoring of HAI rates (NNIS system)
- Infection Control Committee (ICC) in every hospital
- Infection Control Nurse (ICN) / Infection Control Officer (ICO)
All answers are from Park's Textbook of Preventive and Social Medicine (28th edition), Chapters on Leprosy (Chapter on Communicable Diseases), STDs, HIV/AIDS, Emerging Infections, and Hospital-Acquired Infections.
post exposure prophylaxis of HIV for psm exam
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I have all the content needed from Park's. Let me now compile the complete, exam-ready answer:
Post-Exposure Prophylaxis (PEP) of HIV
(From Park's Textbook of Preventive and Social Medicine)
1. Definition
PEP for HIV consists of a comprehensive set of services to prevent HIV infection developing in an exposed person, including:
- First aid care
- Counselling and risk assessment
- HIV testing and counselling
- Short-term provision of antiretroviral drugs (28 days)
- Support and follow-up
"PEP for HIV consists of a comprehensive set of services to prevent infection developing in an exposed person." - Park's
2. Types of PEP
| Type | Exposure Context |
|---|---|
| Occupational PEP (oPEP) | Healthcare workers - needlestick, sharps injury, splash |
| Non-occupational PEP (nPEP) | Sexual exposure, sharing needles, assault |
3. Principle / Rationale
- HIV does not immediately enter the bloodstream and seed systemic infection
- After exposure, virus replicates locally at the site of exposure and in regional lymph nodes before systemic dissemination
- This "window of opportunity" (estimated 24-72 hours) allows ARV drugs to prevent or abort infection if given promptly
- Therefore, PEP must be started as early as possible, ideally within 2 hours, and must be started within 72 hours
4. Risk of HIV Transmission per Exposure
| Type of Exposure | Approximate Risk |
|---|---|
| Blood transfusion (HIV+) | ~90% |
| Sharing needles / IDU | 0.67% |
| Receptive anal intercourse | 0.1-3% |
| Receptive vaginal intercourse | 0.1-0.2% |
| Insertive vaginal intercourse | 0.03-0.09% |
| Needlestick injury (healthcare) | 0.3% |
| Mucous membrane splash | 0.09% |
| Non-intact skin exposure | < 0.09% |
5. Eligibility Criteria for PEP
PEP SHOULD be offered to:
- All individuals with exposure that has potential for HIV transmission, initiated as early as possible, ideally within 72 hours
- Assessment based on HIV status of source whenever possible (also considers background prevalence and local epidemiology)
- Exposures warranting PEP include:
- Parenteral or mucous membrane exposure - sexual exposure, splashes to the eye, nose, oral cavity
- Body fluids posing HIV risk: blood, blood-stained saliva, breast milk, genital secretions, CSF, amniotic fluid, rectal/peritoneal/synovial/pericardial/pleural fluids
PEP is NOT required when:
a. The exposed individual is already HIV positive
b. The source is established to be HIV negative
c. Exposure to body fluids that do not pose significant risk: tears, non-blood-stained saliva, urine, sweat
Important: Assessment of the HIV status of the exposed individual should NOT be a barrier to initiating PEP. If HIV testing is not immediately available but risk is high - start PEP first, test later.
6. Time Window
| Time from Exposure | Action |
|---|---|
| 0-2 hours | Ideal time to start PEP (maximum efficacy) |
| Up to 72 hours | PEP can still be initiated |
| > 72 hours | PEP is NOT recommended (ineffective) |
The sooner, the better - every hour counts.
7. Immediate First Aid After Exposure
For needlestick / sharps injury:
- Wash the wound immediately with soap and running water
- Allow wound to bleed freely (do NOT squeeze/press wound to force bleeding)
- Apply antiseptic (povidone-iodine)
- Do NOT suck the wound
For splash to mucous membrane / eye:
- Flush with copious water or normal saline immediately
- For eye: flush with clean water or eye wash
8. PEP Regimen (As per Park's / WHO 2016 Guidelines)
Preferred 3-Drug Regimen (Adults and Adolescents):
Option 1 (Most Preferred):
Raltegravir (RAL) 400 mg PO twice daily + Tenofovir DF (TDF) 300 mg / Emtricitabine (FTC) 200 mg (Truvada) PO once daily
Option 2 (Once-daily alternative):
Dolutegravir (DTG) 50 mg once daily + Tenofovir DF (TDF) 300 mg / Emtricitabine (FTC) 200 mg once daily
- Duration: 28 days (4 weeks)
- Three-drug regimens are now recommended for all exposures regardless of severity
- 2-drug regimens: only when recommended ARVs unavailable or concern about adherence/toxicity (require expert consultation)
For Children < 10 years:
- LPV/r (Lopinavir/ritonavir) is the preferred third drug
- Age-appropriate alternatives: ATV/r, RAL, DRV, EFV, NVP
Special Consideration - Women of Childbearing Age:
- Pregnancy test before starting PEP
- If prescribed DTG: counsel to use effective contraception during PEP course
- Pregnant women on DTG: monitor for neural tube defects (especially if exposure in first trimester)
9. Complete PEP Protocol - Step by Step
| Step | Action |
|---|---|
| 1. Immediate first aid | Wash wound / flush eyes immediately |
| 2. Risk assessment | Type of exposure, source HIV status, time since exposure |
| 3. HIV test of exposed person | Baseline HIV test (ELISA/Rapid) - if reactive, do NOT give PEP |
| 4. Start PEP | As early as possible (within 72 hours) |
| 5. Baseline investigations | HIV, CBC, LFT, RFT, HBsAg, Anti-HCV, pregnancy test (if applicable) |
| 6. Counselling | Adherence, side effects, safe sex during PEP period |
| 7. Follow-up HIV testing | At 6 weeks, 3 months, 6 months post exposure |
| 8. Report | Report to infection control committee (occupational exposure) |
10. Counselling Points During PEP
- Importance of completing the full 28-day course (adherence)
- Common side effects of ARVs (nausea, fatigue, headache, diarrhoea)
- PEP is not 100% effective - still requires condom use during follow-up period
- Avoid blood donation, pregnancy, unprotected sex during PEP and until confirmed HIV negative
- Importance of follow-up HIV testing even if PEP completed
- Psychological support for the exposed person
11. Follow-Up HIV Testing Schedule
| Time | Test | Purpose |
|---|---|---|
| Baseline (Day 0) | HIV ELISA / Rapid test | Rule out pre-existing HIV infection |
| 6 weeks | HIV test | Detect early seroconversion |
| 3 months | HIV test | Standard window period |
| 6 months | HIV test | Final confirmation (for those on newer 4th gen assays, 3 months may suffice) |
12. Effectiveness of PEP
- When taken correctly and promptly, PEP reduces the risk of HIV infection by approximately 80% after exposure
- Efficacy depends on: time to initiation, adherence, duration of full 28-day course
- Not 100% effective - hence counselling on safe behaviour during follow-up is essential
13. PEP vs PrEP - Quick Comparison (Exam Favourite)
| Feature | PEP | PrEP |
|---|---|---|
| Full form | Post-Exposure Prophylaxis | Pre-Exposure Prophylaxis |
| Timing | AFTER exposure | BEFORE potential exposure |
| Indication | Known exposure event | Ongoing high-risk behaviour |
| Duration | 28 days | Ongoing (continuous daily) |
| Start time | Within 72 hours | Before any exposure |
| Drug | TDF/FTC + RAL or DTG | TDF + FTC (Truvada) |
| Target | Exposed HIV-negative person | High-risk HIV-negative person |
14. Key Exam Memory Points
| Point | Fact |
|---|---|
| Time window | Within 72 hours (ideally 2 hours) |
| Duration | 28 days |
| Preferred regimen | RAL or DTG + TDF/FTC |
| Duration of HIV follow-up | 6 months |
| PEP NOT indicated | Source HIV negative, exposed person HIV positive, exposure > 72 hours, non-risky body fluids |
| Preferred 3rd drug in children | LPV/r |
| PEP not barrier | HIV status of exposed person should NOT delay PEP |
| Effectiveness | Reduces risk by ~80% |
Source: Park's Textbook of Preventive and Social Medicine, Chapter on HIV/AIDS - Post-Exposure Prophylaxis section (Block 5, pages 403-404), WHO 2016 ARV guidelines.
Revised drug policy of malaria treatment
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed. Here is the complete, exam-ready answer:
Revised Drug Policy of Malaria Treatment (India - 2013)
From Park's Textbook of Preventive and Social Medicine
Key Principle of the Revised Drug Policy 2013
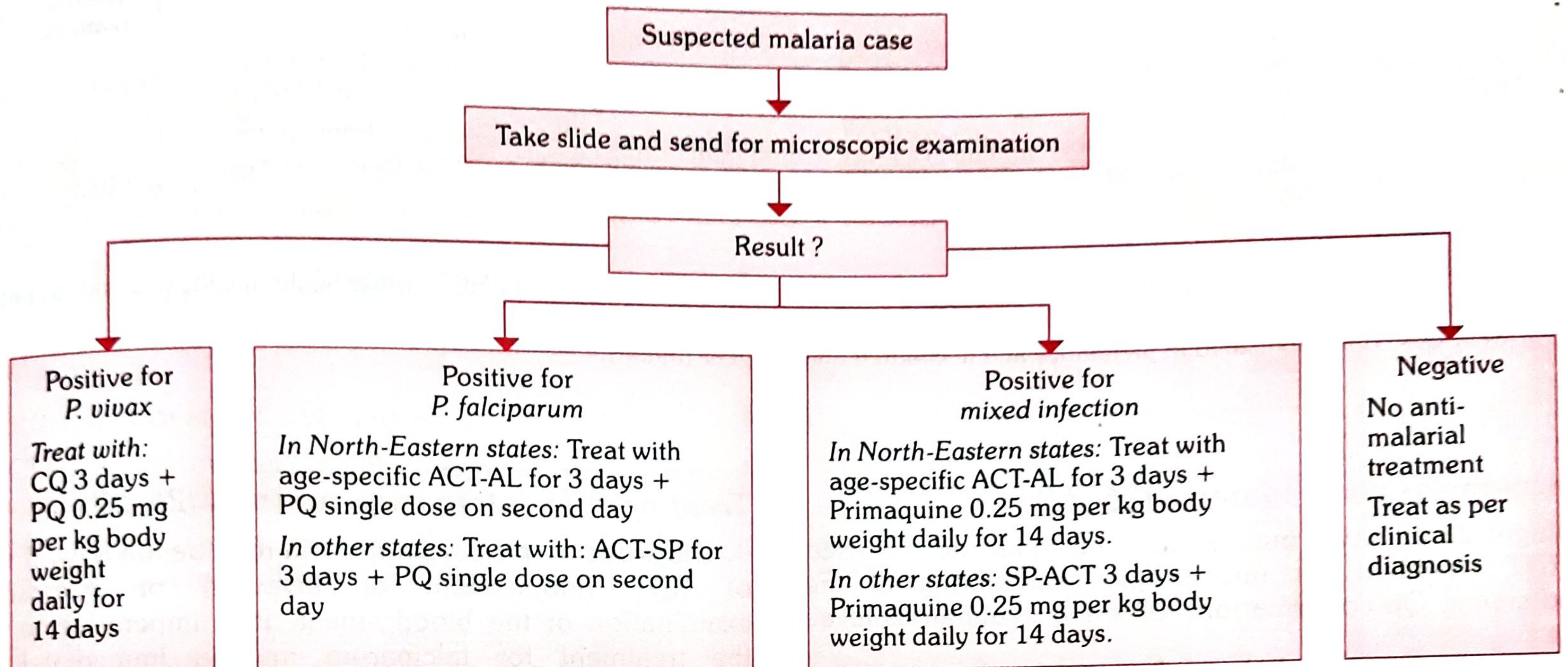
"According to the revised drug policy 2013, there is NO scope of presumptive treatment in malaria control."
- All fever cases must be confirmed by either microscopy or Rapid Diagnostic Test (RDT) before starting anti-malarial treatment
- This replaced the old policy of giving chloroquine empirically to all fever cases
- ACT (Artemisinin Combination Therapy) replaced chloroquine as first-line for P. falciparum
Diagnostic Flowchart (Fig. 2 from Park's)
I. Treatment of Uncomplicated P. vivax Malaria
Drugs:
1. Chloroquine (CQ): 25 mg/kg body weight, divided over 3 days
- Day 1: 10 mg/kg
- Day 2: 10 mg/kg
- Day 3: 5 mg/kg
2. Primaquine (PQ): 0.25 mg/kg/day for 14 days (for radical cure - to eliminate hypnozoites)
- Relapse rate in vivax malaria in India: ~30%
- 14-day regimen must be given under supervision
Primaquine Contraindications:
- Infants (children < 1 year)
- Pregnant women
- G6PD deficient individuals
Caution: In areas with high G6PD deficiency prevalence, screen before giving PQ. Warn patients to stop immediately if dark urine, yellow conjunctiva, bluish lips, abdominal pain, nausea/vomiting appear.
Dosage Chart - P. vivax Treatment:
| Age | Day 1 CQ (150 mg tab) | Day 1 PQ (2.5 mg tab) | Day 2 CQ | Day 2 PQ | Day 3 CQ | Day 4-14 PQ |
|---|---|---|---|---|---|---|
| < 1 year | ½ | 0 | ½ | 0 | ¼ | 0 |
| 1-4 years | 1 | 1 | 1 | 1 | ½ | 1 |
| 5-8 years | 2 | 2 | 2 | 2 | 1 | 2 |
| 9-14 years | 3 | 4 | 3 | 4 | 1½ | 4 |
| ≥ 15 years | 4 | 6 | 4 | 6 | 2 | 6 |
| Pregnancy | 4 | 0 | 4 | 0 | 2 | 0 |
(PQ contraindicated in pregnancy - only CQ given)
II. Treatment of Uncomplicated P. falciparum Malaria
A. Other States (All states except North-East):
ACT-SP regimen:
- Artesunate (AS): 4 mg/kg body weight/day for 3 days
- Sulfadoxine-Pyrimethamine (SP): Sulfadoxine 25 mg/kg + Pyrimethamine 1.25 mg/kg on Day 1 only
- Primaquine (PQ): 0.75 mg/kg body weight as single dose on Day 2 (gametocytocidal)
All tablets for the day to be taken together, swallowed with water.
Dosage Chart - P. falciparum (ACT-SP):
| Age (Years) | Colour | Day 1 AS | Day 1 SP | Day 2 AS | Day 2 PQ | Day 3 AS |
|---|---|---|---|---|---|---|
| 0-1 | Pink | 1 (25 mg) | 1 (250+12.5 mg) | 1 (25 mg) | Nil | 1 (25 mg) |
| 1-4 | Yellow | 1 (50 mg) | 1 (500+25 mg) | 1 (50 mg) | 1 (7.5 mg) | 1 (50 mg) |
| 5-8 | Green | 1 (100 mg) | 1 (750+37.5 mg) | 1 (100 mg) | 2 (7.5 mg) | 1 (100 mg) |
| 9-14 | Red | 1 (150 mg) | 2 (500+25 mg) | 1 (150 mg) | 4 (7.5 mg) | 1 (150 mg) |
| ≥ 15 | White | 1 (200 mg) | 2 (750+37.5 mg) | 1 (200 mg) | 6 (7.5 mg) | 1 (200 mg) |
B. North-Eastern States (NE States):
Due to SP resistance in NE states, the Technical Advisory Committee recommends:
ACT-AL: Co-formulated Artemether (20 mg) + Lumefantrine (120 mg)
| Weight/Age | Dose | Tablets | Pack colour |
|---|---|---|---|
| 5-14 kg (>5 months to <3 years) | 20/120 mg twice daily x 3 days | 1 tab BD x 3 days | Yellow |
| 15-24 kg (3-8 years) | 40/240 mg twice daily x 3 days | 2 tabs BD x 3 days | Green |
| 25-34 kg (9-14 years) | 60/360 mg twice daily x 3 days | 3 tabs BD x 3 days | Red |
| >34 kg (>14 years) | 80/480 mg twice daily x 3 days | 4 tabs BD x 3 days | White |
- Plus Primaquine 0.75 mg/kg single dose on Day 2
ACT-AL is NOT recommended:
- During 1st trimester of pregnancy
- Children weighing < 5 kg
IMPORTANT: Production and sale of Artemisinin monotherapy has been BANNED in India as it can lead to development of parasite resistance.
III. Treatment of P. falciparum in Pregnancy
| Trimester | Drug |
|---|---|
| 1st trimester | Quinine (ACT is NOT given in 1st trimester; Artemether-Lumefantrine also not recommended) |
| 2nd and 3rd trimester | ACT-SP (safe) |
Primaquine is CONTRAINDICATED in ALL trimesters of pregnancy.
IV. Treatment of Mixed Infections (P. falciparum + P. vivax)
- Mixed infections with P. falciparum should be treated as P. vivax malaria:
- NE states: ACT-AL for 3 days + Primaquine 0.25 mg/kg/day for 14 days
- Other states: ACT-SP for 3 days + Primaquine 0.25 mg/kg/day for 14 days
V. Treatment Failure / Drug Resistance
- Resistance suspected if: despite full treatment (no vomiting/diarrhoea), patient does not respond within 72 hours clinically and parasitologically
- Cases not responding to ACT: treat with Quinine + Tetracycline/Doxycycline (oral)
- Such cases must be reported to District Malaria Officer / State Malaria Officer / ROHFW for initiation of therapeutic efficacy studies
VI. Treatment of Severe / Complicated Malaria
Features of Severe Malaria (any one):
- Impaired consciousness / coma (Cerebral malaria)
- Repeated generalized convulsions
- Renal failure (Serum Creatinine > 3 mg/dl)
- Jaundice (Serum Bilirubin > 3 mg/dl)
- Severe anaemia (Hb < 5 g/dl)
- Pulmonary oedema / ARDS
- Hypoglycaemia (Plasma glucose < 40 mg/dl)
- Metabolic acidosis
- Circulatory collapse / shock (SBP < 80 mmHg; < 50 mmHg in children)
- Abnormal bleeding / DIC
- Haemoglobinuria
- Hyperthermia (> 106°F / 42°C)
- Hyperparasitaemia (> 5% parasitized RBCs in low endemic; > 10% in hyperendemic areas)
Treatment of Severe Malaria:
Step 1: Initial Parenteral Treatment (minimum 48 hours) - choose ONE:
| Drug | Dose |
|---|---|
| Quinine | 20 mg/kg body weight IV infusion on admission (loading dose), then 10 mg/kg 8-hourly; infusion rate ≤ 5 mg/kg/hr |
| Artesunate | 2.4 mg/kg IV or IM at 0 h, 12 h, 24 h, then once daily |
| Artemether | 3.2 mg/kg IM on admission, then 1.6 mg/kg/day |
| Arteether | 150 mg IM daily for 3 days (adults only, NOT for children) |
Parenteral treatment must be given for minimum 24 hours once started, irrespective of patient's ability to take oral medicine.
Step 2: Follow-up Oral Treatment (once patient can swallow):
- After parenteral Quinine: Oral Quinine 10 mg/kg TDS + Doxycycline 100 mg OD (or Clindamycin in pregnant women/children < 8 yrs) to complete 7 days total
- After parenteral Artemisinin derivative: Full oral course of area-specific ACT for 3 days
Special Note - Severe Malaria in Pregnancy:
- Pregnant women with severe malaria in any trimester can be treated with artemisinin derivatives (unlike uncomplicated malaria in 1st trimester)
- Artemisinin, unlike quinine, does not aggravate hypoglycaemia
"Don'ts" in Severe Malaria:
- Do NOT use corticosteroids
- Do NOT give IV mannitol
- Do NOT use heparin as anticoagulant
- Do NOT administer adrenaline
- Do NOT overhydrate
- Do NOT use mefloquine in cerebral malaria (risk of neuropsychiatric complications)
VII. Summary Table - Revised Drug Policy 2013 at a Glance
| Species | Condition | Drug(s) | Duration |
|---|---|---|---|
| P. vivax | Uncomplicated | CQ 25 mg/kg over 3 days + PQ 0.25 mg/kg/day | CQ: 3 days, PQ: 14 days |
| P. falciparum | Uncomplicated (other states) | ACT-SP + PQ single dose Day 2 | AS: 3 days, SP: Day 1 only |
| P. falciparum | Uncomplicated (NE states) | ACT-AL + PQ single dose Day 2 | 3 days |
| P. falciparum | Pregnancy 1st trimester | Quinine (no ACT) | 7 days |
| P. falciparum | Pregnancy 2nd/3rd trimester | ACT-SP | 3 days |
| Mixed | Uncomplicated | Treat as P. vivax (ACT + PQ 14 days) | - |
| Severe malaria | Any species | Parenteral: Artesunate / Artemether / Arteether / Quinine | Min 24-48 hr parenteral, then oral |
VIII. Key Exam Points to Remember
| Point | Fact |
|---|---|
| Revised drug policy year | 2013 |
| Key change | No presumptive treatment; only after confirmed diagnosis (RDT/microscopy) |
| P. vivax first-line | Chloroquine + Primaquine 14 days |
| P. falciparum first-line (other states) | ACT-SP (Artesunate + S-P) + PQ single dose Day 2 |
| P. falciparum NE states | ACT-AL (Artemether + Lumefantrine) + PQ |
| Why ACT-AL in NE states? | SP resistance |
| PQ dose in P. vivax (radical cure) | 0.25 mg/kg/day x 14 days |
| PQ dose in P. falciparum (gametocytocidal) | 0.75 mg/kg single dose on Day 2 |
| PQ contraindications | Infants, pregnant women, G6PD deficiency |
| Pf in pregnancy 1st trimester | Quinine |
| Pf in pregnancy 2nd/3rd trimester | ACT-SP |
| Banned in India | Artemisinin monotherapy |
| Severe malaria preferred parenteral drug | Artesunate IV/IM (or Artemether, Arteether, Quinine) |
| Avoid in cerebral malaria | Mefloquine (neuropsychiatric side effects) |
| Don't give in severe malaria | Corticosteroids, mannitol, heparin, adrenaline |
Source: Park's Textbook of Preventive and Social Medicine - "Guidelines for Diagnosis and Treatment of Malaria in India - 2013" (Block 4, pages 307-312), based on National Drug Policy for Malaria 2013, Ministry of Health and Family Welfare, Government of India.
NACP
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Acculturation for psm exam
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Kangaroo mother care for psm exam
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching the Web
WHO Kangaroo Mother Care guidelines 2022 components benefits PSM
I now have comprehensive content from Park's and WHO guidelines. Here is the complete, exam-ready answer:
Kangaroo Mother Care (KMC)
From Park's Textbook of Preventive and Social Medicine + WHO Guidelines
1. Introduction / Historical Background
- KMC was introduced in Bogota, Colombia in 1979 by Drs. Hector Martinez and Edgar Rey
- It was developed as a response to:
- High infection and mortality rates in neonates
- Overcrowding in hospitals
- Shortage of incubators
- Has since been adopted across the developing world and has become an essential element in the continuum of neonatal care
"Kangaroo mother care for low birth-weight babies was introduced in Colombia in 1979 by Drs. Hector Martinez and Edzar Rey as a response to, inter alia, high infection and mortality rates due to overcrowding in hospitals." - Park's
2. Definition
Kangaroo Mother Care (KMC) is a method of care for low birth-weight (LBW) and preterm newborns that involves:
- Early and continuous skin-to-skin contact between the newborn and mother (or father/caregiver)
- Exclusive breastfeeding/breast milk feeding support
- Ambulatory / early discharge from hospital
- Supportive care to the mother and family
WHO defines KMC as: "A package of early and continuous skin-to-skin contact, breast-feeding support, and supportive care in stable newborns weighing less than 2000 grams."
3. Target Beneficiaries
- All low birth-weight (LBW) babies - birth weight < 2500 g
- Preterm babies - gestational age < 37 weeks
- Especially effective for very low birth weight babies (birth weight 1000-1799 g)
- Can be practiced even at home - thus improving chances of newborn survival
4. Four Components of KMC (PARK'S)
Park's clearly states: "The four components of kangaroo mother care are all essential for ensuring the best care option, especially for low birth-weight babies."
| Component | Details |
|---|---|
| 1. Skin-to-skin positioning | Baby placed in upright position on mother's bare chest, between the breasts; baby's head turned to one side; baby's hips flexed in "frog-leg" position |
| 2. Adequate nutrition | Exclusive breastfeeding or expressed breast milk; direct breastfeeding promoted whenever baby can suck |
| 3. Ambulatory care | Earlier discharge from hospital; mother carries baby at home; monitoring done on ambulatory basis |
| 4. Support for mother and family | Education, counselling, and support for the mother and family to care for the baby at home |
5. How to Practice KMC - Position
- Baby is placed upright (vertical position) against the mother's chest
- Baby is between mother's breasts, with head turned to one side
- Baby's neck is slightly extended (to keep airway open)
- Hips are flexed (frog-leg position) and abdomen at mother's epigastric level
- Baby is secured using a wrap/cloth/binder
- Mother can move around with baby attached
- Duration: As long and as continuous as possible (ideally 24 hours/day, with breaks for hygiene and feeding)
6. When to Start KMC
- Can start as soon as the newborn is clinically stable
- Immediate KMC (started immediately after birth) is now recommended by WHO 2022 for stable preterm/LBW newborns even before full stabilization
- In India under NACP/NHM: KMC is recommended at the health facility level as an Essential (E) intervention
7. Benefits of KMC
A. Benefits to the Baby
| System | Benefit |
|---|---|
| Thermoregulation | Prevents hypothermia; maintains body temperature through maternal body heat |
| Respiration | Improved cardiac and respiratory stability; reduces apnea episodes |
| Nutrition | Promotes breastfeeding; better weight gain |
| Infection | Reduces nosocomial/hospital-acquired infections |
| Neurological | Reduces pain and stress; more organized sleep patterns; better neurodevelopment |
| Mortality | Reduces mortality in LBW babies by up to 40% (Cochrane review 2016) |
| Growth | Faster weight gain; earlier discharge |
B. Benefits to the Mother
- Promotes mother-newborn bonding and attachment
- Reduces maternal anxiety and depression
- Promotes and prolongs breastfeeding
- Boosts mother's confidence in caring for her newborn
- Empowers mother as primary caregiver
- May reduce postpartum haemorrhage
C. Benefits to Health Facility / System
- Reduces dependence on incubators (especially in resource-poor settings)
- Shorter hospital stay - earlier discharge
- Cost-effective - significant cost savings
- Less need for additional nursing staff
- Reduces overcrowding in NICUs
8. KMC vs Conventional (Incubator) Care
| Feature | Incubator Care | KMC |
|---|---|---|
| Temperature control | Mechanical | Maternal body heat |
| Cost | High | Minimal |
| Infection risk | Higher (nosocomial) | Lower |
| Bonding | Reduced | Enhanced |
| Breastfeeding | Difficult | Promoted |
| Availability | Only in hospital | At home too |
| Monitoring | Continuous by machines | By mother + periodic check |
9. KMC under India's National Programmes
Under NHM / RMNCH+A:
- KMC is listed as an Essential (E) intervention at the health facility level for care of small and sick newborns
- Part of India Newborn Action Plan (INAP)
Facility-based care continuum (from Park's block 7):
- Thermal care and feeding support (community)
- IMNCI and oral antibiotics (sub-centre)
- Injectable Gentamicin by ANMs (pre-referral)
- KMC at facility (Health Facility) - Essential
- Full supportive care at block (NBSU) and district level (SNCU)
- NICU services at regional level
Under NHM interventions to reduce neonatal mortality (Park's):
- "Newer interventions to reduce newborn mortality: vitamin K injection at birth, antenatal corticosteroids for preterm labour, kangaroo mother care and injection gentamicin to young infants in cases of suspected sepsis."
Under Sub-centre / CHC services (Park's):
- Essential newborn care includes: "provision of warmth / Kangaroo Mother Care (KMC), maintain the airway and breathing, initiate breastfeeding within one hour, infection protection, cord care and identification of sick newborn and prompt referral."
10. WHO 2022 Updated Recommendations
- WHO updated KMC recommendations in 2022
- Immediate KMC (initiated immediately or very soon after birth, even before stabilization) is now recommended for all preterm (<37 weeks) or LBW (<2500g) newborns requiring specialized care
- KMC should be provided as soon as possible and continued for as long as possible
- Can be practiced by father or other family members (not just mother) - also called "Kangaroo Father Care"
11. Intensive Care for LBW Babies (Park's - alongside KMC)
Park's also describes conventional intensive care for LBW babies as comprising:
(a) Incubator care:
- Adjustment of temperature, humidity, oxygen supply
- Continuous monitoring of oxygen levels in blood (to prevent hypoxia → cerebral palsy)
- Excess oxygen may lead to retrolental fibroplasia (ROP)
(b) Feeding:
- Breastfeeding promoted; breast milk used if available
- Feeding may be by nasal catheter if baby cannot suck
(c) Prevention of infection:
- Infection is the greatest hazard in LBW babies
- Death may occur within hours following respiratory infection
Leading Causes of Death in LBW Babies (Park's):
- Atelectasis
- Malformation
- Pulmonary haemorrhage
- Intracranial bleeding (secondary to anoxia or birth trauma)
- Pneumonia and other infections
12. Key Exam Points to Remember
| Point | Fact |
|---|---|
| Introduced by | Drs. Hector Martinez and Edgar Rey |
| Year & Place | 1979, Bogota, Colombia |
| Target babies | LBW (< 2500 g) and preterm (< 37 weeks); WHO 2022: < 2000 g for KMC |
| Four components | Skin-to-skin contact + Breastfeeding + Ambulatory care + Family support |
| Position | Upright/vertical, chest-to-chest, frog-leg position |
| Key benefit | Reduces LBW mortality by 40% |
| Temperature benefit | Prevents hypothermia |
| Infection benefit | Reduces nosocomial infections |
| Programme link | NHM, RMNCH+A, India Newborn Action Plan (INAP) |
| Level in health system | Essential at health facility level |
| WHO update | 2022 - recommended immediate KMC even before full stabilization |
| Excess oxygen hazard | Retrolental fibroplasia (ROP) |
| Can be done at | Home (not just hospital) |
Source: Park's Textbook of Preventive and Social Medicine - Kangaroo Mother Care section (Block 8, p. ~480); Child Health / RMNCH+A section (Block 7); NHM section (Block 6); Sub-centre services (Block 12); WHO Kangaroo Mother Care Guidelines 2022.
It's too long, including main points only
Kangaroo Mother Care (KMC)
Definition
A method of care for LBW/preterm newborns involving early and continuous skin-to-skin contact, breastfeeding support, and supportive care in stable newborns weighing < 2000 g.
Origin
- Introduced in Bogota, Colombia, 1979
- By Drs. Hector Martinez & Edgar Rey
- Developed due to high neonatal mortality and shortage of incubators
Four Components (Park's)
- Skin-to-skin positioning - baby upright on mother's bare chest
- Breastfeeding / breast milk - exclusive, as early as possible
- Ambulatory / early discharge - mother carries baby at home
- Support for mother and family - education and counselling
Who Benefits
- All LBW babies (< 2500 g)
- Preterm babies (< 37 weeks)
- Can be practiced at home also
Benefits
| To Baby | To Mother |
|---|---|
| Prevents hypothermia | Promotes bonding |
| Reduces infections | Boosts breastfeeding |
| Better weight gain | Reduces anxiety |
| Reduces mortality by 40% | Empowers as caregiver |
Under India's Programmes
- Essential (E) intervention at health facility level under NHM / RMNCH+A
- Part of India Newborn Action Plan (INAP)
- Listed alongside Vitamin K, antenatal corticosteroids, Gentamicin as key interventions to reduce neonatal mortality
Key Exam Facts
| Point | Fact |
|---|---|
| Year & place | 1979, Colombia |
| Target weight | < 2000 g (WHO) / < 2500 g (LBW) |
| Position | Upright, chest-to-chest, frog-leg |
| Mortality reduction | 40% (Cochrane 2016) |
| WHO update | 2022 - immediate KMC even before stabilization |
| Excess O₂ hazard | Retrolental fibroplasia |
| Programme level | Essential at health facility |
Source: Park's PSM - Block 8 (KMC section) + Block 7 (RMNCH+A)


17821590226196617969450094896334.jpg
17821590309493201060030018283145.jpg
Give explanation of each question for psm exam
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here are all 12 questions answered concisely from Park's PSM (Environment & Health chapter):
Environment & Health - All 12 Questions
From Park's Textbook of Preventive and Social Medicine
Q1. Chlorination of Water (6/10 marks)
Definition
Chlorination is the process of adding chlorine to water for disinfection. It is a supplement, NOT a substitute to sand filtration.
Action of Chlorine
- Cl₂ + H₂O → HCl + HOCl (hypochlorous acid)
- HOCl → H⁺ + OCl⁻
- Hypochlorous acid is the active germicidal agent - 70-80 times more effective than hypochlorite ion
- Best action at pH 7; unreliable above pH 8.5
What Chlorine Kills/Does NOT Kill
| Kills | Does NOT kill |
|---|---|
| Pathogenic bacteria | Spores |
| Most pathogens | Certain viruses (polio, viral hepatitis) - except at high doses |
Secondary Properties of Chlorine
- Oxidizes iron, manganese, hydrogen sulphide
- Destroys taste and odour-producing substances
- Controls algae and slime
- Aids coagulation
Principles of Chlorination
- Water must be clear and free from turbidity (turbidity impedes chlorination)
- Chlorine demand of water must be satisfied first
- Free residual chlorine of 0.5 mg/litre must remain after 1 hour contact
- Sufficient contact time must be allowed
Methods of Chlorination
For large water supplies (urban):
- Chlorine gas - first choice; cheap, quick, efficient; applied using "chlorinating equipment" (Paterson's Chloronome)
- Chloramine - slower action; persistent residual; less taste; not widely used
- Perchloron (HTH) - 60-70% available chlorine
For small/emergency use:
- Bleaching powder, chlorine tablets, HTH solutions
Break-Point Chlorination
- Adding chlorine to water with ammonia produces chloramines (less efficient)
- As more chlorine is added, residual falls (chloramines destroyed)
- Then rises again - the point where residual reappears = "break point"
- Breakpoint chlorination = controlled superchlorination; all combined chlorine destroyed; only free chlorine remains
Superchlorination
- Addition of large doses of chlorine, followed by dechlorination
- Used for heavily polluted, variable-quality water
OT (Orthotolidine) Test
- Used to measure free and combined residual chlorine
- Turns yellow in presence of chlorine; intensity varies with concentration
Q2. Purification of Water at Small Scale (10 marks)
Three methods available individually or in combination:
(a) BOILING
- Water brought to rolling boil for 10-20 minutes
- Kills all bacteria, spores, cysts, ova → yields sterile water
- Removes temporary hardness (precipitates CaCO₃)
- Disadvantage: No residual protection against re-contamination; taste altered
- Store in the same container in which it was boiled
(b) CHEMICAL DISINFECTION
1. Bleaching Powder (CaOCl₂)
- White powder, pungent smell
- Contains ~33% available chlorine (freshly made)
- Unstable - loses chlorine on exposure to air, light, moisture
- Store in dark, cool, dry, closed, corrosion-resistant container
- Ensure free residual chlorine of 0.5 mg/L after 1 hour
2. Chlorine Solution
- Prepared from bleaching powder: 4 kg BP (25% Cl) + 20L water = 5% chlorine solution
- Store away from light
3. High Test Hypochlorite (HTH / Perchloron)
- 60-70% available chlorine
- More stable than bleaching powder
4. Chlorine Tablets (Halazone)
- Good for small quantities; costly
- NEERI tablet: 1 tablet (0.5 g) disinfects 20 litres
5. Iodine
- 2 drops of 2% iodine solution per litre of clear water
- Contact time: 20-30 minutes
- Used for emergency disinfection
(c) FILTRATION AT HOUSEHOLD LEVEL
- Sand/candle filters (Berkefeld, Chamberland filters)
- Removes turbidity and some bacteria
- Does NOT sterilize - still needs chemical disinfection
(d) SOLAR DISINFECTION (SODIS)
- PET bottles filled with clear water, placed in sunlight 6-8 hours
- UV rays and heat kill pathogens
Q3. Safe and Wholesome Water (6/10 marks)
Definition (Park's)
Water intended for human consumption should be both safe and wholesome:
- (a) Free from pathogenic agents
- (b) Free from harmful chemical substances
- (c) Pleasant to taste - free from colour and odour
- (d) Usable for domestic purposes
Water is polluted/contaminated when it does NOT fulfil these criteria.
Water Requirements
- Basic physiological minimum: 2 litres/person/day
- Urban domestic standard: 150-200 litres/capita/day
- India's rural target: 40 litres/capita/day
WHO/BIS Standards for Drinking Water
| Parameter | Acceptable limit |
|---|---|
| Turbidity | < 1 NTU (desirable), < 5 NTU (permissible) |
| pH | 6.5-8.5 |
| Coliform organisms | 0/100 mL (no coliforms permissible) |
| Dissolved oxygen | > 6 mg/L |
| Nitrates | < 45 mg/L |
| Fluoride | 0.6-1.2 mg/L |
| Arsenic | < 0.01 mg/L |
| Lead | < 0.01 mg/L |
| Residual chlorine | 0.2-0.5 mg/L |
Water-Related Diseases
- Waterborne - cholera, typhoid, hepatitis A, dysentery (water vehicle)
- Water-washed - trachoma, scabies (inadequate water for hygiene)
- Water-based - guinea worm, schistosomiasis (aquatic host)
- Water-related vector - malaria, dengue, filaria (vectors breed in water)
Q4. Surveillance of Drinking Water Quality (10 marks)
Definition
Systematic, continuous assessment and oversight of drinking water safety from source to consumer to protect public health.
Objectives
- Ensure drinking water meets quality standards at all times
- Early detection of deterioration in quality
- Identify sources of contamination
- Evaluate effectiveness of treatment processes
- Provide data for action
Components of Surveillance
1. Source Water Monitoring
- Quality of raw water (river, lake, groundwater) before treatment
2. Treatment Plant Monitoring
- Adequacy of each treatment step (coagulation, filtration, disinfection)
- Check residual chlorine after disinfection
3. Distribution System Monitoring
- Quality at various points in distribution network
- Check for cross-connections, leakages, back-siphonage
- Residual chlorine must be ≥ 0.2 mg/L at consumer's tap
4. Consumer End Monitoring
- Tap water testing at households
Water Quality Parameters Tested
- Physical: turbidity, colour, taste, odour, temperature
- Chemical: pH, dissolved oxygen, nitrates, fluoride, heavy metals, pesticides
- Bacteriological: total coliform, faecal coliform (E. coli), faecal streptococci
Bacteriological Tests
- MPN (Most Probable Number) - estimates coliform count per 100 mL
- Membrane filtration technique - most widely used
- Presence/absence test (P-A test) - for field use
Standard
- Zero coliforms per 100 mL of treated piped water
- E. coli: nil/100 mL
WHO Guidelines
- National surveillance should be independent of water supply authorities
- WHO recommends Water Safety Plans (WSPs) - risk assessment and risk management approach
Q5. Water Conservation (6 marks)
Definition
Protection, development, and efficient management of water resources to ensure adequate supply for present and future generations.
Why Needed?
- Freshwater constitutes only 2.5% of total water on earth
- Increasing demand due to population growth, urbanization, industrialization
- Climate change causing water scarcity
Methods of Water Conservation
1. Rainwater Harvesting
- Collection and storage of rainwater from rooftops, roads, open areas
- Recharges groundwater; reduces runoff
2. Watershed Management
- Conservation of soil and water in a catchment area
- Contour farming, check dams, afforestation
3. Reducing Wastage
- Repair of leaky pipes and taps in distribution systems
- About 30-40% of urban water is lost through leakages (non-revenue water)
4. Recycling and Reuse
- Treated sewage reused for irrigation, industrial cooling
- Greywater recycling for flushing
5. Efficient Irrigation
- Drip irrigation, sprinkler systems (reduce 30-60% water use vs flood irrigation)
6. Legislation
- Water Pollution Prevention Acts
- Regulation of groundwater extraction
7. Public Education
- Awareness campaigns on water conservation practices
Q6. Air Pollution (10 marks)
Definition (Park's)
"Presence in the ambient atmosphere of substances generated by activities of man in concentrations that interfere with human health, safety or comfort, or injurious to vegetation, animals and other environmental media."
Types of Air Pollutants
- Primary pollutants: Emitted directly from source (automobiles, industry) - CO, SO₂, NO₂, particulate matter
- Secondary pollutants: Formed within atmosphere by chemical reactions - Ozone, photochemical smog
- Gaseous: CO, SO₂, H₂S, NOx, ozone, hydrocarbons
- Particulate: Dust, smoke, soot, fly ash, aerosols
Sources of Air Pollution
- Automobiles - CO, hydrocarbons, lead, NOx, particulates
- Industries - SO₂, NOx, CO, fly ash, fluorides
- Domestic - coal, wood, oil burning → smoke, SO₂ (London disaster, 1952)
- Tobacco smoke - most direct source affecting individual health ("passive smoking")
- Miscellaneous - burning refuse, pesticide spraying, natural sources
Meteorological Factors
- Temperature inversion - cold air trapped below warm air; pollutants cannot disperse; leads to SMOG (common in winter)
- Wind, topography, humidity affect pollution levels
Major Pollutants and Effects
| Pollutant | Source | Health Effect |
|---|---|---|
| CO | Automobile exhaust | Binds Hb → carboxyhaemoglobinaemia; death |
| SO₂ | Power plants, smelters | Asthma, COPD exacerbation |
| NOx | Vehicles, gas stoves | Bronchiolitis, lung damage |
| Lead | Leaded petrol | Impaired neuropsychological development in children |
| Ozone | Photochemical smog | Cough, bronchoconstriction |
| Hydrocarbons | Vehicles, cigarettes | Lung cancer |
| Particulates (PM2.5) | Industries, vehicles | Deep lung penetration; lung cancer, COPD |
Health Effects of Air Pollution
- Immediate: acute bronchitis, suffocation (London fog 1952: thousands died)
- Delayed/Chronic: chronic bronchitis, lung cancer, bronchial asthma, emphysema, respiratory allergies
- Most vulnerable: elderly, children, smokers, chronic respiratory disease patients
Control of Air Pollution
- Substitution - replace coal with cleaner fuels (gas, electricity)
- Process changes - switch from leaded to unleaded petrol
- Treatment of waste gases - catalytic converters in vehicles, scrubbers in industries
- Dilution - tall chimneys, green belts between industrial and residential areas
- Legislation - The Air (Prevention and Control of Pollution) Act, 1981 (India); Clean Air Acts
- International action - WHO global air quality monitoring network
- Disinfection of air - mechanical ventilation, UV radiation (OT/wards), chemical mists (triethylene glycol)
Q7. Noise Pollution (10 marks)
Definition
Noise is defined as unwanted sound that is physiologically and psychologically harmful. It is measured in decibels (dB).
Sources of Noise
- Transportation - road traffic, aircraft, railways (major urban source)
- Industrial - factories, construction sites, drilling
- Domestic - TV, music systems, household appliances
- Social - loudspeakers, firecrackers, public gatherings
- Occupational - textile mills, metal workshops, airports
Measurement
- Decibel (dB) - unit of sound intensity
- dB(A) - A-weighted decibel scale (matches human ear response)
WHO Permissible Noise Levels
| Setting | Permissible Level |
|---|---|
| Residential areas (day) | 55 dB |
| Residential areas (night) | 45 dB |
| Hospital/school | 35-40 dB |
| Industry | 90 dB (8 hrs) |
Health Effects of Noise
Auditory effects:
- Noise-Induced Hearing Loss (NIHL) - most important; irreversible
- Temporary Threshold Shift (TTS) - temporary hearing loss after acute exposure; recovers with rest
- Permanent Threshold Shift (PTS) - irreversible after prolonged exposure
- Acoustic trauma - sudden intense noise (explosion)
Non-auditory effects:
- Cardiovascular: hypertension, increased heart rate, vasoconstriction
- Psychological: stress, irritability, anxiety, sleep disturbance, reduced concentration
- Performance: reduced work efficiency, decreased productivity
- Endocrine: increased cortisol, catecholamines
- Interference with communication
Control of Noise Pollution
- At source - use of silencers, mufflers, vibration dampers; engine redesign
- During transmission - sound-insulating materials (double glazed windows), noise barriers/walls along highways, green belts
- At receiver - ear muffs, ear plugs (most common occupational protection); limit exposure time
- Land use planning - industries, airports away from residential areas
- Legislation - Noise Pollution (Regulation and Control) Rules, 2000 (India)
- Education - awareness about harmful effects of noise
Q8. Radiation Hazards and Prevention (6/10 marks)
Types of Radiation
A. Ionizing Radiation (high energy - can ionize atoms)
- Alpha particles - low penetration; dangerous if inhaled/ingested
- Beta particles - moderate penetration; skin burns
- Gamma rays - high penetration; most dangerous externally
- X-rays - similar to gamma rays
- Neutrons - highly penetrating
B. Non-Ionizing Radiation (lower energy)
- Ultraviolet (UV) rays - from arc welding, sun
- Infrared rays - from molten metal, glass blowing, welding
- Microwaves, radiofrequency - mobile phones, radar
Sources of Occupational Exposure (Park's)
- Painting luminous dials (radium)
- Mining radioactive ores (uranium, monazite sand)
- X-ray use in medicine and industry
- Arc/electric welding (UV rays)
- Glass blowing, foundry work, welding (Infrared)
- Nuclear energy programmes
Health Effects
| Radiation Type | Effect |
|---|---|
| Ionizing (acute) | Burns, dermatitis, blood dyscrasias (leucopenia) |
| Ionizing (chronic) | Malignancies (lung cancer in uranium miners), genetic effects, leukaemia, cataract |
| UV rays | Photokeratitis (welder's eye), skin cancer, sunburn |
| Infrared | Cataract (glassblower's cataract), heat stroke |
| X-rays | Radiation sickness, cancer, sterility |
Units of Radiation
- Roentgen (R) - exposure dose of X/gamma rays
- Rad - absorbed dose (100 ergs/g tissue)
- Rem - dose equivalent (biological effect)
- Gray (Gy) = 100 rad; Sievert (Sv) = 100 rem (SI units)
- Maximum Permissible Dose (MPD): 5 rem/year for radiation workers
Prevention (Park's - 7 Measures)
- Avoid inhalation, swallowing, or direct skin contact
- Shielding - lead aprons, lead glass for X-rays; adequate material thickness
- Monitoring - film badge or pocket electrometer every 6 months max for workers
- Protective clothing against contact with harmful materials
- Adequate ventilation to prevent inhalation of gases/dusts
- Periodic examination of workers every 2 months; if effects found → transfer to non-radiation work
- Pregnant women should NOT be allowed to work in areas of continuous radiation exposure
3 Principles of Radiation Protection (ALARA)
- Justification - benefit must outweigh risk
- Optimization / ALARA - As Low As Reasonably Achievable
- Dose limitation - not exceed MPD
Q9. Overcrowding (6 marks)
Definition
Overcrowding exists when a dwelling accommodates more persons than it can reasonably house, leading to adverse health and social consequences.
Criteria / Measurement
- Persons per room - most practical measure
- Room density standard: > 1.5 persons per room = overcrowding
- Air space standard: minimum 14 m³/person (Indian standard: 28-40 m³/person for adults)
- Floor area: minimum 4.5 m²/person
Causes
- Rapid urbanization, rural-urban migration
- Poverty and unaffordable housing
- Population explosion
- Slum development
Health Effects
- Airborne diseases - TB, measles, influenza, meningitis, COVID-19; more efficient droplet/airborne spread
- Contact diseases - scabies, ringworm, impetigo, conjunctivitis
- Gastrointestinal diseases - due to shared toilets/water, poor hygiene
- Mental health - stress, anxiety, violence, domestic abuse
- Accidents - fire hazards, falls
- Impaired sleep and reduced productivity
- Promotes vector breeding (mosquitoes, rodents)
Control
- Urban planning and housing development
- Slum improvement programmes
- Regulation of minimum floor space per person (building codes)
- National Urban Housing Policy
- Rajiv Awas Yojana / Pradhan Mantri Awas Yojana (PMAY)
Q10. Sanitation Barrier (6 marks)
Concept (Park's)
The disease cycle of faecal-borne diseases (typhoid, cholera, dysentery, hepatitis A) is transmitted through:
Faeces → Water / Fingers / Flies / Soil / Food → New Host
Community medicine aims to break this cycle at vulnerable points.
Definition of Sanitation Barrier
A sanitation barrier is a physical barrier imposed to segregate faeces and prevent it from reaching the new host directly or indirectly.
"In simple terms, this barrier can be provided by a sanitary latrine and a disposal pit. The more elaborate schemes envisage installation of a sewerage system and sewage treatment plants." - Park's
The Five "Fs" Blocked by Sanitation Barrier
- Faeces → stopped at source by latrine
- Fingers → hand washing (personal hygiene)
- Flies → proper disposal removes breeding ground
- Food → protection of food from contamination
- Fluids (Water) → proper water supply and treatment
Methods of Excreta Disposal
I. Unsewered Areas:
- Service type latrines (bucket/pail type) - least preferred
- Non-service (sanitary) latrines:
- Bore hole latrine
- Pit latrine
- Water-seal latrines - PRAI type, RCA type, Sulabh Shauchalaya (most popular in India)
- Septic tank
- Aqua privy
II. Sewered Areas:
- Water-carriage system with sewage treatment (primary, secondary, tertiary)
Swachh Bharat Mission
- India's national programme to achieve Open Defecation Free (ODF) status
- Constructing individual household latrines in rural and urban areas
- The sanitation barrier at national scale
Q11. Breeding Places of Mosquitoes + Reasons + Control (10 marks)
Types of Mosquitoes and Their Breeding Places
| Mosquito | Disease | Breeding Place |
|---|---|---|
| Anopheles | Malaria | Clear, fresh, slow-moving or stagnant water - rice fields, ponds, streams, seepages, hoof prints, drains |
| Culex | Filaria, Japanese encephalitis, West Nile fever | Polluted/stagnant water - drains, cesspools, septic tanks, water-logged areas, pot holes, old tyres |
| Aedes aegypti | Dengue, Chikungunya, Zika, Yellow fever | Clean, stored, man-made water - flower pots, water coolers, overhead tanks, plastic containers, old tyres, blocked gutters |
| Aedes albopictus | Dengue, Chikungunya | Similar to Aedes aegypti + tree holes, bamboo stumps |
| Mansonia | Filaria | Water bodies with aquatic vegetation (pistia, water hyacinth) - larvae attach to roots of plants |
Reasons Why These Are Breeding Places
- Mosquitoes require still or slow-moving water for egg-laying (oviposition)
- Larvae are aquatic and require water to complete development (egg → larva → pupa → adult)
- Anopheles needs clean water; Culex thrives in polluted water; Aedes uses stored clean water in small containers
- Temperature optimum: 25-30°C; favoured by tropical climate
Life Cycle
Egg → Larva (4 instars) → Pupa → Adult
- Larval stage: 5-14 days in water
- Female mosquito requires blood meal for egg development
Q12. Mosquito Control Measures (10 marks)
A. Anti-Larval Measures (Source Reduction)
1. Environmental / Mechanical
- Drainage - filling, levelling, draining of stagnant water bodies
- Intermittent irrigation - dry rice fields every 7-10 days (breaks larval cycle)
- Removal of water from containers, old tyres, flower pots weekly
- Cleaning and covering water storage containers
- Anti-larval fish - Gambusia affinis (Larvivorous fish) - eats larvae; most eco-friendly method; used for Anopheles control
- Oreochromis mossambicus (Tilapia) also used
2. Chemical Anti-larval
- Temephos (Abate) - organophosphate; 1 mg/L; safe for drinking water containers; used for Aedes
- Paris green (copper acetoarsenite) - only for Anopheles in rice fields; applied at 4-5 kg/acre
- Pyrethrum oil - applied to water surface; kills larvae
- Mineral oils / petroleum products - surface film suffocates larvae; 28 litres/acre
3. Biological
- Bacillus thuringiensis israelensis (Bti) - bacterial larvicide; highly specific; safe
- Bacillus sphaericus - for Culex
- Larvivorous fish (Gambusia, Tilapia)
B. Anti-Adult Measures
1. Indoor Residual Spraying (IRS)
- Spraying insecticide on indoor walls/ceilings
- Resting mosquitoes killed when they sit on treated surfaces
- Insecticides: DDT, Malathion, Deltamethrin, Bifenthrin
- Done twice a year before and during malaria season
2. Space Spraying
- Fogging (ULV) / Misting - insecticide dispersed as fine mist outdoors
- Kills adult mosquitoes in flight
- Used for dengue/chikungunya outbreaks
3. Personal Protection
- Mosquito nets (bed nets, preferably ITNs - Insecticide-Treated Nets)
- LLINs (Long-Lasting Insecticide-treated Nets) - treated with permethrin, last 3-5 years
- Repellents: DEET (diethyl toluamide), Citronella oil, Picaridin
- Protective clothing (full sleeves, socks)
- Window and door screens
4. Mosquito Coils, Mats, Vaporizers
- Pyrethroid-based products for indoor use
C. Integrated Vector Management (IVM)
WHO recommended approach combining:
- Environmental management (source reduction)
- Biological control
- Chemical control (judicious use)
- Personal protection
- Community participation
D. Legal Measures
- Prevention of Food Adulteration Act / Public Health Acts empower authorities to eliminate mosquito breeding sites
- Community notification to remove stagnant water around premises
All answers from Park's Textbook of Preventive and Social Medicine - Environment & Health chapter (Blocks 10, 11)
ESI act
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have complete data from Park's. Here is the full answer:
The Employees' State Insurance (ESI) Act, 1948
From Park's Textbook of Preventive and Social Medicine
1. Introduction
The ESI Act was passed in 1948 (amended in 1975, 1984, 1989, 2010 and 2019). It is an important measure of social security and health insurance for industrial workers in India.
It provides cash and medical benefits to industrial employees in case of:
- Sickness
- Maternity
- Employment injury
It is listed as one of the two most important factory laws in India (alongside the Factories Act, 1948).
2. Historical Background
The ESI Act was shaped by several important reports:
- Adarkar's Report on Health Insurance for Industrial Workers (1945)
- Report of the Health Survey and Development Committee (1946)
- Thomas Bedford's Report on Health of Industrial Workers (1946)
- Jones's Report on Health of Workers in Plantation (1947)
3. Scope / Coverage
Original Coverage (1948):
- All power-using factories (excluding mines, railways, defence) employing 10 or more persons
- Excluded seasonal factories
Extended by Amendment Act 1975 to:
| Category | Minimum Workers |
|---|---|
| Small factories (with or without power) | 10 or more |
| Shops | 10 or more |
| Hotels and restaurants | 10 or more |
| Cinemas and theatres | 10 or more |
| Road motor transport establishments | 10 or more |
| Newspaper establishments | 10 or more |
| Private medical & educational institutions (some states) | 20 or more |
Wage Ceiling:
- Effective 1.5.2010: employees earning up to Rs. 15,000/month covered
- Revised to Rs. 21,000/month w.e.f. 6.9.2016
- Employees earning daily wages below Rs. 176 are exempted from contribution
4. Administration
The Act is administered by the ESI Corporation (ESIC) - an autonomous body.
| Officer | Role |
|---|---|
| Chairman | Union Minister for Labour |
| Vice-Chairman | Secretary, Ministry of Labour |
| Chief Executive | Director General |
| Principal Officers (4) | Insurance Commissioner, Medical Commissioner, Financial Commissioner, Actuary |
| Medical Benefit Council | Headed by DGHS (Director General of Health Services) |
Infrastructure (as on 31.3.2020):
- Beneficiaries: ~13.24 crore
- Coverage: ~341 lakh family units in 7.83 lakh factories/establishments
- 1526 ESI dispensaries
- 1753 panel clinics
- 307 diagnostic centres
- 159 ESI hospitals + 42 hospital annexes
- > 22,600 beds
- 559 branch offices, 185 cash offices, 406 inspection offices
5. Finance (Contributions)
The scheme is funded by three sources:
| Contributor | Rate (revised w.e.f. 1.7.2019) |
|---|---|
| Employer | 3.25% of total wage bill |
| Employee | 0.75% of wages |
| State Government | 1/8 of total medical care cost |
| ESI Corporation | 7/8 of total medical care cost |
Employees earning daily wages < Rs. 176 are exempted from contributions but still eligible for all benefits.
6. Benefits to Employees (7 Benefits)
(1) Medical Benefit - Most Important
Full medical care, free of cost, including:
- Out-patient care
- Supply of drugs and dressings
- Specialist services (all branches of medicine)
- Pathological and radiological investigations
- Domiciliary services
- Antenatal, natal and postnatal services
- Immunization services
- Family planning services
- Emergency services
- Ambulance services
- Health education
- In-patient treatment
- Also: dentures, spectacles, hearing aids free for employment injury
- Artificial limbs free for those who lose limbs due to employment injury
How medical care is delivered:
- Direct pattern: ESI dispensaries (full-time for ≥1000 employee family units; part-time for <750; mobile dispensaries for scattered areas)
- Indirect pattern (Panel system): Registered Medical Practitioners appointed as Insurance Medical Practitioners (IMPs)
Family coverage:
- "Restricted medical care" = outpatient care only for families
- "Expanded medical care" = full care except hospitalization for families
(2) Sickness Benefit
- Cash payment certified by Insurance Medical Officer/Practitioner
- Payable for maximum 91 days in any continuous period of 365 days
- Daily rate: approximately 70% of average daily wages
Extended Sickness Benefit (ESB):
- For 34 specified long-term diseases (must be in continuous employment for 2 years)
- Payable for maximum 2 years
- Selected diseases include:
- TB, Leprosy, AIDS (Infectious)
- Malignant diseases (Cancer)
- Diabetes with complications
- Neurological disorders (hemiplegia, paraplegia)
- Cardiac diseases (MI, CHF, Cardiomyopathy)
- Renal failure / Transplant
(3) Maternity Benefit
- For confinement (delivery)
- Payable for 26 weeks (12 weeks before + 6 weeks after expected date of delivery)
- For miscarriage/MTP: 6 weeks
- At rate of full wages (double the sickness benefit rate)
(4) Disablement Benefit
- For temporary disablement due to employment injury
- Payable as long as disablement lasts at full wages (100% of daily wages)
- For permanent disablement: pension for life based on loss of earning capacity
- Permanent total disablement: same rate as temporary disablement (100% of wages)
(5) Dependant's Benefit
- Pension to dependants of insured worker who dies due to employment injury
- Widow receives pension for life (or until remarriage)
- Children until age 18 (or 25 if unmarried female)
- Aggregate not to exceed the full rate paid for total permanent disablement
(6) Funeral Expenses
- Lump sum payment to person performing last rites of deceased insured person
- Amount: Rs. 15,000 (revised)
(7) Rehabilitation Allowance
- For insured persons who suffer permanent disablement and undergo vocational rehabilitation at a recognised institution
- Paid during rehabilitation period
(8) Unemployment Allowance (Rajiv Gandhi Shramik Kalyan Yojana)
- For insured persons losing employment involuntarily (factory closure, retrenchment, permanent invalidity from non-employment injury)
- Must have contributed for 5 or more years
- Allowance for maximum 6 months (in one or multiple spells of ≥1 month)
- Medical care also continues during unemployment allowance period
7. Summary Table - Key Facts
| Feature | Detail |
|---|---|
| Year enacted | 1948 |
| Type | Social security and health insurance |
| Applicability | Whole of India |
| Coverage | Factories/establishments with ≥10 workers |
| Wage ceiling | Rs. 21,000/month (revised 2016) |
| Administering body | ESI Corporation (ESIC) |
| Chairman of ESIC | Union Minister for Labour |
| Employer contribution | 3.25% of wage bill |
| Employee contribution | 0.75% of wages |
| Sickness benefit | 70% wages for 91 days |
| Extended sickness | Up to 2 years (34 diseases) |
| Maternity benefit | 26 weeks at full wages |
| Funeral benefit | Rs. 15,000 |
| Unemployment benefit | Up to 6 months (after 5 years service) |
| Total benefits | 7 types |
8. Exam Memory Trick - Benefits (S M D D F R U)
| Letter | Benefit |
|---|---|
| S | Sickness benefit (91 days, 70% wages) |
| M | Maternity benefit (26 weeks) |
| D | Disablement benefit (temporary + permanent) |
| D | Dependant's benefit (pension to family) |
| F | Funeral expenses (Rs. 15,000) |
| R | Rehabilitation allowance |
| U | Unemployment allowance (6 months) |
| Med | Medical benefit (full free care - most important) |
Source: Park's Textbook of Preventive and Social Medicine - The Employees' State Insurance Act, 1948 (Block 11, pages 919-921); Social Security for Industrial Workers section (Block 10)
IUC DEVICE AND HORMONAL CONTRACEPTIVE
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from Park's. Here is the complete answer:
IUD (Intrauterine Contraceptive Device) and Hormonal Contraceptives
From Park's Textbook of Preventive and Social Medicine
PART A: INTRAUTERINE CONTRACEPTIVE DEVICE (IUCD)
1. Definition
An IUCD is a small device placed inside the uterine cavity for contraception. It is one of the most widely used reversible contraceptive methods worldwide.
2. Types / Generations of IUDs
First Generation - Inert / Non-Medicated Devices
- Made of polyethylene or other polymers
- Shapes: loops, spirals, coils, rings, bows
- Best known: Lippes Loop
Lippes Loop:
- Double-S shaped device made of polyethylene (non-toxic, non-tissue reactive)
- Contains barium sulphate (for X-ray visibility)
- Has a nylon tail/thread projecting into vagina - confirms position, aids removal
- Available in 4 sizes: A, B, C, D (D = largest)
- Larger sizes (C, D) suitable for multiparous women
- Larger size = greater anti-fertility + lower expulsion, but higher removal rate (more side effects)
Second Generation - Copper-Bearing Devices
- Metallic copper added to IUD in 1970s - strong anti-fertility effect
- Smaller; easier to fit even in nulliparous women
| Earlier devices | Newer devices |
|---|---|
| Copper-7 | Cu-T-220C |
| Copper T-200 | Cu-T-380A (most effective; used in India) |
| Cu-T-380 Ag | |
| Nova T | |
| Multiload Cu-250, Cu-375 |
- The number indicates copper surface area in mm² - effectiveness proportional to copper area
- Cu-T-380A (IUCD 380A): Effective for 10 years; pregnancy rate only 0.5-0.8%/year - used under India's National Family Planning Programme
- IUCD 375: Effective for 5 years
Third Generation - Hormone-Releasing Devices
- Release progesterone or levonorgestrel locally
| Device | Hormone | Duration |
|---|---|---|
| Progestasert | Progesterone 38 mg | 1 year |
| LNG-IUS (Mirena) | Levonorgestrel 52 mg | 5 years |
- Levonorgestrel IUD: lowest pregnancy rate - 0.2%/year
3. Mechanism of Action (Park's)
Inert IUDs:
"The most widely accepted view is that the IUD causes a foreign-body reaction in the uterus causing cellular and biochemical changes in the endometrium and uterine fluids, impairing viability of the gamete and reducing chances of fertilization."
Copper IUDs additionally:
- Copper enhances cellular response in endometrium
- Alters biochemical composition of cervical mucus
- Affects sperm motility, capacitation and survival
Hormone-releasing IUDs additionally:
- Increases viscosity of cervical mucus → prevents sperm entry
- Maintains high progesterone in endometrium → unfavourable for implantation
- Inhibits ovulation (with LNG-IUS)
4. Effectiveness
| Device | Pregnancy Rate (%/year) | Expulsion Rate | Removal Rate |
|---|---|---|---|
| Lippes Loop | 3 | 12-20% | 12-15% |
| Cu-7 | 2-3 | 6% | 11% |
| TCu-200 | 3 | 8% | 11% |
| TCu-380A | 0.5-0.8 | 5% | 14% |
| Progesterone IUD | 1.3-1.6 | 2.7% | 9.3% |
| LNG-IUD | 0.2 | 6% | 17% |
Overall pregnancy rate: 3-5 per 100 typical users in first year. "Theoretical effectiveness" of IUD is less than oral/injectable pills, but due to higher continuation rates, overall effectiveness is about the same in family planning programmes.
5. Timing of Insertion
- Any time during menstrual cycle if not pregnant
- Preferably during or just after menstruation
- Post-partum: After 6 weeks (not between 48 hours and 6 weeks - higher perforation risk)
- Post-abortion: Immediately after (first trimester)
- Post-coital (emergency): Within 5 days of unprotected sex
6. Contraindications
| Absolute | Relative |
|---|---|
| Pregnancy | Nulliparity |
| Undiagnosed vaginal bleeding | Multiple sexual partners (PID risk) |
| Active PID or STD | Anaemia |
| Uterine abnormalities (fibroids, malformation) | Heavy/painful periods |
| Malignancy of cervix/uterus | Anticoagulant therapy |
| Copper allergy | Recent STD history |
7. Complications / Side Effects
(1) Menstrual Problems - Most Common
- Increased menstrual blood loss (esp. inert/copper devices) → anaemia
- Intermenstrual bleeding and spotting
- Dysmenorrhoea (painful periods)
- Hormone-releasing devices REDUCE blood loss - benefit
(2) Pain
- Cramp-like lower abdominal pain especially after insertion
- Usually subsides with analgesics
(3) Pelvic Inflammatory Disease (PID) - Important
- IUD users are 2-8 times more likely to develop PID
- Risk highest in first few months after insertion
- Organisms: Gardnerella, Anaerobic streptococci, Bacteroides, Coliforms, Actinomyces
- Bacteria ascend via IUD tail from lower genital tract
- Even 1-2 episodes of PID can cause permanent infertility (blocked tubes)
- Management: broad-spectrum antibiotics; remove IUD if no response in 24-48 hours
(4) Uterine Perforation
- Incidence: 1:150 to 1:9000 insertions
- With trained physicians: not higher than 0.3%
- Device may migrate into peritoneal cavity → intestinal obstruction
- Copper devices cause intense tissue reaction → peritoneal adhesions
- Diagnosed by pelvic X-ray
- Higher risk: insertion between 48 hours and 6 weeks postpartum
(5) Expulsion
- More common in: young women, nulliparous women, postpartum insertion
- Usually in first few weeks or during menstruation
- 20% of expulsions go undetected → may lead to pregnancy
- Expulsion rates: copper < inert devices
(6) Pregnancy
- Actual use failure rate: ~3% in first year
- If pregnancy occurs with IUD in situ → increased risk of ectopic pregnancy and spontaneous abortion
- If intrauterine pregnancy: IUD should be removed if thread visible
(7) Ectopic Pregnancy
- IUD protects against intrauterine pregnancy but does NOT protect equally against ectopic pregnancy
- If pregnancy occurs despite IUD → increased risk of ectopic
(8) Fertility After Removal
- Fertility NOT impaired if no episode of PID
- >70% conceive within 1 year of IUD removal
(9) Cancer/Teratogenesis
- NO evidence that IUD use increases cancer risk
- No evidence of congenital malformations in offspring
(10) Mortality
- Extremely rare: 1 death per 100,000 woman-years
- IUD is safer than oral contraceptives in mortality - especially in older/high-risk patients
8. Advantages of IUD
- Highly effective long-term reversible contraception
- Independent of coitus (no need to remember daily)
- Does not interfere with lactation
- No systemic metabolic effects (inert/copper devices)
- Cost-effective (long life)
- High continuation rates
- Suitable for women who cannot take hormonal pills
PART B: HORMONAL CONTRACEPTIVES
1. Classification of Hormonal Contraceptives
Hormonal Contraceptives
├── Oral (Pills)
│ ├── Combined (Estrogen + Progestogen)
│ │ ├── Monophasic
│ │ ├── Biphasic
│ │ └── Triphasic
│ ├── Progestogen-only (Mini-pill)
│ └── Emergency contraceptive pill
├── Injectable
│ ├── Progestogen-only (DMPA, NET-EN)
│ └── Combined (monthly injection)
├── Implants (Subdermal)
├── Vaginal rings
└── Hormonal IUS (LNG-IUS/Mirena)
2. Combined Oral Contraceptive Pills (COC)
Composition
- Estrogen component: Ethinyl estradiol (EE) - 20, 30, 35 or 50 mcg
- Progestogen component: Levonorgestrel, Norgestrel, Norethisterone, Desogestrel, Drospirenone
Types in India (National Programme)
| Brand | Composition | Notes |
|---|---|---|
| Mala-N | Levonorgestrel 0.15 mg + EE 0.03 mg | Free through PHCs, UFWCs |
| Mala-D | Same + 7 iron (ferrous fumarate 60 mg) tablets | Rs. 3/packet social marketing; 28-pill pack |
| Chhaya (Centchroman) | Non-steroidal; 30 mg weekly | New addition to contraceptive basket |
How to Take the Pill
- Start on 5th day of menstrual period (strictly)
- Take daily at fixed time (preferably at night)
- 21 pills taken, then 7-day break → withdrawal bleeding occurs
- Not true menstruation; loss is about half of normal
- If a pill is missed: take it as soon as remembered + take next pill at usual time
Mode of Action (Park's)
- Inhibits ovulation - blocks pituitary secretion of gonadotropins (FSH, LH)
- Thickens cervical mucus → inhibits sperm penetration (progestogen)
- Alters endometrium → unfavourable for implantation
- Inhibits tubal motility → delays sperm and ovum transport
Effectiveness
- Almost 100% effective when taken correctly (theoretical)
- Actual use: pregnancy rate < 1%/year in developed countries
- Reduced effectiveness with: Rifampicin, Phenobarbitone, Ampicillin (enzyme inducers)
3. Progestogen-Only Pill (Mini-pill)
- Contains only progestogen (Norethisterone, Levonorgestrel)
- Mechanism: thickens cervical mucus, inhibits tubal motility; does NOT reliably inhibit ovulation
- Disadvantages: poor cycle control, higher pregnancy rate than combined pill
- Indications: women for whom combined pill is contraindicated (cardiovascular risk, older women >35 years, lactating women)
4. Injectable Contraceptives
a. DMPA (Depot Medroxyprogesterone Acetate) - "Antara Programme" in India
| Feature | Detail |
|---|---|
| Trade name | Depo-Provera, Megestron |
| Dose | 150 mg IM |
| Frequency | Every 3 months (12 weeks) |
| Failure rate | 0.1%/year |
| Route | Deep IM injection - gluteus maximus |
| Timing | First 5 days of menstrual period |
| Do NOT | Massage injection site after giving |
b. NET-EN (Norethisterone Enantate)
- Dose: 200 mg IM every 2 months (60 days)
- Slightly higher failure rate (0.4%) than DMPA
- Available since 1966
c. DMPA-SC (Subcutaneous)
- Dose: 104 mg subcutaneously (lower than IM)
- Given every 3 months
Combined Monthly Injectable
- Medroxyprogesterone 25 mg + Estradiol cypionate 5 mg
- One IM injection every 28-30 days
- Trade names: Cyclofem, Lunelle
Mode of Action of Injectables
- Inhibit ovulation (primary)
- Progestogenic effects on cervical mucus → sperm cannot penetrate
- Alter endometrium
Side Effects of Injectables
- Menstrual irregularities (most common) - spotting, amenorrhoea
- Weight gain
- Delayed return of fertility (average 10-12 months after last injection)
- No protection against STIs
5. Adverse Effects of Combined Oral Pills
a. Cardiovascular Effects
- Deep vein thrombosis (DVT) and pulmonary embolism - due to estrogen component
- Myocardial infarction - risk increased, especially in smokers over 35
- Hypertension - small but real increase in BP
- Current low-dose pills (30-35 mcg EE) have much reduced risk compared to earlier high-dose pills
b. Neoplastic Effects
- Cervical cancer: Slightly increased risk with long-term use
- Breast cancer: Very small/no overall increase in risk
- Liver tumours: Rare benign hepatic adenoma associated with use
- PROTECTIVE against: endometrial cancer, ovarian cancer, benign breast disease, ovarian cysts
c. Other Adverse Effects
- Nausea, vomiting (especially initial weeks)
- Headache, breast tenderness
- Mood changes, depression
- Breakthrough bleeding (spotting)
- Chloasma (skin pigmentation)
- Weight gain
d. Effects on Fertility After Stopping
- Post-pill amenorrhoea - delay in return of menstruation
- Fertility does return; most women conceive within 1-2 years
6. Benefits of Combined Oral Pills
- Nearly 100% effective when used correctly
- Reduces menstrual blood loss and dysmenorrhoea
- Protection against endometrial and ovarian cancer
- Reduces benign breast disease and ovarian cysts
- Reduces PID (thickened cervical mucus)
- Treats endometriosis and PCOS
- Regularizes menstrual cycle
- Reversible - fertility returns after stopping
7. Contraindications to OCP
| Absolute | Relative |
|---|---|
| Pregnancy | Hypertension |
| Thromboembolic disorders | Diabetes mellitus |
| Cardiovascular disease | Migraine |
| Liver disease | Depression |
| Oestrogen-dependent cancer | Age > 35 years + smoking |
| Undiagnosed vaginal bleeding | Lactation (within 6 weeks postpartum) |
8. Emergency Contraception (Post-coital)
Within 72 hours of unprotected intercourse:
| Method | Regimen |
|---|---|
| Levonorgestrel (India-approved) | 0.75 mg within 72 hrs + 0.75 mg after 12 hrs |
| OCP (50 mcg EE) | 2 pills within 72 hrs + 2 pills after 12 hrs |
| OCP (30/35 mcg EE) | 4 pills within 72 hrs + 4 pills after 12 hrs |
| Mifepristone | 10 mg once within 72 hrs |
| Copper IUD | Insert within 5 days |
- Failure rate: < 1%
- Emergency only - NOT for regular use
9. Summary Comparison Table
| Feature | IUD (Cu-T 380A) | COC | DMPA Injectable |
|---|---|---|---|
| Mechanism | Foreign body + copper effect | Inhibits ovulation + mucus | Inhibits ovulation + mucus |
| Effectiveness | 0.5-0.8% failure/yr | < 1%/yr | 0.1%/yr |
| Duration | 10 years | Daily | Every 3 months |
| Hormonal effects | None (copper) | Systemic | Systemic |
| Lactation safe? | Yes | No (combined; mini-pill OK) | Yes |
| Return of fertility | Immediate on removal | Immediate on stopping | Delayed 10-12 months |
| STD protection | None | None | None |
| India programme | IUCD 380A / 375 | Mala-N / Mala-D / Chhaya | Antara Programme |
Source: Park's Textbook of Preventive and Social Medicine - Contraception / Family Planning chapter (Block 7, pages 582-590)
asom csom
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.