I have my university exam of 1 st year of subject physiology These are the important long answer give me answer of this question "Describe the referred & radiating pain. Explain the Gate Control Theory of Pain." and remeber it's a long question and make it easy to memorized
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed from authoritative textbooks (Guyton & Hall, Neuroscience: Exploring the Brain, Kandel's Principles of Neural Science) plus both diagrams. Let me now write the complete, exam-ready answer.
Referred Pain, Radiating Pain & Gate Control Theory of Pain
Source: Guyton & Hall Textbook of Medical Physiology | Neuroscience: Exploring the Brain (Bear, Connors, Paradiso) | Kandel's Principles of Neural Science
PART 1 — REFERRED PAIN
Definition
Referred pain is pain that is felt at a site distant from (remote from) the actual diseased organ or tissue that is causing the pain.
Think: "The disease is HERE, but you feel the pain THERE."
Why is it Clinically Important?
In many visceral diseases, referred pain is the ONLY clinical sign the patient presents with. Without knowing these patterns, a doctor can easily miss the diagnosis.
Mechanism of Referred Pain (Convergence-Projection Theory)
This is the most accepted explanation:
- Visceral pain fibers (from internal organs) and somatic pain fibers (from the skin) converge onto the SAME second-order neurons in the dorsal horn of the spinal cord.
- When the visceral organ sends pain signals, these travel through the same spinal neurons that normally carry pain from the skin.
- The brain cannot distinguish which source the pain is coming from - it assumes (incorrectly) the pain is coming from the skin/body surface.
- So pain is perceived at the skin area that shares the same spinal segment as the diseased organ.
Diagram from Guyton & Hall:
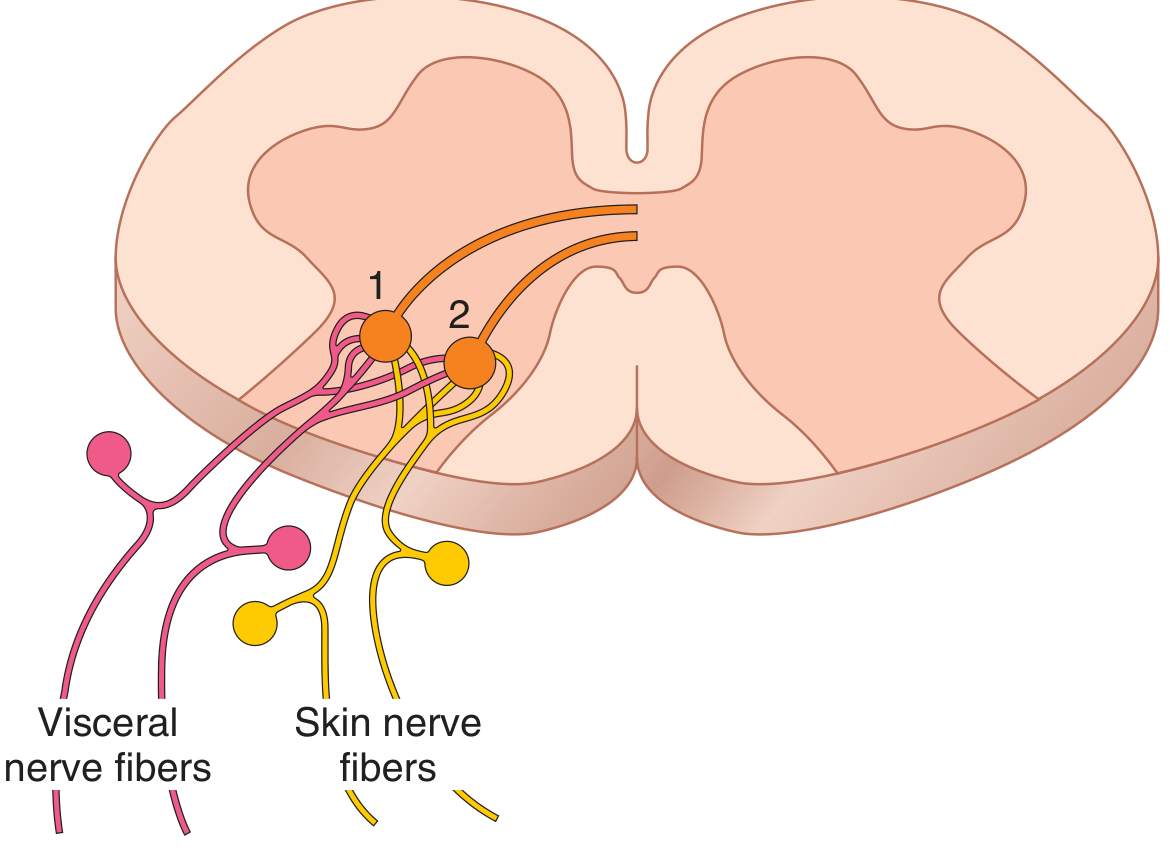
Neurons 1 and 2 receive pain signals from BOTH the skin and the viscera - the brain then attributes the pain to the skin.
Common Examples of Referred Pain (HIGH YIELD - must memorize!)
| Diseased Organ | Site of Referred Pain |
|---|---|
| Heart (MI / Angina) | Left arm, left shoulder, jaw, chest |
| Appendix (early) | Umbilicus / periumbilical area |
| Diaphragm irritation | Tip of shoulder (C4 dermatome) |
| Gallbladder | Right shoulder / right subscapular area |
| Kidney / Ureter stone | Groin / testis / inner thigh |
| Pancreas | Back (between shoulder blades) |
| Pelvic organs (uterus) | Lower back / inner thighs |
Memory trick for heart: "The Left side breaks your heart" - Left arm, Left jaw = Heart pain
Mechanism Summary in 3 Steps:
- Visceral pain fibers enter the spinal cord
- They synapse on the same neurons that receive signals from the skin
- Brain "projects" the sensation to the skin area - referred pain is felt there
PART 2 — RADIATING PAIN
Definition
Radiating pain is pain that travels or "radiates" or spreads along the course of a nerve from the point of origin to the area supplied by that nerve.
Think: "Pain travels ALONG a nerve, following its path."
Key Features:
- The pain follows a specific dermatomal or nerve distribution
- It spreads outward from the original source
- The patient can trace a "path" of the pain
Classic Example:
- Sciatica: Pain starts in the lower back and radiates down the buttock, posterior thigh, calf, to the foot - following the sciatic nerve (L4-S3)
- Cervical disc herniation: Pain from neck radiates down the arm to fingers
Referred Pain vs Radiating Pain - Key Difference
| Feature | Referred Pain | Radiating Pain |
|---|---|---|
| Origin | Visceral organ | Nerve/spinal nerve root |
| Mechanism | Convergence on same spinal neurons | Irritation/compression of nerve |
| Pattern | Felt at a distant skin area (not along a path) | Follows the nerve path/dermatome |
| Example | Heart attack felt as left arm pain | Sciatica - back to leg |
| Intervening area | No pain in the path between | Pain continuous along the nerve path |
PART 3 — GATE CONTROL THEORY OF PAIN
Proposed By:
Ronald Melzack and Patrick Wall (1965) - at MIT
This is one of the most important theories in pain physiology!
Background - Why was this theory needed?
Before this theory, pain was thought to be a simple, direct transmission. But observations showed:
- Rubbing an injured area reduces pain (e.g., rubbing a bruised shin)
- TENS (Transcutaneous Electrical Nerve Stimulation) can reduce chronic pain
- The same injury can produce more or less pain depending on context/emotions
This needed an explanation - hence the Gate Control Theory.
The Nerve Fibers Involved (Must Know!)
| Fiber Type | Size | Function | Effect on Gate |
|---|---|---|---|
| Aβ fibers (A-beta) | Large diameter, myelinated | Touch, pressure, vibration | CLOSE the gate (reduce pain) |
| C fibers | Small diameter, unmyelinated | Nociception (pain, slow burning) | OPEN the gate (increase pain) |
| Aδ fibers | Medium, lightly myelinated | Sharp/fast pain | OPEN the gate |
Location of the "Gate"
The gate is located in the dorsal horn of the spinal cord - specifically in Substantia Gelatinosa (Lamina II).
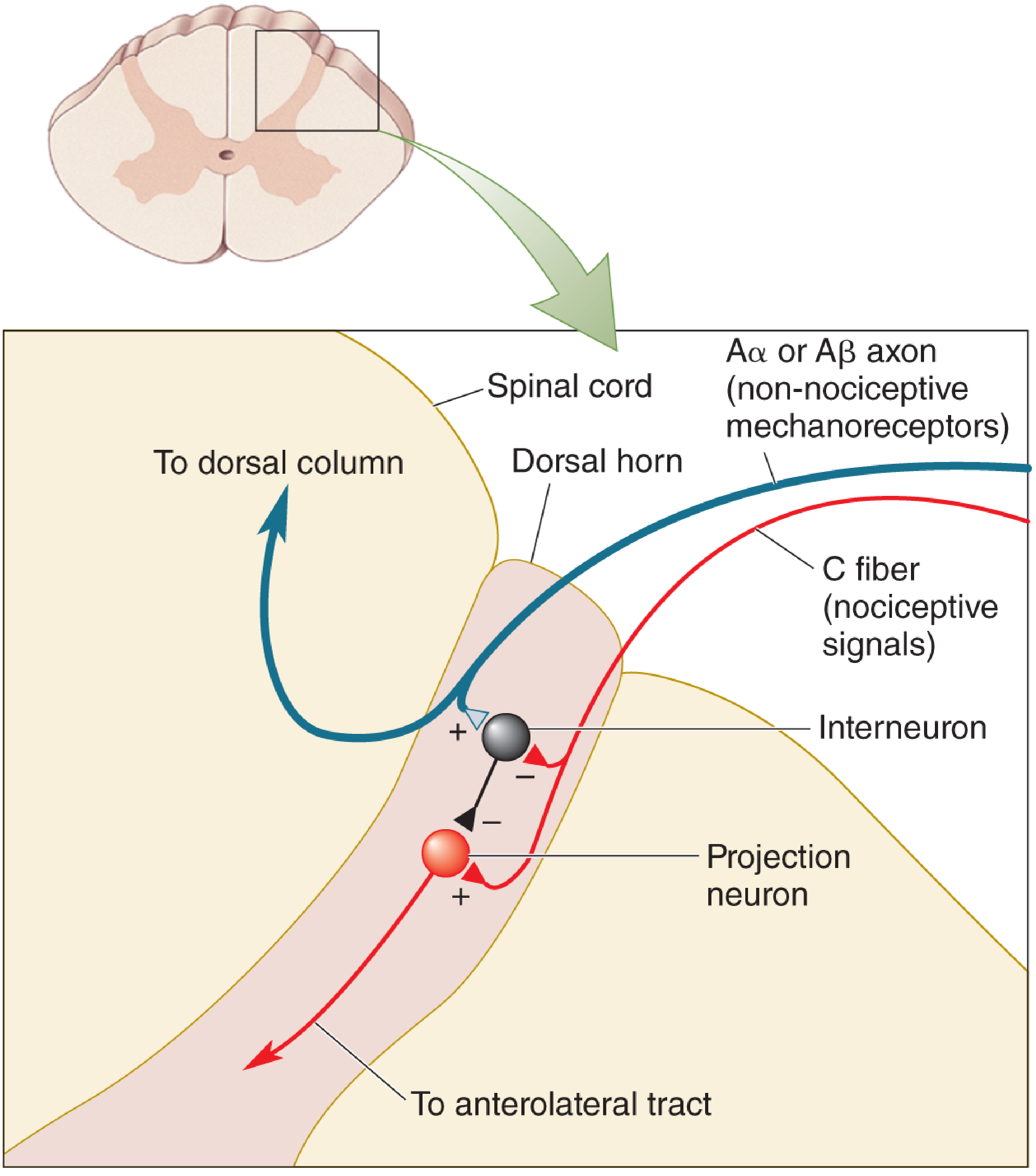
Mechanism of Gate Control Theory
The gate consists of 3 key cells:
- Aβ fiber (large diameter - touch fiber)
- C fiber (small diameter - pain fiber)
- Inhibitory Interneuron (in substantia gelatinosa - the "gatekeeper")
- Projection Neuron / T-cell (Transmission Cell) - sends signals up to the brain via anterolateral tract
The Rules:
- Aβ fiber activates (+) the inhibitory interneuron → interneuron INHIBITS (-) the projection neuron → Gate CLOSES → Less pain
- C fiber INHIBITS (-) the inhibitory interneuron → interneuron cannot block the projection neuron → projection neuron fires freely → Gate OPENS → More pain
Gate Control Theory Diagram (from Neuroscience: Exploring the Brain):
Simple Analogy to Remember:
Think of the inhibitory interneuron as a security guard at a gate.
- The Aβ fiber (touch) gives the guard ENERGY to LOCK the gate (closes it - pain blocked)
- The C fiber (pain) EXHAUSTS or FIRES the guard → Gate swings OPEN → Pain gets through
Gate Open vs Gate Closed - Summary
| Situation | Fiber Active | Gate Status | Pain Perception |
|---|---|---|---|
| Rubbing injured skin | Aβ (large) fires | CLOSED | Pain reduced |
| Tissue injury / no touch | C fibers dominate | OPEN | Pain felt |
| TENS therapy | Aβ stimulated | CLOSED | Pain reduced |
| Inflammation | More C fiber activity | OPEN | More pain |
Clinical Applications of Gate Control Theory
- TENS (Transcutaneous Electrical Nerve Stimulation) - stimulates Aβ fibers to close the gate - used in arthritis, chronic pain
- Rubbing/massage after injury - activates large Aβ fibers - explains why it helps
- Acupuncture - may work by activating large fiber pathways
- Spinal cord stimulation - electrodes placed over dorsal columns to activate large fibers
- Psychological factors - the theory also explains how emotions, attention, and context modify pain (descending control from the brain can also modulate the gate)
Limitations / Later Modifications:
- The original circuit has been modified many times - but the core concept (balance of large vs small fiber activity modulating pain) has stood the test of time
- It does not fully explain all types of chronic pain
- Descending pathways from the brain (e.g., PAG - periaqueductal gray) were later added to explain top-down pain modulation
QUICK REVISION SUMMARY (for last-minute study)
REFERRED PAIN:
→ Felt DISTANT from origin
→ Mechanism: Convergence of visceral + skin fibers on SAME spinal neuron
→ Heart = Left arm | Gallbladder = Right shoulder | Kidney = Groin
→ Brain projects sensation to the SKIN (not the organ)
RADIATING PAIN:
→ Pain TRAVELS along the nerve path
→ Example: Sciatica (back → leg along sciatic nerve)
→ Follows a dermatome
GATE CONTROL THEORY (Melzack & Wall, 1965):
→ Gate = Dorsal horn (Substantia Gelatinosa)
→ Aβ (large, touch) → activates inhibitory interneuron → CLOSES gate → ↓ Pain
→ C fiber (small, pain) → inhibits interneuron → OPENS gate → ↑ Pain
→ Applications: TENS, massage, spinal cord stimulation
Sources: Guyton and Hall Textbook of Medical Physiology; Neuroscience: Exploring the Brain (5th ed.); Kandel's Principles of Neural Science (6th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.