Make detailed notes on osteomyelitis with good images, flow charts and tables, so that I can use it directly in my university exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
OSTEOMYELITIS - Complete Exam Notes
Sources: Bailey & Love's Short Practice of Surgery 28e, Robbins & Kumar Pathologic Basis of Disease, Campbell's Operative Orthopaedics 15e (2026), Rosen's Emergency Medicine, Rockwood & Green's Fractures in Adults 10e (2025), Grainger & Allison's Diagnostic Radiology
1. DEFINITION
Osteomyelitis = Infection and inflammation of bone and bone marrow. It may complicate any systemic infection but frequently manifests as a solitary primary focus. All types of organisms (viruses, parasites, fungi, bacteria) can produce osteomyelitis, but pyogenic bacteria and mycobacteria are the most common causes.
2. ROUTES OF INFECTION
┌─────────────────────────────────────────────────────────┐
│ ROUTES OF BONE INFECTION │
├─────────────────┬───────────────┬───────────────────────┤
│ HAEMATOGENOUS │ CONTIGUOUS │ DIRECT INOCULATION │
│ (most common │ SPREAD │ │
│ in children) │ │ │
├─────────────────┼───────────────┼───────────────────────┤
│ Bacteraemia │ Soft tissue │ Open fractures │
│ seeds metaphy- │ infection │ Surgery/procedures │
│ seal vessels │ spreading to │ Puncture wounds │
│ due to slow │ bone │ Bite wounds │
│ sinusoidal flow │ │ Burns │
│ + microtrauma │ │ │
└─────────────────┴───────────────┴───────────────────────┘
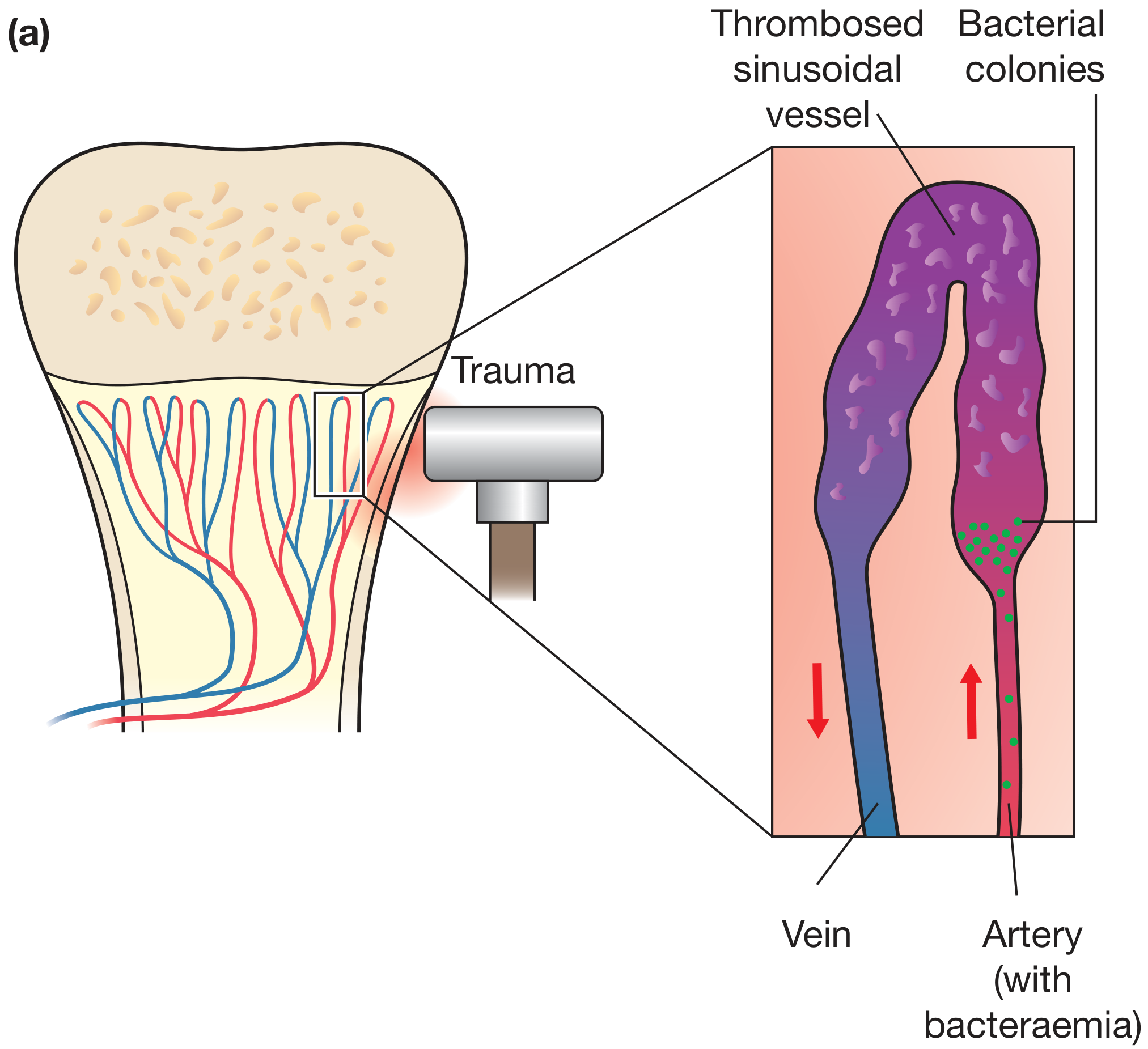
3. PATHOGENESIS - HAEMATOGENOUS SPREAD (Key for Exams)
Why the metaphysis? Blood flow in the looped metaphyseal sinusoidal vessels is slow, and this combined with microtrauma encourages bacterial seeding during bacteraemia.
4. PATHOLOGY - PROGRESSION FLOWCHART
Bacteraemia + Metaphyseal microtrauma
↓
Bacterial seeding of metaphysis
↓
Acute inflammation / neutrophils
↓
Necrosis of bone & marrow (within 48 hrs)
↓
Bacteria spread via Haversian canals → periosteum
↓
Subperiosteal abscess
(periosteum loosely attached in children)
↓
Periosteal elevation → ↓ blood supply → more necrosis
↓
┌──────────────────────────────────────┐
│ Pus formation │
└────────────┬─────────────────────────┘
↓ (if untreated)
Cortical bone perforation by pus
↓
Periosteal elevation → NEW BONE = INVOLUCRUM
Dead necrotic bone within = SEQUESTRUM
↓
"Bone within bone" appearance
↓
Pus tracks through gaps in involucrum (cloacae)
↓
Sinus tracts to skin surface
Key Pathological Terms
| Term | Definition | Significance |
|---|---|---|
| Sequestrum | Dead necrotic cortical bone separated from living bone | Hallmark of chronic osteomyelitis; acts as nidus for infection |
| Involucrum | Shell of new reactive periosteal bone encasing the sequestrum | Formed by periosteal elevation; "bone-within-bone" on X-ray |
| Cloaca | Openings/gaps in the involucrum | Allow pus to drain |
| Brodie abscess | Chronic walled-off abscess with sclerotic rim | Subacute form; lytic lesion on X-ray |
| Sinus tract | Channel from medullary cavity to skin | Indicates chronicity; risk of SCC in longstanding cases |
5. PATHOLOGY - DETAILED STAGES
Histological Changes by Stage
| Stage | Time | Histology |
|---|---|---|
| Acute | 0-48 hrs | Neutrophilic infiltrate, bone cell/marrow necrosis |
| Subacute | Days-weeks | Chronic inflammatory cells, cytokines, bone resorption, fibrous tissue ingrowth |
| Chronic | Weeks+ | Marrow fibrosis, sequestrum, lymphocytes + plasma cells, involucrum |
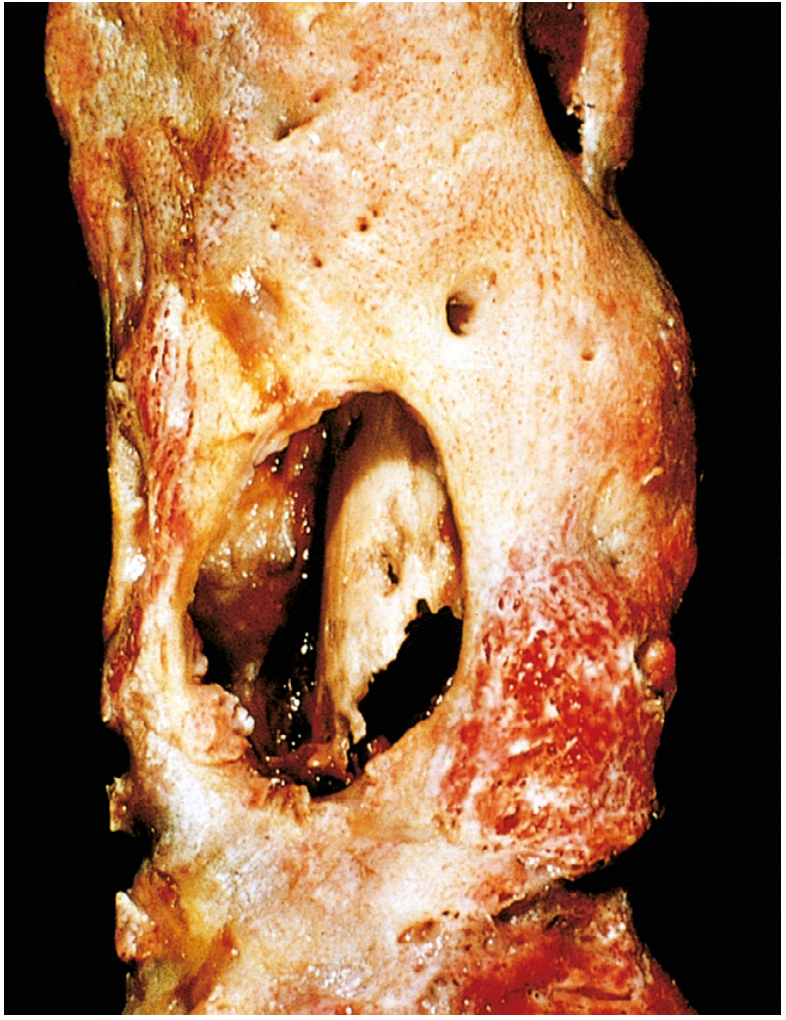
6. GROSS PATHOLOGY - SEQUESTRUM AND INVOLUCRUM
7. MICROBIOLOGY
Organisms by Age/Setting
| Patient Group | Most Likely Organisms |
|---|---|
| Neonates | Group B Streptococcus, E. coli |
| Children (all ages) | S. aureus (most common), Streptococcus pyogenes, H. influenzae* |
| Adults (general) | S. aureus (80-90% of culture-positive cases) |
| Sickle cell disease | Salmonella + other gram-negatives (areas of osteonecrosis = nidus) |
| Post-surgery / open fracture | Polymicrobial, gram-negatives |
| IV drug users | S. aureus, Pseudomonas, gram-negatives |
| Immunocompromised | Fungi, Candida, Aspergillus |
| TB osteomyelitis | M. tuberculosis (haematogenous from primary TB) |
H. influenzae no longer common after routine vaccination
Why S. aureus dominates: Staphylococcal cell wall proteins bind to bone matrix components (collagen), facilitating bacterial adherence to bone.
Note: Specific organisms identified in only ~50% of patients even with cultures. PCR of microbe-specific DNA sequences is improving this yield.
8. SITE OF INVOLVEMENT BY AGE
AGE GROUP SITE INVOLVED REASON
──────────────────────────────────────────────────────
Neonates Metaphysis + EPIPHYSIS Metaphyseal vessels penetrate
+ Joint (common) growth plate → high incidence
of joint involvement
Children METAPHYSIS (typical) Vessels do NOT penetrate
(>1yr) of long bones growth plate
Adults Epiphysis + subchondral Growth plate closure creates
region anastomoses between
metaphyseal & epiphyseal vessels
9. CLASSIFICATION
A. By Duration/Type
| Type | Time Course | Key Feature |
|---|---|---|
| Acute | < 2 weeks | Inflammatory changes, no bone destruction |
| Subacute | 2-6 weeks | Brodie abscess may form |
| Chronic | > 6 weeks | Bone destruction + sequestra evident |
B. Cierny-Mader Classification (Chronic Osteomyelitis - Most Used System)
This pathoanatomical system combines 4 anatomic types + 3 physiologic host classes = 12 distinct clinical stages
Anatomic Types
| Type | Name | Description |
|---|---|---|
| I | Medullary | Endosteal/intramedullary disease only |
| II | Superficial | Cortical surface infected due to soft tissue coverage defect |
| III | Localized | Full-thickness cortical sequestrum; stable bone |
| IV | Diffuse | Permeative infection; mechanically unstable bone |
Physiologic Host Classes
| Class | Host | Description |
|---|---|---|
| A | Normal | Immunocompetent, good local vascularity |
| B | Compromised | Local (Bᴸ) or Systemic (Bˢ) factors compromising immunity/healing |
| C | Prohibitive | Treatment worse than disease; minimal disability; not surgical candidate |
Systemic (S) factors degrading host class: Malnutrition, renal/hepatic failure, DM, chronic hypoxia, immune disease, smoking
Local (L) factors: Chronic lymphedema, venous stasis, major vessel compromise, arteritis, extensive scarring
A type II lesion in a class B host = Stage IIB chronic osteomyelitis. Guides whether treatment is simple/complex, curative/palliative, limb-sparing/ablative.
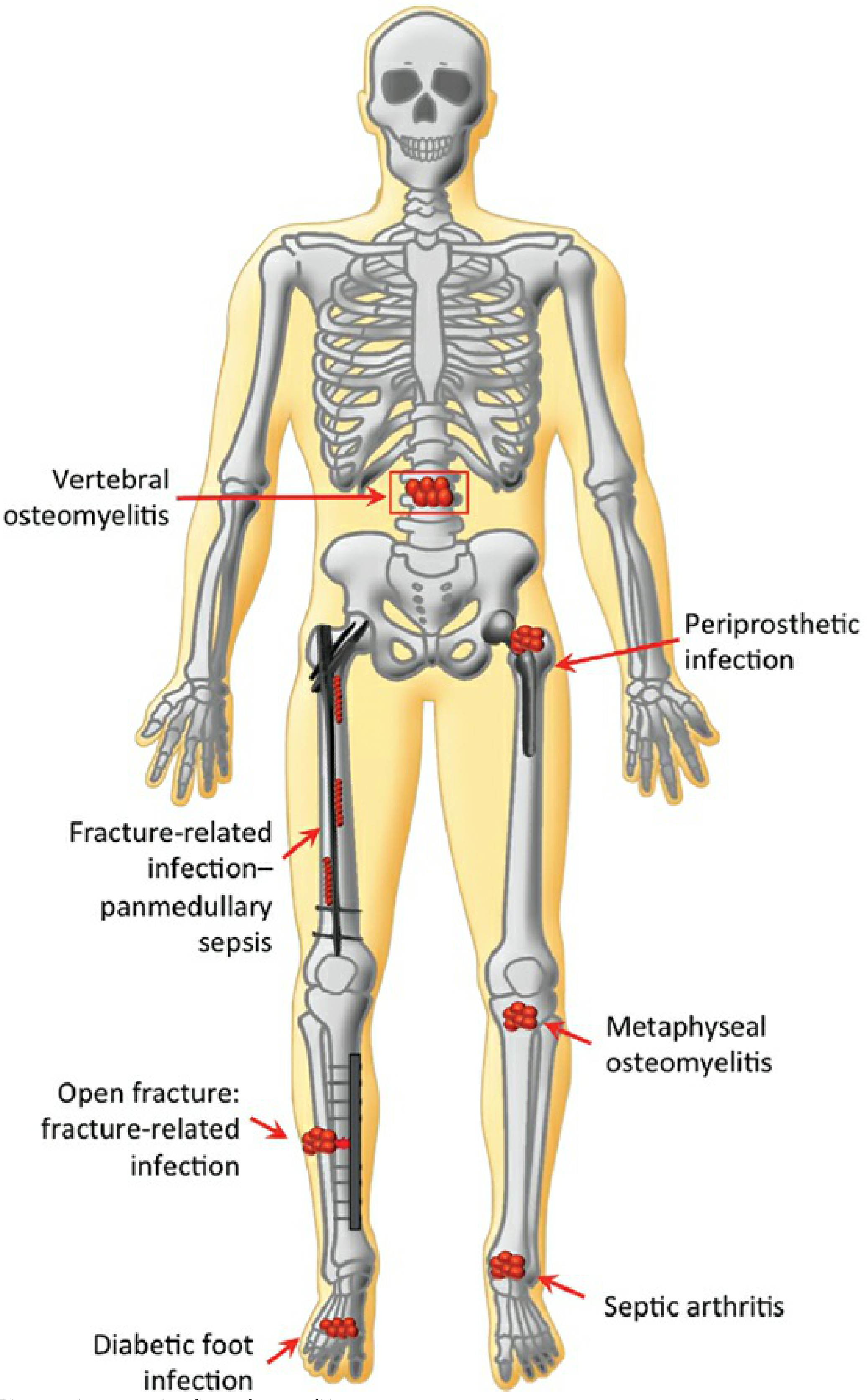
C. Anatomic Sites - Types of Osteomyelitis
10. CLINICAL FEATURES
Acute Osteomyelitis
SYSTEMIC LOCAL
───────────────── ──────────────────────────
• High fever + rigors • Point tenderness (most
• Malaise, fatigue important finding)
• Anorexia • Swelling
• Headache • Erythema + warmth
• Appear toxic • Pseudoparalysis (children)
• Limp / inability to bear weight
• Sympathetic joint effusion
Chronic Osteomyelitis
- Systemic symptoms less pronounced
- May feel palpable sequestrum or involucrum
- Sinus tracts discharging pus
- Recurrent flares after years of dormancy
Special Presentations
| Subset | Key Features |
|---|---|
| Children (AHO) | Male > Female (2:1 to 3:1), usually long bones (~80%), distal metaphysis, may NOT appear toxic |
| Vertebral osteomyelitis | Back pain, fever; often coexists with diskitis in adults |
| Diabetic foot | Insidious onset, peripheral neuropathy masks pain |
| Posttraumatic | History of open fracture, surgery; polymicrobial |
| Brodie abscess | Subacute, localized pain, sclerotic lytic lesion on X-ray |
11. INVESTIGATIONS
Laboratory
| Test | Finding | Comment |
|---|---|---|
| WBC | ↑ (leukocytosis) | Variable; may be normal |
| ESR | ↑↑ (often >50 mm/hr) | Sensitive; slow to normalize |
| CRP | ↑↑ | Faster to rise and fall than ESR; better for monitoring |
| Blood culture | Positive ~40% AHO | Always send before antibiotics |
| Bone biopsy | Gold standard for organism ID | Histology + culture; send immediately |
Imaging
| Modality | Findings | Timing/Note |
|---|---|---|
| Plain X-ray | Soft tissue swelling (early); cortical destruction + periosteal reaction (late); lytic focus | Changes lag 10-21 days behind disease! |
| Ultrasound | Subperiosteal fluid/abscess; guides aspiration | Best in infants/children; non-invasive |
| CT | Defines cortical destruction; detects sequestra | Also guides needle aspiration |
| MRI | HIGHEST sensitivity + specificity; shows intramedullary + soft tissue extent; contrast shows ring enhancement of abscess | Investigation of choice; also identifies spinal/intraspinal involvement |
| Bone scan (⁹⁹ᵐTc-MDP) | 3-phase scintigraphy; useful when MRI unavailable | False negatives in neonates; used to detect multifocal disease |
Brodie Abscess on MRI: "Penumbra sign" - peripheral high-signal ring (granulation tissue) surrounding low-signal central abscess cavity on T2
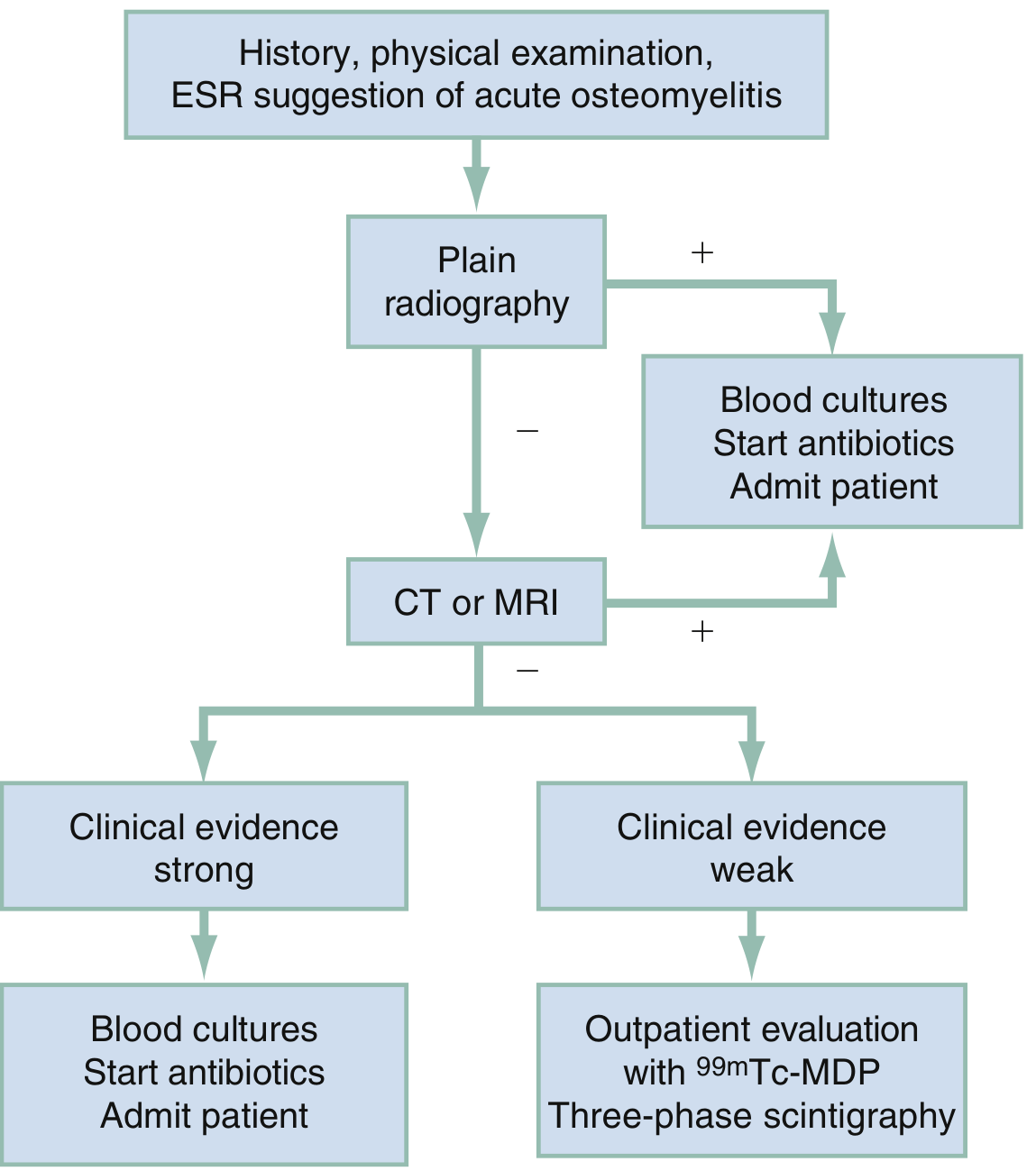
12. DIAGNOSIS - FLOWCHART
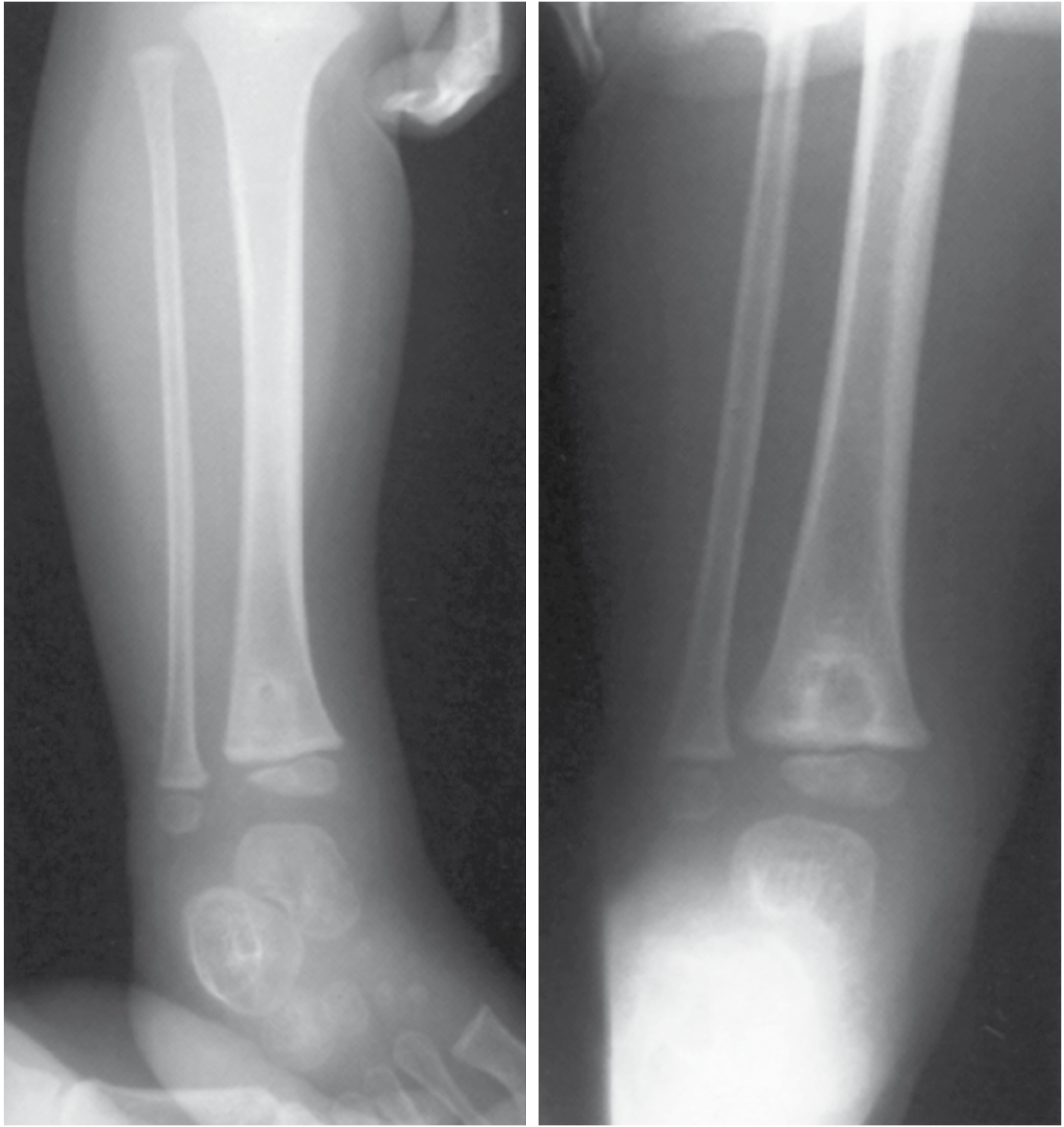
13. RADIOLOGY IMAGES
Brodie Abscess - X-ray
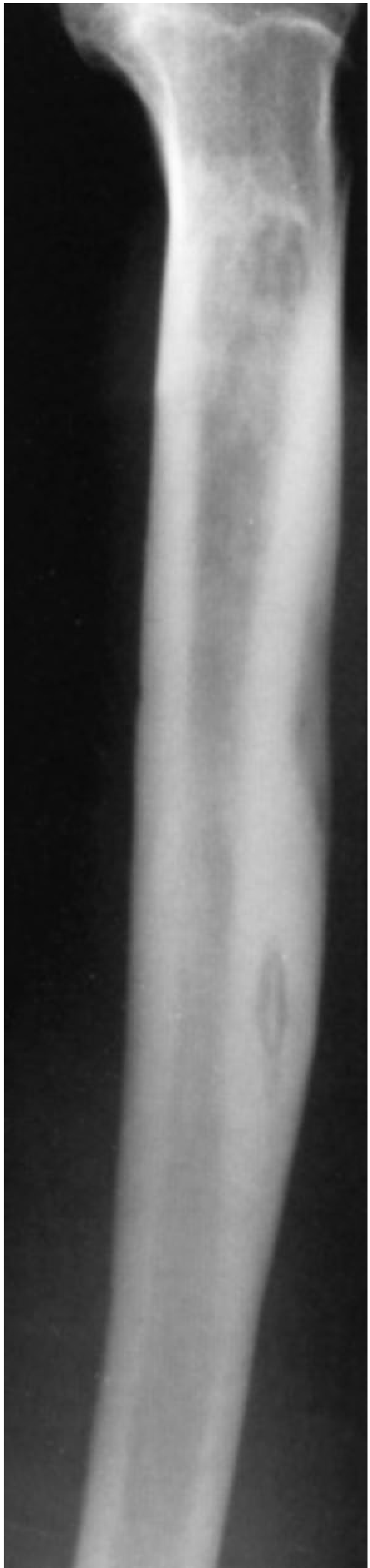
Sequestrum of Chronic Osteomyelitis - Tibia X-ray
14. TREATMENT
A. General Principles
Confirm diagnosis → Blood culture + bone biopsy
(before antibiotics if possible)
↓
IV antibiotics (empirical initially)
↓
Adjust to sensitivities
↓
Surgical drainage if pus present
("Pus needs to be drained")
↓
Rest / splintage of affected limb
+ Analgesia
B. Antibiotic Treatment
Empirical Antibiotic Selection by Age/Setting
| Patient Group | First Choice | Alternative |
|---|---|---|
| Children (general) | Anti-staphylococcal penicillin (flucloxacillin) | Clindamycin (MRSA areas) |
| Children (MRSA) | Vancomycin / clindamycin | Linezolid |
| Adults (community) | Flucloxacillin / nafcillin | Vancomycin |
| Adults (MRSA suspected) | Vancomycin | Daptomycin |
| Sickle cell | Cover Salmonella - fluoroquinolone + anti-staph | Ceftriaxone |
| Post-surgical / polymicrobial | Broad spectrum (pip-tazobactam) | |
| TB osteomyelitis | Standard 4-drug ATT (HRZE) |
Duration: Traditionally IV x 4-6 weeks. Current evidence supports switch to oral after clinical/haematological improvement (shortened IV + oral regimes for uncomplicated cases). MRSA + Panton-Valentine leukocidin (PVL) gene = higher morbidity; affects antibiotic choice.
C. Surgical Treatment
| Indication | Procedure |
|---|---|
| Abscess / pus under pressure | Drainage (needle or surgical) |
| Subperiosteal abscess | Surgical decompression |
| Chronic osteomyelitis with sequestrum | Sequestrectomy (removal of dead bone) |
| Failed medical management | Debridement + dead space management |
| Infected hardware | Hardware removal (usually) |
| Soft tissue defect after debridement | Muscle flap / free flap coverage |
| Bone defect | Bone grafting / Masquelet technique / transport |
| Refractory/amputation-risk | Amputation in selected cases |
Dead Space Management After Debridement:
- Antibiotic-loaded PMMA cement beads (non-biodegradable)
- Biodegradable antibiotic carriers (calcium sulphate, hydroxyapatite)
- Muscle/soft tissue flap
15. SPECIFIC FORMS
A. Vertebral Osteomyelitis / Diskitis
- Adults: vertebral osteomyelitis often coexists with diskitis
- Children: isolated diskitis more common
- Symptoms: back pain ± radiculopathy ± fever; may refuse to walk
- MRI: best modality; shows disc and vertebral involvement; detects intraspinal complications
- CT: guides needle aspiration of disc (cultures positive ~30-60%)
- Treatment: largely non-operative (antibiotics); surgery for instability or cord compression
B. Brodie Abscess (Subacute Osteomyelitis)
- Chronic walled-off intraosseous abscess
- Localized pain, low-grade fever
- X-ray: well-defined lytic lesion with sclerotic rim
- MRI: penumbra sign
- Treatment: surgical drainage + curettage + antibiotics
C. TB Osteomyelitis (Pott's Disease when spinal)
- Haematogenous spread from primary pulmonary TB (~1-3% of TB cases)
- More destructive and resistant than pyogenic osteomyelitis
- Presents with localized pain, low-grade fever, weight loss
- Usually solitary; typically involves vertebrae (Pott's disease)
- Tuberculous dactylitis (spina ventosa): cyst-like cavities + diaphyseal expansion, hands > feet
- Treatment: standard ATT (at least 12 months for bone TB)
D. Diabetic Foot Osteomyelitis
- Neuropathy masks pain → late presentation
- Secondary to soft tissue ulceration → contiguous spread
- Plain X-ray first; MRI for extent
- Management: debridement + prolonged antibiotics ± revascularization
16. COMPLICATIONS
ACUTE OSTEOMYELITIS CHRONIC OSTEOMYELITIS
────────────────── ──────────────────────
• Bacteraemia / Sepsis • Pathologic fracture
• Septic arthritis (esp. neonates) • Secondary (reactive) amyloidosis
• Growth arrest / deformity • Endocarditis
(if epiphysis involved in children) • Marsupialization → sinus tracts
• Pathologic fracture • Squamous cell carcinoma
• Chronic osteomyelitis in draining sinus tracts*
• Local spread → brain abscess, • Sarcoma in infected bone (rare)
meningitis, empyema, spinal • Malignant transformation
cord compression (SCC most common)
*Marjolin's ulcer principle: Longstanding draining sinus of chronic osteomyelitis can undergo malignant transformation to squamous cell carcinoma. Signs: increased pain, increased discharge, foul smell. Treatment: wide excision or amputation + chemo/radiation.
17. QUICK SUMMARY TABLE - ACUTE vs CHRONIC OSTEOMYELITIS
| Feature | Acute | Chronic |
|---|---|---|
| Duration | < 2-6 weeks | > 6 weeks |
| Pathology | Neutrophils, necrosis, abscess | Sequestrum, involucrum, fibrosis |
| Organisms | S. aureus (mainly) | S. aureus, polymicrobial |
| Symptoms | Fever, systemic toxicity | Low grade, sinus tracts |
| X-ray | Often normal initially; soft tissue swelling | Sequestrum, involucrum, "bone-in-bone" |
| MRI | High signal marrow on T2/STIR | Sequestrum (low signal); ring enhancement |
| Treatment | IV antibiotics ± drainage | Debridement + sequestrectomy + long antibiotics |
| Outcome if untreated | Progresses to chronic | Flares, amyloidosis, SCC |
18. HIGH-YIELD EXAM POINTS (Quick Recall)
- Most common organism overall = S. aureus (80-90%)
- Sickle cell = Salmonella (due to osteonecrosis nidus + impaired splenic function)
- Neonates = Group B Strep + E. coli; metaphysis AND epiphysis AND joint can all be involved
- Metaphysis is the preferred site due to slow sinusoidal blood flow + microtrauma
- Sequestrum = dead bone; Involucrum = new bone shell around sequestrum
- X-ray lag = 10-21 days - MRI is the investigation of choice for early diagnosis
- Brodie abscess = subacute walled-off abscess; lytic lesion with sclerotic rim; "penumbra sign" on MRI
- Cierny-Mader = gold standard classification for chronic osteomyelitis; 4 anatomic types × 3 host classes = 12 stages
- Chronic sinus + SCC = Marjolin's ulcer-type malignant transformation
- Pott's disease = TB osteomyelitis of spine; kyphosis + cord compression complications
- Treatment principle = "Drain pus, give antibiotics" - IV initially, oral switch once improving
- Panton-Valentine leukocidin (PVL)-positive MRSA = more aggressive; higher morbidity
Sources: Bailey & Love's Short Practice of Surgery 28e | Robbins & Kumar Pathologic Basis of Disease | Campbell's Operative Orthopaedics 15e | Rosen's Emergency Medicine | Rockwood & Green's Fractures in Adults 10e | Grainger & Allison's Diagnostic Radiology
Make a poster, including all the details and images given above, use for revision during exam
Reading File
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/osteomyelitis-poster && ls /home/daytona/worksp…
Running Command
cd /home/daytona/workspace/osteomyelitis-poster && node /home/daytona/skills/sha…
Writing File
~/osteomyelitis-poster/build_poster.js
const pptxgen = require("pptxgenjs");
const fs = require("fs");
// Load images
const images = JSON.parse(fs.readFileSync("/home/daytona/workspace/osteomyelitis-poster/images.json"));
const img = {};
const urls = [
"4732ddb81e78e31e89dc1e21c97601e082b1405bba5480593863baf467873c6f", // [0] hematogenous spread diagram
"e83fd0f264806a68553cae82263600e1785e2686eec72e1819ef879a16764cd5", // [1] bone abscess anatomy
"dd8e3ef10b89a9003d848e81343bbac22b8a7388e2c20ac8cce085c867dbe5d7", // [2] joint spread diagram
"407ff4d4c5193e5071c7911cfc4a538d051a419d3480b098ab1ff538dcf524d9", // [3] gross pathology sequestrum
"1cf3b081e38306134a895e0958682b57eacdb683bcffb4d568ae1f9474577bc1", // [4] Brodie abscess xray
"bc19268ff7b4d4d0c1f6b6f5485c82fcdfbd9c598f8b1b58a9a3c969880ec9e5", // [5] sequestrum tibia xray
"a0c2103869355b0b49eb5135ff9c8bed3505bd64778d92df683950a58668d702", // [6] types of osteomyelitis diagram
"205bc6043834c1f15a18357d1d39d65ccfc708774011904d340d0e03940137d8", // [7] diagnostic flowchart
];
images.forEach((item, i) => { img[i] = item.base64; });
// ─── Color Palette ───────────────────────────────────────────────────
const C = {
navy: "0D2B55", // dominant dark navy
teal: "0B6E8C", // mid-tone teal
ltblue: "D6EAF2", // light panel background
orange: "E06B2D", // accent/highlight
gold: "F0A500", // table header
white: "FFFFFF",
offwht: "F4F7FB",
dark: "1A1A2E",
gray: "555555",
ltgray: "E8EEF4",
red: "C0392B",
green: "1A7A4A",
yellow: "FFF9C4",
teallt: "B2D8E4",
};
let pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" x 7.5"
pres.title = "Osteomyelitis - Exam Revision Poster";
// ────────────────────────────────────────────────────────────────────────
// Helper: Add slide header bar
// ────────────────────────────────────────────────────────────────────────
function addHeader(slide, title, subtitle) {
// Dark navy top bar
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 13.3, h: 0.7, fill: { color: C.navy }, line: { color: C.navy } });
// Orange accent stripe
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.7, w: 13.3, h: 0.07, fill: { color: C.orange }, line: { color: C.orange } });
slide.addText(title, { x: 0.2, y: 0.05, w: 9, h: 0.6, fontSize: 22, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
if (subtitle) {
slide.addText(subtitle, { x: 9.3, y: 0.1, w: 3.8, h: 0.5, fontSize: 10, color: C.teallt, fontFace: "Calibri", align: "right", italic: true, margin: 0 });
}
// Slide background
slide.background = { color: C.offwht };
}
// ────────────────────────────────────────────────────────────────────────
// Helper: Section label box
// ────────────────────────────────────────────────────────────────────────
function sectionLabel(slide, text, x, y, w, h, bg, fg) {
bg = bg || C.teal;
fg = fg || C.white;
slide.addShape(pres.shapes.RECTANGLE, { x, y, w, h, fill: { color: bg }, line: { color: bg } });
slide.addText(text, { x, y, w, h, fontSize: 9, bold: true, color: fg, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
}
// ────────────────────────────────────────────────────────────────────────
// SLIDE 1 - TITLE / OVERVIEW
// ────────────────────────────────────────────────────────────────────────
{
let slide = pres.addSlide();
slide.background = { color: C.navy };
// Large title
slide.addText("OSTEOMYELITIS", {
x: 0.5, y: 1.1, w: 12.3, h: 1.4,
fontSize: 56, bold: true, color: C.white, fontFace: "Calibri",
align: "center", charSpacing: 8
});
// Subtitle
slide.addText("Comprehensive Exam Revision Notes", {
x: 0.5, y: 2.55, w: 12.3, h: 0.55,
fontSize: 22, color: C.gold, fontFace: "Calibri", align: "center", italic: true
});
// Orange divider
slide.addShape(pres.shapes.RECTANGLE, { x: 3.5, y: 3.2, w: 6.3, h: 0.07, fill: { color: C.orange }, line: { color: C.orange } });
// Definition box
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 1.5, y: 3.4, w: 10.3, h: 1.35, fill: { color: "152040" }, line: { color: C.teal, pt: 2 }, rectRadius: 0.1 });
slide.addText([
{ text: "DEFINITION: ", options: { bold: true, color: C.gold } },
{ text: "Osteomyelitis is infection and inflammation of bone and bone marrow. It may complicate systemic infection but frequently manifests as a solitary primary focus. Pyogenic bacteria and mycobacteria are the most common causes.", options: { color: C.white } }
], { x: 1.7, y: 3.5, w: 9.9, h: 1.1, fontSize: 13, fontFace: "Calibri", valign: "middle" });
// Bottom row - quick facts
const facts = [
{ label: "Most Common\nOrganism", val: "S. aureus\n(80–90%)" },
{ label: "Preferred\nSite", val: "Metaphysis\n(long bones)" },
{ label: "Key Pathology", val: "Sequestrum &\nInvolucrum" },
{ label: "Best\nImaging", val: "MRI\n(gold standard)" },
{ label: "X-ray Lag", val: "10–21 days\nbehind disease" },
];
facts.forEach((f, i) => {
const x = 0.5 + i * 2.47;
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y: 5.0, w: 2.27, h: 1.4, fill: { color: C.teal }, line: { color: C.orange, pt: 1.5 }, rectRadius: 0.1 });
slide.addText(f.label, { x, y: 5.05, w: 2.27, h: 0.45, fontSize: 9, bold: true, color: C.teallt, fontFace: "Calibri", align: "center" });
slide.addText(f.val, { x, y: 5.5, w: 2.27, h: 0.8, fontSize: 13, bold: true, color: C.white, fontFace: "Calibri", align: "center" });
});
// Source
slide.addText("Sources: Bailey & Love 28e | Robbins Pathology | Campbell's Orthopaedics 15e | Rosen's EM | Rockwood & Green 10e", {
x: 0, y: 7.3, w: 13.3, h: 0.2, fontSize: 7, color: "6699BB", align: "center", italic: true
});
}
// ────────────────────────────────────────────────────────────────────────
// SLIDE 2 - ROUTES + PATHOGENESIS + HAEMATOGENOUS SPREAD IMAGE
// ────────────────────────────────────────────────────────────────────────
{
let slide = pres.addSlide();
addHeader(slide, "ROUTES OF INFECTION & PATHOGENESIS", "Bailey & Love 28e | Robbins Pathology");
// LEFT COLUMN - Routes box
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 4.0, h: 3.1, fill: { color: C.ltblue }, line: { color: C.teal, pt: 1.5 } });
sectionLabel(slide, "ROUTES OF INFECTION", 0.15, 0.85, 4.0, 0.32, C.teal, C.white);
const routes = [
{ title: "1. HAEMATOGENOUS (Most common in children)", body: "Bacteraemia seeds metaphyseal sinusoidal vessels\nSlow sinusoidal flow + microtrauma = seeding site\nCommon sites: distal femur, proximal tibia, proximal humerus" },
{ title: "2. CONTIGUOUS SPREAD", body: "Infection spreads from adjacent soft tissues / joints\nE.g. diabetic foot, dental abscess → jaw bone" },
{ title: "3. DIRECT INOCULATION", body: "Open fractures, surgery, puncture wounds\nBite wounds, burns, prosthetic procedures\nOften POLYMICROBIAL" },
];
routes.forEach((r, i) => {
const y = 1.25 + i * 0.88;
slide.addShape(pres.shapes.RECTANGLE, { x: 0.2, y, w: 3.9, h: 0.22, fill: { color: C.teal }, line: { color: C.teal } });
slide.addText(r.title, { x: 0.25, y, w: 3.8, h: 0.22, fontSize: 8, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
slide.addText(r.body, { x: 0.25, y: y + 0.23, w: 3.8, h: 0.6, fontSize: 8, color: C.dark, fontFace: "Calibri" });
});
// MIDDLE - Haematogenous diagram image
slide.addShape(pres.shapes.RECTANGLE, { x: 4.25, y: 0.85, w: 4.5, h: 3.1, fill: { color: C.white }, line: { color: C.teal, pt: 1 } });
slide.addImage({ data: img[0], x: 4.3, y: 0.9, w: 4.4, h: 2.75, altText: "Haematogenous spread diagram" });
slide.addText("Fig: Bacterial seeding of metaphyseal sinusoidal vessels via bacteraemia + microtrauma", {
x: 4.25, y: 3.65, w: 4.5, h: 0.32, fontSize: 7.5, italic: true, color: C.gray, fontFace: "Calibri", align: "center"
});
// RIGHT - Bone anatomy image
slide.addShape(pres.shapes.RECTANGLE, { x: 8.85, y: 0.85, w: 4.3, h: 3.1, fill: { color: C.white }, line: { color: C.teal, pt: 1 } });
slide.addImage({ data: img[1], x: 8.9, y: 0.9, w: 4.2, h: 2.75 });
slide.addText("Fig: Bone abscess formation — pus under periosteum, cortex and medullary cavity", {
x: 8.85, y: 3.65, w: 4.3, h: 0.32, fontSize: 7.5, italic: true, color: C.gray, fontFace: "Calibri", align: "center"
});
// BOTTOM - Site by age table
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 4.05, w: 13.0, h: 0.3, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("SITE OF INVOLVEMENT BY AGE", { x: 0.15, y: 4.05, w: 13.0, h: 0.3, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const ageRows = [
["Age Group", "Site Involved", "Reason", "Common Organisms"],
["Neonates\n(<1 month)", "Metaphysis + EPIPHYSIS + Joint\n(all three simultaneously)", "Metaphyseal vessels penetrate growth plate\n→ high incidence of joint involvement", "Group B Strep, E. coli"],
["Children\n(1–16 yrs)", "METAPHYSIS of long bones\n(distal femur, proximal tibia)", "Slow sinusoidal flow\n+ microtrauma during bacteraemia", "S. aureus (80–90%), MRSA in AHO\nStrep pyogenes, Kingella kingae"],
["Adults", "Epiphysis + subchondral region\nVertebrae (haematogenous)", "Growth plate closure creates anastomoses\nbetween metaphyseal & epiphyseal vessels", "S. aureus, polymicrobial\n(post-surgery/fracture)"],
];
const colW = [2.0, 3.5, 4.3, 3.05];
const startX = 0.15;
const startY = 4.38;
const rowH = [0.3, 0.55, 0.55, 0.55];
let curY = startY;
ageRows.forEach((row, ri) => {
let curX = startX;
row.forEach((cell, ci) => {
const isHeader = ri === 0;
const bg = isHeader ? C.teal : (ri % 2 === 0 ? C.ltblue : C.white);
slide.addShape(pres.shapes.RECTANGLE, { x: curX, y: curY, w: colW[ci], h: rowH[ri], fill: { color: bg }, line: { color: C.teallt, pt: 0.5 } });
slide.addText(cell, { x: curX + 0.05, y: curY, w: colW[ci] - 0.1, h: rowH[ri], fontSize: isHeader ? 8.5 : 8, bold: isHeader, color: isHeader ? C.white : C.dark, fontFace: "Calibri", valign: "middle" });
curX += colW[ci];
});
curY += rowH[ri];
});
}
// ────────────────────────────────────────────────────────────────────────
// SLIDE 3 - PATHOLOGY PROGRESSION + GROSS SPECIMEN + TERMS
// ────────────────────────────────────────────────────────────────────────
{
let slide = pres.addSlide();
addHeader(slide, "PATHOLOGY — PROGRESSION, KEY TERMS & GROSS SPECIMEN", "Robbins Pathology | Bailey & Love 28e");
// LEFT: Flowchart of pathology
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 5.2, h: 6.5, fill: { color: C.ltblue }, line: { color: C.teal, pt: 1.5 } });
sectionLabel(slide, "PATHOGENESIS FLOWCHART", 0.15, 0.85, 5.2, 0.3, C.navy, C.white);
const flowSteps = [
{ text: "Bacteraemia + Metaphyseal Microtrauma", bg: C.navy, fg: C.white },
{ text: "↓", bg: C.offwht, fg: C.orange },
{ text: "Bacterial seeding of metaphysis\n(sinusoidal slow-flow vessels)", bg: C.teal, fg: C.white },
{ text: "↓", bg: C.offwht, fg: C.orange },
{ text: "Acute inflammation → NEUTROPHILS\nNecrosis of bone & marrow (within 48 hrs)", bg: "1A6B8A", fg: C.white },
{ text: "↓", bg: C.offwht, fg: C.orange },
{ text: "Spread via Haversian canals → PERIOSTEUM\nSubperiosteal abscess formation", bg: "246E8C", fg: C.white },
{ text: "↓", bg: C.offwht, fg: C.orange },
{ text: "Periosteal elevation → ↓ blood supply\n→ MORE NECROSIS", bg: C.orange, fg: C.white },
{ text: "↓ (if untreated)", bg: C.offwht, fg: C.gray },
{ text: "SEQUESTRUM = Dead necrotic cortical bone\nINVOLUCRUM = New periosteal bone shell", bg: C.red, fg: C.white },
{ text: "↓", bg: C.offwht, fg: C.orange },
{ text: "Cloacae → Sinus tracts → Skin surface\n\"Bone-within-bone\" on X-ray", bg: "6B2737", fg: C.white },
];
const stepStartY = 1.22;
const stepH = [0.28, 0.2, 0.33, 0.2, 0.35, 0.2, 0.35, 0.2, 0.33, 0.2, 0.37, 0.2, 0.33];
let sy = stepStartY;
flowSteps.forEach((step, i) => {
if (step.text.startsWith("↓")) {
slide.addText(step.text, { x: 0.2, y: sy, w: 5.05, h: stepH[i], fontSize: step.text === "↓" ? 16 : 9, color: step.fg, fontFace: "Calibri", align: "center", bold: true });
} else {
slide.addShape(pres.shapes.RECTANGLE, { x: 0.25, y: sy, w: 4.95, h: stepH[i], fill: { color: step.bg }, line: { color: step.bg } });
slide.addText(step.text, { x: 0.3, y: sy, w: 4.85, h: stepH[i], fontSize: 9, bold: true, color: step.fg, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
}
sy += stepH[i];
});
// MIDDLE - Joint spread image + key terms table
// Image
slide.addShape(pres.shapes.RECTANGLE, { x: 5.5, y: 0.85, w: 3.9, h: 2.8, fill: { color: C.white }, line: { color: C.teal, pt: 1 } });
slide.addImage({ data: img[2], x: 5.55, y: 0.9, w: 3.8, h: 2.6 });
slide.addText("Fig: Spread of bone abscess into joint cavity\n(esp. in neonates — intracapsular metaphysis)", {
x: 5.5, y: 3.65, w: 3.9, h: 0.35, fontSize: 7.5, italic: true, color: C.gray, fontFace: "Calibri", align: "center"
});
// Histological stages table
slide.addShape(pres.shapes.RECTANGLE, { x: 5.5, y: 4.1, w: 3.9, h: 0.28, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("HISTOLOGICAL STAGES", { x: 5.5, y: 4.1, w: 3.9, h: 0.28, fontSize: 9, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const histRows = [
["Stage", "Time", "Histology"],
["ACUTE", "0–48 hrs", "Neutrophilic infiltrate, bone + marrow necrosis"],
["SUBACUTE", "Days–weeks", "Chronic inflammatory cells, bone resorption, fibrous tissue ingrowth"],
["CHRONIC", "Weeks+", "Marrow fibrosis, sequestrum, lymphocytes + plasma cells, involucrum"],
];
const hColW = [1.0, 0.9, 1.95];
let hCurY = 4.38;
histRows.forEach((row, ri) => {
let hCurX = 5.5;
row.forEach((cell, ci) => {
const isH = ri === 0;
const bg = isH ? C.teal : (ri % 2 === 0 ? C.ltblue : C.white);
slide.addShape(pres.shapes.RECTANGLE, { x: hCurX, y: hCurY, w: hColW[ci], h: 0.38, fill: { color: bg }, line: { color: C.teallt, pt: 0.5 } });
slide.addText(cell, { x: hCurX + 0.04, y: hCurY, w: hColW[ci] - 0.08, h: 0.38, fontSize: isH ? 8 : 7.5, bold: isH, color: isH ? C.white : C.dark, fontFace: "Calibri", valign: "middle" });
hCurX += hColW[ci];
});
hCurY += 0.38;
});
// RIGHT - Gross Pathology + key terms
slide.addShape(pres.shapes.RECTANGLE, { x: 9.55, y: 0.85, w: 3.6, h: 3.1, fill: { color: C.white }, line: { color: C.teal, pt: 1 } });
slide.addImage({ data: img[3], x: 9.6, y: 0.9, w: 3.5, h: 2.7 });
slide.addText("Fig: Resected femur — sequestrum inside involucrum (Robbins Pathology Fig 26.16)", {
x: 9.55, y: 3.65, w: 3.6, h: 0.35, fontSize: 7.5, italic: true, color: C.gray, fontFace: "Calibri", align: "center"
});
// KEY TERMS
slide.addShape(pres.shapes.RECTANGLE, { x: 9.55, y: 4.1, w: 3.6, h: 0.28, fill: { color: C.orange }, line: { color: C.orange } });
slide.addText("KEY PATHOLOGICAL TERMS", { x: 9.55, y: 4.1, w: 3.6, h: 0.28, fontSize: 9, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const terms = [
{ term: "Sequestrum", def: "Dead necrotic cortical bone — hallmark of chronic OM; acts as nidus for infection" },
{ term: "Involucrum", def: "Shell of new reactive periosteal bone around sequestrum; 'bone-within-bone' on X-ray" },
{ term: "Cloaca", def: "Openings in involucrum through which pus drains" },
{ term: "Brodie Abscess", def: "Chronic walled-off abscess; well-defined lytic lesion + sclerotic rim" },
{ term: "Sinus Tract", def: "Channel from medullary cavity to skin; longstanding → risk of SCC (Marjolin's)" },
];
let termY = 4.42;
terms.forEach((t, i) => {
const bg = i % 2 === 0 ? C.ltblue : C.white;
slide.addShape(pres.shapes.RECTANGLE, { x: 9.55, y: termY, w: 3.6, h: 0.44, fill: { color: bg }, line: { color: C.teallt, pt: 0.3 } });
slide.addText([
{ text: t.term + ": ", options: { bold: true, color: C.teal, fontSize: 8 } },
{ text: t.def, options: { color: C.dark, fontSize: 7.5 } }
], { x: 9.6, y: termY + 0.03, w: 3.5, h: 0.38, fontFace: "Calibri", valign: "top" });
termY += 0.44;
});
}
// ────────────────────────────────────────────────────────────────────────
// SLIDE 4 - MICROBIOLOGY + CLASSIFICATION
// ────────────────────────────────────────────────────────────────────────
{
let slide = pres.addSlide();
addHeader(slide, "MICROBIOLOGY & CLASSIFICATION (CIERNY-MADER)", "Rockwood & Green 10e | Campbell's Orthopaedics 15e");
// LEFT - Microbiology table
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 5.6, h: 0.28, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("MICROBIOLOGY — ORGANISMS BY SETTING", { x: 0.15, y: 0.85, w: 5.6, h: 0.28, fontSize: 9.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const microRows = [
["Patient Group", "Most Likely Organisms", "Notes"],
["Neonates", "Group B Strep, E. coli", "Metaphysis + epiphysis + joint"],
["Children (general)", "S. aureus (MRSA in AHO), Strep pyogenes, Kingella kingae", "Male:female = 2:1 to 3:1"],
["Adults", "S. aureus (80–90% culture-positive)", "Hematogenous or post-traumatic"],
["Sickle Cell Disease", "Salmonella + gram-negatives", "Osteonecrosis = nidus; impaired spleen"],
["Post-surgery / Open Fx", "Polymicrobial, gram-negatives", "Gustilo grading guides Abx"],
["IV Drug Users", "S. aureus, Pseudomonas", "Unusual sites (spine, clavicle)"],
["Immunocompromised", "Fungi (Candida, Aspergillus)", "Consider if not improving"],
["TB Osteomyelitis", "Mycobacterium tuberculosis", "1–3% of TB cases; more destructive"],
];
const mColW = [2.1, 2.4, 1.0];
let mCurY = 1.16;
microRows.forEach((row, ri) => {
let mCurX = 0.15;
row.forEach((cell, ci) => {
const isH = ri === 0;
const bg = isH ? C.teal : (ri % 2 === 0 ? C.ltblue : C.white);
slide.addShape(pres.shapes.RECTANGLE, { x: mCurX, y: mCurY, w: mColW[ci], h: 0.42, fill: { color: bg }, line: { color: C.teallt, pt: 0.4 } });
slide.addText(cell, { x: mCurX + 0.04, y: mCurY, w: mColW[ci] - 0.08, h: 0.42, fontSize: isH ? 8 : 7.5, bold: isH, color: isH ? C.white : C.dark, fontFace: "Calibri", valign: "middle" });
mCurX += mColW[ci];
});
mCurY += 0.42;
});
// Staph note
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.15, y: 4.98, w: 5.6, h: 0.45, fill: { color: "FFF3CD" }, line: { color: C.gold, pt: 1 }, rectRadius: 0.05 });
slide.addText("★ Why S. aureus? Staphylococcal cell wall proteins bind bone matrix components (collagen) → facilitating bacterial adherence to bone. Cultures only identify organism in ~50% cases; PCR improving this.", {
x: 0.2, y: 4.99, w: 5.5, h: 0.43, fontSize: 7.5, color: "5D4037", fontFace: "Calibri", valign: "middle"
});
// MIDDLE/RIGHT - Cierny-Mader Classification
slide.addShape(pres.shapes.RECTANGLE, { x: 5.9, y: 0.85, w: 7.25, h: 0.28, fill: { color: C.orange }, line: { color: C.orange } });
slide.addText("CIERNY-MADER CLASSIFICATION — CHRONIC OSTEOMYELITIS (Most Widely Used System)", {
x: 5.9, y: 0.85, w: 7.25, h: 0.28, fontSize: 9.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0
});
// Anatomic types
slide.addShape(pres.shapes.RECTANGLE, { x: 5.9, y: 1.16, w: 3.55, h: 0.25, fill: { color: C.teal }, line: { color: C.teal } });
slide.addText("ANATOMIC TYPES (4)", { x: 5.9, y: 1.16, w: 3.55, h: 0.25, fontSize: 9, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const anatTypes = [
["Type I", "Medullary", "Endosteal / intramedullary only"],
["Type II", "Superficial", "Cortical surface infected — coverage defect"],
["Type III", "Localized", "Full-thickness cortical sequestrum; stable bone"],
["Type IV", "Diffuse", "Permeative infection; MECHANICALLY UNSTABLE bone"],
];
const aColW = [0.6, 0.9, 2.0];
let aCurY = 1.44;
anatTypes.forEach((row, ri) => {
let aCurX = 5.9;
row.forEach((cell, ci) => {
const bg = ri % 2 === 0 ? C.ltblue : C.white;
slide.addShape(pres.shapes.RECTANGLE, { x: aCurX, y: aCurY, w: aColW[ci], h: 0.42, fill: { color: bg }, line: { color: C.teallt, pt: 0.4 } });
const isBold = ci === 0;
slide.addText(cell, { x: aCurX + 0.04, y: aCurY, w: aColW[ci] - 0.08, h: 0.42, fontSize: 8, bold: isBold, color: isBold ? C.teal : C.dark, fontFace: "Calibri", valign: "middle" });
aCurX += aColW[ci];
});
aCurY += 0.42;
});
// Physiologic classes
slide.addShape(pres.shapes.RECTANGLE, { x: 5.9, y: 3.18, w: 3.55, h: 0.25, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("PHYSIOLOGIC HOST CLASSES (3)", { x: 5.9, y: 3.18, w: 3.55, h: 0.25, fontSize: 9, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const hostClasses = [
["A Host", "Normal", "Immunocompetent, good local vascularity"],
["B Host", "Compromised", "Bᴸ = local factors; Bˢ = systemic factors"],
["C Host", "Prohibitive", "Treatment worse than disease; poor prognosis; not surgical candidate"],
];
const hcColW = [0.7, 0.9, 1.9];
let hcCurY = 3.46;
hostClasses.forEach((row, ri) => {
let hcCurX = 5.9;
row.forEach((cell, ci) => {
const bgs = [C.ltblue, C.white, C.ltblue];
slide.addShape(pres.shapes.RECTANGLE, { x: hcCurX, y: hcCurY, w: hcColW[ci], h: 0.47, fill: { color: bgs[ri] }, line: { color: C.teallt, pt: 0.4 } });
slide.addText(cell, { x: hcCurX + 0.04, y: hcCurY, w: hcColW[ci] - 0.08, h: 0.47, fontSize: 8, bold: ci === 0, color: ci === 0 ? C.orange : C.dark, fontFace: "Calibri", valign: "middle" });
hcCurX += hcColW[ci];
});
hcCurY += 0.47;
});
// Staging note
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.9, y: 4.95, w: 3.55, h: 0.48, fill: { color: "FFF3CD" }, line: { color: C.gold, pt: 1 }, rectRadius: 0.05 });
slide.addText("4 Anatomic Types × 3 Host Classes = 12 Clinical Stages\nE.g. Type II + B Host → Stage IIB Chronic Osteomyelitis", {
x: 5.95, y: 4.96, w: 3.45, h: 0.46, fontSize: 8, color: "5D4037", fontFace: "Calibri", bold: true
});
// RIGHT side - types of OM body diagram
slide.addShape(pres.shapes.RECTANGLE, { x: 9.55, y: 1.16, w: 3.6, h: 3.45, fill: { color: C.white }, line: { color: C.teal, pt: 1 } });
slide.addImage({ data: img[6], x: 9.6, y: 1.2, w: 3.5, h: 3.1 });
slide.addText("Fig: Types of Osteomyelitis — Vertebral, Metaphyseal, Periprosthetic, Fracture-related, Diabetic foot (Rockwood & Green 10e)", {
x: 9.55, y: 4.62, w: 3.6, h: 0.38, fontSize: 7, italic: true, color: C.gray, fontFace: "Calibri", align: "center"
});
// By duration
slide.addShape(pres.shapes.RECTANGLE, { x: 9.55, y: 5.02, w: 3.6, h: 0.25, fill: { color: C.teal }, line: { color: C.teal } });
slide.addText("CLASSIFICATION BY DURATION", { x: 9.55, y: 5.02, w: 3.6, h: 0.25, fontSize: 8.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const durRows = [
["Type", "Duration", "Key Feature"],
["Acute", "< 2 wks", "Inflammatory, no bone destruction"],
["Subacute", "2–6 wks", "Brodie abscess may form"],
["Chronic", "> 6 wks", "Sequestrum + involucrum evident"],
];
const dColW = [0.85, 0.9, 1.8];
let dCurY = 5.3;
durRows.forEach((row, ri) => {
let dCurX = 9.55;
row.forEach((cell, ci) => {
const isH = ri === 0;
const bg = isH ? C.navy : (ri % 2 === 0 ? C.ltblue : C.white);
slide.addShape(pres.shapes.RECTANGLE, { x: dCurX, y: dCurY, w: dColW[ci], h: 0.38, fill: { color: bg }, line: { color: C.teallt, pt: 0.4 } });
slide.addText(cell, { x: dCurX + 0.04, y: dCurY, w: dColW[ci] - 0.08, h: 0.38, fontSize: isH ? 7.5 : 7.5, bold: isH, color: isH ? C.white : C.dark, fontFace: "Calibri", valign: "middle" });
dCurX += dColW[ci];
});
dCurY += 0.38;
});
}
// ────────────────────────────────────────────────────────────────────────
// SLIDE 5 - CLINICAL FEATURES + INVESTIGATIONS + RADIOLOGY
// ────────────────────────────────────────────────────────────────────────
{
let slide = pres.addSlide();
addHeader(slide, "CLINICAL FEATURES, INVESTIGATIONS & RADIOLOGY", "Rosen's Emergency Medicine | Campbell's Orthopaedics 15e | Grainger & Allison");
// LEFT: Clinical features
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 4.3, h: 0.28, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("CLINICAL FEATURES", { x: 0.15, y: 0.85, w: 4.3, h: 0.28, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
// Acute features - two sub-boxes
sectionLabel(slide, "ACUTE — SYSTEMIC", 0.15, 1.15, 2.1, 0.25, C.red, C.white);
const systemicFeatures = ["High fever + rigors", "Malaise, fatigue", "Anorexia, headache", "May appear toxic", "Tachycardia"];
systemicFeatures.forEach((f, i) => {
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 1.42 + i * 0.3, w: 2.1, h: 0.28, fill: { color: i % 2 === 0 ? "FDECEA" : C.white }, line: { color: "FFCDD2", pt: 0.3 } });
slide.addText("• " + f, { x: 0.2, y: 1.42 + i * 0.3, w: 2.0, h: 0.28, fontSize: 8, color: C.dark, fontFace: "Calibri", valign: "middle" });
});
sectionLabel(slide, "ACUTE — LOCAL", 2.28, 1.15, 2.15, 0.25, "1A6B4A", C.white);
const localFeatures = ["Point tenderness ★", "Swelling + warmth", "Erythema", "Sympathetic effusion", "Limp / can't weight bear"];
localFeatures.forEach((f, i) => {
slide.addShape(pres.shapes.RECTANGLE, { x: 2.28, y: 1.42 + i * 0.3, w: 2.15, h: 0.28, fill: { color: i % 2 === 0 ? "E8F5E9" : C.white }, line: { color: "C8E6C9", pt: 0.3 } });
slide.addText("• " + f, { x: 2.33, y: 1.42 + i * 0.3, w: 2.05, h: 0.28, fontSize: 8, color: C.dark, fontFace: "Calibri", valign: "middle" });
});
// Chronic features
sectionLabel(slide, "CHRONIC OSTEOMYELITIS", 0.15, 2.97, 4.3, 0.25, C.teal, C.white);
const chronicF = ["Systemic symptoms less prominent", "Palpable sequestrum / involucrum", "SINUS TRACTS discharging pus", "Recurrent flares after years of dormancy", "Draining wound (long-standing)"];
chronicF.forEach((f, i) => {
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 3.25 + i * 0.3, w: 4.3, h: 0.28, fill: { color: i % 2 === 0 ? C.ltblue : C.white }, line: { color: C.teallt, pt: 0.3 } });
slide.addText("• " + f, { x: 0.2, y: 3.25 + i * 0.3, w: 4.2, h: 0.28, fontSize: 8, color: C.dark, fontFace: "Calibri", valign: "middle" });
});
// Complications box
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 4.78, w: 4.3, h: 0.25, fill: { color: C.red }, line: { color: C.red } });
slide.addText("COMPLICATIONS", { x: 0.15, y: 4.78, w: 4.3, h: 0.25, fontSize: 9, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const comps = [
"Acute: Bacteraemia/Sepsis, Septic arthritis (esp. neonates), Growth arrest, Pathologic fracture",
"Chronic: Secondary amyloidosis, Endocarditis, Pathologic fracture",
"★ Marjolin's: SCC in longstanding sinus tract — increased pain + foul smell → BIOPSY",
];
comps.forEach((c, i) => {
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 5.05 + i * 0.37, w: 4.3, h: 0.35, fill: { color: i === 2 ? "FFF3CD" : (i % 2 === 0 ? "FDECEA" : C.white) }, line: { color: "FFCDD2", pt: 0.3 } });
slide.addText(c, { x: 0.2, y: 5.05 + i * 0.37, w: 4.2, h: 0.35, fontSize: 7.5, color: i === 2 ? "5D4037" : C.dark, fontFace: "Calibri", valign: "middle" });
});
// MIDDLE - Investigations table
slide.addShape(pres.shapes.RECTANGLE, { x: 4.6, y: 0.85, w: 5.0, h: 0.28, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("INVESTIGATIONS", { x: 4.6, y: 0.85, w: 5.0, h: 0.28, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const invRows = [
["Test", "Finding", "Comment"],
["WBC", "↑ Leukocytosis", "Variable; may be normal"],
["ESR", "↑↑ (often >50 mm/hr)", "Sensitive; slow to normalize; use to monitor"],
["CRP", "↑↑ elevated", "Faster rise & fall than ESR; better for monitoring treatment"],
["Blood Culture", "+ve ~40% in AHO", "Always send BEFORE antibiotics"],
["Bone Biopsy", "Gold standard", "Histology + culture — essential for pathogen ID"],
["X-ray", "Soft tissue swelling (early)\nCortical destruction + periosteal reaction (late)", "Lag of 10–21 days! Always first investigation"],
["Ultrasound", "Subperiosteal fluid/abscess", "Best in infants; non-invasive; guides aspiration"],
["CT", "Cortical destruction; detects sequestra", "Guides needle aspiration; great for sequestrum"],
["MRI", "High T2 signal; ring enhancement of abscess;\nPenumbra sign (Brodie)", "Highest sensitivity + specificity; GOLD STANDARD"],
["Bone Scan\n(⁹⁹ᵐTc-MDP)", "3-phase uptake", "If MRI unavailable; false -ve in neonates"],
];
const iColW = [1.15, 1.9, 1.9];
let iCurY = 1.16;
invRows.forEach((row, ri) => {
let iCurX = 4.6;
const rH = (ri >= 6) ? 0.46 : 0.36;
row.forEach((cell, ci) => {
const isH = ri === 0;
const bg = isH ? C.teal : (ri % 2 === 0 ? C.ltblue : C.white);
slide.addShape(pres.shapes.RECTANGLE, { x: iCurX, y: iCurY, w: iColW[ci], h: rH, fill: { color: bg }, line: { color: C.teallt, pt: 0.4 } });
slide.addText(cell, { x: iCurX + 0.04, y: iCurY, w: iColW[ci] - 0.08, h: rH, fontSize: isH ? 8 : 7.5, bold: isH, color: isH ? C.white : C.dark, fontFace: "Calibri", valign: "middle" });
iCurX += iColW[ci];
});
iCurY += rH;
});
// RIGHT - X-ray images
slide.addShape(pres.shapes.RECTANGLE, { x: 9.75, y: 0.85, w: 3.4, h: 2.9, fill: { color: C.white }, line: { color: C.teal, pt: 1 } });
slide.addImage({ data: img[4], x: 9.8, y: 0.9, w: 3.3, h: 2.55 });
slide.addText("Fig: Brodie abscess — distal tibial epiphysis, 3-year-old\n(well-defined lytic lesion + sclerotic rim)", {
x: 9.75, y: 3.75, w: 3.4, h: 0.38, fontSize: 7.5, italic: true, color: C.gray, fontFace: "Calibri", align: "center"
});
slide.addShape(pres.shapes.RECTANGLE, { x: 9.75, y: 4.2, w: 3.4, h: 2.65, fill: { color: C.white }, line: { color: C.teal, pt: 1 } });
slide.addImage({ data: img[5], x: 9.8, y: 4.25, w: 3.3, h: 2.3 });
slide.addText("Fig: Sequestrum of chronic osteomyelitis in tibia — dense fragment within lytic area", {
x: 9.75, y: 6.85, w: 3.4, h: 0.35, fontSize: 7.5, italic: true, color: C.gray, fontFace: "Calibri", align: "center"
});
}
// ────────────────────────────────────────────────────────────────────────
// SLIDE 6 - DIAGNOSIS FLOWCHART + TREATMENT
// ────────────────────────────────────────────────────────────────────────
{
let slide = pres.addSlide();
addHeader(slide, "DIAGNOSIS FLOWCHART & TREATMENT", "Rosen's Emergency Medicine | Bailey & Love 28e | Campbell's Orthopaedics 15e");
// LEFT - Diagnostic flowchart image
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 4.5, h: 5.0, fill: { color: C.white }, line: { color: C.teal, pt: 1.5 } });
slide.addText("DIAGNOSTIC ALGORITHM", { x: 0.15, y: 0.85, w: 4.5, h: 0.28, fontSize: 9.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", fill: { color: C.navy } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 4.5, h: 0.28, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("DIAGNOSTIC ALGORITHM", { x: 0.15, y: 0.85, w: 4.5, h: 0.28, fontSize: 9.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
slide.addImage({ data: img[7], x: 0.25, y: 1.2, w: 4.3, h: 4.45 });
slide.addText("Fig: Imaging algorithm for diagnosis of osteomyelitis in ED — Rosen's Emergency Medicine Fig 125.2", {
x: 0.15, y: 5.88, w: 4.5, h: 0.3, fontSize: 7, italic: true, color: C.gray, fontFace: "Calibri", align: "center"
});
// MIDDLE - Treatment (Medical)
slide.addShape(pres.shapes.RECTANGLE, { x: 4.8, y: 0.85, w: 4.1, h: 0.28, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("ANTIBIOTIC TREATMENT", { x: 4.8, y: 0.85, w: 4.1, h: 0.28, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
// Treatment flowchart
const txSteps = [
{ t: "Confirm diagnosis", sub: "Blood culture + Bone biopsy BEFORE antibiotics (if safe)", bg: C.navy },
{ t: "↓" },
{ t: "Empirical IV antibiotics", sub: "Based on age/setting/local MRSA prevalence", bg: C.teal },
{ t: "↓" },
{ t: "Adjust to sensitivities", sub: "When culture results return (48–72 hrs)", bg: "1A6B8A" },
{ t: "↓" },
{ t: "Monitor CRP + clinical response", sub: "Switch to oral when improving (CRP falling)", bg: C.orange },
{ t: "↓" },
{ t: "Total duration: 4–6 weeks minimum", sub: "Longer for chronic; vertebral = 8–12 wks", bg: C.red },
];
let txY = 1.18;
txSteps.forEach((s) => {
if (s.t === "↓") {
slide.addText("↓", { x: 4.8, y: txY, w: 4.1, h: 0.18, fontSize: 14, color: C.orange, fontFace: "Calibri", align: "center", bold: true });
txY += 0.18;
} else {
slide.addShape(pres.shapes.RECTANGLE, { x: 4.8, y: txY, w: 4.1, h: 0.27, fill: { color: s.bg }, line: { color: s.bg } });
slide.addText(s.t, { x: 4.85, y: txY, w: 4.0, h: 0.27, fontSize: 9, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
txY += 0.27;
slide.addText(s.sub, { x: 4.85, y: txY, w: 4.0, h: 0.26, fontSize: 8, color: C.dark, fontFace: "Calibri" });
txY += 0.28;
}
});
// Antibiotic table
slide.addShape(pres.shapes.RECTANGLE, { x: 4.8, y: 3.92, w: 4.1, h: 0.25, fill: { color: C.teal }, line: { color: C.teal } });
slide.addText("EMPIRICAL ANTIBIOTIC SELECTION", { x: 4.8, y: 3.92, w: 4.1, h: 0.25, fontSize: 8.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const abxRows = [
["Patient", "First Choice", "Alternative"],
["Children (general)", "Flucloxacillin IV", "Clindamycin"],
["Children (MRSA)", "Vancomycin IV", "Linezolid"],
["Adults (community)", "Flucloxacillin / Nafcillin", "Vancomycin"],
["Adults (MRSA)", "Vancomycin IV", "Daptomycin"],
["Sickle Cell", "Fluoroquinolone +\nanti-Staph", "Ceftriaxone"],
["Post-surgical", "Pip-Tazobactam\n(broad spectrum)", "Meropenem"],
["TB Osteomyelitis", "HRZE × 2 months\nthen HR × 10 months", "Per sensitivities"],
];
const abxColW = [1.3, 1.5, 1.25];
let abxY = 4.2;
abxRows.forEach((row, ri) => {
let abxX = 4.8;
row.forEach((cell, ci) => {
const isH = ri === 0;
const bg = isH ? C.navy : (ri % 2 === 0 ? C.ltblue : C.white);
const rH = (ri >= 5) ? 0.43 : 0.33;
slide.addShape(pres.shapes.RECTANGLE, { x: abxX, y: abxY, w: abxColW[ci], h: rH, fill: { color: bg }, line: { color: C.teallt, pt: 0.4 } });
slide.addText(cell, { x: abxX + 0.04, y: abxY, w: abxColW[ci] - 0.08, h: rH, fontSize: isH ? 7.5 : 7.5, bold: isH, color: isH ? C.white : C.dark, fontFace: "Calibri", valign: "middle" });
abxX += abxColW[ci];
});
const rH = (ri >= 5) ? 0.43 : 0.33;
abxY += rH;
});
// RIGHT - Surgical Treatment
slide.addShape(pres.shapes.RECTANGLE, { x: 9.05, y: 0.85, w: 4.1, h: 0.28, fill: { color: C.orange }, line: { color: C.orange } });
slide.addText("SURGICAL TREATMENT", { x: 9.05, y: 0.85, w: 4.1, h: 0.28, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const surgRows = [
["Indication", "Procedure"],
["Abscess / pus under pressure", "Drainage (needle or surgical)"],
["Subperiosteal abscess", "Surgical decompression"],
["Sequestrum present", "Sequestrectomy (remove dead bone)"],
["Failed medical management", "Debridement + dead space management"],
["Infected hardware", "Hardware removal (usually)"],
["Soft tissue defect after debridement", "Muscle flap / free flap coverage"],
["Bone defect post-debridement", "Bone graft / Masquelet technique"],
["Refractory / limb-threatening", "Amputation (selected cases)"],
];
const sColW = [2.0, 2.05];
let sCurY = 1.16;
surgRows.forEach((row, ri) => {
let sCurX = 9.05;
row.forEach((cell, ci) => {
const isH = ri === 0;
const bg = isH ? C.teal : (ri % 2 === 0 ? C.ltblue : C.white);
slide.addShape(pres.shapes.RECTANGLE, { x: sCurX, y: sCurY, w: sColW[ci], h: 0.4, fill: { color: bg }, line: { color: C.teallt, pt: 0.4 } });
slide.addText(cell, { x: sCurX + 0.04, y: sCurY, w: sColW[ci] - 0.08, h: 0.4, fontSize: isH ? 8.5 : 7.5, bold: isH, color: isH ? C.white : C.dark, fontFace: "Calibri", valign: "middle" });
sCurX += sColW[ci];
});
sCurY += 0.4;
});
// Dead space management
slide.addShape(pres.shapes.RECTANGLE, { x: 9.05, y: 4.82, w: 4.1, h: 0.25, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("DEAD SPACE MANAGEMENT", { x: 9.05, y: 4.82, w: 4.1, h: 0.25, fontSize: 9, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const dsItems = [
"• Antibiotic-loaded PMMA cement beads (non-biodegradable)",
"• Biodegradable carriers — calcium sulphate, hydroxyapatite",
"• Muscle / soft tissue flap coverage",
"• Bone transport (Ilizarov) for large defects",
];
dsItems.forEach((d, i) => {
slide.addShape(pres.shapes.RECTANGLE, { x: 9.05, y: 5.1 + i * 0.31, w: 4.1, h: 0.29, fill: { color: i % 2 === 0 ? C.ltblue : C.white }, line: { color: C.teallt, pt: 0.3 } });
slide.addText(d, { x: 9.1, y: 5.1 + i * 0.31, w: 4.0, h: 0.29, fontSize: 8, color: C.dark, fontFace: "Calibri", valign: "middle" });
});
}
// ────────────────────────────────────────────────────────────────────────
// SLIDE 7 - SPECIAL FORMS + HIGH-YIELD SUMMARY
// ────────────────────────────────────────────────────────────────────────
{
let slide = pres.addSlide();
addHeader(slide, "SPECIAL FORMS & HIGH-YIELD EXAM SUMMARY", "All Sources");
// LEFT - Special forms
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 6.3, h: 0.28, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("SPECIAL FORMS OF OSTEOMYELITIS", { x: 0.15, y: 0.85, w: 6.3, h: 0.28, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const specials = [
{
title: "BRODIE ABSCESS (Subacute OM)",
color: C.teal,
points: [
"Chronic walled-off intraosseous abscess",
"Localized pain, minimal systemic symptoms",
"X-ray: Well-defined lytic lesion + SCLEROTIC RIM",
"MRI: PENUMBRA SIGN — high-signal ring (granulation tissue) around low-signal abscess",
"Treatment: Surgical drainage + curettage + antibiotics",
]
},
{
title: "VERTEBRAL OSTEOMYELITIS / POTT'S DISEASE (TB Spine)",
color: C.orange,
points: [
"Adults: vertebral OM often coexists with diskitis",
"Children: isolated diskitis more common",
"Back pain ± radiculopathy ± fever; may refuse to walk",
"MRI best: vertebral + disc involvement + intraspinal complications",
"CT-guided aspiration: cultures positive 30–60%",
"TB spine (Pott's): kyphosis + paraplegia (Pott's paraplegia) as complications",
"Treatment: ATT 12+ months; surgery for instability/cord compression",
]
},
{
title: "TUBERCULOUS DACTYLITIS (Spina Ventosa)",
color: "6B3A9F",
points: [
"Rare TB osteomyelitis of small bones",
"Cyst-like cavities + diaphyseal expansion",
"Hands > Feet",
"Treatment: Standard ATT",
]
},
{
title: "DIABETIC FOOT OSTEOMYELITIS",
color: C.red,
points: [
"Neuropathy masks pain → late presentation",
"Secondary to soft tissue ulceration → CONTIGUOUS spread",
"Plain X-ray first; MRI for extent",
"Management: debridement + prolonged Abx ± revascularization",
"Probe-to-bone test: positive = 89% PPV for osteomyelitis",
]
},
{
title: "POSTTRAUMATIC / POST-SURGICAL OM",
color: "4A5568",
points: [
"Open fractures, burns, bites, surgery",
"Gustilo classification guides antibiotic treatment",
"Often polymicrobial; hardware often needs removal",
"Rate: 0.05% open long-bone fractures; 1–2% prosthetic joints",
"Early (<12 wks): likely surgical contamination; Late: haematogenous",
]
},
];
let spY = 1.17;
specials.forEach((sp) => {
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: spY, w: 6.3, h: 0.24, fill: { color: sp.color }, line: { color: sp.color } });
slide.addText(sp.title, { x: 0.2, y: spY, w: 6.2, h: 0.24, fontSize: 8.5, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
spY += 0.24;
const blockH = sp.points.length * 0.26;
sp.points.forEach((p, i) => {
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: spY, w: 6.3, h: 0.24, fill: { color: i % 2 === 0 ? C.ltblue : C.white }, line: { color: C.teallt, pt: 0.3 } });
slide.addText("• " + p, { x: 0.25, y: spY, w: 6.1, h: 0.24, fontSize: 7.5, color: C.dark, fontFace: "Calibri", valign: "middle" });
spY += 0.24;
});
spY += 0.05;
});
// RIGHT - High yield summary
slide.addShape(pres.shapes.RECTANGLE, { x: 6.6, y: 0.85, w: 6.55, h: 0.28, fill: { color: C.orange }, line: { color: C.orange } });
slide.addText("HIGH-YIELD EXAM POINTS ★", { x: 6.6, y: 0.85, w: 6.55, h: 0.28, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0 });
const highYield = [
{ num: "1", text: "Most common organism overall = S. aureus (80–90% culture-positive cases)" },
{ num: "2", text: "Sickle cell = Salmonella (osteonecrosis nidus + impaired splenic function)" },
{ num: "3", text: "Neonates = Group B Strep + E. coli; metaphysis AND epiphysis AND joint can all be involved simultaneously" },
{ num: "4", text: "Metaphysis = preferred site due to SLOW sinusoidal blood flow + microtrauma" },
{ num: "5", text: "SEQUESTRUM = dead bone; INVOLUCRUM = new reactive periosteal bone shell around sequestrum" },
{ num: "6", text: "X-ray LAG = 10–21 days behind clinical disease. MRI = investigation of choice for early diagnosis" },
{ num: "7", text: "Brodie abscess = subacute walled-off abscess; lytic lesion + sclerotic rim; PENUMBRA SIGN on MRI" },
{ num: "8", text: "Cierny-Mader = gold standard classification; 4 anatomic types × 3 host classes = 12 stages" },
{ num: "9", text: "MARJOLIN'S: Longstanding draining sinus → SCC (squamous cell carcinoma). Signs: ↑ pain, ↑ discharge, foul smell → BIOPSY" },
{ num: "10", text: "Pott's disease = TB osteomyelitis of spine; complications include kyphosis + paraplegia" },
{ num: "11", text: "Treatment principle = 'Drain pus, give antibiotics'. IV first → switch to oral when clinically improving (CRP falling)" },
{ num: "12", text: "PVL-positive MRSA (Panton-Valentine leukocidin) = more aggressive; higher morbidity; affects antibiotic choice" },
{ num: "13", text: "Diabetic foot OM: CONTIGUOUS spread; late presentation due to neuropathy; probe-to-bone test = 89% PPV" },
{ num: "14", text: "AHO in children: Male > Female (2:1 to 3:1 ratio); blood cultures positive only 40% of cases" },
{ num: "15", text: "Chronic OM: 5–25% of acute OM fails to resolve; complications include amyloidosis, endocarditis, SCC, sarcoma" },
];
highYield.forEach((item, i) => {
const y = 1.17 + i * 0.38;
const bg = i % 2 === 0 ? "FFF8E1" : C.white;
slide.addShape(pres.shapes.RECTANGLE, { x: 6.6, y, w: 6.55, h: 0.36, fill: { color: bg }, line: { color: "FFE082", pt: 0.5 } });
slide.addShape(pres.shapes.RECTANGLE, { x: 6.6, y, w: 0.32, h: 0.36, fill: { color: C.orange }, line: { color: C.orange } });
slide.addText(item.num, { x: 6.6, y, w: 0.32, h: 0.36, fontSize: 9, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
slide.addText(item.text, { x: 6.95, y: y + 0.01, w: 6.15, h: 0.34, fontSize: 7.5, color: C.dark, fontFace: "Calibri", valign: "middle" });
});
// Bottom source
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 7.3, w: 13.3, h: 0.22, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("Bailey & Love 28e | Robbins & Kumar Pathologic Basis of Disease | Campbell's Operative Orthopaedics 15e | Rosen's Emergency Medicine | Rockwood & Green's Fractures in Adults 10e | Grainger & Allison's Diagnostic Radiology", {
x: 0, y: 7.3, w: 13.3, h: 0.22, fontSize: 6.5, color: C.teallt, fontFace: "Calibri", align: "center", italic: true, margin: 0
});
}
// ────────────────────────────────────────────────────────────────────────
// SLIDE 8 - COMPARISON TABLE: ACUTE vs CHRONIC
// ────────────────────────────────────────────────────────────────────────
{
let slide = pres.addSlide();
addHeader(slide, "ACUTE vs CHRONIC OSTEOMYELITIS — COMPARISON TABLE", "All Sources");
slide.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 12.95, h: 0.3, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText("COMPREHENSIVE COMPARISON: ACUTE vs CHRONIC OSTEOMYELITIS", {
x: 0.15, y: 0.85, w: 12.95, h: 0.3, fontSize: 11, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0
});
const compareRows = [
["Feature", "ACUTE OSTEOMYELITIS", "CHRONIC OSTEOMYELITIS"],
["Duration", "< 2 weeks (inflammatory changes present)", "> 6 weeks (bone destruction + sequestra)"],
["Pathology", "Neutrophilic infiltrate, bone/marrow necrosis, abscess formation", "Sequestrum, involucrum, marrow fibrosis, lymphocytes + plasma cells"],
["Organisms", "S. aureus (mainly); age-specific (see microbiology)", "S. aureus, polymicrobial (especially post-traumatic)"],
["Systemic Symptoms", "High fever, rigors, malaise, appear toxic", "Low-grade or absent; chronic draining sinus"],
["Local Signs", "Point tenderness, swelling, warmth, erythema", "Sinus tracts, palpable sequestrum/involucrum"],
["X-ray", "Often NORMAL initially; only soft tissue swelling\n(lag of 10–21 days!)", "Sequestrum, involucrum, 'bone-within-bone', sclerosis, cortical destruction"],
["MRI", "High T2/STIR marrow signal; rim enhancement of abscess", "Low signal sequestrum; ring enhancement; intramedullary changes"],
["Bone Scan", "Hot (3-phase positive)", "May be falsely negative (avascular area)"],
["Treatment", "IV antibiotics ± aspiration/drainage; switch to oral when improving", "Debridement + sequestrectomy + long-course antibiotics + reconstruction"],
["Duration of Abx", "4–6 weeks (can shorten if improving)", "6–12 weeks; may need indefinite suppressive therapy"],
["Prognosis", "Good if treated promptly; 5–25% fail to resolve → chronic", "Flares after years; risk of amyloidosis, SCC, sarcoma; amputation sometimes needed"],
["Special Forms", "Haematogenous (children), post-traumatic (adults)", "Brodie abscess (subacute); Cierny-Mader staging used here"],
];
const cColW = [2.5, 5.2, 5.2];
let cCurY = 1.18;
compareRows.forEach((row, ri) => {
let cCurX = 0.15;
const isH = ri === 0;
const rH = isH ? 0.32 : (ri >= 6 && ri <= 7 ? 0.52 : 0.38);
row.forEach((cell, ci) => {
let bg;
if (isH) {
bg = ci === 0 ? C.navy : (ci === 1 ? C.teal : C.orange);
} else {
bg = ci === 0 ? C.ltgray : (ci === 1 ? (ri % 2 === 0 ? "E3F2F7" : C.white) : (ri % 2 === 0 ? "FFF3E0" : C.white));
}
slide.addShape(pres.shapes.RECTANGLE, { x: cCurX, y: cCurY, w: cColW[ci], h: rH, fill: { color: bg }, line: { color: C.teallt, pt: 0.5 } });
slide.addText(cell, {
x: cCurX + 0.06, y: cCurY, w: cColW[ci] - 0.12, h: rH,
fontSize: isH ? 10 : 8,
bold: isH || ci === 0,
color: isH ? C.white : (ci === 0 ? C.navy : C.dark),
fontFace: "Calibri",
valign: "middle"
});
cCurX += cColW[ci];
});
cCurY += rH;
});
// Bottom note
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.15, y: 6.9, w: 12.95, h: 0.38, fill: { color: "FFF3CD" }, line: { color: C.gold, pt: 1.5 }, rectRadius: 0.05 });
slide.addText([
{ text: "★ KEY EXAM PEARL: ", options: { bold: true, color: C.orange } },
{ text: "X-ray in acute osteomyelitis is NORMAL for the first 10–21 days — periosteal reaction and lytic changes appear only AFTER significant bone destruction. MRI is the gold standard for early diagnosis. ESR may remain elevated even after clinical improvement — use CRP to monitor treatment response.", options: { color: C.dark } }
], { x: 0.25, y: 6.93, w: 12.75, h: 0.32, fontSize: 8.5, fontFace: "Calibri", valign: "middle" });
}
// ────────────────────────────────────────────────────────────────────────
// Save
// ────────────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/osteomyelitis-poster/Osteomyelitis_Exam_Poster.pptx" })
.then(() => console.log("✅ Poster saved successfully!"))
.catch(err => { console.error("❌ Error:", err); process.exit(1); });
Running Command
cd /home/daytona/workspace/osteomyelitis-poster && node build_poster.js 2>&1
Running Command
ls -lh /home/daytona/workspace/osteomyelitis-poster/Osteomyelitis_Exam_Poster.pp…
Your exam revision poster is ready! Download it here:
Osteomyelitis Exam Poster
Presentation · PPTX
What's inside (8 slides, WIDE 13.3" × 7.5" format):
| Slide | Content |
|---|---|
| 1 - Title | Full definition, 5 quick-recall fact cards (organism, site, key pathology, imaging, X-ray lag) |
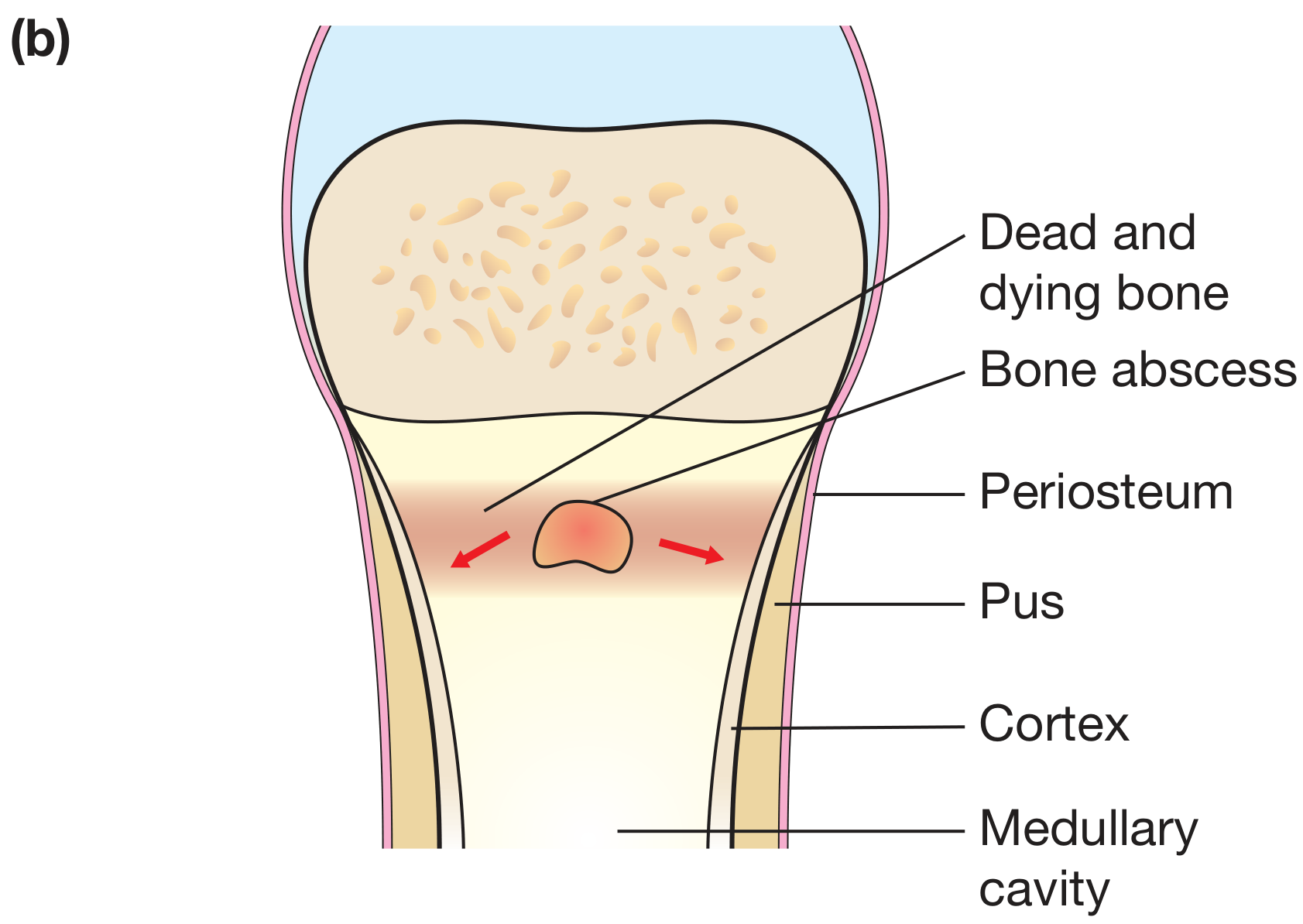
| 2 - Routes & Pathogenesis | Routes of infection table, haematogenous spread diagram (Bailey & Love), bone abscess anatomy diagram, site-by-age table |
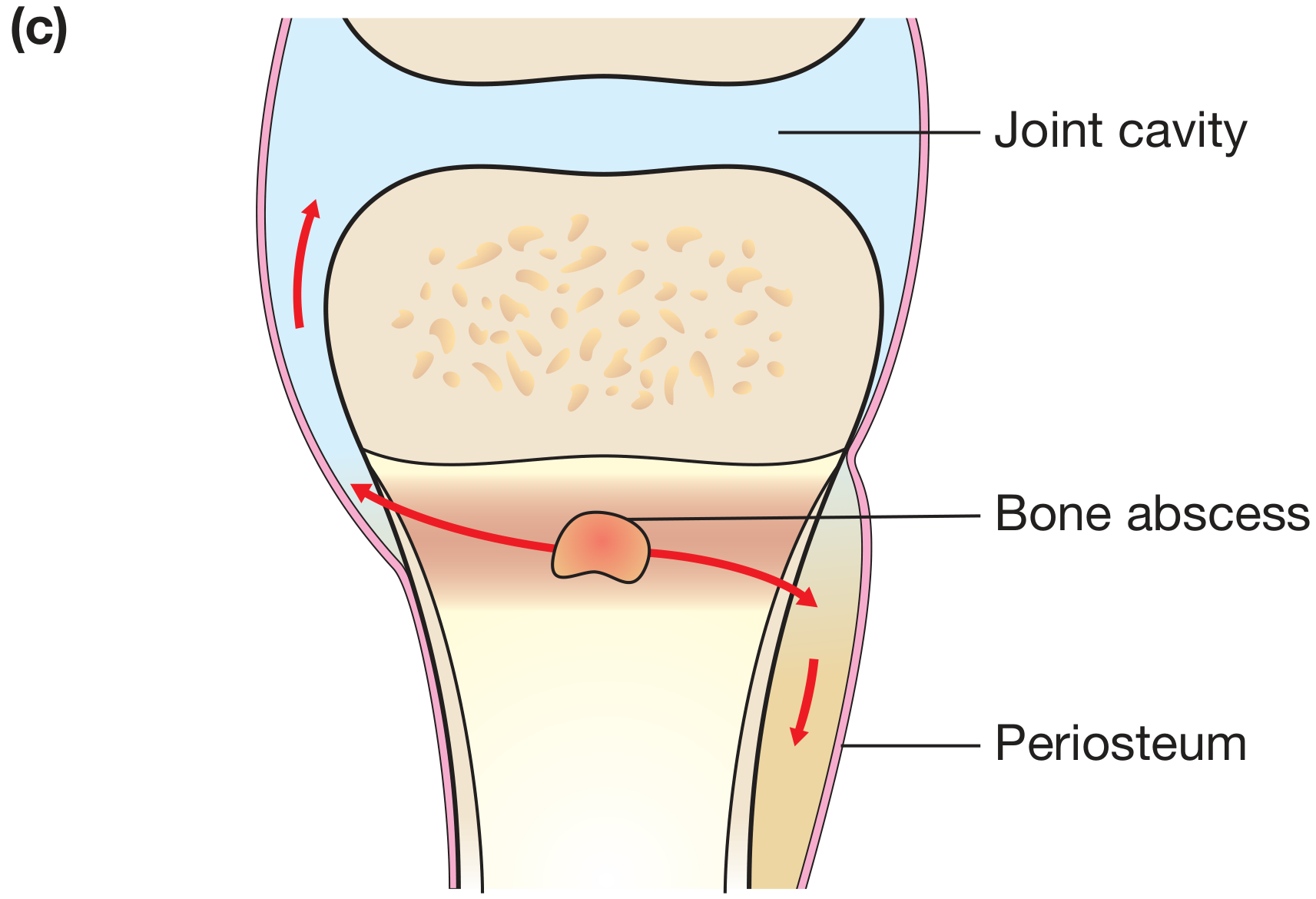
| 3 - Pathology | Colour-coded pathogenesis flowchart (Bacteraemia → Sequestrum), joint spread diagram, gross specimen photo (sequestrum in involucrum), histological stages table, key terms reference |
| 4 - Microbiology & Classification | Full microbiology table by patient group, Cierny-Mader anatomic types + physiologic host classes, types-of-OM body diagram (Rockwood & Green), classification by duration |
| 5 - Clinical Features & Investigations | Systemic vs local features boxes, chronic OM features, complications (incl. Marjolin's), full investigations table, Brodie abscess X-ray + sequestrum tibia X-ray |
| 6 - Diagnosis & Treatment | Diagnostic algorithm flowchart (Rosen's EM), IV→oral antibiotic protocol, empirical antibiotic table by setting, surgical indications table, dead space management options |
| 7 - Special Forms & High-Yield Points | Brodie abscess, Vertebral OM/Pott's, Tuberculous dactylitis, Diabetic foot, Post-traumatic OM; 15 high-yield exam pearls with numbered badges |
| 8 - Comparison Table | Full Acute vs Chronic OM side-by-side: pathology, organisms, symptoms, imaging, treatment, prognosis + key exam pearl box |
This is a shared conversation. Sign in to Orris to start your own chat.