Give me all details about acute cholecystitis and cholecystectomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute cholecystitis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative sources. Let me compile the full, detailed answer.
Acute Cholecystitis and Cholecystectomy: Complete Guide
PART 1: ACUTE CHOLECYSTITIS
Definition
Acute cholecystitis is acute inflammation of the gallbladder, most commonly caused by obstruction of the cystic duct. It is the primary complication of gallstone disease and the most common reason for emergency cholecystectomy.
- Robbins Pathologic Basis of Disease, p.1841
Epidemiology & Classification
| Type | Prevalence | Key Feature |
|---|---|---|
| Calculous (acute) | ~90% of cases | Gallstone obstructing cystic duct/neck |
| Acalculous | ~10% of cases | Ischemia/stasis; critically ill patients |
Acute calculous cholecystitis is particularly common in diabetic patients with symptomatic gallstones. Acalculous cholecystitis carries higher morbidity and mortality than calculous cholecystitis.
Pathophysiology
Calculous cholecystitis:
- A stone obstructs the neck of the gallbladder or cystic duct
- Chemical irritation ensues: mucosal phospholipases hydrolyze luminal lecithins into toxic lysolecithins
- The protective glycoprotein mucus layer is disrupted, exposing mucosa to the direct detergent action of bile salts
- Prostaglandins released within the distended gallbladder wall contribute to mucosal and mural inflammation
- Increased intraluminal pressure compromises blood flow to the mucosa
- These events initially occur WITHOUT bacterial infection; bacterial superinfection occurs later and exacerbates inflammation
Acalculous cholecystitis:
-
Primarily results from ischemia - the cystic artery is an end artery with no collateral circulation
-
Contributing factors: wall edema (compromising blood flow), gallbladder stasis from biliary sludge and mucus causing functional cystic duct obstruction
-
Risk factors: (1) sepsis with hypotension/multiorgan failure; (2) immunosuppression; (3) major trauma and burns; (4) diabetes mellitus; (5) infections
-
Robbins Pathologic Basis of Disease, p.1841-1847
Morphology (Pathological Features)
-
Gallbladder is enlarged and tense, may show bright red, violaceous, or green-black discoloration from subserosal hemorrhages
-
Serosa covered by fibrinous exudate (fibrinopurulent in severe cases)
-
Lumen contains turbid bile mixed with fibrin, pus, and hemorrhage
-
Obstructing stone present in neck/cystic duct in calculous form
-
Mild cases: Gallbladder wall thickened, edematous, hyperemic
-
Severe forms:
- Empyema: Lumen filled with virtually pure pus
- Gangrenous cholecystitis: Green-black necrotic organ with perforations
- Emphysematous cholecystitis: Gas-forming organisms (Clostridia, coliforms) invade the wall
-
Histology: Edema, congestion, mucosal erosion; neutrophils sparse unless superinfected
-
Robbins Pathologic Basis of Disease, p.1852
Clinical Features
- Prior episodes of biliary pain are common (but not universal)
- Attack begins with progressive RUQ or epigastric pain lasting >6 hours (distinguishes from biliary colic)
- Fever, anorexia, tachycardia, sweating, nausea, vomiting
- Most patients are afebrile initially - jaundice suggests common bile duct obstruction (Mirizzi syndrome or choledocholithiasis)
- Murphy's sign: Inspiratory arrest on deep palpation of RUQ (positive in ~80%)
- Boas' sign: Hyperesthesia below the right scapula (referred pain via phrenic nerve)
- Leukocytosis (WBC typically 12,000-15,000/mm³; >15,000 suggests gangrene or perforation)
- Mild elevations in alkaline phosphatase, bilirubin, and transaminases may occur
Diagnostic Workup
Laboratory:
- CBC (leukocytosis), LFTs (mild elevation common), serum bilirubin, amylase/lipase (exclude pancreatitis)
- Blood cultures if sepsis suspected
Imaging:
| Modality | Findings | Sensitivity/Specificity |
|---|---|---|
| RUQ Ultrasound (first-line) | Gallstones, gallbladder wall thickening (>3mm), pericholecystic fluid, sonographic Murphy's sign | 88-94% / 78-80% |
| HIDA Scan (cholescintigraphy) | Non-visualization of gallbladder = cystic duct obstruction | 96% / 90% |
| CT Scan | Emphysematous cholecystitis, pericholecystic abscess, perforation, peritonitis | Best for complications |
HIDA scan is recommended when ultrasound is inconclusive or discordant with clinical findings.
- Mulholland & Greenfield's Surgery 7e, p.461
Severity Grading: Tokyo Guidelines (TG18)
| Grade | Description | Clinical Criteria |
|---|---|---|
| Grade I (Mild) | Localized inflammation, no organ dysfunction | WBC <18,000; mild symptoms |
| Grade II (Moderate) | Marked local inflammation | WBC >18,000; palpable mass; duration >72h; marked local inflammation |
| Grade III (Severe) | Organ dysfunction | Cardiovascular, neurological, respiratory, renal, hepatic, or hematological dysfunction |
Treatment decisions are based on severity grade and patient comorbidities (ASA classification). Higher severity grades are associated with worse outcomes, prolonged hospital stay, and higher conversion-to-open rates.
The AAST Emergency General Surgery (EGS) grades also stratify from Grade I (localized inflammation) to Grade V (pericholecystic abscess, bilioenteric fistula, peritonitis).
- Sabiston Textbook of Surgery, p.1831
Microbiology
Bile cultures are positive in >40% of cases. Common pathogens:
- Gram-negative aerobic: E. coli, Klebsiella, Enterobacter, Proteus
- Gram-positive aerobic: Enterococcus, Streptococcus
- Anaerobes: ~15% of isolates; Clostridium species in emphysematous cholecystitis
Management
Initial (all patients):
- NPO (nothing by mouth)
- IV hydration and electrolyte restoration
- IV antibiotics - directed against above pathogens:
- Mild-moderate: Cefoxitin (cephalosporin)
- Severe: Piperacillin-tazobactam OR third-generation cephalosporin + metronidazole
- Gangrenous/emphysematous: Must include anaerobic coverage
- Parenteral analgesia
- If source control achieved with surgery, post-op antibiotics not needed in mild-moderate cholecystitis
- Continue postoperative antibiotics in: severe infection, intraoperative perforation, gangrenous cholecystitis
Definitive Treatment - Surgery Timing:
Based on 7 pooled randomized controlled trials, early cholecystectomy (within 72 hours) is superior to delayed surgery (6-8 weeks):
| Early | Delayed | |
|---|---|---|
| Patients | 378 | 364 |
| Mortality | 0% | 2.0% |
| Bile duct injuries | 0 | 0 |
| Mean hospital stay | 9.6 days | 17.8 days |
| Failure rate | N/A | 26% |
Early operation reduces total hospitalization, reduces costs, prevents progressive cholecystitis deaths, and does NOT substantially increase bile duct injury risk.
- Sleisenger & Fordtran's GI & Liver Disease, p.1263
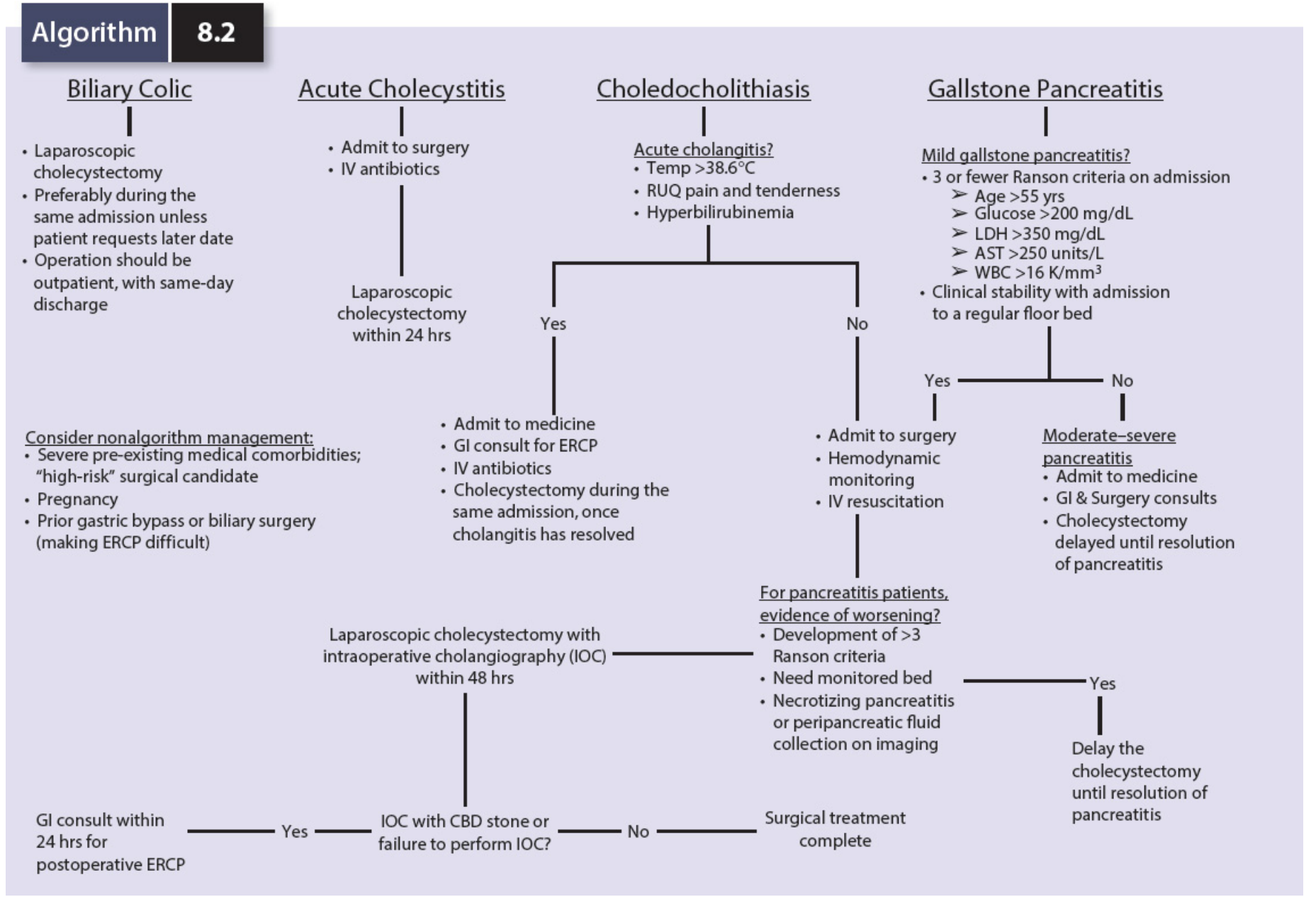
Algorithm overview:
Special Populations
- Diabetic patients: Higher frequency of infectious complications (sepsis); early cholecystectomy is warranted
- Elderly patients: Deceptively benign presentation but high rates of occult severe cholecystitis including empyema and gangrene; early cholecystectomy warranted
- High-risk surgical patients (severe liver/pulmonary/cardiac failure): Cholecystostomy (gallbladder drainage) preferred; percutaneous approach is standard
- Pregnancy: See recent 2025 meta-analysis (PMID 40610639) showing operative vs. nonoperative management data
- Septic/hemodynamically unstable patients: Percutaneous cholecystostomy tube provides source control; mortality up to 35% in severe cholecystitis
Percutaneous cholecystostomy indications: high surgical risk rather than severity of cholecystitis alone. After recovery, laparoscopic cholecystectomy should be performed if condition permits. ~50% of cholecystostomy-only patients develop recurrent biliary symptoms.
Endoscopic transmural gallbladder drainage (connecting gallbladder to duodenum via endoluminal stent) is as effective as percutaneous drainage in patients unfit for surgery - but NOT for patients who may become surgical candidates later (duodenum repair adds complexity).
Complications of Acute Cholecystitis
| Complication | Features |
|---|---|
| Empyema | Pus-filled gallbladder; high fever, leukocytosis |
| Gangrenous cholecystitis | Necrosis; male sex, DM, CVD, WBC >15,000 are risk factors |
| Emphysematous cholecystitis | Gas in gallbladder wall on CT; Clostridium/coliforms; DM common |
| Perforation | Free perforation (peritonitis) or walled-off (pericholecystic abscess) |
| Mirizzi syndrome | Large stone compresses common hepatic duct from outside |
| Cholecystoenteric fistula | Gallstone erodes into duodenum or colon |
| Gallstone ileus | Large stone traverses fistula into bowel; causes SBO |
| Malignant transformation | Chronic cholecystitis → gallbladder carcinoma (rare) |
PART 2: CHOLECYSTECTOMY
Overview
Cholecystectomy is one of the most common abdominal operations in Western countries, with over 750,000 performed annually in the United States alone. Key historical milestones:
-
1882: Carl Langenbuch performed the first successful open cholecystectomy
-
1987: Philippe Mouret introduced laparoscopic cholecystectomy in France
-
Laparoscopic approach rapidly became the gold standard and largely ended non-surgical therapies (lithotripsy, bile salts)
-
Schwartz's Principles of Surgery 11e, p.1438
Types of Cholecystectomy
- Laparoscopic cholecystectomy - standard of care
- Robotic cholecystectomy - equivalent outcomes, longer operative time
- Open cholecystectomy - conversion or specific indications
- Subtotal cholecystectomy (fenestrating or reconstituting) - for hostile hepatocystic triangle
Indications
- Symptomatic cholelithiasis (biliary colic)
- Acute cholecystitis (early or interval)
- Chronic cholecystitis
- Gallbladder polyps >10mm or with risk features
- Biliary dyskinesia (ejection fraction <35%)
- Gallstone pancreatitis
- Porcelain gallbladder (if associated with malignancy risk)
Contraindications
Absolute contraindications to laparoscopic approach:
- Hemodynamic instability
- Uncontrolled coagulopathy
- Frank peritonitis
Relative contraindications (now considered risk factors for difficult cholecystectomy, not prohibitive):
- Acute cholecystitis, gangrene, empyema
- Biliary-enteric fistulae
- Obesity, pregnancy
- Ventriculoperitoneal shunts
- Cirrhosis
- Previous upper abdominal surgery
Patients with severe COPD or CHF (EF <20%) may not tolerate CO₂ pneumoperitoneum and may require open approach.
- Schwartz's Principles of Surgery 11e, p.1396-1399
Preoperative Preparation
- Labs: CBC, LFTs; LFT abnormalities may prompt MRCP or ERCP to exclude choledocholithiasis
- DVT prophylaxis: Low molecular weight heparin OR compression stockings
- Bladder: Patient empties bladder preoperatively (avoids urinary catheterization)
- Orogastric tube: Placed if stomach distended; removed at end of operation
- Informed consent: Must include possibility of conversion to open
Laparoscopic Cholecystectomy: Surgical Technique
Step-by-step:
1. Positioning and Access:
- Patient supine; surgeon stands at patient's left
- Split-leg positioning optional for ergonomic RUQ access
- One arm tucked if cholangiogram planned (for fluoroscopy maneuverability)
- Pneumoperitoneum established with CO₂ via:
- Open technique (Hasson)
- Closed Veress needle (supraumbilical)
- Optical viewing trocar
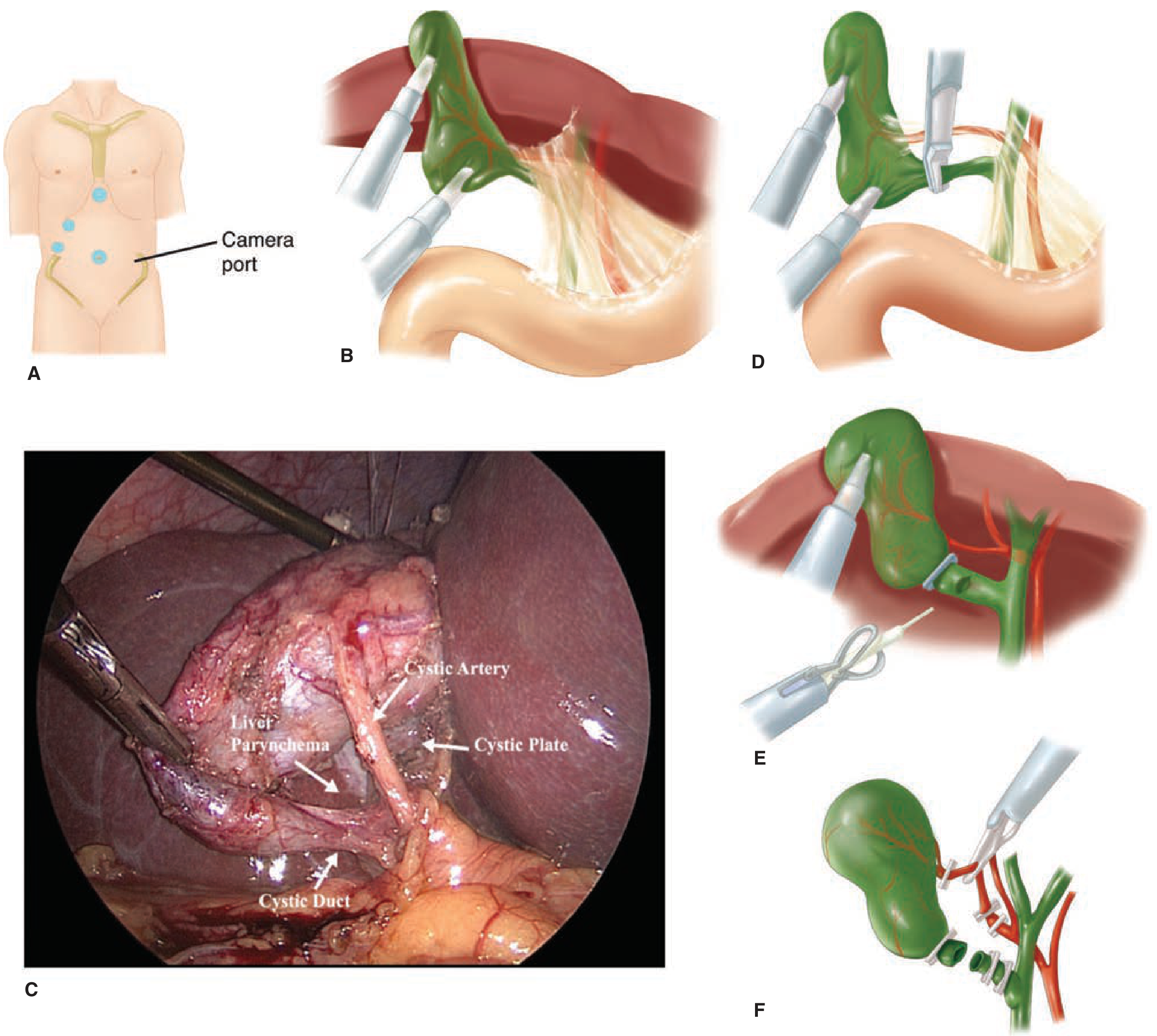
2. Port Placement (standard 4-port technique):
- 5- or 10-mm supraumbilical port: camera (30° laparoscope)
- 10- or 12-mm epigastric port: main operating hand
- 5-mm right midclavicular line port: left-hand grasper
- 5-mm right flank port: retraction/assistance
- Additional ports may be added for difficult cases
3. Retraction and Exposure:
- Lateral port grasper retracts gallbladder fundus cephalad over liver edge toward right shoulder
- Reverse Trendelenburg position with right-side-up tilt improves exposure
- Adhesions between omentum, duodenum, colon and gallbladder taken down first
4. Dissection of the Hepatocystic Triangle:
- Midclavicular port grasper retracts gallbladder infundibulum posterolaterally
- Dissection starts just above the cystic duct takeoff
- Peritoneum, fat, and loose areolar tissue cleared from around cystic duct-gallbladder junction
- Cystic duct and cystic artery (usually parallel to duct, often behind Lund's/Calot's node) are identified
5. Critical View of Safety (CVS) - MANDATORY:
Three criteria must ALL be met:
- Hepatocystic triangle cleared of ALL fat and fibrous tissue
- Lower one-third of gallbladder separated from the liver (cystic plate exposed)
- Two and ONLY two structures seen entering the gallbladder (cystic duct + cystic artery)
CVS is the primary strategy to prevent bile duct injury (BDI).
6. Optional: Intraoperative Cholangiogram (IOC):
- Small opening made in cystic duct; catheter inserted; contrast injected
- Confirms biliary anatomy, detects CBD stones
- Indocyanine green (ICG) fluorescent cholangiography now commonly used: real-time, no radiation, identifies biliary structures before clipping
- Particularly valuable in acute cholecystitis where inflammation distorts anatomy
7. Division:
- Cystic duct: clipped with 2 clips at base, 1 clip on gallbladder side, then divided
- Cystic artery: same clipping technique
- For dilated cystic duct too large for clips: endoloop, laparoscopic stapler, or suture closure
8. Gallbladder Dissection from Liver Bed:
- Electrocautery used to dissect gallbladder from liver
- Watch for abnormal posterior ductal/arterial branches
- Before complete removal, use gallbladder as retractor for final field inspection
- Check for bleeding, bile staining, clip placement
9. Specimen Removal:
- Removed through epigastric or umbilical incision, often with retrieval bag
- Fascial defect enlarged if stones are large or gallbladder very inflamed
- Retrieve any spilled stones
10. Drain placement:
-
NOT routinely required or recommended
-
Consider if severely inflamed/gangrenous gallbladder, expected bile/blood accumulation
-
Placed through 5-mm port under right liver lobe near gallbladder fossa
-
Schwartz's Principles of Surgery 11e, p.1439-1440
Critical View of Safety - Detail
The CVS was specifically designed to minimize bile duct injury. Key point: the hepatocystic triangle (bounded by the cystic duct, common hepatic duct, and liver margin) must be completely cleared before any structure is divided. If CVS cannot be achieved:
- Consider subtotal cholecystectomy (fenestrating removes anterior wall; reconstituting closes the stump)
- Consider conversion to open
- Use IOC or ICG cholangiography to confirm anatomy
Conversion to Open Cholecystectomy
Indications for conversion:
- Patient unable to tolerate pneumoperitoneum
- Complication that cannot be fixed laparoscopically
- Important anatomic structures cannot be clearly identified
- No progress made over a set period
Conversion rates:
- Elective setting: ~5%
- Emergent/complicated disease: 10-30%
Conversion is NOT a failure - it is sound surgical judgment.
Open Cholecystectomy
Approach:
- Midline laparotomy OR (more commonly) right subcostal (Kocher) incision
- Dissection starts at fundus, working proximally to hepatocystic triangle (fundus-first technique)
- Same principles: identify, clip, and divide cystic artery and cystic duct; confirm CVS
- In difficult cases, the cystic duct can be suture-ligated
Robotic Cholecystectomy
-
Extension of the laparoscopic toolset; port placement and technique equivalent
-
Advantages: 3D visualization, wristed instrument movement
-
Outcomes: equivalent mortality and complication rates; slightly longer operative time
-
Early concerns about higher BDI rates have not been confirmed in recent meta-analyses
-
Sabiston Textbook of Surgery
Complications of Cholecystectomy
| Complication | Rate | Notes |
|---|---|---|
| Mortality | ~0.1% (laparoscopic) | Higher for open |
| Bile duct injury (BDI) | 0.3-0.5% | Most serious; may require biliary reconstruction |
| Bile leak | 1-2% | Often from cystic duct stump or ducts of Luschka |
| Wound infection | Lower with laparoscopic | |
| Port-site hernia | Uncommon | More common with 10-12mm ports |
| Dropped stones | Rare | Retrieve all spilled stones; abandoned stones cause delayed abscess |
| Post-cholecystectomy syndrome | 10-15% | Persistent biliary-type pain; rule out retained CBD stone |
| Retained CBD stone | Detected on IOC | Treated with post-op ERCP |
| Cardiopulmonary complications | Lower with laparoscopic | CO₂ pneumoperitoneum increases IAP |
Intraoperative Cholangiogram (IOC) and ERCP Workflow
Per Algorithm 8.2 (Mulholland & Greenfield):
- If IOC reveals CBD stone → GI consult within 24h for post-op ERCP
- If choledocholithiasis suspected preoperatively with acute cholangitis → ERCP first, then cholecystectomy during same admission once cholangitis resolves
Special Considerations
Acute cholecystitis setting:
- Laparoscopic cholecystectomy is feasible in most cases
- Technical problems occasionally occur from severe inflammation obscuring hepatocystic triangle structures
- Cholangiography particularly valuable to confirm ductal anatomy
- Laparoscopic subtotal cholecystectomy or conversion to open are valid alternatives
Post-cholecystectomy drainage:
- Routine use of surgical drains is NOT warranted and may be deleterious
- Sleisenger & Fordtran, p.332
Diabetic patients: Expeditious cholecystectomy - significantly higher infectious complications
Elderly patients: Early cholecystectomy; deceptively mild presentation can mask severe disease
Recent Evidence (2025 PubMed Meta-Analyses)
- PMID 40610639 (2025): Operative vs. nonoperative treatment of acute cholecystitis during pregnancy - systematic review and meta-analysis confirming safety data for surgical approach during pregnancy
- PMID 40483437 (2025, World J Emerg Surg): Percutaneous treatment vs. cholecystectomy in acute cholecystitis - comparing outcomes of drainage vs. definitive surgery
- PMID 40266401 (2025): Incisional hernia after minimally invasive cholecystectomy - impact of comorbidities and surgical approach
Summary Comparison: Laparoscopic vs. Open Cholecystectomy
| Feature | Laparoscopic | Open |
|---|---|---|
| Standard of care | Yes | No (reserved for conversion/laparotomy) |
| Mortality | ~0.1% | Higher |
| Hospital stay | 1-2 days | 3-5 days |
| Return to activity | 1-2 weeks | 4-6 weeks |
| Pain | Less | More |
| BDI rate | Historically higher, now comparable | Historical standard |
| Conversion needed | ~5% elective, 10-30% emergent | N/A |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Robbins Pathology)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- Schwartz's Principles of Surgery, 11th Edition
- Mulholland & Greenfield's Surgery, 7th Edition
- Sabiston Textbook of Surgery
- Current Surgical Therapy, 14th Edition
This is a shared conversation. Sign in to Orris to start your own chat.