A 26-year-old male. Present with history of fever for one month. Uh, following progressive breathlessness and history of cough.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have excellent material. Let me compile the full clinical answer.
Clinical Case Analysis: 26-year-old Male with 1 Month Fever, Progressive Breathlessness & Cough
Step 1 - Differential Diagnosis
Given this presentation (young male, subacute onset, 1 month), the differentials must be approached systematically:
| Priority | Diagnosis | Key Reasoning |
|---|---|---|
| 1st | Pulmonary Tuberculosis (PTB) | Most common cause of subacute fever + cough + breathlessness in a young person, especially in endemic regions |
| 2nd | HIV-related pulmonary disease (PCP, TB-HIV co-infection) | Young male - risk factors must be screened; HIV changes TB presentation entirely |
| 3rd | Bacterial pneumonia (CAP) with complication | Less likely at 1 month without antibiotic response |
| 4th | Lymphoma (Hodgkin's / Mediastinal NHL) | Classic presentation in young adults: B symptoms (fever, night sweats, weight loss) + mediastinal widening |
| 5th | Fungal infections (Histoplasmosis, Cryptococcosis) | Consider if immunocompromised or exposure history |
| 6th | Malignancy with pleural effusion | Less common at 26 but possible |
Step 2 - Why Pulmonary TB is the Top Diagnosis
"The most commonly reported symptom of pulmonary TB is persistent cough... accompanied by systemic symptoms such as fever, night sweats, and weight loss."
This patient fits the classic picture:
- Subacute fever (1 month) - hallmark of TB
- Progressive breathlessness - from consolidation, pleural effusion, or miliary spread
- Persistent cough - cardinal symptom
Critical point: Evaluation using any of these symptoms - cough of any duration, fever, night sweats, or weight loss - should prompt TB workup in high-risk groups and high-incidence areas.
Step 3 - Radiographic Patterns to Expect
Murray & Nadel's Textbook of Respiratory Medicine, p. 1187-1188:
Primary TB (recent infection - more likely in a 26-year-old):
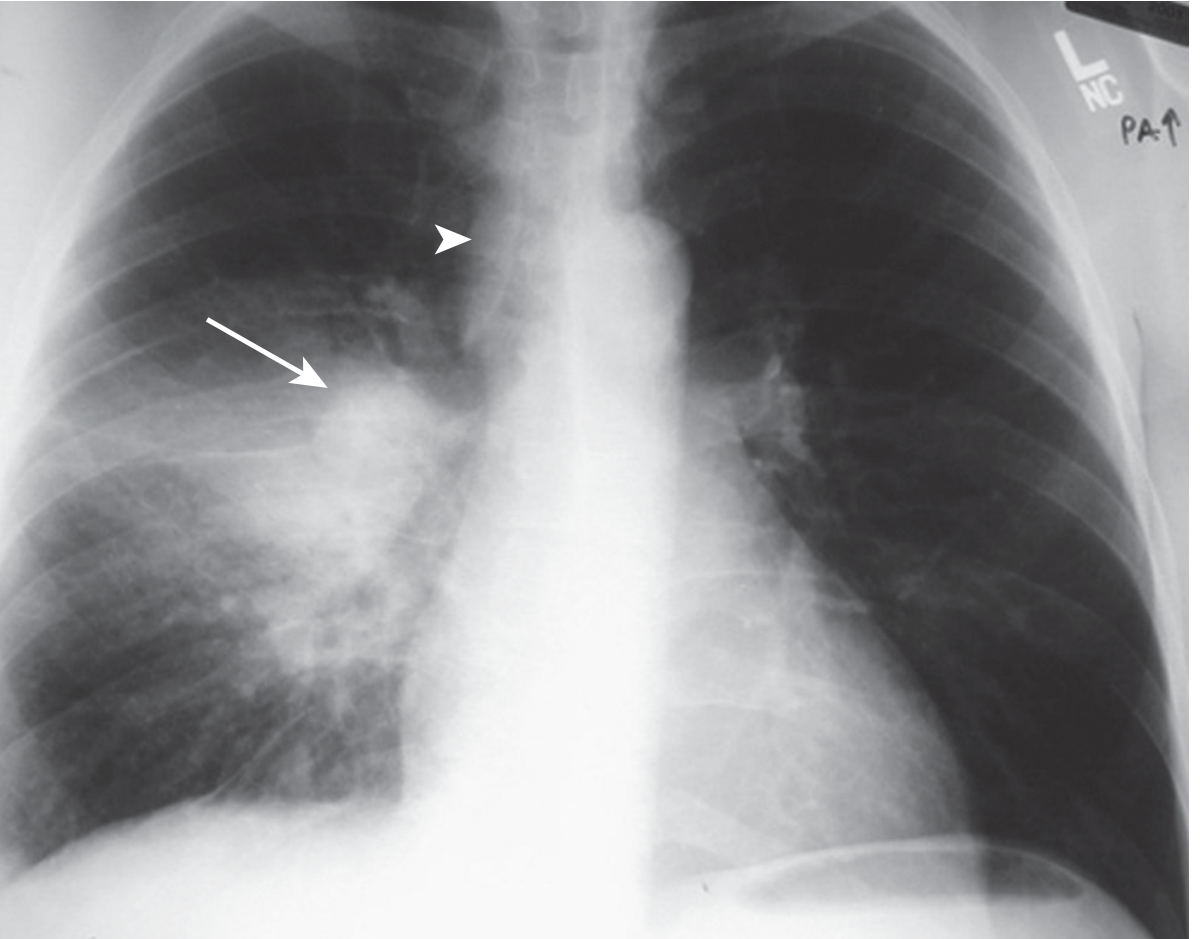
Middle/lower lung zone opacity + ipsilateral hilar adenopathy. Arrows indicate right lower lobe consolidation with right hilar lymphadenopathy.
Reactivation TB: Upper lobe involvement with cavitation (apical/posterior segments RUL most common)
Miliary TB (disseminated - can cause progressive breathlessness):
Numerous small randomly distributed bilateral nodules - this pattern explains severe progressive dyspnea even in a young patient.
TB in HIV-infected patients: Bilateral hilar lymphadenopathy + parenchymal nodular opacities + lower lobe or diffuse infiltrates (atypical pattern).
Step 4 - Mandatory History Points to Elicit
- Exposure history: Contact with known TB patient; household crowding
- HIV risk factors: Sexual history, IV drug use, prior STIs
- Constitutional symptoms: Night sweats, weight loss (quantify), anorexia
- Character of cough: Productive? Hemoptysis (suggests cavity or advanced disease)?
- Travel/occupation: Exposure to endemic fungal areas
- Immunosuppression: Steroids, biologics, diabetes mellitus
- BCG vaccination status
- Prior TB treatment history
Step 5 - Recommended Workup
Immediate (First Line):
| Investigation | Purpose |
|---|---|
| Chest X-ray (PA view) | Screen for consolidation, cavitation, hilar nodes, miliary pattern, effusion |
| Sputum AFB smear x 2 (morning + spot) | Direct TB diagnosis |
| GeneXpert MTB/RIF (CBNAAT) | Rapid molecular diagnosis + rifampicin resistance (WHO-recommended first test) |
| HIV serology (ELISA/rapid test) | Mandatory in all suspected TB; changes management |
| CBC with differential | Anaemia, lymphopenia (HIV/TB), eosinophilia (parasitic) |
| ESR, CRP | Inflammatory markers |
| LFT, RFT | Baseline before ATT |
| Sputum culture (MGIT/LJ medium) | Gold standard, also gives drug sensitivity |
Second Line (if first line inconclusive):
| Investigation | Purpose |
|---|---|
| HRCT Chest | More sensitive than CXR: 96% vs 48% sensitivity for active TB; better for lymphadenopathy and bronchogenic spread |
| IGRA (QuantiFERON-TB Gold / T-SPOT.TB) | Latent TB in immunocompetent; less useful in HIV |
| Bronchoscopy + BAL | If sputum AFB negative but high suspicion |
| CD4 count + HIV viral load | If HIV positive |
| LDH | Elevated in PCP (Pneumocystis) pneumonia |
| Serum Cryptococcal antigen | If HIV+ with severe immunosuppression |
| Bone marrow biopsy / FNAC nodes | If lymphoma suspected (lymphadenopathy, mediastinal mass) |
Step 6 - Red Flags Warranting Urgent Action
- SpO2 < 94% - consider severe PCP or miliary TB with respiratory failure
- Miliary pattern on CXR - disseminated TB, treat as emergency
- Mediastinal widening - lymphoma or TB adenitis with compression
- Hemoptysis - advanced TB, aspergilloma in old cavity
- Altered sensorium - TB meningitis coexisting
Step 7 - Management Principle (Once TB Confirmed)
The WHO/national guidelines recommend DOTS-based Anti-Tubercular Therapy (ATT):
Intensive phase (2 months): HRZE - Isoniazid + Rifampicin + Pyrazinamide + Ethambutol
Continuation phase (4 months): HR - Isoniazid + Rifampicin
- If HIV co-infected: start ATT first, then ART within 2-8 weeks (CD4-dependent timing)
- Monitor LFT (hepatotoxicity from INH/RIF/PZA)
- Pyridoxine (B6) supplementation with INH to prevent peripheral neuropathy
Summary
This 26-year-old male with 1-month fever, progressive breathlessness, and cough has a high pre-test probability for pulmonary tuberculosis. HIV co-infection must be excluded immediately as it dramatically alters the clinical presentation, radiographic pattern, and management. The workup should be initiated urgently with CXR, sputum GeneXpert, and HIV serology in parallel. Lymphoma remains an important differential if lymphadenopathy or mediastinal widening is found.
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 1186-1188 (TB Diagnosis chapter)
- Bailey and Love's Short Practice of Surgery 28th Ed, p. 6954 (Tuberculosis clinical features)
This is a shared conversation. Sign in to Orris to start your own chat.