Act as professional physiology professor and give me all contents for cardiovascular system take gluton and hall’s physiology book as a reference for a bds 1 year student
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Here is your complete, professor-level cardiovascular physiology guide for BDS 1st year, drawn directly from Guyton and Hall Textbook of Medical Physiology (14th Edition, ISBN 9780443111013).
🫀 CARDIOVASCULAR SYSTEM — Complete Notes for BDS 1st Year
Reference: Guyton and Hall Textbook of Medical Physiology
UNIT 1: OVERVIEW OF THE CARDIOVASCULAR SYSTEM
The cardiovascular system is essentially a transport system. It performs three core functions:
- Circulation of blood - mixes and transports extracellular fluid to all cells
- Nutrient delivery - carries O₂, glucose, amino acids, fatty acids to tissues
- Waste removal - carries CO₂, urea, and other metabolites to lungs, kidneys, and liver
Basic design: The heart is actually two pumps in series:
- Right heart - pumps deoxygenated blood through the pulmonary circulation (lungs)
- Left heart - pumps oxygenated blood through the systemic circulation (rest of body)
Each side consists of an atrium (primer pump) and a ventricle (main pumping chamber). The heart is enclosed by the pericardium - a double-layer protective sac.
(Guyton & Hall, p. 123 — Chapter 9)
UNIT 2: CARDIAC MUSCLE PHYSIOLOGY
2.1 Types of Cardiac Muscle
Three major types exist:
| Type | Function |
|---|---|
| Atrial muscle | Contracts to prime the ventricles |
| Ventricular muscle | Provides main pumping force |
| Specialized excitatory/conductive fibers | Generates and conducts impulses; contracts feebly |
2.2 Cardiac Muscle Anatomy (Histology)
- Fibers arranged in a latticework - divide, recombine, and spread again
- Striated in the same manner as skeletal muscle (contains actin and myosin)
- Connected by intercalated discs containing gap junctions (nexuses)
- Gap junctions allow low electrical resistance - action potentials spread freely from one cell to the next
- This makes the entire atrial and ventricular muscle act as a functional syncytium - when one fiber is excited, all fibers contract
Syncytium concept: The atria form one syncytium; the ventricles form another. These are separated by fibrous tissue except at the AV bundle (Bundle of His).
(Guyton & Hall, p. 123)
2.3 Left Ventricular Torsion (Clinically Important!)
- The LV has complex muscle fiber layers running in different directions
- Subepicardial fibers spiral leftward; subendocardial fibers spiral rightward
- Result: wringing/twisting motion - LV base rotates clockwise, apex rotates counterclockwise (viewed apex to base)
- During diastole, the LV untwists like a loaded spring, rapidly sucking blood in
- This torsion aids both ejection (systole) and filling (diastole)
(Guyton & Hall, p. 123)
UNIT 3: ACTION POTENTIALS IN CARDIAC MUSCLE
3.1 Ventricular Muscle Action Potential
The ventricular action potential has 5 phases and lasts ~250–300 ms:
| Phase | Name | Ion Movement |
|---|---|---|
| Phase 0 | Rapid depolarization | Fast Na⁺ channels open → rapid Na⁺ influx |
| Phase 1 | Brief initial repolarization | Fast Na⁺ channels close; brief K⁺ efflux |
| Phase 2 | Plateau | L-type (slow) Ca²⁺ channels open → Ca²⁺ + Na⁺ influx; K⁺ permeability decreases |
| Phase 3 | Rapid repolarization | L-type Ca²⁺ channels close; K⁺ channels open → K⁺ efflux |
| Phase 4 | Resting potential | Na⁺/K⁺ ATPase restores ion balance; resting potential = -85 to -90 mV |
Key difference from skeletal muscle:
- The plateau phase (Phase 2) is unique to cardiac muscle
- Caused by slow L-type Ca²⁺ channels remaining open for several tenths of a second
- Makes cardiac contraction last 15 times longer than skeletal muscle contraction
- K⁺ permeability decreases 5-fold after onset of AP - this also helps maintain the plateau
Clinical significance: The plateau creates an absolute refractory period lasting almost as long as the contraction. This prevents tetanic contractions in the heart - which would be fatal!
(Guyton & Hall, p. 123)
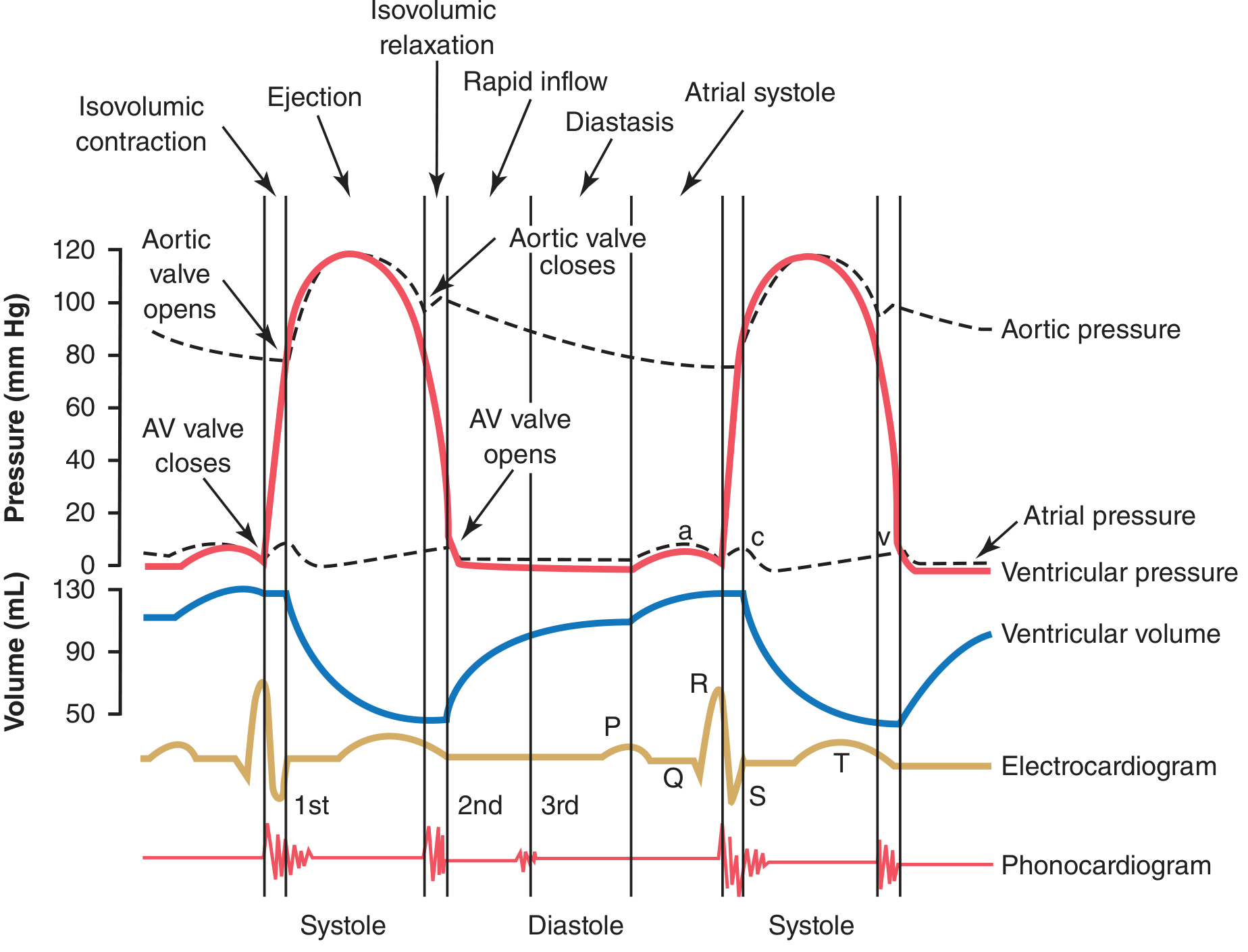
UNIT 4: THE CARDIAC CYCLE
The cardiac cycle includes all events from the beginning of one heartbeat to the beginning of the next. At a normal heart rate of 72 beats/min, each cycle lasts about 0.8 seconds.
4.1 Phases of the Cardiac Cycle (Left Ventricle)
Diastole (Filling phase):
- Isovolumetric relaxation - All valves closed; LV pressure falls; no change in volume
- Rapid filling - Mitral valve opens; ~70-80% of blood flows passively into LV
- Slow filling (diastasis) - Slow continued flow
- Atrial systole (a-wave) - Atrial contraction adds final 20-30% to LV filling
Systole (Ejection phase):
5. Isovolumetric contraction - All valves closed; LV pressure rises rapidly; no volume change
6. Rapid ejection - Aortic valve opens when LV pressure > aortic pressure; blood ejected
7. Slow (reduced) ejection - Flow slows as systole ends
4.2 Pressure Values (Normal)
| Location | Systolic | Diastolic |
|---|---|---|
| Left ventricle | 120 mmHg | ~0-8 mmHg |
| Aorta | 120 mmHg | 80 mmHg |
| Right ventricle | 25 mmHg | ~0-8 mmHg |
| Pulmonary artery | 25 mmHg | 8 mmHg |
4.3 Atrial Pressure Waves (a, c, v waves)
- a wave - caused by atrial contraction (right atrium ~4-6 mmHg; left ~7-8 mmHg)
- c wave - caused by tricuspid and mitral valve bulging backward into the atria at the start of ventricular contraction
- v wave - caused by slow buildup of blood in atria while the AV valves are closed during ventricular contraction
4.4 Heart Valves
- AV valves (mitral, tricuspid) - prevent backflow from ventricles to atria during systole
- Semilunar valves (aortic, pulmonary) - prevent backflow from great arteries to ventricles during diastole
- Valve closure produces heart sounds (S1 and S2)
4.5 Heart Sounds
| Sound | Cause | Timing |
|---|---|---|
| S1 (lub) | Mitral + tricuspid valve closure | Beginning of systole |
| S2 (dub) | Aortic + pulmonary valve closure | End of systole / beginning of diastole |
| S3 | Rapid ventricular filling (pathological in adults) | Early diastole |
| S4 | Atrial contraction against stiff ventricle | Late diastole (pre-systolic) |
(Guyton & Hall, p. 127)
UNIT 5: WORK OUTPUT OF THE HEART
5.1 Definitions
- Stroke volume (SV) - amount of blood ejected per beat (~70 mL at rest)
- Cardiac output (CO) - CO = Heart Rate × Stroke Volume = 72 × 70 = ~5 L/min
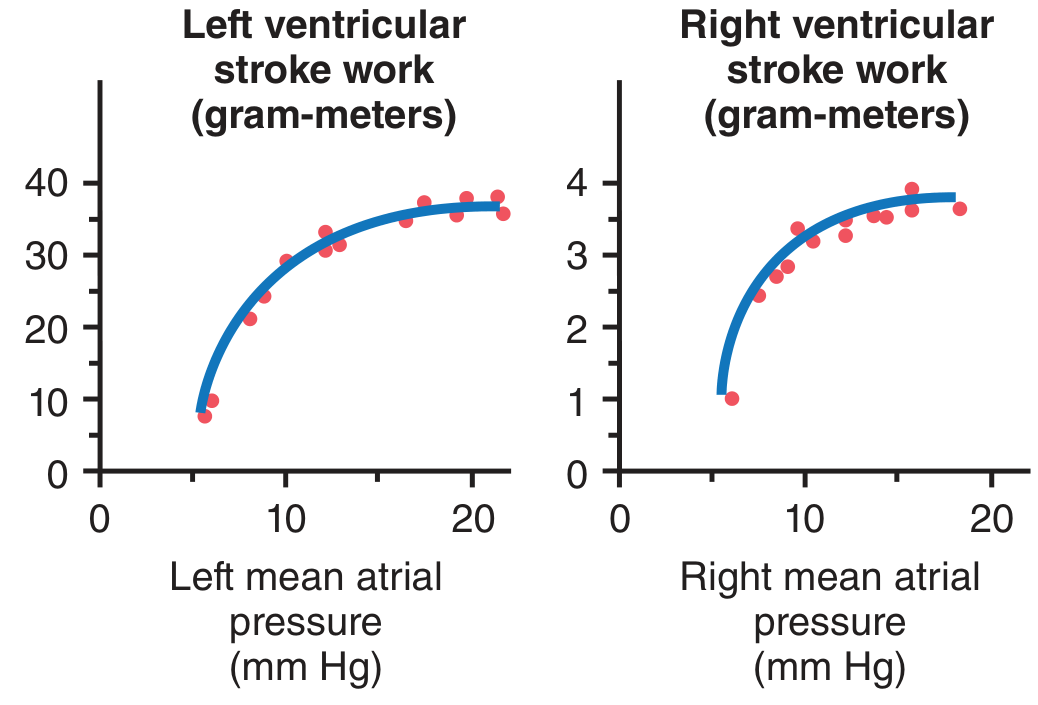
5.2 Stroke Work
- Stroke work output = Stroke volume × Mean arterial pressure
- The left ventricle does ~6 times more work per beat than the right ventricle (because systemic BP >> pulmonary BP)
5.3 Ventricular Volume-Pressure Diagram
- End-diastolic volume (EDV) - volume at end of filling: ~110-120 mL
- End-systolic volume (ESV) - volume remaining after ejection: ~40-50 mL
- Ejection fraction (EF) = SV/EDV = 70/120 = ~58% (normal >55%)
(Guyton & Hall, p. 128-131)
UNIT 6: REGULATION OF HEART PUMPING
6.1 Intrinsic Regulation - Frank-Starling Law
"The heart pumps all the blood that comes to it."
Mechanism:
- More venous return → more stretch of ventricular muscle fibers → actin and myosin filaments reach more optimal overlap → greater force of contraction → more blood ejected
Physiological significance:
- Balances output of left and right ventricles
- Automatically adjusts cardiac output to match venous return
- Prevents blood pooling in lungs or systemic circulation
Ventricular Function Curves show stroke work output vs. mean atrial pressure - the curve shifts upward with sympathetic stimulation, downward in heart failure.
(Guyton & Hall, p. 132)
6.2 Extrinsic (Nervous) Regulation
| Nerve | Receptor | Effect on Heart Rate | Effect on Contractility |
|---|---|---|---|
| Sympathetic | β₁-adrenergic | ↑ (positive chronotropy) | ↑ (positive inotropy) |
| Parasympathetic (vagus) | Muscarinic (M₂) | ↓ (negative chronotropy) | ↓ (mainly atria) |
Sympathetic effects:
- Releases norepinephrine at cardiac nerve endings
- Increases permeability of fiber membranes to Na⁺ and Ca²⁺ → stronger, faster contraction
- Can increase cardiac output to 2.5× normal (25-30 L/min during exercise)
Parasympathetic effects:
- Releases acetylcholine
- Increases K⁺ permeability → hyperpolarization → slows SA node discharge → decreases heart rate
- Strong vagal stimulation can stop the heart momentarily
6.3 Effect of Ions on Heart Function
| Ion | Effect |
|---|---|
| ↑ K⁺ (hyperkalemia) | Dilated, flaccid heart; decreased rate and contractility; can cause death |
| ↓ K⁺ (hypokalemia) | Increased irritability (arrhythmias) |
| ↑ Ca²⁺ (hypercalcemia) | Spastic, powerful contraction ("calcium rigor") |
| ↓ Ca²⁺ (hypocalcemia) | Decreased contractility; can cause tetany |
6.4 Effect of Temperature
- ↑ Temperature → ↑ Heart rate (fever increases rate significantly)
- ↓ Temperature → ↓ Heart rate; used in cardiac surgery (hypothermia)
(Guyton & Hall, p. 137-141)
UNIT 7: RHYTHMICAL EXCITATION OF THE HEART (Conduction System)
7.1 Components of the Conduction System
SA Node → Internodal pathways → AV Node → Bundle of His →
Left + Right Bundle Branches → Purkinje Fibers → Ventricular myocardium
| Structure | Location | Inherent Rate |
|---|---|---|
| SA Node (Sinoatrial) | Superior posterolateral wall of right atrium (below SVC opening) | 60-100 bpm (actual pacemaker) |
| AV Node | Posterior-inferior right atrium near tricuspid valve | 40-60 bpm |
| Bundle of His | Upper ventricular septum | 40-60 bpm |
| Purkinje fibers | Inner ventricular walls | 15-40 bpm |
"The SA node fires first because it has the fastest inherent rate - it suppresses all lower pacemakers by depolarizing them before they can self-fire."
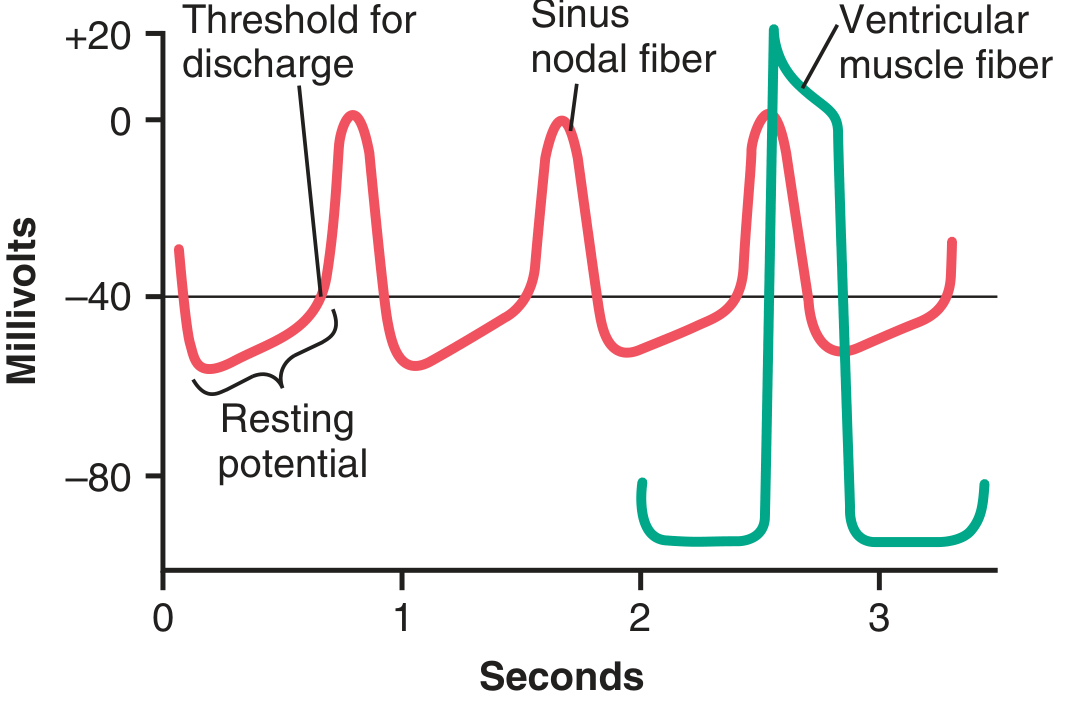
7.2 SA Node: Self-Excitation (Automaticity)
The SA node fires automatically because:
- Resting membrane potential is only -55 to -60 mV (less negative than ventricular muscle at -85 mV)
- The membrane is naturally leaky to Na⁺ and Ca²⁺ - these positive ions slowly depolarize the cell
- This spontaneous depolarization is called the pacemaker potential or prepotential
Funny current (If): Sodium channels that open at negative potentials, allowing Na⁺ influx during diastole, driving the membrane toward threshold - key to automaticity.
When the threshold potential (approximately -40 mV) is reached, L-type Ca²⁺ channels open and generate the upstroke of the action potential.
7.3 AV Node - The Gatekeeper
Critical function: Delay of 0.09 seconds before impulse passes to the ventricles.
Why is the delay important?
- Allows atria to complete contraction and empty blood into the ventricles before the ventricles contract
- Without this delay, atria and ventricles would contract simultaneously - reducing cardiac output
AV Block: If the AV node is damaged, the ventricles may beat at their own slow rate (40-60 bpm) independent of atrial rhythm = complete heart block.
7.4 Purkinje System
- Extremely large diameter fibers → very rapid conduction (1.5-4 m/s vs. 0.3-0.5 m/s in ventricular muscle)
- Distributes impulse to all parts of ventricles almost simultaneously
- Ensures synchronized contraction for maximum pumping efficiency
- Conduct the impulse from the endocardium toward the epicardium
7.5 Conduction Velocities
| Pathway | Conduction Velocity |
|---|---|
| SA node | Very slow (0.05 m/s) |
| Atrial muscle | 1.0 m/s |
| AV node | 0.02-0.05 m/s (slowest - creates delay) |
| Bundle of His | 1.0 m/s |
| Purkinje fibers | 1.5-4.0 m/s (fastest) |
| Ventricular muscle | 0.3-0.5 m/s |
(Guyton & Hall, p. 145-152)
UNIT 8: CARDIAC OUTPUT, VENOUS RETURN & THEIR REGULATION
8.1 Normal Values
| Parameter | Normal Value |
|---|---|
| Cardiac output (CO) | ~5 L/min (men), ~4.9 L/min (women) |
| Cardiac index | ~3.0 L/min/m² body surface area |
| Heart rate | 72 bpm |
| Stroke volume | ~70 mL |
8.2 Venous Return
- Venous return = amount of blood returning to the right atrium per minute
- Under steady-state conditions: Cardiac output = Venous return (they must be equal)
- The heart pumps whatever blood comes to it (Frank-Starling mechanism ensures this)
8.3 Factors Controlling Cardiac Output
1. Tissue metabolism (most important):
- Active tissues release O₂, CO₂, lactic acid, adenosine - these cause local vasodilation
- ↑ metabolism → ↑ local blood flow → ↑ venous return → ↑ cardiac output
2. Sympathetic stimulation:
- Increases heart rate and contractility
- Can raise CO to 25-30 L/min during vigorous exercise in athletes
3. Total peripheral resistance (afterload):
- Up to moderate levels, increasing arterial pressure does NOT decrease cardiac output (Frank-Starling compensates)
- Severe hypertension can decrease CO
8.4 Hypereffective vs. Hypoeffective Heart
Hypereffective (↑ CO):
- Sympathetic stimulation
- Hypertrophy from athletic training
- Low afterload
Hypoeffective (↓ CO) - causes of heart failure:
- Myocardial infarction
- Severe valvular disease
- Myocarditis
- Vitamin B₁ deficiency (beriberi)
(Guyton & Hall, p. 230-250)
UNIT 9: ELECTROCARDIOGRAPHY (ECG/EKG)
9.1 Basic Concept
The ECG records electrical potentials generated by the depolarizing and repolarizing heart muscle, detected from the body surface.
9.2 Normal ECG Waveforms
| Wave/Interval | What It Represents | Normal Duration |
|---|---|---|
| P wave | Atrial depolarization (SA node → atrial muscle) | < 0.12 s |
| PR interval | From atrial depolarization to ventricular depolarization (includes AV delay) | 0.12-0.20 s |
| QRS complex | Ventricular depolarization | 0.06-0.10 s |
| ST segment | Period of ventricular plateau (all cells depolarized equally) | isoelectric |
| T wave | Ventricular repolarization | - |
| QT interval | Total duration of ventricular electrical activity | 0.35-0.44 s |
Note: There is no separate wave for atrial repolarization because it is masked by the large QRS complex.
9.3 ECG and Cardiac Cycle Correlation
- P wave → atrial depolarization → atrial contraction begins
- QRS complex (0.16 s after P wave onset) → ventricular depolarization → ventricular systole begins
- T wave → ventricular repolarization → ventricular muscle begins to relax
(Guyton & Hall, p. 127)
UNIT 10: BLOOD PRESSURE & ITS REGULATION
10.1 Normal Blood Pressure Values
- Normal systemic BP: 120/80 mmHg (systolic/diastolic)
- Mean arterial pressure (MAP) = Diastolic + 1/3 pulse pressure = 93 mmHg
- Pulse pressure = Systolic - Diastolic = 40 mmHg
- Normal pulmonary artery pressure: 25/8 mmHg
10.2 Factors Determining Blood Pressure
MAP = Cardiac Output × Total Peripheral Resistance (TPR)
Any factor that raises CO or TPR raises blood pressure.
10.3 Short-Term BP Regulation (Seconds to Minutes)
Baroreceptor Reflex (most important):
- Baroreceptors located in carotid sinus and aortic arch
- They detect stretch/pressure changes
- ↑ BP → baroreceptors fire more → inhibit vasomotor center → ↓ sympathetic, ↑ parasympathetic → ↓ HR and vasodilation → BP normalizes
- Acts within seconds - very effective against sudden BP changes
Chemoreceptors:
- Located in carotid and aortic bodies
- Detect ↓ O₂, ↑ CO₂, ↑ H⁺ in blood
- When activated: ↑ ventilation + ↑ sympathetic outflow → ↑ BP
10.4 Long-Term BP Regulation
Renin-Angiotensin-Aldosterone System (RAAS) - most powerful long-term system:
Low BP / Low Na⁺ / Low renal blood flow
↓
Kidney releases RENIN
↓
Renin cleaves angiotensinogen → Angiotensin I
↓
ACE (in lungs) converts → Angiotensin II
↓
1. Vasoconstriction (↑ TPR)
2. ↑ Aldosterone release from adrenal cortex → Na⁺ and water retention → ↑ blood volume → ↑ CO
3. ↑ ADH (vasopressin) → water retention
Result: Blood pressure rises back to normal over hours to days.
(Guyton & Hall, Block 3, p. ~18-130)
UNIT 11: MICROCIRCULATION & CAPILLARY DYNAMICS
11.1 Structure of the Microcirculation
Arteriole → Metarteriole → Precapillary sphincter → Capillary → Venule
- Arterioles are the major resistance vessels (control blood flow to tissues)
- Precapillary sphincters open and close intermittently (vasomotion) based on local O₂ needs
11.2 Capillary Exchange - Starling Forces
Fluid movement across the capillary wall depends on 4 forces:
| Force | Direction of Fluid Movement | Normal Value |
|---|---|---|
| Capillary hydrostatic pressure (Pc) | Out of capillary (filtration) | ~25 mmHg (venous end) to 35 mmHg (arterial end) |
| Interstitial fluid hydrostatic pressure (Pif) | Into capillary (absorption) | -3 mmHg |
| Plasma colloid osmotic pressure (πc) | Into capillary (absorption) | ~28 mmHg |
| Interstitial colloid osmotic pressure (πif) | Out of capillary (filtration) | ~8 mmHg |
Net Filtration Pressure (NFP) = (Pc + πif) - (πc + Pif)
- At arterial end: net filtration outward → fluid leaves capillary
- At venous end: net absorption inward → fluid re-enters capillary
- Roughly 90% of filtered fluid is reabsorbed; remaining 10% returns via lymphatics
11.3 Edema
- Occurs when fluid filtration exceeds lymphatic drainage
- Causes: ↑ capillary pressure (heart failure), ↓ plasma proteins (hypoalbuminemia), lymphatic obstruction, ↑ capillary permeability
UNIT 12: CARDIAC OUTPUT IN SPECIAL STATES
12.1 Exercise
- CO can rise to 20-25 L/min (trained athletes up to 35 L/min)
- Mechanism: sympathetic stimulation + ↑ venous return (muscle pump + respiratory pump)
12.2 Pregnancy
- Maternal blood volume ↑ by ~30-40%
- CO increases to support fetoplacental unit
12.3 Fetal Circulation
- Blood bypasses the lungs via:
- Foramen ovale (right atrium → left atrium)
- Ductus arteriosus (pulmonary artery → aorta)
- Ductus venosus (umbilical vein → inferior vena cava, bypasses liver)
- At birth: foramen ovale closes (first breath → ↑ left atrial pressure), ductus arteriosus closes (↑ O₂)
QUICK SUMMARY TABLE: Key Numbers to Remember (BDS Exams)
| Parameter | Value |
|---|---|
| Resting cardiac output | ~5 L/min |
| Stroke volume | ~70 mL |
| Heart rate | 72 bpm |
| Ejection fraction | ~58% |
| Systolic BP (aorta) | 120 mmHg |
| Diastolic BP (aorta) | 80 mmHg |
| Mean arterial pressure | ~93 mmHg |
| Pulmonary artery pressure | 25/8 mmHg |
| SA node inherent rate | 60-100 bpm |
| AV node inherent rate | 40-60 bpm |
| Purkinje fiber rate | 15-40 bpm |
| AV nodal delay | 0.09 s |
| Cardiac cycle duration | 0.8 s |
| Action potential plateau duration | ~0.2 s |
| Resting membrane potential (ventricle) | -85 to -90 mV |
| Plasma colloid osmotic pressure | ~28 mmHg |
| Cardiac index | ~3.0 L/min/m² |
IMPORTANT EXAM TOPICS FOR BDS 1ST YEAR
Based on the standard BDS syllabus, the most frequently asked topics from this unit are:
- Frank-Starling law of the heart - mechanism and significance
- Cardiac cycle - phases, pressure changes, heart sounds
- Properties of cardiac muscle - automaticity, conductivity, contractility, rhythmicity, excitability
- Conduction system of the heart - SA node, AV node, Bundle of His, Purkinje fibers
- Differences between cardiac and skeletal muscle (action potentials, refractory period)
- Regulation of blood pressure - baroreceptor reflex, RAAS
- ECG - waves and their significance
- Cardiac output - normal values, methods of measurement (Fick's principle, thermodilution)
- Starling's law of capillaries - capillary dynamics and edema
All content referenced from: Guyton and Hall Textbook of Medical Physiology, 14th Edition (Guyton AC, Hall JE) — ISBN 9780443111013, available in your library at blocks 1-3 covering Chapters 9, 10, 11, 18, 20, and related chapters.
Now give complete detailed notes with diagrams and flowcharts for each unit from (1 to 12 )acc to the content you provided
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
🫀 CARDIOVASCULAR SYSTEM — Complete Detailed Notes with Diagrams
BDS 1st Year | Reference: Guyton & Hall Textbook of Medical Physiology, 14th Ed.
UNIT 1: OVERVIEW OF THE CARDIOVASCULAR SYSTEM
1.1 Basic Organization
FLOWCHART 1 — Blood Flow Through the Heart
┌─────────────────────────────────────────────────────────────────────┐
│ SYSTEMIC CIRCULATION │
│ (Body tissues: head, trunk, limbs) │
└──────────────────┬──────────────────────────┬───────────────────────┘
│ Deoxygenated blood │ Oxygenated blood
│ via Venae Cavae │ via Aorta
▼ ▲
┌──────────────┐ ┌──────────────────┐
│ RIGHT ATRIUM │ │ LEFT VENTRICLE │
│ (Primer pump)│ │ (Main systemic │
└──────┬───────┘ │ pump) │
│ Tricuspid valve └────────┬─────────┘
▼ │ Mitral valve
┌──────────────┐ ┌────────┴─────────┐
│RIGHT VENTRICLE│ │ LEFT ATRIUM │
│(Pulm. pump) │ │ (Primer pump) │
└──────┬────────┘ └────────┬─────────┘
│ Pulmonary valve │ Pulmonary veins
│ via Pulmonary artery │ (Oxygenated)
▼ ▲
┌───────────────────────────────────┐
│ PULMONARY CIRCULATION │
│ (LUNGS) │
│ Gas exchange occurs here │
└───────────────────────────────────┘
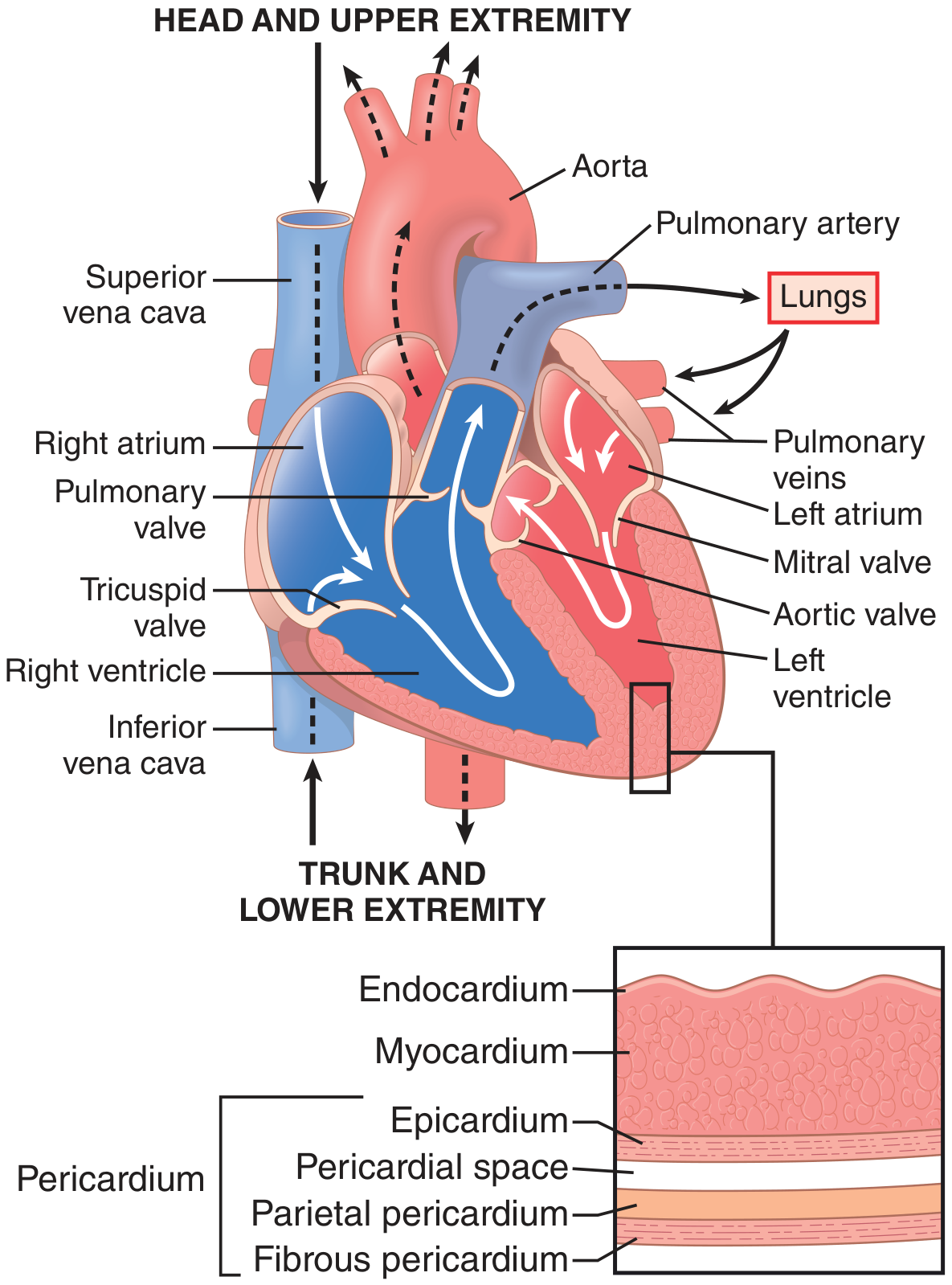
DIAGRAM — Structure of the Heart (from Guyton & Hall, Fig. 9.1)
1.2 Layers of the Heart Wall
OUTERMOST → Fibrous Pericardium (tough protective outer layer)
↓
Parietal Pericardium (lines the pericardial sac)
↓
Pericardial Space (10–20 mL of lubricating fluid)
↓
Visceral Pericardium = Epicardium (covers the heart)
↓
Myocardium (cardiac muscle — the actual pump)
↓
INNERMOST → Endocardium (smooth inner lining of chambers)
1.3 Functions of the Cardiovascular System
| Function | Detail |
|---|---|
| Transport | O₂, nutrients, hormones to every cell |
| Waste removal | CO₂ → lungs; urea, creatinine → kidneys |
| Temperature regulation | Skin vessels dilate/constrict to lose/conserve heat |
| Immune defense | White cells and antibodies circulate via blood |
| Homeostasis | Maintains stable extracellular fluid composition |
UNIT 2: CARDIAC MUSCLE PHYSIOLOGY
2.1 Types of Cardiac Muscle
CARDIAC MUSCLE
│
├──► Atrial muscle → contracts to fill ventricles
├──► Ventricular muscle → main pumping force
└──► Specialized fibers → generates & conducts impulses
(SA node, AV node, Bundle of His, Purkinje)
2.2 Histology of Cardiac Muscle
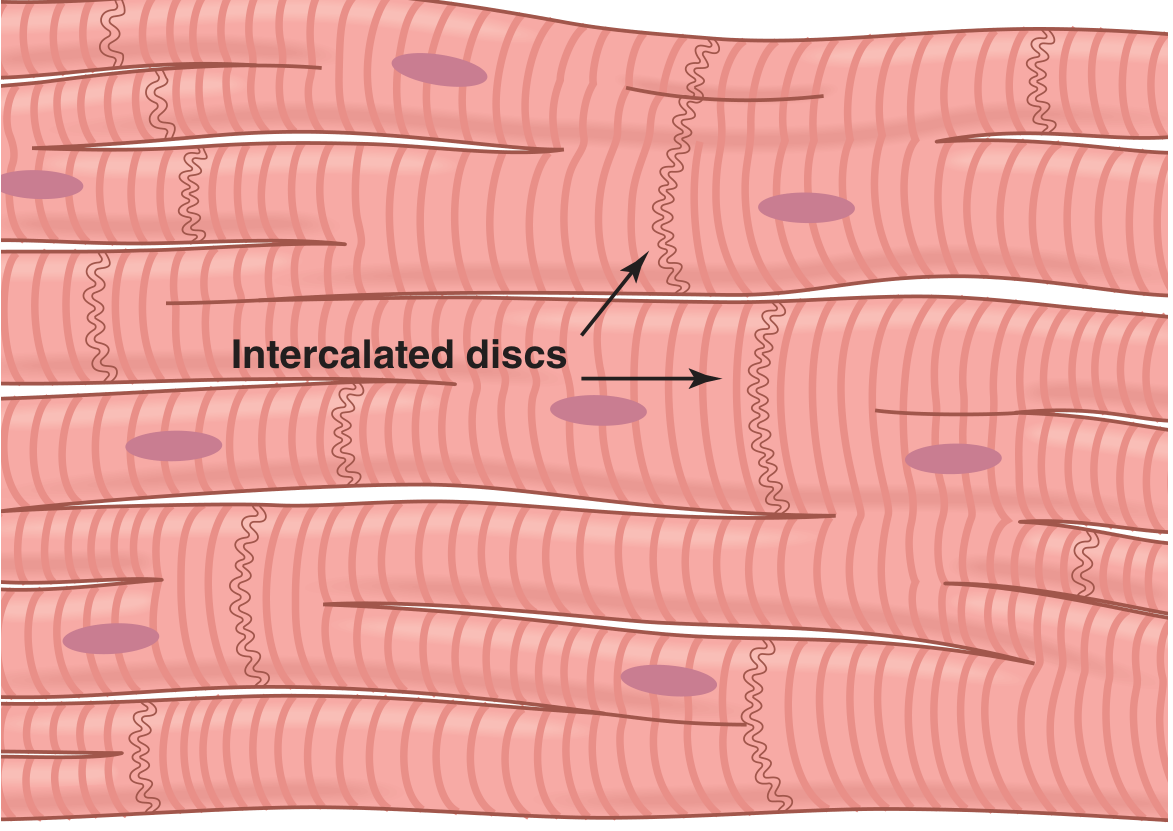
DIAGRAM — Syncytial Nature of Cardiac Muscle Fibers (Guyton & Hall, Fig. 9.2)
Key structural features:
- Fibers arranged in a latticework (divide, recombine, spread)
- Striated - actin and myosin filaments just like skeletal muscle
- Intercalated discs - connect cells end-to-end
- Gap junctions (nexuses) within intercalated discs - low electrical resistance - ions flow freely
- Desmosome junctions - mechanical attachment preventing cells from pulling apart
2.3 Cardiac Syncytium - Most Important Concept
┌─────────────────────────────────────────────────────────┐
│ THE SYNCYTIUM CONCEPT │
│ │
│ Cell 1 ──[Gap junction]── Cell 2 ──[Gap junction]──... │
│ │
│ Action potential spreads from cell 1 to ALL cells │
│ │
│ "All or nothing" law applies to the ENTIRE HEART │
│ │
│ Two separate syncytia exist: │
│ • Atrial syncytium (fires first) │
│ • Ventricular syncytium (fires second, 0.1–0.2 s later)│
│ │
│ Separated by fibrous tissue EXCEPT at AV bundle │
└─────────────────────────────────────────────────────────┘
2.4 Cardiac vs. Skeletal Muscle — Comparison Table
| Feature | Cardiac Muscle | Skeletal Muscle |
|---|---|---|
| Striations | Present | Present |
| Nucleus | Single, central | Multiple, peripheral |
| Intercalated discs | Present (unique) | Absent |
| Syncytium | Yes (functional) | No |
| Control | Involuntary (autonomic) | Voluntary |
| Action potential duration | ~250-300 ms | 1-2 ms |
| Plateau phase | Present (Ca²⁺ channels) | Absent |
| Refractory period | Very long (~250 ms) | Short |
| Tetanus possible? | NO (due to long ARP) | Yes |
| Ca²⁺ source | Extracellular + sarcoplasmic reticulum | Mainly sarcoplasmic reticulum |
| Self-excitation | Yes (SA node) | No (needs neural input) |
2.5 Left Ventricular Torsion
SYSTOLE (Contraction):
Subepicardial fibers → apex rotates COUNTERCLOCKWISE
Subendocardial fibers → base rotates CLOCKWISE
NET EFFECT: Wringing/twisting motion → like squeezing a wet towel
DIASTOLE (Relaxation):
LV "untwists like a loaded spring"
Creates suction → rapid blood inflow
Helps BOTH ejection AND filling
UNIT 3: ACTION POTENTIALS IN CARDIAC MUSCLE
3.1 Ventricular Muscle Action Potential — Phases
DIAGRAM — Action Potential with Ionic Currents (Guyton & Hall, Fig. 9.5)
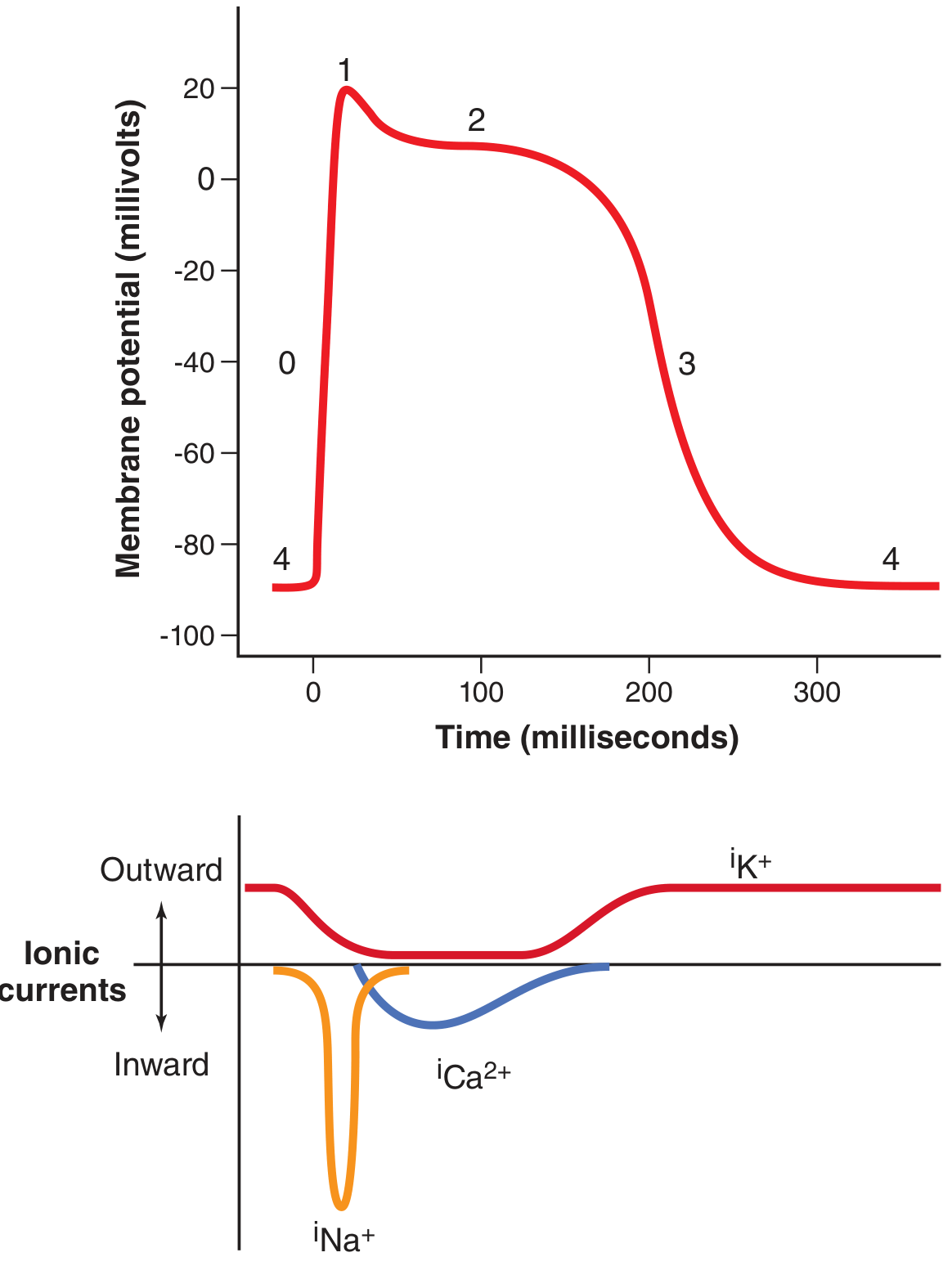
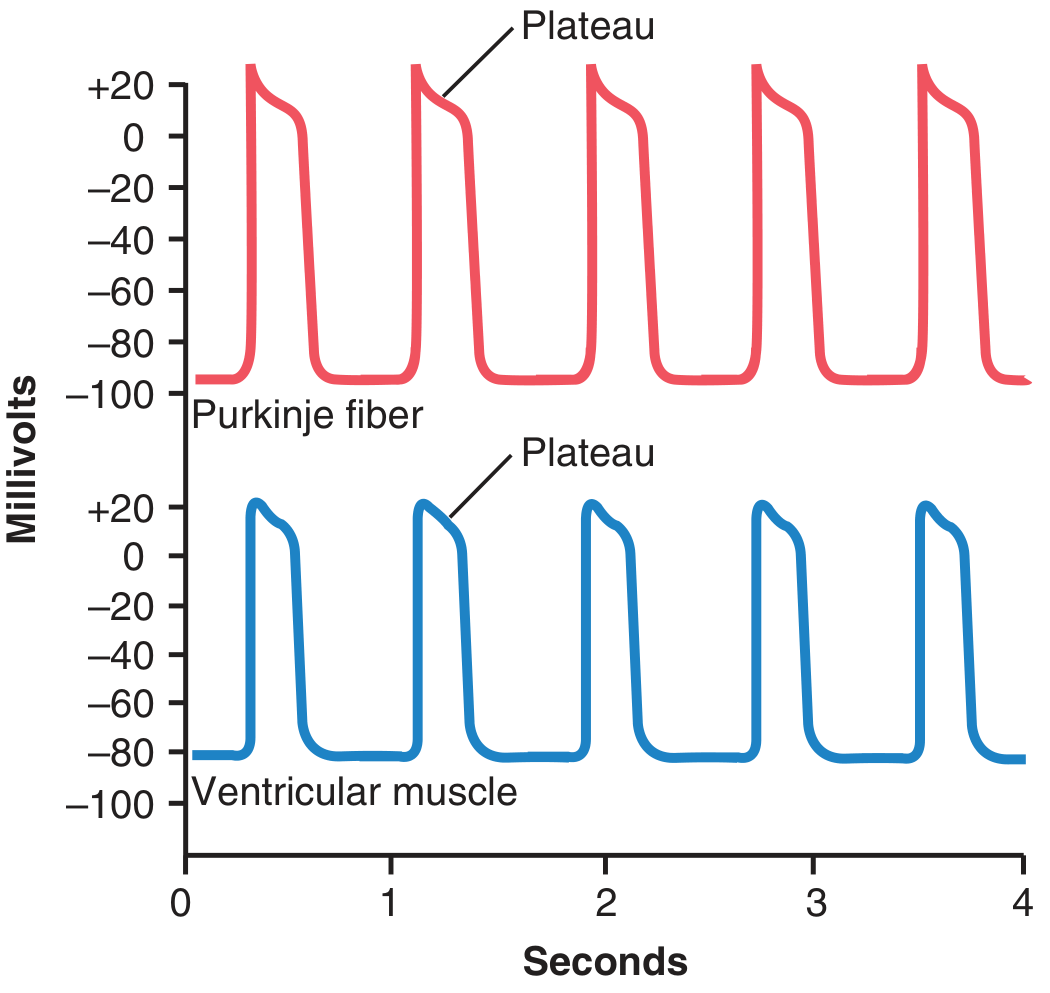
DIAGRAM — Rhythmical APs in Purkinje fiber vs. Ventricular muscle (Guyton & Hall, Fig. 9.4)
3.2 The 5 Phases Explained
mV
+20 ─── ___________ ← PHASE 2: PLATEAU
| | L-type Ca²⁺ channels open
| | Na⁺ inflow maintains + potential
0 ─ | | K⁺ permeability ↓ 5-fold
| Phase 1 |
-20 ─ | |
| | Phase 3 ← PHASE 3: RAPID REPOLARIZATION
-40 ─ | |_____ K⁺ channels open → K⁺ efflux
| Ca²⁺ channels close
-60 ─ |
|
-80 ─ Phase 4 Phase 0 | Phase 4
(resting)(upstroke) (resting)
-90 ───────────────────────────────────► Time (300 ms total)
| Phase | Name | Ion Channel | Movement |
|---|---|---|---|
| 0 | Rapid depolarization | Fast Na⁺ channels open | Na⁺ rushes IN (inward current) |
| 1 | Initial repolarization | Fast Na⁺ channels close; transient K⁺ | Brief K⁺ efflux |
| 2 | Plateau | L-type Ca²⁺ channels open | Ca²⁺ + Na⁺ IN; K⁺ permeability ↓ |
| 3 | Rapid repolarization | K⁺ channels open; Ca²⁺ channels close | K⁺ OUT |
| 4 | Resting potential | Na⁺/K⁺ ATPase active | Resting: -85 to -90 mV |
3.3 Why the Plateau is Clinically Crucial
FLOWCHART — Why Cardiac Tetanus is Impossible
Long plateau phase (Phase 2 lasts ~200 ms)
↓
Absolute Refractory Period (ARP) = ~250 ms
↓
Heart CANNOT respond to a second stimulus
during the entire duration of contraction
↓
Tetanic (sustained) contraction is IMPOSSIBLE
↓
LIFE-SAVING: Prevents the heart from being
"frozen" in contraction (which would be fatal)
Exam Tip: Cardiac muscle cannot tetanize because the ARP lasts almost as long as the mechanical contraction. This is a major difference from skeletal muscle.
3.4 SA Node Action Potential - Different from Ventricular!
SA Node Action Potential:
+20 ─ /\ Threshold ~-40 mV
/ \ Slow Ca²⁺ channels cause upstroke
0 ─ / \ (NOT fast Na⁺ channels!)
/ \
-20 ─ / \
↑ ↓
-40 ─ Threshold ─ ─ ─ ─ ─ ─
↑
-55 ─ Pacemaker potential (slow)
(If channels: "funny" Na⁺ leak in)
-60 ─_________
Resting potential after hyperpolarization
UNIT 4: THE CARDIAC CYCLE
4.1 The Master Diagram (Memorize This!)
DIAGRAM — Wiggers Diagram (Guyton & Hall, Fig. 9.8)
4.2 Phases of the Cardiac Cycle (0.8 seconds total at 72 bpm)
FLOWCHART — Complete Cardiac Cycle
START
│
▼
┌─────────────────────────────────────────────────────────┐
│ DIASTOLE (0.5 s) │
│ │
│ 1. ISOVOLUMETRIC RELAXATION (0.04 s) │
│ • Aortic + pulmonary valves just closed │
│ • All 4 valves CLOSED │
│ • LV pressure falls rapidly (120 → ~0 mmHg) │
│ • Volume unchanged (ESV ~50 mL) │
│ │
│ 2. RAPID VENTRICULAR FILLING (0.11 s) │
│ • LV pressure < atrial pressure │
│ • Mitral valve OPENS │
│ • 70-80% of ventricular filling occurs here │
│ • Blood flows passively (no atrial contraction) │
│ │
│ 3. DIASTASIS (0.19 s) │
│ • Slow continued filling │
│ • Pressure equilibrates between atrium & ventricle │
│ │
│ 4. ATRIAL SYSTOLE (0.11 s) │
│ • P wave on ECG triggers atrial contraction │
│ • "Booster pump" - adds final 20-30% to LV filling │
│ • EDV reaches ~120-130 mL │
└─────────────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ SYSTOLE (0.3 s) │
│ │
│ 5. ISOVOLUMETRIC CONTRACTION (0.05 s) │
│ • QRS complex → ventricular depolarization │
│ • All 4 valves CLOSED │
│ • LV pressure rises rapidly (0 → 80 mmHg) │
│ • Volume unchanged (EDV ~120 mL) │
│ • S1 heart sound (mitral + tricuspid close) │
│ │
│ 6. RAPID EJECTION (0.12 s) │
│ • LV pressure > aortic pressure (>80 mmHg) │
│ • Aortic valve OPENS │
│ • 70% of SV ejected here │
│ • LV pressure peaks at 120 mmHg │
│ │
│ 7. REDUCED (SLOW) EJECTION (0.13 s) │
│ • Blood flow slows; LV starts to relax │
│ • Remaining 30% of SV ejected │
│ • S2 heart sound (aortic + pulmonary valve close) │
│ • ESV remains ~50 mL │
└─────────────────────────────────────────────────────────┘
│
▼
CYCLE REPEATS (next beat begins with isovolumetric relaxation)
4.3 Atrial Pressure Waves
ATRIAL PRESSURE CURVE (as seen on Wiggers diagram):
a c v
/\ /\ /\
──────/ \──────/ \──/ \────
a wave = Atrial contraction (LA: 7-8 mmHg; RA: 4-6 mmHg)
c wave = AV valve bulging back into atrium during isovolumetric contraction
v wave = Venous filling of atrium while AV valve is closed (during ventricular systole)
4.4 Heart Sounds
HEART SOUNDS:
SYSTOLE DIASTOLE
───────────────────────────────────────
S1 (lub) S2 (dub)
│ │
Mitral + Tricuspid Aortic + Pulmonary
valves CLOSE valves CLOSE
(Start of systole) (End of systole)
Extra sounds (abnormal in adults):
S3 = Rapid ventricular filling → Heart failure
S4 = Atrial contraction against stiff LV → Hypertension, LVH
4.5 Key Pressure Values Table
| Chamber/Vessel | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Left ventricle | 120 | 0-8 |
| Aorta | 120 | 80 |
| Left atrium | 8 (v wave) | 1-4 |
| Right ventricle | 25 | 0-8 |
| Pulmonary artery | 25 | 8 |
| Right atrium | 6 (a wave) | 0-2 |
UNIT 5: WORK OUTPUT OF THE HEART
5.1 Key Formulas and Definitions
STROKE VOLUME (SV) = EDV - ESV = 120 - 50 = ~70 mL per beat
CARDIAC OUTPUT (CO) = HR × SV = 72 × 70 = ~5040 mL/min ≈ 5 L/min
EJECTION FRACTION (EF) = SV/EDV × 100 = 70/120 × 100 = 58%
(Normal EF > 55%; EF <40% = Heart failure)
STROKE WORK = SV × Mean Arterial Pressure
Left ventricle: 70 mL × 100 mmHg ≈ 0.90 joules
Right ventricle: 70 mL × 14 mmHg ≈ 0.13 joules
(LV does ~6× more work than RV)
CARDIAC INDEX = CO / Body Surface Area = 5 L/min ÷ 1.7 m² ≈ 3 L/min/m²
5.2 Volume-Pressure Loop (Ventricular)
LV Pressure (mmHg)
120 │ D_____C
│ / \
80 │ / \ ← Aortic valve opens at C
│ / \
│ / \
0 │─────────A B
└────────────────────────────
40 70 120 LV Volume (mL)
(ESV) (EDV)
A → B = Diastolic filling (mitral valve open, pressure low)
B → C = Isovolumetric contraction (all valves closed, pressure rises)
C → D = Ejection (aortic valve open, volume decreases)
D → A = Isovolumetric relaxation (all valves closed, pressure falls)
Area inside loop = STROKE WORK of the ventricle
5.3 Oxygen Consumption of the Heart
- Heart extracts ~70-80% of available O₂ from coronary blood (vs. ~25% for other organs)
- This is why coronary blood flow must increase to meet increased demand
- During exercise: coronary flow increases 4-5 fold
- Primary energy substrate: Free fatty acids (60-70%), then glucose
UNIT 6: REGULATION OF HEART PUMPING
6.1 Frank-Starling Law (Intrinsic Regulation)
DIAGRAM — Ventricular Function Curves (Guyton & Hall, Fig. 9.12)
FLOWCHART — Frank-Starling Mechanism
INCREASED VENOUS RETURN
↓
More blood fills the ventricle during diastole
↓
↑ End-Diastolic Volume (EDV) → ↑ stretch of cardiac muscle fibers
↓
Actin & myosin filaments reach MORE OPTIMAL OVERLAP
↓
↑ Force of contraction (more cross-bridges formed)
↓
↑ Stroke Volume → ↑ Cardiac Output
↓
Heart automatically pumps exactly what it receives
(Venous return = Cardiac output)
Three mechanisms of Frank-Starling:
- Optimal actin-myosin overlap (length-tension relationship)
- Increased end-diastolic stretch activates more troponin-Ca²⁺ binding sites
- Bainbridge reflex: RA stretch → ↑ HR by 10-20% (minor contribution)
6.2 Nervous (Extrinsic) Regulation
FLOWCHART — Autonomic Control of the Heart
SYMPATHETIC STIMULATION PARASYMPATHETIC (VAGUS) STIMULATION
(Norepinephrine + Epinephrine) (Acetylcholine)
│ │
▼ ▼
β₁ receptors on heart M₂ receptors on heart
│ │
┌───────┴──────────┐ ┌─────────────┴──────────┐
│ │ │ │
▼ ▼ ▼ ▼
↑ Heart Rate ↑ Contractility ↓ Heart Rate ↓ Contractility
(Chronotropy) (Inotropy) (Chronotropy) (mainly atria)
│ │ │
▼ ▼ ▼
Can reach CO up to Strong vagal
~180 bpm 25-30 L/min → heart stops briefly
during exercise (then escapes)
6.3 Ionic Effects on the Heart
ION IMBALANCE → CARDIAC EFFECT:
K⁺ ↑ (Hyperkalemia) K⁺ ↓ (Hypokalemia)
"High K makes the heart SLOW" "Low K makes it IRRITABLE"
↓ resting potential (less negative) Hyperpolarization
↓ heart rate, ↓ contractility Arrhythmias
Dilated, flaccid heart Ectopic beats
Can cause cardiac arrest Ventricular fibrillation
│ │
└─────────────► BOTH DANGEROUS ◄────────┘
Ca²⁺ ↑ (Hypercalcemia) Ca²⁺ ↓ (Hypocalcemia)
Spastic powerful contraction Decreased contractility
"Calcium rigor" (tetanic-like) Prolonged QT interval
Eventually cardiac arrest Cardiac weakness
in systole
6.4 Temperature Effects
TEMPERATURE:
↑ Temperature (fever):
→ ↑ metabolic rate of cardiac cells
→ ↑ Heart rate
→ 1°C rise = ~10 bpm increase
→ 42°C (107.6°F) → heart failure
↓ Temperature (hypothermia):
→ ↓ Heart rate dramatically
→ Used in cardiac surgery to
PROTECT the heart (reduces O₂ demand)
→ 20°C → heart rate may fall to 20-30 bpm
UNIT 7: RHYTHMICAL EXCITATION OF THE HEART (Conduction System)
7.1 The Conduction System Diagram
DIAGRAM — Conduction System of the Heart (Guyton & Hall, Fig. 10.1)
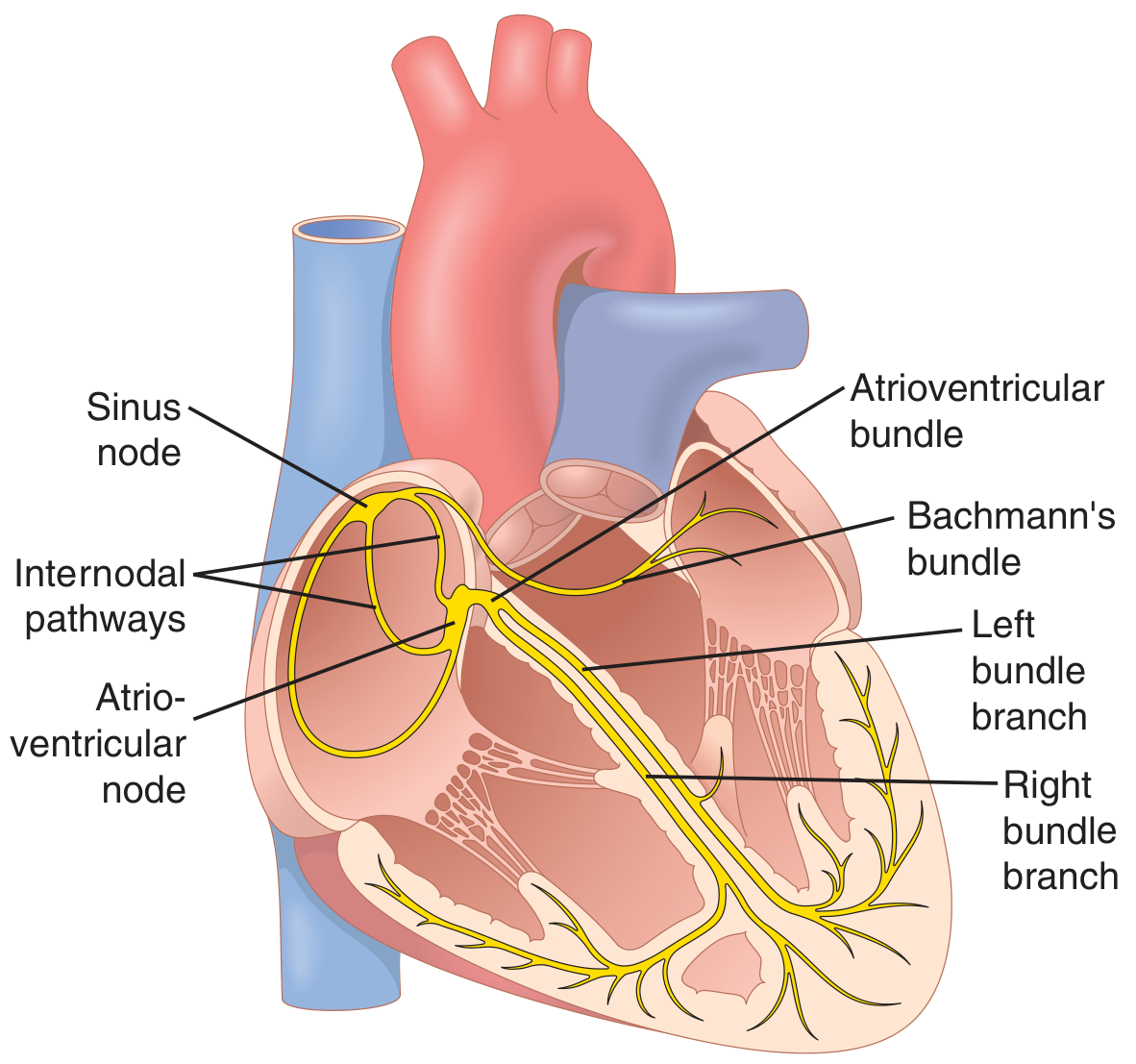
7.2 Components — Detailed
CONDUCTION SYSTEM - SEQUENTIAL PATH:
1. SA NODE (Sinoatrial Node)
• Location: Superior posterolateral wall of RIGHT ATRIUM
(just below and lateral to SVC opening)
• Size: 3 mm wide × 15 mm long × 1 mm thick
• Fiber diameter: 3-5 μm (vs 10-15 μm atrial muscle)
• Fires at: 60-100 bpm (dominant pacemaker)
• Blood supply: SA nodal artery (from RCA in 55-60% of people)
↓
2. INTERNODAL PATHWAYS (in atria)
• Anterior: Bachmann's bundle (also sends branch to LEFT atrium)
• Middle: Wenckebach's tract
• Posterior: Thorel's tract
• Conduct at: 1.0 m/s
↓
3. AV NODE (Atrioventricular Node)
• Location: Posterior-inferior RIGHT ATRIUM, near tricuspid valve
• Size: 6 mm × 3 mm × 1 mm (very small)
• DELAY: 0.09-0.13 seconds (intentional delay!)
• Conducts at: 0.02-0.05 m/s (SLOWEST in heart)
• Inherent rate if it takes over: 40-60 bpm
↓
4. BUNDLE OF HIS (AV Bundle)
• Penetrates fibrous skeleton separating atria from ventricles
• Only electrical connection between atria and ventricles
• Runs through interventricular septum
↓
5. LEFT AND RIGHT BUNDLE BRANCHES
• Right bundle branch → right ventricle
• Left bundle branch → divides into:
- Left anterior fascicle
- Left posterior fascicle
↓
6. PURKINJE FIBERS
• Subendocardial network in BOTH ventricles
• Fiber diameter: very large (70-80 μm)
• Conduction speed: 1.5-4.0 m/s (FASTEST in heart)
• Spreads impulse to ALL ventricular muscle within 0.03 s
• Inherent rate: 15-40 bpm
↓
7. VENTRICULAR MYOCARDIUM
• Impulse spreads from endocardium → epicardium
• Conduction: 0.3-0.5 m/s
7.3 SA Node - Self-Excitation (Automaticity)
DIAGRAM — SA Nodal Action Potential vs. Ventricular Muscle (Guyton & Hall, Fig. 10.2)
FLOWCHART — SA Node Self-Excitation Mechanism
After each action potential, SA node repolarizes to ~-55 to -60 mV
↓
Cell membrane is LEAKY to Na⁺ and Ca²⁺ (funny channels, If)
↓
Na⁺ slowly leaks INTO the cell (inward "funny" current)
↓
Membrane potential slowly drifts toward less-negative value
(THE PACEMAKER POTENTIAL / PREPOTENTIAL)
↓
When membrane potential reaches THRESHOLD: ~-40 mV
↓
L-type Ca²⁺ channels OPEN → Ca²⁺ rushes in
↓
ACTION POTENTIAL FIRES (upstroke caused by Ca²⁺, NOT Na⁺)
↓
Ca²⁺ channels inactivate (close at 100-150 ms)
+ K⁺ channels open → K⁺ efflux → REPOLARIZATION + hyperpolarization
↓
K⁺ channels close → funny current restarts → CYCLE REPEATS
(Inherent rate: 60-100 times/minute)
Why SA node fires first: Its resting potential is only -55 mV (vs. -90 mV in ventricle). The membrane is already "half-ready" to fire. The pacemaker potential reaches threshold faster than in any other part of the conduction system.
7.4 AV Node — The Gatekeeper
WHY is the AV delay essential?
Without AV delay (0.09-0.13 s):
┌──────────┐ ┌──────────┐
│ ATRIA │ contracts │VENTRICLES│
│ (at SA) │ TOGETHER │ │
└──────────┘ → └──────────┘
↓ Result: Atria and ventricles contract SIMULTANEOUSLY
↓ Atria CANNOT empty into ventricles
↓ Ventricular filling is IMPAIRED
↓ Cardiac output DROPS significantly
With AV delay (0.09-0.13 s):
┌──────────┐ 0.09-0.13 s later ┌──────────┐
│ ATRIA │─────────────────────────► │VENTRICLES│
└──────────┘ Atria contract & empty └──────────┘
↓ Ventricles are properly filled BEFORE they contract
↓ Optimal cardiac output
7.5 Purkinje System — Speed is the Advantage
WHY are Purkinje fibers so fast?
• Very large diameter fibers (70-80 μm vs. 10-15 μm)
• Large diameter = low internal resistance = fast conduction
RESULT:
Impulse reaches ALL parts of both ventricles
in ~0.03 seconds (30 milliseconds)
→ ALL ventricular cells depolarize NEARLY SIMULTANEOUSLY
→ Maximum pressure development in the ventricle
→ Optimal ejection of blood
7.6 Conduction Velocities Summary
Structure Velocity Purpose
─────────────────────────────────────────────────────────
SA node 0.05 m/s Slow (pacemaker)
Atrial muscle 1.0 m/s Normal conduction
Internodal pathways 1.0-1.5 m/s Rapid atrial spread
AV node 0.02-0.05 m/s ← SLOWEST (creates delay)
Bundle of His 1.0 m/s Normal
Bundle branches 2.0 m/s Rapid
Purkinje fibers 1.5-4.0 m/s ← FASTEST (synchronizes ventricles)
Ventricular muscle 0.3-0.5 m/s Final spread
7.7 Escape Rhythms — Clinical Significance
If SA node fails:
SA node (60-100 bpm) FAILS
↓
AV node takes over: 40-60 bpm
(Junctional rhythm)
↓
If AV node also fails:
Purkinje/Ventricular rhythm: 15-40 bpm
(Very dangerous — patient may collapse)
This is OVERDRIVE SUPPRESSION: the faster pacemaker
suppresses all slower pacemakers by continuously
depolarizing them before they can fire spontaneously.
UNIT 8: CARDIAC OUTPUT, VENOUS RETURN & REGULATION
8.1 Normal Values
| Parameter | Value |
|---|---|
| Resting CO (men) | ~5.6 L/min |
| Resting CO (women) | ~4.9 L/min |
| Commonly quoted average | 5 L/min |
| Cardiac index | 3 L/min/m² |
| Heart rate | 72 bpm |
| Stroke volume | ~70 mL |
| EDV | ~120-130 mL |
| ESV | ~50 mL |
| EF | ~58% |
8.2 Cardiac Output Equation
CO = HR × SV
WHERE:
HR = Heart Rate (beats/min)
SV = Stroke Volume (mL/beat)
SV is determined by:
• Preload (EDV — affected by venous return)
• Afterload (arterial pressure — opposes ejection)
• Contractility (intrinsic strength of myocardium)
8.3 Factors Controlling Cardiac Output
FLOWCHART — Determinants of Cardiac Output
CARDIAC OUTPUT (CO)
║
╔═══════════╩═══════════╗
║ ║
HEART RATE STROKE VOLUME
(Chronotropy) (Inotropy)
║ ║
┌─────────┴──────────┐ ┌────────┴──────────┐
▼ ▼ ▼ ▼
Sympathetic Vagus Preload Afterload
(↑ HR) (↓ HR) (EDV) (Aortic BP)
Thyroid hormone ↑ by venous ↑ = ↓ SV
Temperature return
Epinephrine Frank-Starling
8.4 Venous Return — The Actual Controller
Under normal resting conditions, CO is determined by VENOUS RETURN
(not by the heart itself)
Why?
• The heart can always pump MORE than what comes to it
• The heart never "limits" output under normal conditions
• The PERIPHERAL TISSUES control their own blood flow
Tissues active → ↓ O₂ + ↑ CO₂ + ↑ adenosine → local vasodilation
→ ↑ blood flow to that tissue
→ ↑ venous return
→ ↑ EDV (Frank-Starling)
→ ↑ SV → ↑ CO
8.5 Fick's Principle (Measurement of CO)
CO = O₂ consumption rate ÷ (Arteriovenous O₂ difference)
Example:
O₂ consumed by body = 250 mL/min
O₂ in pulmonary vein = 0.20 mL/mL blood
O₂ in pulmonary artery = 0.15 mL/mL blood
A-V difference = 0.05 mL/mL blood
CO = 250 ÷ (0.05 × 1000) = 250 ÷ 50 = 5 L/min ✓
UNIT 9: ELECTROCARDIOGRAPHY (ECG)
9.1 Basic Principle
Depolarization wave passing through heart
↓
Current spreads through surrounding tissues
↓
Reaches body surface
↓
Electrodes on skin detect tiny voltage differences
↓
ECG machine amplifies and records these as waves
9.2 Normal ECG Waveform
mV
0.8│ R
│ / \
0.6│ / \
│ / \
0.4│ / \
│ / \ T
0.2│ / ST \ _____
│ P segment \ /
0 │ / \ \/
│/ \
-0│ Q S
└──────────────────────────── Time
│←P→│←PR→│←─QRS─→│←ST─→│← T →│
│0.08│0.16│ 0.08 │ │0.16 │
seconds
9.3 ECG Waves — Meaning and Duration
| Component | Ionic Event | Mechanical Event | Duration |
|---|---|---|---|
| P wave | Atrial depolarization | Atrial contraction begins | < 0.12 s |
| PR interval | Atrial depol. + AV delay | From atrial to ventricular contraction | 0.12-0.20 s |
| QRS complex | Ventricular depolarization | Ventricular systole begins | 0.06-0.10 s |
| ST segment | All ventricular cells at plateau (Phase 2) | Ventricular contraction (systole) | Isoelectric |
| T wave | Ventricular repolarization (Phase 3) | Ventricular relaxation begins | 0.16 s |
| QT interval | Total ventricular electrical activity | Entire systole duration | 0.35-0.44 s |
Why is there no atrial repolarization wave visible? Atrial repolarization occurs during the QRS complex and is hidden within it (the large ventricular signal masks the small atrial signal).
9.4 ECG-Cardiac Cycle Correlation
ECG WAVE → MECHANICAL EVENT → HEART SOUND
P wave → Atrial contraction → (silent)
PR interval → AV delay → (silent)
QRS complex → Ventricular systole begins → S1 (lub): valves close
ST segment → Active ejection → (silent)
T wave onset → Ventricles start relaxing → (silent)
T wave end → End of systole → S2 (dub): valves close
After T wave → Ventricular diastole → (silent)
UNIT 10: BLOOD PRESSURE & ITS REGULATION
10.1 Definitions and Normal Values
SYSTOLIC BP = Peak pressure during ventricular ejection = 120 mmHg
DIASTOLIC BP = Lowest pressure during diastole = 80 mmHg
PULSE PRESSURE = Systolic - Diastolic = 120 - 80 = 40 mmHg
MEAN ARTERIAL PRESSURE (MAP) = DBP + 1/3 Pulse Pressure
= 80 + 1/3 (40) = 80 + 13 = 93 mmHg
Also: MAP = CO × Total Peripheral Resistance (TPR)
10.2 Short-Term BP Regulation (Seconds to Minutes)
A) Baroreceptor Reflex (Most Important)
FLOWCHART — Baroreceptor Reflex
BP RISES SUDDENLY (e.g., standing up, excitement)
↓
Baroreceptors STRETCH more
(Location: CAROTID SINUS + AORTIC ARCH)
↓
↑ Firing rate of baroreceptor neurons
↓
Signals travel via CN IX (Carotid sinus nerve)
and CN X (Aortic nerve) → Nucleus tractus solitarius (NTS) in medulla
↓
┌───────┴────────┐
▼ ▼
↓ Sympathetic ↑ Parasympathetic (vagal)
output output
│ │
▼ ▼
↓ Vasoconstriction ↓ Heart rate
↓ Cardiac output ↓ Contractility
│ │
└───────┬────────┘
▼
BP FALLS BACK TO NORMAL
Reversal: If BP drops suddenly, baroreceptors fire less → sympathetic activity increases → BP rises.
Why the baroreceptor reflex is NOT a long-term regulator:
- It adapts (resets) within 1-2 days to a new BP level
- Cannot permanently hold BP at one level
- Only effective for acute BP changes
B) Chemoreceptor Reflex
↓ O₂ OR ↑ CO₂ OR ↑ H⁺ in blood
↓
Peripheral chemoreceptors activated
(Carotid bodies: CN IX; Aortic bodies: CN X)
↓
┌───────┴────────┐
▼ ▼
↑ Breathing rate ↑ Sympathetic activity
→ ↑ HR, vasoconstriction
→ ↑ BP
C) CNS Ischemic Response (Emergency)
Severe ↓ BP → Brain ischemia → CO₂ builds up in vasomotor center
↓
Massive sympathetic discharge
↓
Extreme vasoconstriction + ↑ HR
↓
Can raise BP to 270 mmHg temporarily
("Last-ditch effort" - only at near-death BP levels)
10.3 Long-Term BP Regulation — The Kidney is King
FLOWCHART — Renin-Angiotensin-Aldosterone System (RAAS)
LOW BLOOD PRESSURE OR LOW Na⁺ delivery to macula densa
↓
Juxtaglomerular (JG) cells of kidney
release RENIN (a proteolytic enzyme)
↓
Renin cleaves ANGIOTENSINOGEN (from liver)
↓
ANGIOTENSIN I (inactive decapeptide)
↓
ACE (Angiotensin Converting Enzyme) in LUNGS
↓
ANGIOTENSIN II (active octapeptide)
↓
┌────────────────┬────────────────┬─────────────────┐
▼ ▼ ▼ ▼
Arteriolar Adrenal cortex ↑ ADH Sympathetic
VASOCONSTRICTION → ALDOSTERONE (posterior activation
↑ TPR → ↑ BP release pituitary)
↓ ↓
Na⁺ + H₂O Water retention
retention ↑ Blood volume
↑ Blood volume ↑ CO
↓
↑ CO → ↑ BP
↓
════════════════
BLOOD PRESSURE NORMALIZED
(over hours to days)
Triggers for Renin Release:
- ↓ Renal perfusion pressure (baroreceptors in JG cells)
- ↓ NaCl delivery to macula densa (tubuloglomerular feedback)
- ↑ Sympathetic activity (β₁ receptors on JG cells)
UNIT 11: MICROCIRCULATION & CAPILLARY DYNAMICS
11.1 Structure of Microcirculation
ARTERIOLE (main resistance vessel; 10-15 μm internal diameter)
│
▼
METARTERIOLE (connects arteriole to capillary; 10-35 μm)
│
├──────────────────────┐
▼ ▼
PRECAPILLARY SPHINCTER PREFERENTIAL CHANNEL
(smooth muscle ring) (thoroughfare channel;
Controls entry to blood bypasses capillaries
true capillaries when not needed)
│
▼
TRUE CAPILLARIES (5-9 μm; single endothelial cell layer)
(Gas and nutrient exchange occurs here)
│
▼
VENULE → VEIN
Vasomotion: Precapillary sphincters alternately open and close (every 10-30 seconds), driven by local O₂ levels. When O₂ is low → sphincter opens → more capillary flow.
11.2 Starling Forces — Capillary Fluid Exchange
FLOWCHART — Forces at the Capillary
ARTERIAL END of capillary: VENOUS END of capillary:
Capillary hydrostatic P = 35 mmHg Capillary hydrostatic P = 15 mmHg
Interstitial hydrostatic P = -3 mmHg Interstitial hydrostatic P = -3 mmHg
Plasma colloid osmotic P = 28 mmHg Plasma colloid osmotic P = 28 mmHg
Interstitial colloid osmotic P = 8 Interstitial colloid osmotic P = 8
FILTRATION forces = 35 + 8 = 43 FILTRATION forces = 15 + 8 = 23
ABSORPTION forces = 28 + 3 = 31 ABSORPTION forces = 28 + 3 = 31
(negative interstitial P adds to abs.)
NET FILTRATION = 43 - 31 = +12 NET FILTRATION = 23 - 31 = -8
→ FLUID LEAVES capillary → FLUID ENTERS capillary
Result:
• Arterial end: filtration OUT (delivers O₂, nutrients to tissues)
• Venous end: absorption IN (removes CO₂, waste from tissues)
• ~90% of filtered fluid reabsorbed at venous end
• Remaining ~10% → lymphatics → returned to circulation
11.3 Starling Equation
Net filtration = Kf [(Pc + πi) - (πc + Pi)]
WHERE:
Kf = Filtration coefficient (capillary permeability × surface area)
Pc = Capillary hydrostatic pressure (pushes fluid OUT)
πi = Interstitial colloid osmotic pressure (pulls fluid OUT)
πc = Plasma colloid osmotic pressure (pulls fluid IN)
Pi = Interstitial hydrostatic pressure (pushes fluid IN)
11.4 Edema — When the Balance is Disturbed
FLOWCHART — Causes of Edema
EDEMA = Excess fluid accumulation in interstitial space
CAUSE 1: ↑ Capillary Hydrostatic Pressure
• Right heart failure → venous congestion → ↑ venous pressure
• Portal hypertension → ascites
→ Net filtration ↑ → fluid moves OUT of capillary
CAUSE 2: ↓ Plasma Colloid Osmotic Pressure
• ↓ Plasma proteins (albumin)
• Causes: Liver failure, nephrotic syndrome, malnutrition
→ Less "pull" to bring fluid back in → edema
CAUSE 3: Lymphatic Obstruction
• Filariasis (elephantiasis)
• Cancer blocking lymph nodes
→ Protein accumulates in interstitium → ↑ πi → more fluid out
CAUSE 4: ↑ Capillary Permeability
• Histamine, bradykinin (allergy, inflammation)
• Burns, trauma
→ Proteins leak out → ↑ πi → fluid follows proteins
UNIT 12: CARDIAC OUTPUT IN SPECIAL STATES
12.1 Exercise
EXERCISE:
↓
Skeletal muscle contraction
↓
↑ O₂ demand + ↑ CO₂ + ↑ H⁺ + ↑ adenosine + ↑ K⁺ (local factors)
↓
Local vasodilation in muscles
↓
↑ Venous return (ALSO aided by: muscle pump + respiratory pump)
↓
↑ EDV → Frank-Starling → ↑ SV
↓
PLUS: Sympathetic activation → ↑ HR + ↑ Contractility
↓
CO INCREASES FROM 5 L/min (rest) TO:
• Moderately fit person: ~15-20 L/min
• Elite athlete: up to 35 L/min
↓
Heart rate reaches 150-180 bpm
Muscle Pump Mechanism:
Skeletal muscle contracts
↓
Compresses veins within the muscle
↓
Blood squeezed toward heart (one-way venous valves prevent backflow)
↓
↑ Venous return → ↑ CO
12.2 Pregnancy
MATERNAL CARDIOVASCULAR CHANGES:
Blood volume ↑ 30-40%
(Driven by ↑ aldosterone + ↑ estrogen → Na⁺ and water retention)
↓
EDV ↑ → Frank-Starling → ↑ SV
↓
CO increases from 5 → 7 L/min (+40-45%) by 32 weeks
↓
HR also increases ~15-20 bpm
↓
BP remains normal or slightly low
(Due to ↓ TPR from progesterone-mediated vasodilation
and the low-resistance placental circulation)
↓
Signs: physiological systolic flow murmur, displaced apex beat,
exaggerated S3 (loud — normal in pregnancy)
12.3 Fetal Circulation
FETAL CIRCULATION DIAGRAM:
PLACENTA (gas exchange)
↓
Umbilical vein
(oxygenated blood, PO₂ ~30-35 mmHg)
↓
DUCTUS VENOSUS ──────────────────► Bypasses liver (liver largely bypassed)
↓ (Small amount goes to liver)
Inferior Vena Cava (IVC)
↓
RIGHT ATRIUM
│
├──(70% via FORAMEN OVALE)──► LEFT ATRIUM → LEFT VENTRICLE → AORTA
│ [Right-to-Left shunt] (Best O₂ blood → brain, heart)
│
└──(30% → RIGHT VENTRICLE → PULMONARY ARTERY)
│
├──(small amount → to the collapsed lungs)
│
└──(DUCTUS ARTERIOSUS)──► AORTA (bypasses lungs)
[Pulmonary-to-aortic shunt]
↓
Descending aorta
↓
Umbilical arteries → Placenta (for O₂ exchange)
Changes at Birth:
BABY TAKES FIRST BREATH
↓
Lungs expand → pulmonary vascular resistance ↓ dramatically
↓
↑ Blood flow to lungs → ↑ blood returning to LEFT atrium
↓
LEFT atrial pressure > RIGHT atrial pressure
↓
FORAMEN OVALE CLOSES (flap valve mechanism, permanent closure in weeks)
↓
↑ O₂ tension in blood → prostaglandins change → smooth muscle contracts
↓
DUCTUS ARTERIOSUS CLOSES (within 10-15 hours; permanent in 1-3 months)
↓
DUCTUS VENOSUS CLOSES (umbilical cord cut → no flow → fibrous remnant)
↓
Adult circulation established
| Fetal Structure | Adult Remnant |
|---|---|
| Foramen ovale | Fossa ovalis (depression in atrial septum) |
| Ductus arteriosus | Ligamentum arteriosum |
| Ductus venosus | Ligamentum venosum |
| Umbilical vein | Ligamentum teres hepatis |
| Umbilical arteries | Medial umbilical ligaments |
MASTER SUMMARY: KEY NUMBERS FOR BDS EXAMS
╔══════════════════════════════════════════════════════════════════╗
║ CARDIOVASCULAR "MUST KNOW" VALUES ║
╠══════════════════════════════════════════════════════════════════╣
║ Cardiac output (rest) │ ~5 L/min ║
║ Cardiac index │ ~3 L/min/m² ║
║ Heart rate │ 72 bpm ║
║ Stroke volume │ ~70 mL ║
║ EDV │ ~120-130 mL ║
║ ESV │ ~50 mL ║
║ Ejection fraction │ ~58% (normal: >55%) ║
╠══════════════════════════════════════════════════════════════════╣
║ Aortic BP (systolic/diastolic) │ 120/80 mmHg ║
║ MAP │ ~93 mmHg ║
║ Pulse pressure │ 40 mmHg ║
║ Pulmonary artery BP │ 25/8 mmHg ║
╠══════════════════════════════════════════════════════════════════╣
║ SA node rate │ 60-100 bpm ║
║ AV node rate │ 40-60 bpm ║
║ Purkinje fiber rate │ 15-40 bpm ║
║ AV nodal delay │ 0.09 s ║
║ Cardiac cycle duration │ 0.8 s (at 72 bpm) ║
╠══════════════════════════════════════════════════════════════════╣
║ AP plateau duration (ventricle)│ ~200 ms ║
║ ARP duration │ ~250 ms ║
║ Resting MP (ventricle) │ -85 to -90 mV ║
║ Resting MP (SA node) │ -55 to -60 mV ║
║ Threshold for SA node firing │ -40 mV ║
║ Ventricular AP amplitude │ ~105 mV (-85 to +20 mV) ║
╠══════════════════════════════════════════════════════════════════╣
║ Plasma colloid osmotic P │ ~28 mmHg ║
║ Capillary HP (arterial end) │ ~35 mmHg ║
║ Capillary HP (venous end) │ ~15 mmHg ║
║ Purkinje conduction velocity │ 1.5-4.0 m/s ║
║ AV node conduction velocity │ 0.02-0.05 m/s ║
╚══════════════════════════════════════════════════════════════════╝
FREQUENTLY ASKED BDS 1ST YEAR EXAM QUESTIONS
Short Answer Questions (SAQ):
- Define cardiac cycle. Describe the events of the cardiac cycle with pressure and volume changes.
- What is Frank-Starling law? Explain its mechanism and significance.
- Describe the properties of cardiac muscle.
- Write about the conduction system of the heart with conduction velocities.
- What is the baroreceptor reflex? Describe its role in blood pressure regulation.
- Compare action potentials of cardiac muscle and skeletal muscle.
- Describe the renin-angiotensin-aldosterone system.
- Write about Starling's forces in capillary exchange. What causes edema?
Long Essay Questions (LEQ):
- Describe the regulation of cardiac output. Add a note on venous return.
- Explain the electrocardiogram (ECG) — its basis, normal waveforms, and relation to the cardiac cycle.
- Describe the fetal circulation. What changes occur at birth?
Reference: Guyton and Hall Textbook of Medical Physiology, 14th Edition (ISBN: 9780443111013) — Chapters 9, 10, 11, 18, 19, 20, and 23. All diagrams sourced directly from this textbook.
Make these notes so that I can, uh, ace my physiology exam and, uh, add more details to it.
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Here are your complete, exam-crushing cardiovascular physiology notes with every diagram, flowchart, mnemonic, clinical correlation, and extra detail added. These are structured for maximum retention and BDS exam performance.
🫀 CARDIOVASCULAR SYSTEM — ULTIMATE BDS EXAM NOTES
Guyton & Hall Textbook of Medical Physiology, 14th Edition
"Everything you need. Nothing you don't."
╔══ UNIT 1: OVERVIEW OF THE CARDIOVASCULAR SYSTEM ══╗
1.1 Basic Design
The cardiovascular system is a closed, pressurized transport circuit powered by a muscular pump (the heart). Its job is simple: get the right stuff to every cell and take the waste away.
DIAGRAM — Heart Structure and Blood Flow (Guyton & Hall, Fig. 9.1)
Fig. 9.1 — Structure of the heart and course of blood flow. Note the wall layers on the bottom-right inset: Endocardium → Myocardium → Epicardium → Pericardial space → Parietal pericardium → Fibrous pericardium. [Guyton & Hall, p. 122]
1.2 The Two Circulations — Side by Side
┌─────────────────────────────────────────────────────────────────┐
│ PULMONARY CIRCULATION SYSTEMIC CIRCULATION │
│ (Right Heart → Lungs) (Left Heart → Body) │
│ │
│ Right Ventricle pumps → Left Ventricle pumps → │
│ Pulmonary artery → Aorta → │
│ Lung capillaries → Systemic capillaries → │
│ Gas exchange (O₂ in, CO₂ out) Nutrient/O₂ delivery → │
│ Pulmonary veins → Venae Cavae → │
│ Left Atrium Right Atrium │
│ │
│ Pressure: 25/8 mmHg Pressure: 120/80 mmHg │
│ Low resistance, high flow High resistance, high pressure │
└─────────────────────────────────────────────────────────────────┘
1.3 Heart Wall Layers — Inside Out
INSIDE THE HEART CAVITY
↓
ENDOCARDIUM ← Smooth inner lining; prevents clot formation
↓
MYOCARDIUM ← Cardiac muscle; the actual PUMP
↓
EPICARDIUM ← = Visceral pericardium; covers the heart
↓
PERICARDIAL SPACE ← Contains 10-20 mL of lubricating fluid
↓
PARIETAL PERICARDIUM ← Lines the inner sac
↓
FIBROUS PERICARDIUM ← Tough outer layer; anchors heart to diaphragm
OUTSIDE
🏥 Clinical — Pericardial Effusion: Too much fluid in the pericardial space (e.g., in tuberculosis, malignancy) compresses the heart → cardiac tamponade → ↓ filling → ↓ CO → shock.
1.4 Five Core Functions
| Function | Mechanism | Example |
|---|---|---|
| O₂ & nutrient delivery | Arterial blood to capillaries | Brain needs continuous O₂ |
| Waste removal | CO₂ → lungs; urea → kidneys | Cessation = unconsciousness in 5s |
| Temperature regulation | Skin vasoconstriction / dilation | Fever → ↑ HR |
| Hormone transport | Endocrine system delivery | Adrenaline from adrenals to heart |
| Immune defense | WBCs and antibodies circulate | Infection response |
1.5 Volumes of Blood Distribution (Resting)
WHERE IS YOUR 5 LITRES OF BLOOD RIGHT NOW?
Systemic veins & venules 64% ████████████████████████████
Pulmonary circulation 9% ███
Heart (at any moment) 7% ██
Systemic arteries 13% █████
Systemic capillaries 7% ██
Exam Tip: Veins are the "blood reservoir" of the body. This is why they are called capacitance vessels. Arteries are resistance vessels (pressure vessels).
╔══ UNIT 2: CARDIAC MUSCLE PHYSIOLOGY ══╗
2.1 Three Types of Cardiac Muscle
╔═══════════════════════════════════════╗
║ THREE TYPES OF CARDIAC MUSCLE ║
╠═══════════════════╦═══════════════════╣
║ Atrial muscle ║ Ventricular muscle ║
║ • Thin walls ║ • Thick walls ║
║ • Low pressure ║ • High pressure ║
║ • Primer pump ║ • Main pump ║
╠═══════════════════╩═══════════════════╣
║ Specialized fibers (SA, AV, Purkinje) ║
║ • Fewer contractile fibrils ║
║ • Cannot contract forcefully ║
║ • GENERATE + CONDUCT electrical signals ║
╚═══════════════════════════════════════╝
2.2 Cardiac Muscle Histology
DIAGRAM — Intercalated Discs in Cardiac Muscle (Guyton & Hall, Fig. 9.2)
Fig. 9.2 — The dark bands crossing the fibers are intercalated discs. Each disc contains gap junctions (for electrical conduction) and desmosomes (for mechanical strength). [Guyton & Hall, p. 122]
What is an Intercalated Disc?
INTERCALATED DISC
│
├── Gap Junctions (Nexuses)
│ → Ion channels connecting cells
│ → Very low electrical resistance
│ → Action potential spreads cell-to-cell freely
│ → Makes cardiac muscle a FUNCTIONAL SYNCYTIUM
│
└── Desmosomes
→ Mechanical attachment (like Velcro between cells)
→ Prevents cells from pulling apart during contraction
2.3 Syncytium — The Most Exam-Important Concept
FUNCTIONAL SYNCYTIUM = The heart behaves as ONE BIG CELL
When one cell fires → ALL cells fire (all-or-nothing for the whole heart)
TWO SYNCYTIA exist (separated by fibrous AV ring):
┌──────────────────┐ ┌───────────────────┐
│ ATRIAL syncytium │ ─gap─ │ VENTRICULAR syncyt.│
│ (fires first) │ only at │ (fires ~0.1-0.2s │
│ Atria contract │ AV node │ later) │
└──────────────────┘ └───────────────────┘
WHY TWO SEPARATE SYNCYTIA? → Atria must contract BEFORE ventricles.
If they were one syncytium, both would contract simultaneously
→ Ventricles wouldn't fill properly → ↓ cardiac output.
2.4 Cardiac vs. Skeletal Muscle — Full Comparison Table
| Feature | Cardiac Muscle | Skeletal Muscle |
|---|---|---|
| Shape | Branched, interconnected | Long, parallel cylinders |
| Nucleus | 1, central | Multiple, peripheral |
| Striations | Yes (actin + myosin) | Yes |
| Intercalated discs | Yes (unique!) | No |
| Syncytium | Yes (functional) | No |
| Control | Involuntary (autonomic) | Voluntary |
| AP duration | 250-300 ms | 1-2 ms |
| Plateau phase | Yes (Phase 2) | No |
| Absolute Refractory Period | ~250 ms (= contraction duration) | Very short |
| Tetanus possible? | NO | Yes |
| Self-excitation (automaticity) | Yes (SA node) | No |
| Ca²⁺ source | Extracellular + SR | Mainly SR only |
| Fatigue | Never fatigues (aerobic metabolism) | Fatigues quickly |
| Energy substrate | Fatty acids (60%), glucose | Glucose, glycogen |
🔑 MNEMONIC for cardiac muscle features: "SAIL-CAP"
- Syncytium (functional)
- Automaticity (self-excitation)
- Intercalated discs
- Long action potential with plateau
- Cannot tetanize (long ARP)
- Aerobic (never fatigues)
- Plateau (Phase 2 of AP)
2.5 Properties of Cardiac Muscle — The "ACERRD" Properties
PROPERTIES OF CARDIAC MUSCLE:
A — AUTOMATICITY : SA node self-excites without neural input
C — CONDUCTIVITY : AP spreads through intercalated discs
E — EXCITABILITY : Responds to stimuli (above threshold)
R — RHYTHMICITY : Regular, repetitive self-excitation
R — REFRACTORINESS : Long ARP prevents tetanus
D — DISTENSIBILITY : Can stretch (Frank-Starling law)
+ CONTRACTILITY : Responds to stretch with more force
2.6 Left Ventricular Torsion (Twist Mechanics)
LEFT VENTRICLE FIBER ARRANGEMENT:
SUBEPICARDIAL fibers: ↙ leftward spiral
MIDWALL fibers: ↔ circumferential
SUBENDOCARDIAL fibers: ↘ rightward spiral
DURING SYSTOLE (contraction):
Apex rotates COUNTERCLOCKWISE (viewed from apex)
Base rotates CLOCKWISE
→ Net: WRINGING / TWISTING like squeezing a towel
→ Pulls base toward apex → efficient ejection
DURING DIASTOLE (relaxation):
Heart UNTWISTS like a loaded spring
→ Creates SUCTION effect
→ Rapid filling of ventricle
→ This is why ~70-80% of filling is PASSIVE (no atrial contraction needed)
╔══ UNIT 3: ACTION POTENTIALS IN CARDIAC MUSCLE ══╗
3.1 The Action Potential Diagram
DIAGRAM — 5 Phases of Ventricular Action Potential with Ionic Currents (Guyton & Hall, Fig. 9.5)
Fig. 9.5 — Phase 0 (Na⁺ rush in), Phase 1 (brief repolarization), Phase 2 (Ca²⁺ plateau), Phase 3 (K⁺ out), Phase 4 (resting). Lower panel shows ionic currents: Na⁺ inward, Ca²⁺ inward, K⁺ outward. [Guyton & Hall, p. 123]
DIAGRAM — Purkinje vs. Ventricular Muscle APs showing the Plateau (Guyton & Hall, Fig. 9.4)
Fig. 9.4 — Note the prominent PLATEAU in both fiber types. Purkinje fiber rests at ~-90 mV; ventricular muscle at ~-80 mV. The plateau lasts ~200 ms, making the AP 15× longer than skeletal muscle. [Guyton & Hall, p. 123]
3.2 All 5 Phases — Detailed
VENTRICULAR MUSCLE ACTION POTENTIAL (Total duration: ~250-300 ms)
══════════════════════════════════════════════════════════════════
PHASE 4 — Resting Membrane Potential
Value: -85 to -90 mV
Na⁺/K⁺-ATPase pump maintains: high K⁺ inside, high Na⁺ outside
Cell is POLARIZED (negative inside)
────────────────────────────────────────────────────────────────
PHASE 0 — Rapid Depolarization (upstroke) [Duration: 1-2 ms]
Trigger: stimulus from adjacent cell via gap junction
Fast Na⁺ channels OPEN → massive Na⁺ influx
Potential shoots from -90 mV to +20 mV (105 mV total swing)
Then fast Na⁺ channels CLOSE (inactivate)
────────────────────────────────────────────────────────────────
PHASE 1 — Early/Initial Repolarization [very brief]
Fast Na⁺ channels close
Transient outward K⁺ current (Ito) causes slight repolarization
────────────────────────────────────────────────────────────────
PHASE 2 — PLATEAU [Duration: ~150-200 ms] ← UNIQUE TO CARDIAC MUSCLE
TWO simultaneous events maintain the plateau:
(a) L-type Ca²⁺ channels (slow calcium channels) OPEN
→ Ca²⁺ + Na⁺ flow IN (positive charges in = keeps it positive)
(b) K⁺ permeability DECREASES 5-fold (K⁺ can't escape)
Net result: membrane stays depolarized for a long time
→ This Ca²⁺ influx directly TRIGGERS MUSCLE CONTRACTION
────────────────────────────────────────────────────────────────
PHASE 3 — Rapid Repolarization [Duration: ~50 ms]
L-type Ca²⁺ channels CLOSE (inactivate after ~100-150 ms)
K⁺ channels OPEN → massive K⁺ efflux (positive charges OUT)
Membrane potential returns rapidly to -90 mV
────────────────────────────────────────────────────────────────
PHASE 4 — Resting Potential restored
Na⁺/K⁺ ATPase pumps Na⁺ out and K⁺ back in
Cell ready for next stimulus
3.3 Refractory Periods — Critical for Exam
ABSOLUTE REFRACTORY PERIOD (ARP) = ~250 ms
→ No stimulus of ANY strength can cause another AP
→ Corresponds to Phase 0, 1, 2, and early Phase 3
→ Lasts almost as long as mechanical contraction (~300 ms)
→ WHY? Fast Na⁺ channel inactivation gates remain closed
RELATIVE REFRACTORY PERIOD (RRP) = ~50 ms
→ A STRONGER than normal stimulus CAN cause an AP
→ Corresponds to late Phase 3
→ Premature ventricular contractions (PVCs) can occur here
SUPERNORMAL PERIOD (SNP)
→ Slightly less stimulus than normal triggers an AP
→ Follows RRP; important in arrhythmia genesis
🔑 WHY IS THE LONG ARP LIFE-SAVING? The ARP lasts as long as the contraction. The heart CANNOT receive a second stimulus during its own contraction. This prevents tetanic contraction (sustained cramping). A tetanic heart would never relax → no filling → death. This is the single most important protective feature of cardiac electrophysiology.
3.4 SA Node Action Potential — Completely Different!
DIAGRAM — SA Nodal Action Potential vs. Ventricular Muscle (Guyton & Hall, Fig. 10.2)
Fig. 10.2 — SA node (pink): resting potential drifts slowly upward to threshold at -40 mV → fires. Ventricular muscle (green): stable resting potential at -90 mV; needs external stimulus. The "funny" Na⁺ current (If) drives the pacemaker potential. [Guyton & Hall, p. 136]
SA NODE AP vs. VENTRICULAR AP — KEY DIFFERENCES:
Feature SA Node Ventricle
─────────────────────────────────────────────────────
Resting potential -55 to -60 mV -85 to -90 mV
Threshold -40 mV -65 mV
Upstroke by Ca²⁺ (slow) Na⁺ (fast)
Plateau Absent Present
Pacemaker potential PRESENT (key feature) Absent
Self-excitation Yes No
AP amplitude ~60-70 mV ~105 mV
AP shape Rounded Sharp spike + plateau
🔑 MNEMONIC: SA node rests at -55 → threshold at -40: "Fifty-Five to Forty" Ventricle rests at -90 → threshold at -65: "Ninety to Sixty-Five"
╔══ UNIT 4: THE CARDIAC CYCLE ══╗
4.1 The Wiggers Diagram — Master Diagram of Cardiology
DIAGRAM — Complete Cardiac Cycle Events (Guyton & Hall, Fig. 9.8)
Fig. 9.8 — The Wiggers Diagram: The single most important diagram in cardiac physiology. Memorize this completely. Correlates LV pressure, aortic pressure, atrial pressure, ventricular volume, ECG, and heart sounds through one complete cardiac cycle. [Guyton & Hall, p. 127]
4.2 Seven Phases of the Cardiac Cycle — The Full Story
CARDIAC CYCLE (Total = 0.8 s at 72 bpm)
HR doubles → cycle halves to 0.4 s (diastole is shortened more than systole)
DIASTOLE = 0.5 s (filling phase)
══════════════════════════════════════════════════════════════
PHASE 1: ISOVOLUMETRIC RELAXATION (0.04 s)
Trigger: T wave on ECG → ventricular muscle begins relaxing
Events:
• Aortic valve CLOSES (LV pressure falls below aortic pressure, ~80 mmHg)
• Mitral valve still CLOSED (LV pressure still > LA pressure)
• ALL FOUR VALVES CLOSED
• LV pressure falls rapidly: 80 mmHg → ~0-5 mmHg
• Volume UNCHANGED (isovolumetric = same volume)
• Volume = End-Systolic Volume (ESV) = ~50 mL
Heart sounds: S2 (aortic + pulmonary valve closure)
──────────────────────────────────────────────────────────────
PHASE 2: RAPID VENTRICULAR FILLING (0.11 s)
Trigger: LV pressure falls below LA pressure
Events:
• Mitral valve OPENS
• Blood rushes passively from LA into LV down pressure gradient
• 70-80% of total ventricular filling occurs here (passive!)
• LV volume rises rapidly
• LA pressure briefly drops (a-wave absent here, v-wave present earlier)
Heart sounds: S3 (rapid filling sound — NORMAL in children, abnormal in adults >40)
──────────────────────────────────────────────────────────────
PHASE 3: DIASTASIS / SLOW FILLING (0.19 s)
Events:
• Filling slows as pressure difference between LA and LV equalizes
• Blood still trickles in passively
• This phase SHORTENS most with increased HR
──────────────────────────────────────────────────────────────
PHASE 4: ATRIAL SYSTOLE (0.11 s)
Trigger: P wave on ECG → SA node fires → atria depolarize + contract
Events:
• Atria contract → "booster pump" adds final 20-30% to LV filling
• LV EDV reaches maximum: ~120-130 mL
• LA pressure shows the "a wave" (atrial contraction wave)
• Critical in FAST heart rates when diastasis is very short
Heart sounds: S4 (atrial kick against stiff ventricle — always ABNORMAL)
SYSTOLE = 0.3 s (ejection phase)
══════════════════════════════════════════════════════════════
PHASE 5: ISOVOLUMETRIC CONTRACTION (0.05 s)
Trigger: QRS complex → ventricles depolarize → contraction begins
Events:
• Mitral valve CLOSES (LV pressure exceeds LA pressure ~5 mmHg)
• ALL FOUR VALVES CLOSED
• LV pressure rises rapidly from ~5 mmHg → 80 mmHg
• Volume UNCHANGED (isovolumetric = same volume, ~120 mL)
Heart sounds: S1 (mitral + tricuspid closure) ← "lub"
──────────────────────────────────────────────────────────────
PHASE 6: RAPID EJECTION (0.12 s)
Trigger: LV pressure exceeds aortic pressure (>80 mmHg)
Events:
• Aortic valve OPENS
• Blood is rapidly ejected into aorta
• LV pressure peaks at 120 mmHg (= systolic BP)
• Aortic pressure also rises to ~120 mmHg
• ~70% of stroke volume ejected in this phase
──────────────────────────────────────────────────────────────
PHASE 7: REDUCED/SLOW EJECTION (0.13 s)
Events:
• LV begins to relax → contraction force decreases
• Blood still flowing into aorta (inertia) but slowing
• Remaining ~30% of stroke volume ejected
• LV pressure falls below aortic pressure (but blood still flows forward due to inertia)
• Aortic valve CLOSES when blood reversal begins
• Dicrotic notch (incisura) on aortic pressure curve = aortic valve closure
• ESV = ~50 mL remains in LV
4.3 Valve Events Summary — 3-Column Quick Ref
| Event | Valve Opening | Valve Closing |
|---|---|---|
| Start of systole | - | Mitral + Tricuspid close (S1) |
| Mid-systole | Aortic + Pulmonary open | - |
| End of systole | - | Aortic + Pulmonary close (S2) |
| Early diastole | Mitral + Tricuspid open | - |
| Late diastole | - | - (all open, filling) |
4.4 Heart Sounds — Complete Detail
S1 ("LUB") — LOUDER, LONGER, LOWER PITCHED
Cause: Closure of MITRAL (M1) + TRICUSPID (T1) valves
Timing: Beginning of SYSTOLE
M1 closes slightly before T1
Best heard: Mitral area (cardiac apex, 5th ICS, MCL)
Splitting: M1-T1 split widens on inspiration (normal wide split)
S2 ("DUB") — SOFTER, SHORTER, HIGHER PITCHED
Cause: Closure of AORTIC (A2) + PULMONARY (P2) valves
Timing: End of SYSTOLE / beginning of DIASTOLE
A2 closes slightly before P2
Best heard: Aortic area (2nd ICS, right sternal border)
NORMAL SPLIT on INSPIRATION: P2 delayed (more venous return to RV
→ RV takes longer to empty → pulmonary valve closes later)
S3 — LOW-PITCHED DULL SOUND
Timing: Early diastole (after S2) — "lub-dub-bum"
Cause: Rapid ventricular filling causing vibration of ventricular walls
NORMAL in: Children, athletes, young adults, pregnancy
ABNORMAL (pathological) in: Adults >40 years = HEART FAILURE
(stiff, dilated, poorly contracting LV)
S4 — LOW-PITCHED DULL SOUND
Timing: Late diastole (just before S1) — "bum-lub-dub"
Cause: Atrial contraction (a-wave) against a STIFF ventricle
ALWAYS PATHOLOGICAL
Causes: Hypertension, aortic stenosis, hypertrophic cardiomyopathy
(stiff LV needs extra atrial push → generates audible vibration)
🔑 MNEMONIC for heart sounds: "Many Things Are Passionately" → valve auscultation areas:
- Mitral = apex (5th ICS, left MCL)
- Tricuspid = left lower sternal border (4th ICS)
- Aortic = 2nd ICS, right sternal border
- Pulmonary = 2nd ICS, left sternal border
4.5 Atrial Pressure Waves — a, c, v
ATRIAL PRESSURE WAVE CAUSE TIMING
─────────────────────────────────────────────────────────────────
"a" wave Atrial CONTRACTION Late diastole
(LA rises 7-8 mmHg; (after P wave)
RA rises 4-6 mmHg)
"c" wave AV valve BULGING back Just after QRS
into atrium during (isovolumetric
isovolumetric contraction contraction)
"v" wave Venous FILLING of atrium During ventricular
while AV valves are closed systole (building
pressure in atrium)
─────────────────────────────────────────────────────────────────
CLINICAL: Absent "a" wave → Atrial fibrillation (no organized atrial contraction)
Large "v" wave → Mitral regurgitation (blood regurgitates into LA during systole)
╔══ UNIT 5: WORK OUTPUT OF THE HEART ══╗
5.1 Essential Formulas
╔══════════════════════════════════════════════════════════════╗
║ STROKE VOLUME (SV) = EDV - ESV = 120 - 50 = 70 mL ║
║ CARDIAC OUTPUT (CO) = HR × SV = 72 × 70 = ~5 L/min ║
║ EJECTION FRACTION = SV ÷ EDV × 100 = 70÷120 × 100 = 58% ║
║ CARDIAC INDEX = CO ÷ BSA = 5 ÷ 1.7 = ~3 L/min/m² ║
║ MEAN ARTERIAL PRESSURE = DBP + ⅓ Pulse Pressure ║
║ = 80 + ⅓(40) = 93 mmHg ║
║ PULSE PRESSURE = SBP - DBP = 120 - 80 = 40 mmHg ║
║ STROKE WORK (LV) = SV × MAP = 70 × 100 = ~7000 mmHg·mL ║
╚══════════════════════════════════════════════════════════════╝
5.2 Ventricular Volume-Pressure Loop — Explained
LV Pressure (mmHg)
120 ──────────────────D────────C
/| |
/ | |
/ | | C = Aortic valve opens
/ | | (LV pressure > 80 mmHg)
80 ────────────── | |
| | D = Peak systolic pressure (120 mmHg)
| | Aortic valve closes when LV < Ao
| |
5 ──A───────────────B | A = Start of diastole (mitral opens)
| | | B = End of diastole / start of
| | | isovolumetric contraction
0 | | |
└───────────────┴────────┴─────
50 120 LV Volume (mL)
ESV EDV
A→B = Diastolic filling (mitral open; pressure barely rises as LV fills)
B→C = Isovolumetric CONTRACTION (all valves closed; pressure ↑, volume same)
C→D = Ejection phase (aortic valve open; volume ↓ as blood leaves)
D→A = Isovolumetric RELAXATION (all valves closed; pressure ↓, volume same)
AREA INSIDE THE LOOP = STROKE WORK of the LV
PRELOAD = filling pressure (left atrial pressure/EDV)
AFTERLOAD = resistance against which LV ejects (aortic pressure/TPR)
5.3 Afterload vs. Preload
PRELOAD AFTERLOAD
= Stretch of ventricle at END = Resistance the LV must overcome
of diastole (EDV) to eject blood
= Corresponds to left atrial = Corresponds to systemic BP /
pressure / ventricular filling total peripheral resistance (TPR)
= ↑ Preload → ↑ SV (Frank-Starling) = ↑ Afterload → ↓ SV initially
(but Frank-Starling compensates
up to a point)
5.4 Work Forms — Two Types
TOTAL CARDIAC WORK OUTPUT:
1. VOLUME-PRESSURE WORK (External work) — 99% of total
= Moving blood from low-pressure veins to high-pressure arteries
= SV × Mean Arterial Pressure
2. KINETIC ENERGY WORK — only 1% of total (usually)
= Accelerating blood to ejection velocity
= ½ × mass × velocity²
BECOMES IMPORTANT in AORTIC STENOSIS (>50% of work may be kinetic)
(Blood forced through narrow valve at high velocity)
LV does 6× MORE WORK than RV (because systemic pressure >> pulmonary)
╔══ UNIT 6: REGULATION OF HEART PUMPING ══╗
6.1 Frank-Starling Law — The Most Important Regulation
DIAGRAM — Ventricular Function Curves (Guyton & Hall, Fig. 9.12)
Fig. 9.12 — As filling pressure (atrial pressure) rises, stroke work increases — demonstrating the Frank-Starling law. LV generates far more stroke work than RV at any given filling pressure. [Guyton & Hall, p. 132]
FRANK-STARLING LAW — "The more you fill it, the harder it pumps"
FLOWCHART:
↑ Venous return (more blood entering heart)
↓
↑ End-Diastolic Volume (EDV)
↓
↑ STRETCH of ventricular muscle fibers
↓
Actin + myosin filaments reach MORE OPTIMAL OVERLAP
(more cross-bridges can form)
↓
↑ Force of contraction per beat
↓
↑ Stroke Volume
↓
↑ Cardiac Output
↓
CO = Venous Return (equilibrium maintained automatically)
Three Mechanisms Behind Frank-Starling:
- Length-tension relationship — stretched sarcomeres have better actin-myosin overlap (up to optimal length of 2.2 μm)
- Calcium sensitivity — stretch increases myofilament sensitivity to Ca²⁺ (more force at same Ca²⁺ level)
- Bainbridge Reflex — RA stretch → ↑ HR by 10-20% (via vagus nerve) — minor contribution
🔑 EXAM PHRASING: "Within physiological limits, the heart pumps all the blood that returns to it." This is the simplest and most precise statement of Frank-Starling's law.
🏥 Clinical — Heart Failure: Failing myocardium loses the Frank-Starling response. The ventricular function curve is shifted downward and to the right — the heart can no longer increase output with increased filling. Blood backs up → pulmonary edema.
6.2 Autonomic (Nervous) Control of the Heart
DIAGRAM — Cardiac Sympathetic and Parasympathetic Nerve Supply (Guyton & Hall, Fig. 9.14)
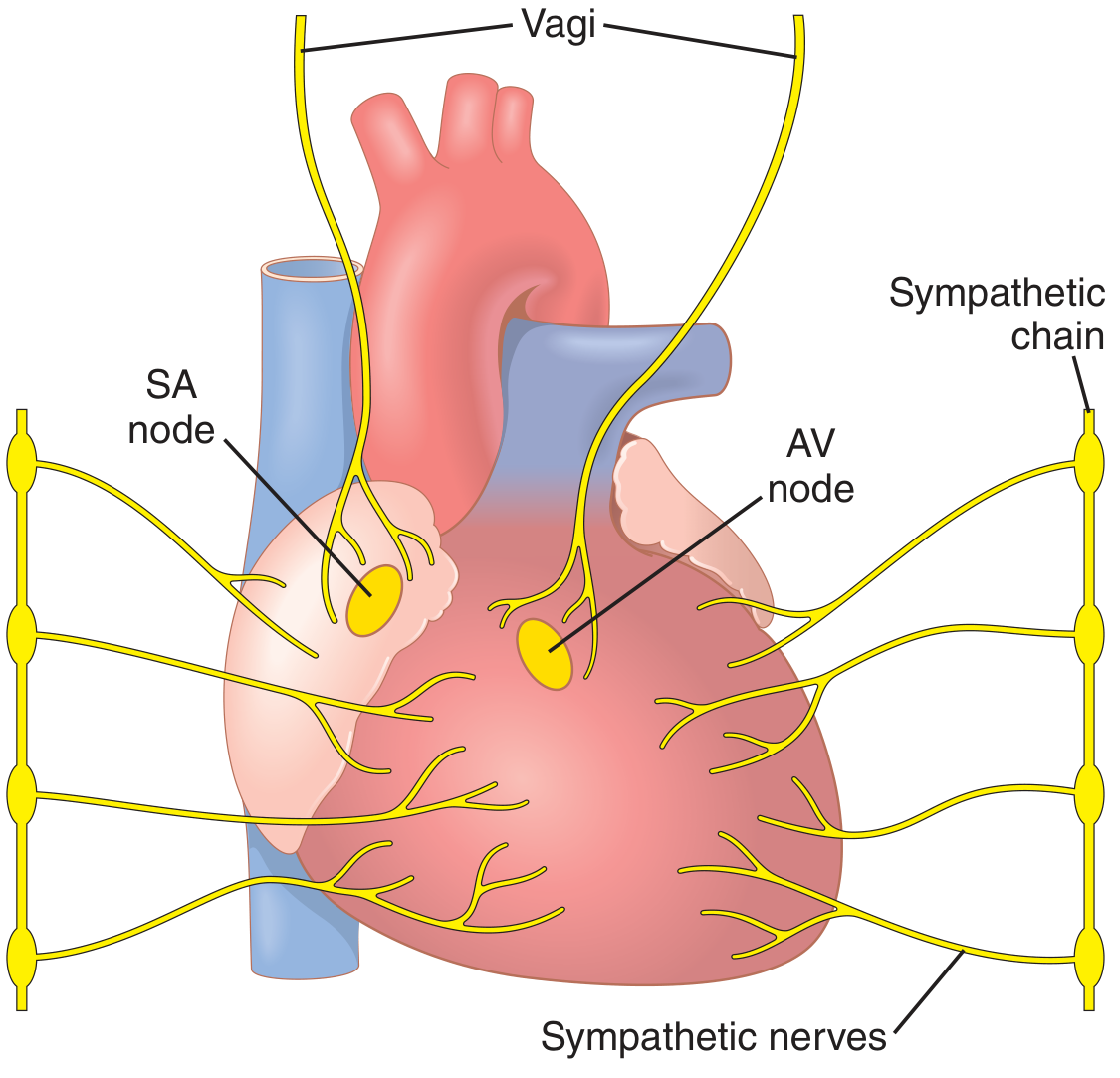
Fig. 9.14 — Sympathetic nerves (yellow branches from sympathetic chain) reach all parts of the heart including ventricles. Vagus nerves (parasympathetic) run at the top and supply mainly the SA and AV nodes and atria — with very little supply to the ventricles. [Guyton & Hall, p. 133]
DIAGRAM — Effect of Sympathetic/Parasympathetic on Cardiac Output (Guyton & Hall, Fig. 9.15)
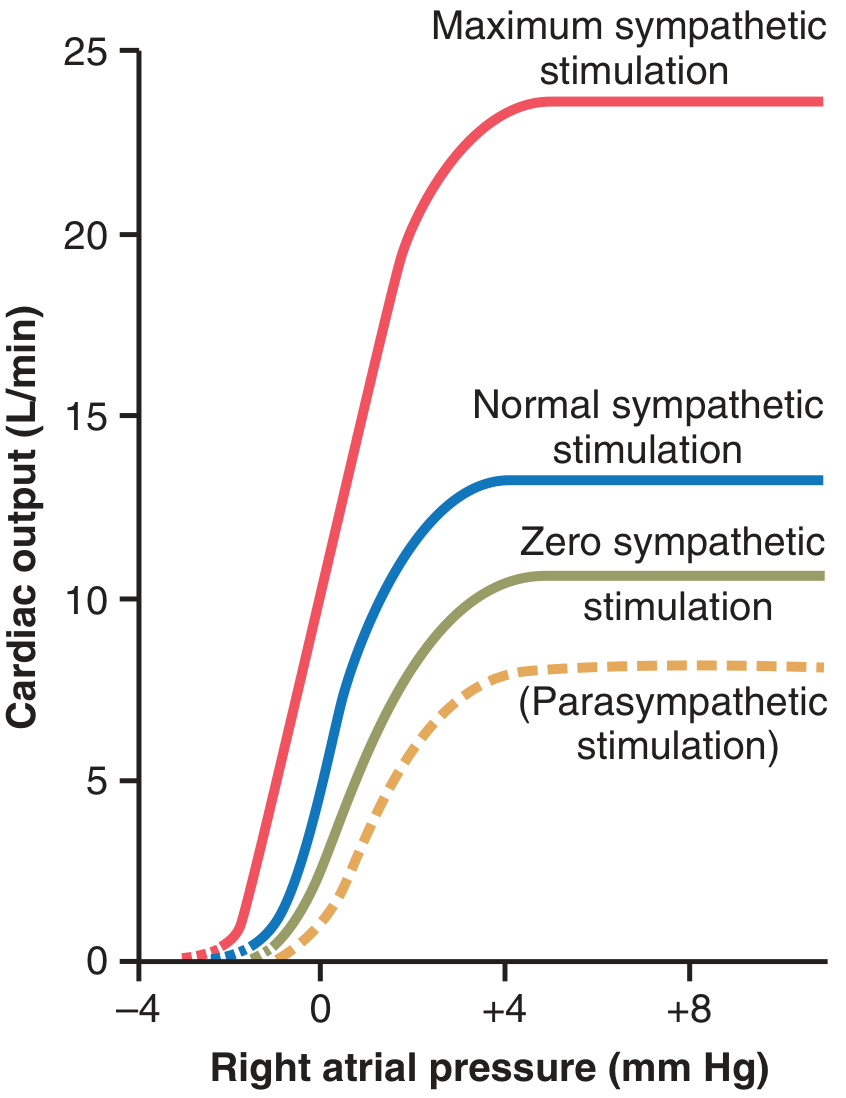
Fig. 9.15 — Maximum sympathetic stimulation (red curve) can push cardiac output to ~25 L/min. Parasympathetic stimulation (dashed orange) reduces it considerably. The x-axis is right atrial pressure — the higher it is (more filling), the more the heart can pump. [Guyton & Hall, p. 133]
SYMPATHETIC vs. PARASYMPATHETIC CARDIAC EFFECTS:
SYMPATHETIC:
Neurotransmitter: NOREPINEPHRINE (+ adrenal epinephrine in blood)
Receptor: β₁-adrenergic receptors
Distribution: SA node, AV node, atria, AND ventricles (all chambers)
Effects:
• Chronotropy (rate): ↑ HR up to 180-200 bpm (rarely 250 bpm)
• Inotropy (contractility): ↑ force of contraction (doubles)
• Dromotropy (conduction): ↑ AV conduction speed (↓ PR interval)
• Lusitropy (relaxation): ↑ relaxation speed (↑ Ca²⁺ reuptake)
Mechanism: ↑ permeability to Na⁺ and Ca²⁺ → faster pacemaker
potential in SA node → faster HR; more Ca²⁺ in cells → stronger contraction
Net: CO can increase 2-3 fold to 25 L/min (beyond Frank-Starling alone)
Note: Normal baseline sympathetic tone maintains CO ~30% above
what would occur with ZERO sympathetic activity
PARASYMPATHETIC (VAGUS):
Neurotransmitter: ACETYLCHOLINE (ACh)
Receptor: M₂ muscarinic receptors
Distribution: SA node, AV node, ATRIA (very little to ventricles)
Effects:
• Chronotropy: ↓ HR strongly (opens K⁺ channels → hyperpolarization)
• Inotropy: ↓ contractility by ~20-30% (mainly atrial muscle)
• Dromotropy: ↓ AV conduction (↑ PR interval, can cause AV block)
Mechanism: ↑ K⁺ permeability → hyperpolarization → SA node fires slower
+ reduces Ca²⁺ entry → weaker contractions (mainly atria)
Extreme vagal stimulation: Heart can STOP for a few seconds → then
"escapes" at 20-40 bpm (ventricular escape rhythm)
Combined vagal + weak ventricle effect: pumping ↓ by >50%
🔑 EXAM DISTINCTION: Parasympathetic mainly affects ATRIA (and rate). Sympathetic affects ALL chambers (rate + force). This is because vagal fibers don't reach the ventricular muscle significantly.
6.3 Ion Effects on the Heart — Detailed
POTASSIUM (K⁺):
HYPERKALEMIA (↑ K⁺): HYPOKALEMIA (↓ K⁺):
───────────────────── ─────────────────────
Resting potential less Resting potential more
negative → closer to threshold negative → farther from
(partial depolarization) threshold
LESS amplitude of AP Spontaneous firing ↑
Slower, weaker contractions (irritability ↑)
Heart: dilated, flaccid Arrhythmias, ectopic beats
↓ Conduction through AV node Ventricular fibrillation
K⁺ 8-12 mEq/L → cardiac arrest Hypokalemia + digoxin
(death from asystole) = very dangerous combo
CALCIUM (Ca²⁺):
HYPERCALCEMIA (↑ Ca²⁺): HYPOCALCEMIA (↓ Ca²⁺):
──────────────────────── ────────────────────────
↑ Contractility ↓ Contractility
Shortened AP plateau Prolonged QT interval
Spastic, over-forceful Weak contractions
contraction Can cause tetany (muscles)
"Calcium rigor" at very ↓ Ca²⁺ rarely causes
high levels (rare clinically) clinical cardiac problems
(Ca²⁺ tightly regulated)
6.4 Contractility (Inotropy) vs. Preload — Key Distinction
PRELOAD (Frank-Starling) CONTRACTILITY (Inotropy)
================================ ================================
Works by STRETCH mechanism Works by changing Ca²⁺ handling
Ventricular function curve Ventricular function curve
MOVES ALONG the same curve SHIFTS TO A DIFFERENT CURVE
↑ Preload → slides up same curve ↑ Contractility → new HIGHER curve
↓ Preload → slides down same curve ↓ Contractility → new LOWER curve
Examples of ↑ Contractility: Examples of ↓ Contractility:
• Sympathetic stimulation • Heart failure (MI, cardiomyopathy)
• Digoxin (↑ intracellular Ca²⁺) • β-blockers
• Exercise • Acidosis, hypoxia
• Hyperthyroidism • Excess K⁺
╔══ UNIT 7: RHYTHMICAL EXCITATION OF THE HEART ══╗
7.1 Conduction System — Full Diagram
DIAGRAM — The Conduction System of the Heart (Guyton & Hall, Fig. 10.1)
Fig. 10.1 — The entire conduction system in gold/yellow. Note: Bachmann's bundle runs to the left atrium. The AV bundle (Bundle of His) is the only electrical connection between atria and ventricles. The left bundle branch runs down the left side, the right bundle branch to the right ventricle, both ending in Purkinje networks on the ventricular endocardium. [Guyton & Hall, p. 136]
7.2 Every Component — Location, Size, Rate, Significance
╔══════════════════════════════════════════════════════════════════╗
║ 1. SA NODE (SINOATRIAL NODE) — "The Pacemaker" ║
╠══════════════════════════════════════════════════════════════════╣
║ Location: Superior posterolateral wall of RIGHT ATRIUM ║
║ (just below & lateral to SVC opening) ║
║ Size: 3 mm wide × 15 mm long × 1 mm thick (tiny!) ║
║ Fiber Ø: 3-5 μm (vs 10-15 μm of surrounding atrial muscle) ║
║ Inherent rate: 60-100 bpm (normally 70-80 bpm) ║
║ Blood supply: SA nodal artery (branch of RCA in 55-60%, ║
║ LCx in 40-45%) ║
║ Why it's the pacemaker: Fastest inherent rate ║
║ Key feature: Automaticity (self-excitation via If current) ║
╚══════════════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════════════════╗
║ 2. INTERNODAL PATHWAYS ║
╠══════════════════════════════════════════════════════════════════╣
║ Three pathways from SA → AV node: ║
║ • Anterior (Bachmann's bundle) — ALSO sends branch to LEFT ║
║ atrium (interatrial bundle) for simultaneous atrial activation ║
║ • Middle (Wenckebach's tract) ║
║ • Posterior (Thorel's tract) ║
║ Speed: ~1.0-1.5 m/s ║
╚══════════════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════════════════╗
║ 3. AV NODE (ATRIOVENTRICULAR NODE) — "The Gatekeeper" ║
╠══════════════════════════════════════════════════════════════════╣
║ Location: Posterior-inferior floor of RIGHT ATRIUM, ║
║ near the opening of the coronary sinus ║
║ (between the tricuspid valve and atrial septum) ║
║ Size: 6 mm × 3 mm × 1 mm ║
║ Speed: 0.02-0.05 m/s — SLOWEST IN HEART (designed for delay) ║
║ Delay: 0.09-0.13 seconds (intentional!) ║
║ Inherent rate: 40-60 bpm (takes over if SA node fails) ║
║ FUNCTION: Provides delay so atria empty into ventricles BEFORE ║
║ ventricles contract ║
║ ║
║ ALSO: Filters rapid atrial impulses (in atrial flutter/fib) ║
║ → prevents ventricles from being driven at 300+ bpm ║
╚══════════════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════════════════╗
║ 4. BUNDLE OF HIS (AV Bundle) ║
╠══════════════════════════════════════════════════════════════════╣
║ ONLY electrical bridge between atria and ventricles ║
║ Passes through fibrous skeleton of heart ║
║ Speed: ~1.0 m/s ║
║ Location: Upper interventricular septum ║
╚══════════════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════════════════╗
║ 5. BUNDLE BRANCHES ║
╠══════════════════════════════════════════════════════════════════╣
║ RIGHT bundle branch → Right ventricle (single fascicle) ║
║ LEFT bundle branch → splits into: ║
║ • Left anterior fascicle (anterosuperior LV) ║
║ • Left posterior fascicle (inferoposterior LV) ║
║ Speed: ~2.0 m/s ║
╚══════════════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════════════════╗
║ 6. PURKINJE FIBERS — "The Expressway" ║
╠══════════════════════════════════════════════════════════════════╣
║ Fiber Ø: 70-80 μm (LARGEST in heart — explains high speed) ║
║ Speed: 1.5-4.0 m/s — FASTEST IN HEART ║
║ Inherent rate: 15-40 bpm (last-resort pacemaker) ║
║ Location: Subendocardium of both ventricles ║
║ Function: Delivers impulse to ALL ventricular muscle in 0.03 s ║
║ Why important: Synchronous contraction = maximum pumping force ║
╚══════════════════════════════════════════════════════════════════╝
7.3 SA Node Self-Excitation — Step-by-Step
STEP 1: After each AP, membrane repolarizes to -55 to -60 mV
(SA node resting potential — already less negative than ventricle)
STEP 2: "FUNNY CURRENT" (If)
Specialized Na⁺ channels (HCN channels — "hyperpolarization-
activated cyclic nucleotide-gated") open at this negative voltage
Na⁺ leaks IN → slowly makes inside less negative
STEP 3: PACEMAKER POTENTIAL / PREPOTENTIAL
Membrane potential SLOWLY DRIFTS from -60 mV toward -40 mV
(like slowly filling a bucket with water until it overflows)
This drift takes ~0.8 seconds at rest = 60-80 bpm
STEP 4: THRESHOLD REACHED at ~ -40 mV
L-type Ca²⁺ channels OPEN (NOT fast Na⁺ channels, which are
inactivated at this less-negative potential)
Ca²⁺ rushes IN → UPSTROKE of SA node AP
STEP 5: ACTION POTENTIAL FIRES AND SPREADS
Ca²⁺ channels inactivate → K⁺ channels open → REPOLARIZATION
K⁺ efflux overshoots slightly → HYPERPOLARIZATION to -60 mV
K⁺ channels close → If current restarts → REPEAT CYCLE
SYMPATHETIC control: ↑ If current rate of rise → threshold reached faster
→ SHORTER prepotential → ↑ HR
PARASYMPATHETIC control: ↑ K⁺ permeability → hyperpolarizes more →
pacemaker potential takes longer to reach threshold
→ ↓ HR
7.4 Why SA Node is the Dominant Pacemaker — Overdrive Suppression
SA node: fires at 70-80 bpm
AV node: would fire at 40-60 bpm if left alone
Purkinje: would fire at 15-40 bpm if left alone
BUT: SA node fires FASTER than anyone else
→ Each SA impulse reaches AV node BEFORE it can self-fire
→ AV node is continuously RESET by SA node impulses
→ AV node never gets to fire on its own
→ SA node SUPPRESSES all lower pacemakers = OVERDRIVE SUPPRESSION
CLINICAL CONSEQUENCE (Stokes-Adams Syndrome):
If SA node suddenly fails → AV node takes 5-20 seconds to "wake up"
(It has been overdrive-suppressed for so long it is in a suppressed state)
During this 5-20 s pause → NO ventricular beats → no blood to brain
→ SYNCOPE (fainting) after 4-5 seconds
→ If pause too long → DEATH
→ Treatment: Permanent pacemaker implantation
7.5 Ectopic Pacemakers
ECTOPIC PACEMAKER = Any pacemaker outside the SA node that takes over
CAUSES:
1. SA node diseased/damaged → lower pacemaker takes over (escape rhythm)
2. A lower center becomes abnormally FAST (faster than SA node)
→ takes over (ectopic tachycardia)
3. SA impulse blocked (can't reach AV node) → AV node escapes
TYPES:
• Junctional (AV nodal) rhythm: 40-60 bpm — usually tolerated
• Idioventricular rhythm: 15-40 bpm — patient is very sick
• Ectopic atrial tachycardia: >100 bpm from atrial focus
EFFECT: Abnormal SEQUENCE of ventricular contraction
(Purkinje system not activated first → muscle contracts from outside in)
→ 20-30% REDUCTION in pumping effectiveness
7.6 Conduction Velocities — Final Table
STRUCTURE VELOCITY FUNCTIONAL SIGNIFICANCE
──────────────────────────────────────────────────────────────────────
SA node fibers 0.05 m/s Very slow; pacemaker function
Atrial muscle 1.0 m/s Normal atrial spread
Bachmann's bundle 1.0-1.5 m/s Synchronizes both atria
AV node 0.02-0.05 m/s ← SLOWEST; creates 0.09-0.13 s delay
Bundle of His 1.0 m/s Bridges atria-ventricles
Bundle branches 2.0 m/s Rapid ventricular distribution
Purkinje fibers 1.5-4.0 m/s ← FASTEST; synchronizes ALL ventricle
Ventricular muscle 0.3-0.5 m/s Final spread endocardium→epicardium
🔑 MNEMONIC: "SA-A-AV-HIS-PUR-V" for the conduction pathway, and remember: AV node = SLOW (gatekeeper), Purkinje = FAST (expressway).
╔══ UNIT 8: CARDIAC OUTPUT, VENOUS RETURN & REGULATION ══╗
8.1 Normal Values and Formulas
CARDIAC OUTPUT REFERENCE VALUES:
──────────────────────────────────────────────────────────────────
Resting CO (adult male) 5.6 L/min
Resting CO (adult female) 4.9 L/min (15% less)
Standard quoted average 5 L/min
Cardiac Index 3 L/min/m² BSA
Maximum CO (untrained) ~15-20 L/min
Maximum CO (trained athlete) ~25-35 L/min
CO at which heart becomes limiting ~13 L/min (2.5× resting)
8.2 Hypereffective vs. Hypoeffective Heart
DIAGRAM — Cardiac Output Curves for Normal, Hypereffective, and Hypoeffective Hearts (Guyton & Hall, Fig. 20.5)
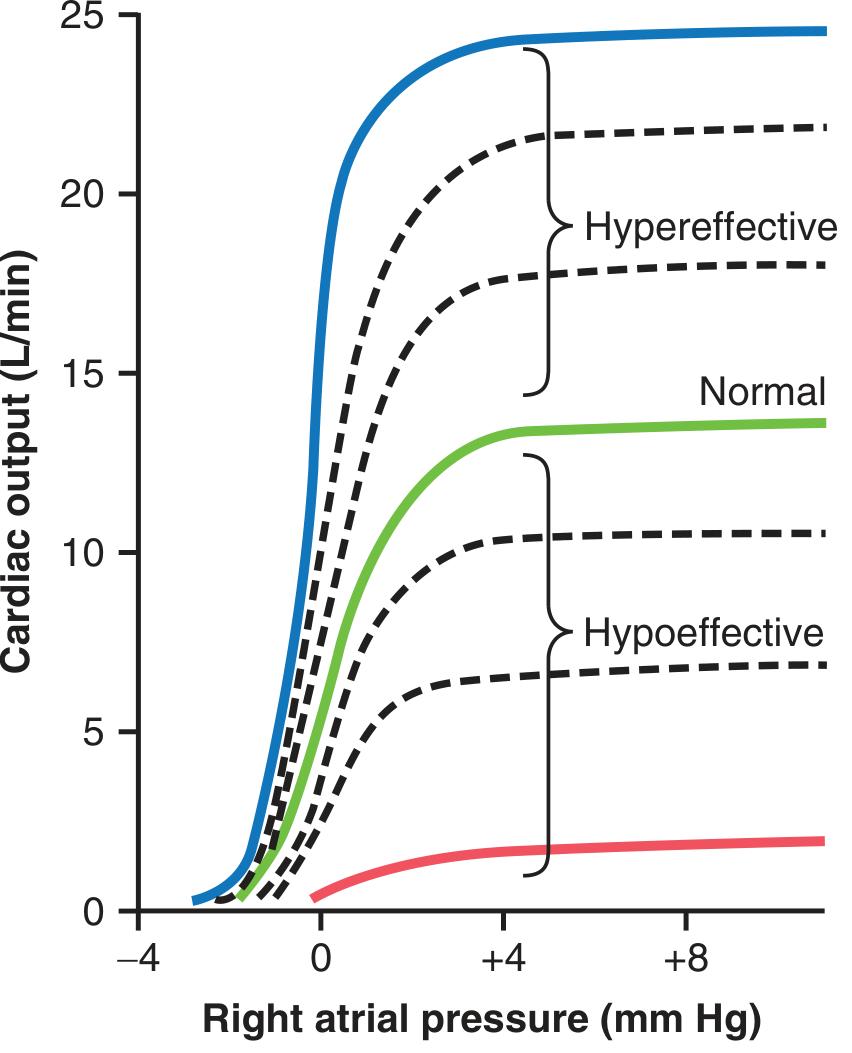
Fig. 20.5 — Cardiac output curves. The plateau level of the NORMAL heart (green) is ~13 L/min = 2.5× resting CO. Maximum sympathetic stimulation pushes the plateau to ~25 L/min. Severe heart failure (bottom red line) plateaus at only ~2 L/min — life-threatening. [Guyton & Hall, p. 253]
HYPEREFFECTIVE HEART (curve shifts UP and LEFT):
Causes:
• Sympathetic stimulation (maximum → 25 L/min plateau)
• Athletic training → cardiac hypertrophy
• Thyrotoxicosis (↑ thyroid hormone)
• Bradycardia (more filling time → ↑ SV)
HYPOEFFECTIVE HEART (curve shifts DOWN and RIGHT):
Causes:
• Myocardial infarction (heart attack — muscle dies)
• Heart failure (dilated cardiomyopathy)
• Myocarditis (viral/inflammatory)
• Valvular disease (stenosis or regurgitation)
• Cardiac tamponade (pericardial compression)
• Vitamin B₁ (thiamine) deficiency — Beriberi heart disease
• Severe acidosis or hypoxia
• Excess potassium
8.3 Fick's Principle — Measurement of Cardiac Output
FICK'S PRINCIPLE:
CO = O₂ consumption ÷ (Arterio-venous O₂ difference)
WORKED EXAMPLE:
O₂ consumed by body at rest: 250 mL O₂/min
O₂ content of aortic blood: 200 mL O₂/L blood
O₂ content of pulmonary artery blood: 150 mL O₂/L blood
A-V difference: 200 - 150 = 50 mL O₂/L
CO = 250 ÷ 50 = 5 L/min ✓
OTHER METHODS:
• Thermodilution (most common in ICU): cold saline injected into RA,
temperature change measured in PA → CO calculated
• Echocardiography (Doppler): measures aortic blood velocity
8.4 Venous Return — Why It Controls Cardiac Output
COMMON MISCONCEPTION: "The heart determines how much it pumps"
REALITY: Under resting conditions, VENOUS RETURN controls CO
REASON:
The heart's intrinsic pumping capacity far exceeds what it normally pumps.
Normal heart can pump 13 L/min at resting atrial pressures.
It only pumps 5 L/min because only 5 L/min returns from the body.
VENOUS RETURN IS DETERMINED BY:
1. Tissue metabolic activity → local vasodilation → ↑ flow → ↑ VR
2. Blood volume (dehydration → ↓ VR; IV fluids → ↑ VR)
3. Body position (lying down → ↑ VR; standing → ↓ VR temporarily)
4. Muscle pump (exercise → ↑ VR)
5. Respiratory pump (breathing in → ↓ intrathoracic pressure → ↑ VR)
6. Venomotor tone (sympathetic venoconstriction → ↑ VR)
MEAN SYSTEMIC FILLING PRESSURE (MSFP):
The pressure that drives blood back to the heart from the peripheral
circulation. Normal = ~7 mmHg. ↑ Blood volume → ↑ MSFP → ↑ VR.
╔══ UNIT 9: ELECTROCARDIOGRAPHY (ECG) ══╗
9.1 The Basis of the ECG
HOW THE ECG WORKS:
HEART DEPOLARIZES
↓
Electrical currents spread through body
(like current spreading through a tank of saltwater)
↓
Electrodes on SKIN surface detect tiny voltage differences
(measured in millivolts — very small!)
↓
ECG machine AMPLIFIES the signal (~1000×)
↓
Records on paper (speed: 25 mm/s)
↓
PAPER CALIBRATION:
Horizontal: 1 small box = 0.04 s; 1 large box = 0.2 s
Vertical: 1 large box = 1 mV (10 small boxes = 1 mV)
9.2 The Normal ECG — Complete Waveform
NORMAL ECG WAVEFORM:
mV
+1.0 ─ R
│ / \
+0.5 ─ / \
│ P / \ T
0 ─ / \ / ST \ ___/ \___
│ / \ / segment \ / \
-0.5 ─ / \/ \/
│ Q S
─────┼──────────────────────────────────── Time
│← PR →│←─── QRS ───→│←─ ST ─→│← T →│
│0.12-0.20│ 0.06-0.10 │Isoel. │0.16 │
│ s│ s │ │ s│
IMPORTANT DURATIONS:
• P wave: <0.12 s; amplitude <0.25 mV
• PR interval: 0.12–0.20 s (0.20 is upper limit of normal)
• QRS complex: 0.06–0.10 s (>0.12 s = bundle branch block)
• QT interval: 0.35–0.44 s (corrected for HR)
• PR segment: isoelectric (between end of P and start of QRS)
• ST segment: isoelectric (deviation = ischemia, infarction, pericarditis)
9.3 Each Wave — What It Means Electrically AND Mechanically
P WAVE
Electrical: Atrial DEPOLARIZATION spreading from SA node outward
Mechanical: Atrial contraction begins just AFTER the P wave
Clinical: Absent P waves = atrial fibrillation or SA node block
Peaked P waves >0.25 mV = right atrial hypertrophy
Notched P waves = left atrial hypertrophy ("P mitrale")
PR INTERVAL (0.12-0.20 s)
Electrical: Time from start of atrial depolarization to start of
ventricular depolarization
INCLUDES: Atrial activation + AV nodal delay + His bundle activation
Mechanical: Time between atrial contraction and ventricular contraction
Clinical: >0.20 s = AV conduction delay (1st degree AV block)
Very short (<0.12 s) = pre-excitation (WPW syndrome)
QRS COMPLEX (0.06-0.10 s)
Electrical: Ventricular DEPOLARIZATION
Q wave = Initial septal depolarization (left → right)
R wave = Main ventricular depolarization (downward, apex)
S wave = Final basal depolarization
Mechanical: Ventricular systole begins just AFTER QRS
Clinical: Wide QRS >0.12 s = bundle branch block or ventricular rhythm
Tall R waves = ventricular hypertrophy
Deep Q waves = old myocardial infarction
ST SEGMENT
Electrical: All ventricular cells are FULLY DEPOLARIZED (at plateau)
No difference in potential → isoelectric
Mechanical: Active ventricular ejection
Clinical: ST elevation = acute MI (STEMI), pericarditis, Prinzmetal angina
ST depression = ischemia, NSTEMI, digoxin effect
T WAVE
Electrical: Ventricular REPOLARIZATION (Phase 3)
Direction: Same direction as QRS (because repolarization goes
epicardium → endocardium, i.e., reverse of depolarization)
Mechanical: Ventricular muscle begins to relax
Clinical: T wave inversion = ischemia, ventricular hypertrophy, PE
Peaked tall T waves = hyperkalemia ("tented T waves")
Flat/inverted T waves = hypokalemia
QT INTERVAL
Total duration of ventricular electrical activity
MUST BE CORRECTED for heart rate (QTc = QT ÷ √RR interval)
Normal QTc: men <0.44 s; women <0.46 s
Long QT → risk of Torsades de Pointes (dangerous arrhythmia)
Causes of long QT: Hypokalemia, hypocalcemia, drugs (quinidine,
amiodarone, erythromycin, antihistamines), congenital long QT syndrome
9.4 Why There Is No Visible Atrial Repolarization Wave
QUESTION: Atria repolarize — why don't we see it on ECG?
ANSWER:
Atrial repolarization occurs during the PR segment and beginning of QRS.
But the QRS complex has a voltage ~10× larger than atrial signals.
The QRS completely OVERWHELMS and BURIES the atrial repolarization wave.
Therefore: No "atrial T wave" is visible on standard ECG.
╔══ UNIT 10: BLOOD PRESSURE AND ITS REGULATION ══╗
10.1 Blood Pressure Fundamentals
MAP = CO × TPR
WHERE:
MAP = Mean Arterial Pressure (~93 mmHg)
CO = Cardiac Output (~5 L/min)
TPR = Total Peripheral Resistance (resistance of all arterioles combined)
ANY factor that ↑ CO or ↑ TPR = ↑ Blood Pressure
NORMAL VALUES:
Systolic BP: 120 mmHg
Diastolic BP: 80 mmHg
Pulse pressure: 40 mmHg (120-80)
MAP: 93 mmHg (80 + 13.3)
HYPERTENSION DEFINED: ≥130/80 mmHg (AHA 2017 criteria)
HYPOTENSION: SBP <90 or MAP <65 mmHg
10.2 Layers of Blood Pressure Regulation — A 3-Tier System
╔═══════════════════════════════════════════════════════════════╗
║ TIER 1: SECONDS-TO-MINUTES (Neural reflexes) ║
║ Baroreceptors, chemoreceptors, CNS ischemic response ║
╠═══════════════════════════════════════════════════════════════╣
║ TIER 2: MINUTES-TO-HOURS (Humoral/fluid shifts) ║
║ RAAS, ADH/vasopressin, capillary fluid shift ║
╠═══════════════════════════════════════════════════════════════╣
║ TIER 3: HOURS-TO-DAYS (Renal-body fluid mechanism) ║
║ Kidneys controlling blood volume = MOST POWERFUL ║
║ long-term controller ║
╚═══════════════════════════════════════════════════════════════╝
10.3 Baroreceptor Reflex — Full Detail
BARORECEPTOR REFLEX (Most important SHORT-TERM regulator):
ANATOMY:
• Baroreceptors = stretch-sensitive mechanoreceptors
• Locations:
- Carotid sinus (at bifurcation of common carotid artery)
→ Nerve: Hering's nerve → CN IX (Glossopharyngeal)
- Aortic arch
→ Nerve: Aortic nerve → CN X (Vagus)
• Both afferents → Nucleus Tractus Solitarius (NTS) in medulla
NTS → Cardiovascular control center (medulla oblongata)
WHEN BP RISES:
BP ↑ → Wall stretch ↑ → Baroreceptors fire MORE
↓
Signals to NTS → medulla
↓
┌─────────────────┬──────────────────┐
▼ ▼ ▼
↓ Sympathetic ↑ Vagal (parasym.) Vasodilation
to heart to heart of arterioles
↓ HR, ↓ CO ↓ HR, ↓ contractility ↓ TPR
└─────────────────┴──────────────────┘
↓
BP FALLS BACK TO NORMAL
WHEN BP FALLS:
BP ↓ → Wall stretch ↓ → Baroreceptors fire LESS
↓
↑ Sympathetic, ↓ Vagal
↑ HR, ↑ CO, vasoconstriction
↓
BP RISES BACK TO NORMAL
LIMITATION: Baroreceptors ADAPT within 1-2 days to chronic hypertension
→ Cannot correct chronically high or low BP
→ Only effective for ACUTE pressure changes
10.4 RAAS — Complete Flowchart
DIAGRAM — RAAS Effect on BP after Hemorrhage (Guyton & Hall, Fig. 19.10)
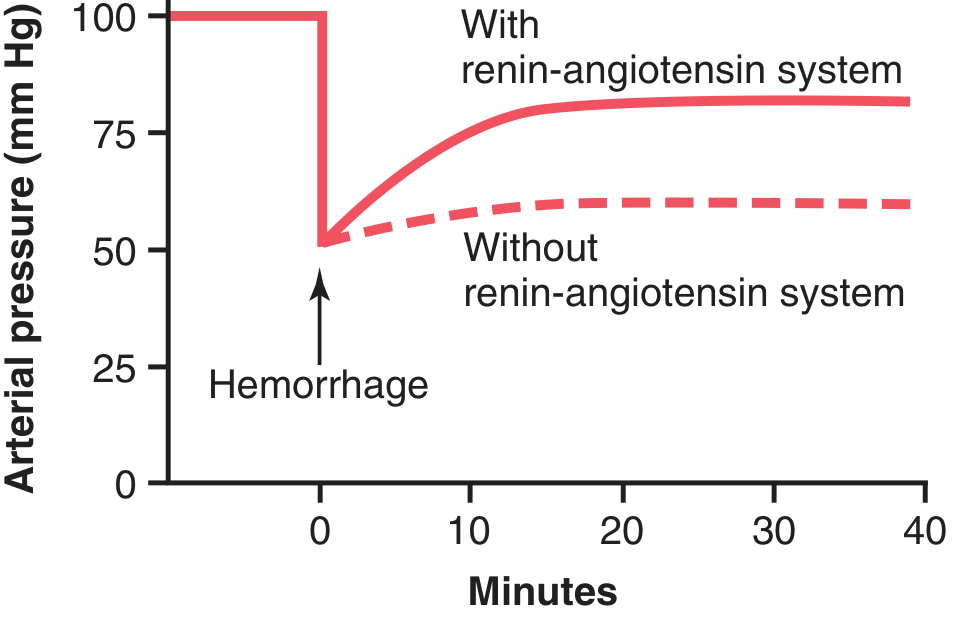
Fig. 19.10 — After severe hemorrhage dropping BP to 50 mmHg: with RAAS intact (solid line), BP recovers to ~83 mmHg. Without RAAS (dashed line), only to ~60 mmHg. The RAAS takes ~20 minutes to become fully active. This demonstrates its life-saving role in hemorrhage and shock. [Guyton & Hall, p. 242]
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM (RAAS):
TRIGGERS for RENIN release (from JG cells of kidney):
1. ↓ Renal perfusion pressure (JG cell baroreceptors detect stretch)
2. ↓ NaCl delivery to macula densa (tubuloglomerular feedback)
3. ↑ Sympathetic activity (β₁ receptors on JG cells)
RENIN (enzyme, from kidney JG cells)
↓ cleaves
ANGIOTENSINOGEN (protein from LIVER)
↓
ANGIOTENSIN I (decapeptide — inactive)
↓ ACE (Angiotensin Converting Enzyme — in LUNG endothelium)
ANGIOTENSIN II (octapeptide — ACTIVE)
↓
┌──────┬──────────────┬──────────────┬───────────────┐
▼ ▼ ▼ ▼ ▼
Vasocon- Adrenal Posterior Direct renal Sympathetic
striction cortex pituitary tubule effect activation
↑ TPR → Aldosterone → ADH (AVP) Na⁺+H₂O ↑ NE release
↑ BP release release retention ↑ HR, ↑ BP
↓ ↓
Na⁺+H₂O Water retention
reabsorption ↑ Blood volume
↑ Blood volume ↑ CO
└─────────────┘
↓
↑ Blood Pressure
(over hours-to-days)
CLINICAL USE:
ACE inhibitors (e.g., ramipril) → block Ang I → Ang II conversion
→ ↓ vasoconstriction, ↓ aldosterone
→ Used in hypertension, heart failure, DM nephropathy
ARBs (e.g., losartan) → block Ang II receptors directly
Spironolactone → blocks aldosterone receptors → ↓ Na⁺ retention
10.5 Other Long-Term BP Regulators
ADH (ANTIDIURETIC HORMONE / VASOPRESSIN):
Released from posterior pituitary
Triggers: ↓ BP, ↑ plasma osmolality, Ang II, pain, stress
Actions: Water retention (V2 receptors in kidney collecting ducts)
Vasoconstriction (V1 receptors on arterioles)
Net: ↑ blood volume + ↑ TPR → ↑ BP
ATRIAL NATRIURETIC PEPTIDE (ANP):
Released from atrial walls when STRETCHED (by ↑ blood volume)
Actions: Opposite of RAAS — ↓ Na⁺ retention, vasodilation, ↓ renin
Net: ↓ blood volume → ↓ BP
Clinical: ANP is a biomarker for heart failure (BNP = Brain NP from ventricles)
╔══ UNIT 11: MICROCIRCULATION & CAPILLARY DYNAMICS ══╗
11.1 Microcirculation Structure
ARTERIOLE (10-15 μm internal Ø)
Main resistance vessel
Smooth muscle wall — regulated by:
• Autonomic nerves (sympathetic → constrict)
• Local metabolites (O₂↓, CO₂↑ → dilate)
• Hormones (Ang II → constrict; NO → dilate)
↓
METARTERIOLE (10-35 μm)
Connects arterioles to capillary bed
Smooth muscle present intermittently
↓
PRECAPILLARY SPHINCTER (smooth muscle ring)
Controlled ONLY by local tissue metabolites (NOT nerves)
Opens when O₂ low; closes when O₂ replenished
Causes VASOMOTION (rhythmic opening/closing every 10-30 s)
↓
TRUE CAPILLARIES (5-9 μm Ø)
Wall = single endothelial cell + basement membrane
RBCs pass through in SINGLE FILE (sometimes deform to fit!)
Exchange of: O₂, CO₂, glucose, amino acids, hormones, waste
Can only be seen with microscope
↓
VENULES → VEINS
Vessel Types by Function:
- Resistance vessels = Arterioles (control flow)
- Exchange vessels = Capillaries (gas/nutrient exchange)
- Capacitance/reservoir vessels = Veins (contain 64% of blood)
- Windkessel vessels = Large arteries (buffer pressure pulses)
11.2 Starling Forces — Detailed Analysis
4 FORCES ACTING AT THE CAPILLARY WALL:
FORCE DIRECTION NORMAL VALUE
─────────────────────────────────────────────────────────────
Capillary hydrostatic P (Pc) OUTWARD (filter) Arterial end: 35 mmHg
Venous end: 15 mmHg
Interstitial hydrostatic P INWARD (absorb) -3 mmHg
(Pi — slightly negative!) (like a suction)
Plasma colloid osmotic P INWARD (absorb) 28 mmHg
(πc = oncotic P — albumin) (constant)
Interstitial colloid osmotic OUTWARD (filter) 8 mmHg
pressure (πi)
STARLING EQUATION:
Net Filtration = Kf [(Pc + πi) - (πc + Pi)]
= Kf [(Pc + 8) - (28 + (-3))]
= Kf [(Pc + 8) - (25)]
AT ARTERIAL END:
= Kf [(35 + 8) - (25)] = Kf [43 - 25] = +18 → FILTRATION
(fluid leaves capillary → delivers O₂, nutrients to tissue)
AT VENOUS END:
= Kf [(15 + 8) - (25)] = Kf [23 - 25] = -2 → ABSORPTION
(fluid returns to capillary → removes CO₂, waste)
NET RESULT:
~90% of filtered fluid is reabsorbed at venous end
~10% excess fluid → LYMPHATIC SYSTEM → eventually back to blood
Normal lymph flow: ~2-4 L/day
11.3 Edema — 4 Causes + Clinical Examples
╔══════════════════════════════════════════════════════════════════╗
║ CAUSE MECHANISM CLINICAL EXAMPLE ║
╠══════════════════════════════════════════════════════════════════╣
║ ↑ Capillary ↑ Filtration out Right heart failure ║
║ hydrostatic P exceeds absorption → leg edema ║
║ DVT → limb edema ║
╠══════════════════════════════════════════════════════════════════╣
║ ↓ Plasma protein ↓ Absorption Liver failure ║
║ (↓ albumin → ↓ πc) (less suction) (↓ albumin synthesis) ║
║ Nephrotic syndrome ║
║ (albumin lost in urine)║
║ Malnutrition ║
╠══════════════════════════════════════════════════════════════════╣
║ Lymphatic Protein accumulates Filariasis (elephantia)║
║ obstruction in interstitium Cancer surgery (lymph ║
║ → ↑ πi → more node removal) ║
║ filtration Milroy's disease ║
╠══════════════════════════════════════════════════════════════════╣
║ ↑ Capillary Proteins leak out Allergy/anaphylaxis ║
║ permeability → ↑ πi → more (histamine, bradykinin)║
║ filtration Burns, sepsis, ║
║ inflammation ║
╚══════════════════════════════════════════════════════════════════╝
PITTING vs. NON-PITTING EDEMA:
Pitting = protein-poor fluid (cardiac, renal, nutritional)
Non-pitting = protein-rich fluid (lymphedema, myxedema in hypothyroidism)
╔══ UNIT 12: CARDIAC OUTPUT IN SPECIAL STATES ══╗
12.1 Exercise — Complete Physiology
EXERCISE PHYSIOLOGY — COMPLETE CHAIN:
EXERCISING MUSCLE:
↑ O₂ consumption + ↑ CO₂ + ↑ H⁺ (lactic acid) + ↑ K⁺ + ↑ adenosine
All of these cause LOCAL VASODILATION in working muscles
↓
↓ Local resistance → ↑ blood flow to muscles → ↑ venous return
↓
THREE PUMPS INCREASE VENOUS RETURN:
1. MUSCLE PUMP: contracting muscles compress veins → blood squeezed toward heart
2. RESPIRATORY PUMP: deeper breathing → ↓ intrathoracic pressure → chest acts as bellows
3. VENOCONSTRICTION: sympathetic → veins constrict → ↑ venous pressure → ↑ VR
↓
↑ EDV → Frank-Starling → ↑ SV
↓
SIMULTANEOUSLY — CNS and Sympathetic:
• ↑ HR (up to 180-200 bpm max)
• ↑ Contractility (sympathetic → ↑ inotropy)
• ↓ Peripheral resistance (skeletal muscle arterioles dilate > sympathetic constriction)
↓
CO RISES:
Untrained person at maximal exercise: 15-20 L/min
Trained endurance athlete at maximal: 25-35 L/min
Cardiovascular Response to Exercise — Summary Table:
| Parameter | Rest | Moderate Exercise | Max Exercise |
|---|---|---|---|
| CO | 5 L/min | 10-12 L/min | 20-35 L/min |
| HR | 72 bpm | 100-140 bpm | 180-200 bpm |
| SV | 70 mL | 100-120 mL | ~120-200 mL (athletes) |
| SBP | 120 mmHg | 150-170 mmHg | 190-220 mmHg |
| DBP | 80 mmHg | 70-80 mmHg | 70-80 mmHg (stays same!) |
| Skeletal muscle flow | 1-1.2 L/min | 8-10 L/min | 15-20 L/min |
Key point: DBP does NOT rise significantly during exercise because skeletal muscle vasodilation lowers TPR, even while CO increases. SBP rises because CO increases.
12.2 Pregnancy
CARDIOVASCULAR CHANGES IN PREGNANCY:
BLOOD VOLUME: ↑ 30-50% by 32 weeks
(Mechanism: ↑ estrogen + progesterone → ↑ RAAS → ↑ aldosterone
→ Na⁺ + water retention → ↑ plasma volume by ~50%)
RBC mass also increases, but less than plasma → DILUTIONAL ANEMIA
CARDIAC OUTPUT: ↑ 40-50% by 32 weeks (from 5 → 7 L/min)
Mechanism: ↑ blood volume → ↑ venous return → Frank-Starling → ↑ SV
Also: ↑ HR by 15-20 bpm
BLOOD PRESSURE: Normal or slightly DECREASED
(↑ CO but ↓↓ TPR due to:
• Progesterone → smooth muscle relaxation → vasodilation
• New low-resistance placental circulation)
HEART CHANGES:
• Heart displaced upward and laterally (by gravid uterus)
• Apex beat displaced laterally
• Physiological systolic FLOW MURMUR (high flow across normal valves)
• Exaggerated S3 (NORMAL in pregnancy — not heart failure!)
• ECG changes: left axis deviation
AORTOCAVAL COMPRESSION (Supine Hypotension Syndrome):
Gravid uterus in late pregnancy compresses IVC in supine position
→ ↓ Venous return → ↓ CO → BP falls → dizziness/syncope
Treatment: LEFT LATERAL DECUBITUS position (tilts uterus off IVC)
12.3 Fetal Circulation — Complete with Changes at Birth
FETAL CIRCULATION:
OXYGENATED blood from placenta (PO₂ ~30-35 mmHg):
UMBILICAL VEIN → Liver
├──(small amount → hepatic sinusoids → liver metabolism)
└──(most → DUCTUS VENOSUS → bypasses liver → IVC)
↓
INFERIOR VENA CAVA → RIGHT ATRIUM
↓
┌───────────────┤
│ FORAMEN OVALE │ (70% of RA blood)
│ (right → left│
│ atrial shunt)│
└───────────────┘
↓
LEFT ATRIUM → LEFT VENTRICLE → ASCENDING AORTA
(Most oxygenated blood → head, brain, heart)
↓
┌──────────────────────────────────┐
│ 30% goes RIGHT VENTRICLE │
│ → PULMONARY ARTERY │
│ → small amount to lungs │
│ → DUCTUS ARTERIOSUS │
│ (PA → descending aorta) │
└──────────────────────────────────┘
↓
DESCENDING AORTA → Body tissues (lower body)
↓
2 UMBILICAL ARTERIES → PLACENTA (for gas exchange)
Three Fetal Shunts:
SHUNT CONNECTS FUNCTION
──────────────────────────────────────────────────────────────────
Foramen ovale RA → LA Bypasses pulmonary circulation
Allows best blood to brain
Ductus arteriosus Pulmonary artery → Bypasses lungs (collapsed in utero)
Descending aorta Lungs only need 5-10% of CO
Ductus venosus Umbilical vein → Bypasses liver
IVC Allows rapid umbilical blood to
reach heart directly
Changes at Birth — Step by Step:
BABY TAKES FIRST BREATH:
↓
Lungs EXPAND → Pulmonary vascular resistance ↓ dramatically
↓
↑ Blood flows to lungs → ↑ blood returns to LEFT atrium
↓
LEFT atrial pressure EXCEEDS right atrial pressure
↓
FORAMEN OVALE CLOSES functionally within hours
(Anatomical closure: fibrous fusion over weeks-months)
↓
↑ Arterial O₂ tension (pO₂ rises from 30 → 100 mmHg)
↓
DUCTUS ARTERIOSUS CONSTRICTS (prostaglandins inhibited by ↑ O₂)
Functional closure: 10-15 hours
Anatomical closure (→ ligamentum arteriosum): 3-4 weeks
↓
DUCTUS VENOSUS closes when umbilical cord cut (no more flow)
→ becomes ligamentum venosum
↓
Adult circulation established
Adult Remnants of Fetal Structures:
| Fetal Structure | Adult Remnant | Clinical Note |
|---|---|---|
| Foramen ovale | Fossa ovalis | Patent foramen ovale in 25% of adults! |
| Ductus arteriosus | Ligamentum arteriosum | Patent DA → loud machinery murmur |
| Ductus venosus | Ligamentum venosum | - |
| Umbilical vein | Ligamentum teres hepatis | - |
| Umbilical arteries | Medial umbilical ligaments | - |
🏆 MASTER EXAM-PREPARATION SECTION
All Key Values at a Glance
╔══════════════════════════════════════════════════════════════════╗
║ CARDIOVASCULAR NUMBERS — MEMORIZE THESE ║
╠══════════════════╦═══════════════════╦═════════════════════════╣
║ CARDIAC FUNCTION ║ VALUES ║ NOTES ║
╠══════════════════╬═══════════════════╬═════════════════════════╣
║ CO (resting) ║ 5 L/min ║ Male 5.6, Female 4.9 ║
║ CO (max exercise)║ 25-35 L/min ║ Athletes highest ║
║ CO (max w/ symp) ║ ~25 L/min ║ From Guyton Fig 9.15 ║
║ Cardiac Index ║ 3 L/min/m² ║ = CO/BSA ║
║ Heart Rate ║ 72 bpm ║ (60-100 normal) ║
║ Stroke Volume ║ 70 mL ║ = EDV - ESV ║
║ EDV ║ 120-130 mL ║ End-Diastolic Volume ║
║ ESV ║ 50 mL ║ End-Systolic Volume ║
║ Ejection Fract. ║ ~58% ║ Normal >55% ║
╠══════════════════╬═══════════════════╬═════════════════════════╣
║ PRESSURES ║ ║ ║
║ Aortic BP ║ 120/80 mmHg ║ Systolic/Diastolic ║
║ MAP ║ ~93 mmHg ║ DBP + ⅓ PP ║
║ Pulse pressure ║ 40 mmHg ║ SBP - DBP ║
║ Pulmonary art. ║ 25/8 mmHg ║ Low-pressure circuit ║
║ LV systolic peak ║ 120 mmHg ║ Same as aortic SBP ║
║ LV diastolic ║ 0-8 mmHg ║ Very low at rest ║
╠══════════════════╬═══════════════════╬═════════════════════════╣
║ CONDUCTION SYSTEM║ ║ ║
║ SA node rate ║ 60-100 bpm ║ Dominant pacemaker ║
║ AV node rate ║ 40-60 bpm ║ Secondary pacemaker ║
║ Purkinje rate ║ 15-40 bpm ║ Tertiary pacemaker ║
║ AV nodal delay ║ 0.09-0.13 s ║ At the AV node ║
║ Ventricular activ║ 0.03 s total ║ Via Purkinje ║
╠══════════════════╬═══════════════════╬═════════════════════════╣
║ ACTION POTENTIAL ║ ║ ║
║ Resting MP (vent)║ -85 to -90 mV ║ Ventricular cell ║
║ Resting MP (SA) ║ -55 to -60 mV ║ Pacemaker cell ║
║ Threshold (SA) ║ ~-40 mV ║ For L-type Ca²⁺ channels ║
║ AP amplitude ║ ~105 mV ║ -90 to +20 mV swing ║
║ AP duration (vent)║ ~250-300 ms ║ 15× longer than skeletal ║
║ ARP duration ║ ~250 ms ║ = mechanical contraction ║
╠══════════════════╬═══════════════════╬═════════════════════════╣
║ ECG INTERVALS ║ ║ ║
║ P wave ║ <0.12 s ║ Atrial depolarization ║
║ PR interval ║ 0.12-0.20 s ║ AV conduction time ║
║ QRS complex ║ 0.06-0.10 s ║ Ventricular depol. ║
║ QT interval ║ 0.35-0.44 s ║ Total ventricular elec. ║
╠══════════════════╬═══════════════════╬═════════════════════════╣
║ CAPILLARY FORCES ║ ║ ║
║ Plasma COP (πc) ║ 28 mmHg ║ Main absorption force ║
║ Cap HP art. end ║ 35 mmHg ║ Main filtration force ║
║ Cap HP ven. end ║ 15 mmHg ║ < plasma COP → absorption ║
║ Interstitial HP ║ -3 mmHg ║ Slightly negative (suction)║
║ Interstitial COP ║ 8 mmHg ║ Tissue proteins ║
╚══════════════════╩═══════════════════╩═════════════════════════╝
Mnemonics Collection
🔑 PROPERTIES OF CARDIAC MUSCLE: "ACERRD"
Automaticity, Conductivity, Excitability, Rhythmicity, Refractoriness,
Distensibility/Contractility
🔑 HEART LAYERS (outside → in): "For Pigs, Every Patient Must Enter"
Fibrous pericardium, Parietal pericardium, Epicardium,
Pericardial space, Myocardium, Endocardium
🔑 ATRIAL PRESSURE WAVES: "acv" = "Atrial Contracts/Valve-bulges/Venous fills"
🔑 HEART SOUNDS SITES: "All Patients Take Medicine"
(going from left to right across chest, roughly):
Aortic (2nd ICS right), Pulmonary (2nd ICS left),
Tricuspid (4th ICS left sternal border), Mitral (apex)
🔑 S3 vs S4:
S3 = "Ken-tuck-y" (lub-dub-BUM) = early diastole = FAILURE (in adults)
S4 = "Ten-nes-see" (BUM-lub-dub) = late diastole = STIFF ventricle
🔑 CARDIAC CYCLE PHASES in order: "IVR - RVF - DIAS - ATRIAL - IVC - RE - SE"
Isovolumetric Relaxation, Rapid Ventricular Filling, Diastasis,
Atrial systole, Isovolumetric Contraction, Rapid Ejection, Slow Ejection
🔑 EDEMA CAUSES: "CLIP"
Capillary HP increase, Low plasma proteins, Impaired lymphatics, Permeability increase
🔑 FETAL SHUNTS: "DAD"
Ductus venosus, foramen ovAle, Ductus arteriosus
All CLOSE at birth.
🔑 PHASES OF AP: "0 is up, 2 is plateau, 3 is down, 4 is flat"
Most Likely Exam Questions — With Answer Pointers
1. "Describe the cardiac cycle with pressure and volume changes"
→ Draw/describe the Wiggers diagram. 7 phases. Pressure values at each stage.
Valve events. Heart sounds. a/c/v waves.
2. "Frank-Starling law — explain mechanism and significance"
→ Definition. Length-tension relationship. Actin-myosin overlap.
Bainbridge reflex. Ventricular function curves. Clinical failure.
3. "Properties of cardiac muscle"
→ ACERRD. Each property with mechanism. Syncytium. Intercalated discs.
Contrast with skeletal muscle.
4. "Conduction system of the heart"
→ Draw Fig 10.1 from memory. Each component with location, rate, velocity.
AV delay and why. Overdrive suppression. Escape rhythms.
5. "Baroreceptor reflex"
→ Location (carotid sinus + aortic arch). Afferents (IX, X). NTS.
Response to ↑BP and ↓BP. Limitation (adaptation). Not a long-term regulator.
6. "Action potential of cardiac muscle — compare with skeletal muscle"
→ 5 phases with ions. Plateau mechanism. ARP = cannot tetanize. Ca²⁺ role.
SA node AP differences (pacemaker potential, threshold at -40 mV, Ca²⁺ upstroke).
7. "RAAS in blood pressure regulation"
→ Complete flowchart. Triggers. Angiotensin II multiple actions.
ACE inhibitors and ARBs. Time course (~20 min to full activity).
8. "Starling forces at the capillary / Edema"
→ 4 forces. Equation. Arterial vs venous end. Lymphatics.
4 causes of edema with examples. Pitting vs non-pitting.
9. "Cardiac output and its regulation"
→ Definition, normal values, Fick's principle. CO = VR.
Frank-Starling. Autonomic control. Hypereffective/hypoeffective.
10. "Fetal circulation and changes at birth"
→ Three shunts and their functions. Draw diagram.
Mechanism of closure of each. Adult remnants.
All content referenced from Guyton and Hall Textbook of Medical Physiology, 14th Edition (Hall JE, Hall ME) — ISBN: 9780443111013. All diagrams sourced directly from this textbook, Chapters 9, 10, 11, 18, 19, 20, and 23.
This is a shared conversation. Sign in to Orris to start your own chat.