Biopsy report shows what???
Asking for Preferences
Reading File
Searching the Web
what does a biopsy report show pathology components
Finding Sources
Here is a thorough breakdown of what a biopsy report (also called a pathology report) generally shows:
What a Biopsy Report Shows
A biopsy report is a document written by a pathologist - a doctor who specializes in diagnosing disease through examination of tissue, cells, and body fluids under a microscope. Here are the key sections and what each one tells you:
1. Patient & Specimen Identification
- Your name, date of birth, and medical record number
- The date the sample was taken
- The source of the specimen - e.g., "core needle biopsy, right breast" or "punch biopsy, left forearm"
- The name of the doctor who ordered the biopsy
2. Gross Description (Macroscopic)
This is what the tissue looks like to the naked eye before it goes under the microscope:
- Size, shape, color, and texture of the tissue
- Whether it is soft, firm, rubbery, calcified, etc.
- Number of fragments or pieces
3. Microscopic Description (Histology)
The core of the report - what the tissue looks like under the microscope after being stained (usually with Hematoxylin & Eosin, or H&E):
- Cell type and architecture - are the cells normal-looking or abnormal?
- Differentiation - how closely do the cells resemble normal tissue?
- Inflammation - is there immune cell infiltration?
- Necrosis - is there dead/dying tissue present?
- Vascular or lymphatic invasion - have abnormal cells entered blood or lymph vessels?
- Margins - if tissue was surgically removed, are the edges (margins) clear of disease?
4. Diagnosis / Final Impression
The most important line in the report. The pathologist gives one of several conclusions:
| Term | Meaning |
|---|---|
| Benign | Not cancer; normal or non-harmful tissue |
| Malignant | Cancer confirmed |
| Suspicious / Atypical | Abnormal cells present, but not definitively cancer - may need repeat biopsy |
| Dysplasia | Pre-cancerous changes (cells are abnormal but have not invaded) |
| Neoplasm | An abnormal growth (can be benign or malignant) |
| In situ | Abnormal cells are present but have NOT spread beyond the original layer |
| Invasive | Cancer has spread into surrounding tissue |
| Non-diagnostic / Insufficient | Not enough tissue was obtained for a firm conclusion |
5. Special Studies (if ordered)
Some biopsies require additional testing beyond routine H&E staining:
- Immunohistochemistry (IHC) - uses antibodies to identify specific proteins on cells (e.g., ER/PR/HER2 in breast cancer, CD markers in lymphoma)
- FISH (Fluorescence In Situ Hybridization) - detects gene amplifications or rearrangements
- Molecular/Genetic Testing - looks for mutations (e.g., EGFR, KRAS, BRAF) that guide targeted therapy
- Special stains - e.g., PAS stain for fungi, Congo red for amyloid, AFB stain for tuberculosis
- Cultures - if infection is suspected
6. Cancer-Specific Information (if applicable)
If cancer is found, the report will include:
- Type - e.g., adenocarcinoma, squamous cell carcinoma, melanoma, sarcoma
- Grade - how abnormal the cells look (Grade 1 = well-differentiated/low grade; Grade 3 = poorly differentiated/high grade)
- Stage markers - tumor size, lymph node involvement (pN), metastasis (pM)
- Lymphovascular invasion - present or absent
- Perineural invasion - whether cancer has spread along nerves
- Margin status - positive (cancer at the edge) vs. negative (clean margins)
7. Pathologist's Signature and Accession Number
- Every report has a unique accession number linking it to the specimen
- Signed off by the pathologist, sometimes with a co-sign from a second pathologist for quality assurance
Key Things to Know
- A biopsy report is not the same as a final clinical diagnosis - your doctor interprets it in the context of your symptoms, imaging, and other tests.
- If something is "suspicious" or "atypical," it does not automatically mean cancer - it means more investigation is needed.
- You can (and should) ask your doctor to walk you through the report if anything is unclear. You can also request a second opinion from another pathologist, which is standard practice for complex or rare findings.
If you have a specific biopsy result or tissue type you want explained further (e.g., skin, breast, colon, prostate, kidney), feel free to share it and I can break it down in more detail.
Immunotherapy
Asking for Preferences
Finding Sources
Searching the Web
immunotherapy cancer general overview types mechanisms 2025
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a thorough general overview of cancer immunotherapy, drawn from Goodman & Gilman's Pharmacological Basis of Therapeutics, Roitt's Essential Immunology, and Sabiston's Textbook of Surgery:
Cancer Immunotherapy - General Overview
What Is It?
Immunotherapy uses the patient's own immune system to recognize and destroy cancer cells. Cancer cells express abnormal proteins (tumor-associated antigens) that should trigger an immune response - but tumors have evolved clever ways to evade this surveillance. Immunotherapy works by overcoming those evasion strategies.
Key principle: Immunotherapy works best when the tumor burden has already been reduced by surgery, radiation, or chemotherapy. The immune system cannot be expected to eliminate a large tumor mass on its own.
The 6 Main Types of Cancer Immunotherapy
1. Immune Checkpoint Inhibitors (ICIs) - Most Widely Used
Cancer cells "put the brakes" on T cells by expressing inhibitory molecules. ICIs remove those brakes.
The two main checkpoint pathways targeted are:
| Checkpoint | What It Does | How Cancer Exploits It |
|---|---|---|
| CTLA-4 | Competes with CD28 for B7 binding, dampening T-cell activation | Upregulated on T cells in the tumor environment |
| PD-1 / PD-L1 | PD-1 on T cells binds PD-L1 on tumor cells, inducing T-cell "exhaustion" | Tumor cells overexpress PD-L1 to hide from T cells |
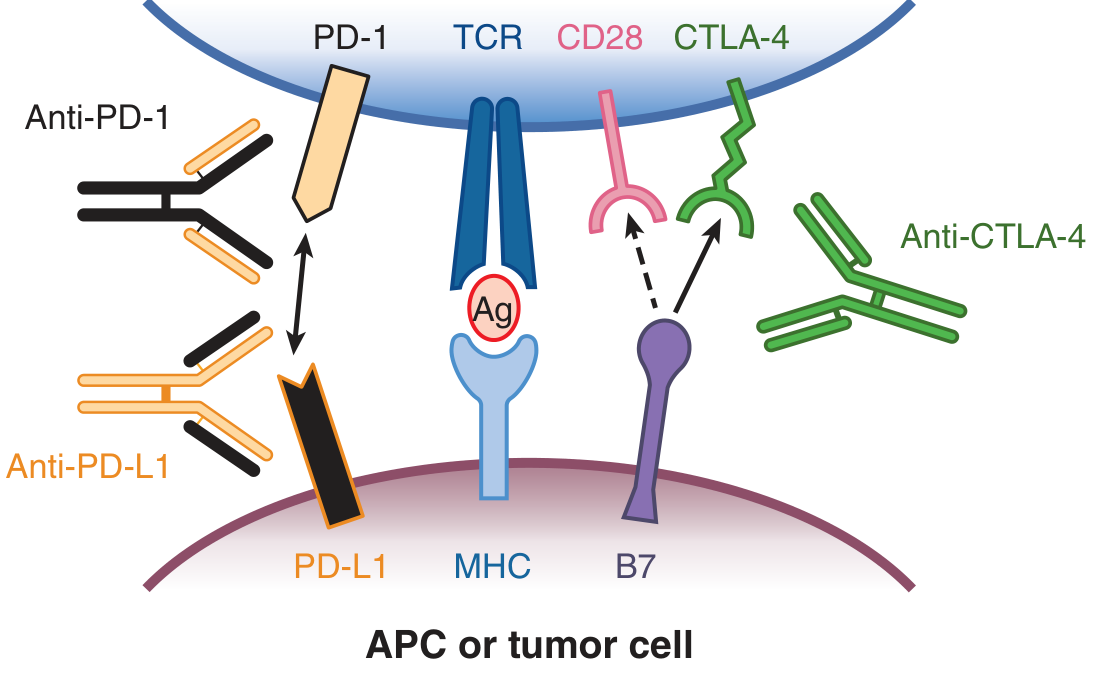
Approved checkpoint inhibitors include:
- Anti-PD-1: Pembrolizumab (Keytruda), Nivolumab (Opdivo)
- Anti-PD-L1: Atezolizumab, Durvalumab, Avelumab
- Anti-CTLA-4: Ipilimumab (Yervoy)
Cancers approved for ICI therapy (FDA-approved): Melanoma, non-small cell lung cancer (NSCLC), renal cell carcinoma, head and neck cancers, bladder cancer, Hodgkin lymphoma, gastric cancer, hepatocellular carcinoma, colorectal cancer (MSI-high), Merkel cell carcinoma, and others.
James Allison (anti-CTLA-4) and Tasuku Honjo (anti-PD-1) shared the 2018 Nobel Prize in Physiology/Medicine for this discovery.
2. Passive Immunotherapy - Monoclonal Antibodies (mAbs)
Humanized antibodies are designed to directly target proteins overexpressed on tumor cells:
| Antibody | Target | Cancer |
|---|---|---|
| Trastuzumab (Herceptin) | HER2 | Breast, gastric cancer |
| Rituximab | CD20 | B-cell lymphoma |
| Cetuximab | EGFR | Colorectal, head & neck |
| Bevacizumab | VEGF-A | Multiple cancers (anti-angiogenic) |
| Alemtuzumab | CD52 | CLL |
These antibodies work by:
- Blocking growth factor receptors (preventing tumor proliferation signals)
- Enabling NK cell-mediated ADCC (antibody-dependent cellular cytotoxicity)
- Activating complement
3. CAR-T Cell Therapy (Chimeric Antigen Receptor T Cells)
A patient's own T cells are collected, genetically engineered in the lab to express a synthetic receptor (CAR) that targets a specific tumor antigen, expanded massively, then infused back into the patient.
- CD19 CAR-T (e.g., Axicabtagene, Tisagenlecleucel) - used in B-cell leukemias/lymphomas (CLL, ALL, DLBCL)
- BCMA CAR-T - used in multiple myeloma
- These can produce highly durable responses in previously untreatable disease
4. Cancer Vaccines
- Prophylactic vaccines: HPV vaccine (Gardasil) prevents cervical cancer; HBV vaccine prevents hepatocellular carcinoma
- Therapeutic vaccines: Designed to stimulate immune responses against existing tumor antigens (e.g., sipuleucel-T for prostate cancer)
- Most effective against virally-induced cancers
5. Cytokine Therapy
Cytokines directly boost the immune response:
- IL-2 (Interleukin-2): High-dose IL-2 can produce durable responses in metastatic melanoma and renal cell carcinoma
- Interferons (IFN-alpha/gamma/beta): Used in hairy cell leukemia, mycosis fungoides, Kaposi's sarcoma, and some lymphomas
- GM-CSF: Enhances anti-tumor immunity
6. Antibody-Drug Conjugates (ADCs) & Other Targeted Biologics
- Monoclonal antibodies are linked to chemotherapy toxins or radiolabels, delivering a "guided missile" directly to tumor cells
- Examples: Trastuzumab emtansine (T-DM1), Brentuximab vedotin (anti-CD30)
- Bispecific antibodies (e.g., Blinatumomab) that bring T cells into proximity with tumor cells
Key Biomarkers Used to Select Patients for Immunotherapy
| Biomarker | Test | Significance |
|---|---|---|
| PD-L1 expression | IHC on biopsy | Higher PD-L1 = better response to PD-1/PD-L1 blockers |
| TMB (Tumor Mutational Burden) | Genomic sequencing | High TMB = more neoantigens = better ICI response |
| MSI-H / dMMR | PCR or IHC | Mismatch repair deficiency = good response to pembrolizumab |
| HER2 amplification | FISH / IHC | Target for trastuzumab |
| CD20 expression | IHC | Target for rituximab |
Side Effects (Immune-Related Adverse Events / irAEs)
Because ICIs release the immune system's brakes, they can cause the immune system to attack normal tissues:
- Skin: Rash, vitiligo, pruritus
- Gut: Colitis, diarrhea
- Lung: Pneumonitis
- Liver: Hepatitis (transaminase elevation)
- Endocrine: Thyroiditis, hypophysitis, adrenal insufficiency, type 1 diabetes
- Joints: Arthritis, myositis
Management involves holding the immunotherapy and treating with corticosteroids (and sometimes other immunosuppressants for severe cases).
Summary Table
| Type | Example Drugs | Mechanism |
|---|---|---|
| Checkpoint inhibitors | Pembrolizumab, Nivolumab, Ipilimumab | Release T-cell brakes |
| Monoclonal antibodies | Trastuzumab, Rituximab, Bevacizumab | Direct tumor targeting, ADCC |
| CAR-T cells | Axicabtagene, Tisagenlecleucel | Engineered T cells attack tumor |
| Cancer vaccines | HPV vaccine, Sipuleucel-T | Prime immune response to tumor antigens |
| Cytokines | IL-2, IFN-alpha | Boost immune system activity |
| ADCs | T-DM1, Brentuximab | Guided chemo delivery |
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Roitt's Essential Immunology; Sabiston Textbook of Surgery
Would you like me to go deeper into any specific type - for example, checkpoint inhibitors for a particular cancer, CAR-T therapy, or the side effects and their management?
This is a shared conversation. Sign in to Orris to start your own chat.