How to treat chronic constipation and bleeding anal fissure
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chronic constipation" AND treatment
Searching PubMed
"anal fissure" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-organized answer. Here it is:
Treatment of Chronic Constipation and Bleeding Anal Fissure
These two conditions are closely linked - chronic constipation causes hard stools that tear the anoderm, and fissure pain triggers sphincter spasm that worsens defecation. Treating both together is essential.
Part 1: Chronic Constipation
The management algorithm below (from Yamada's Textbook of Gastroenterology) guides workup and treatment:
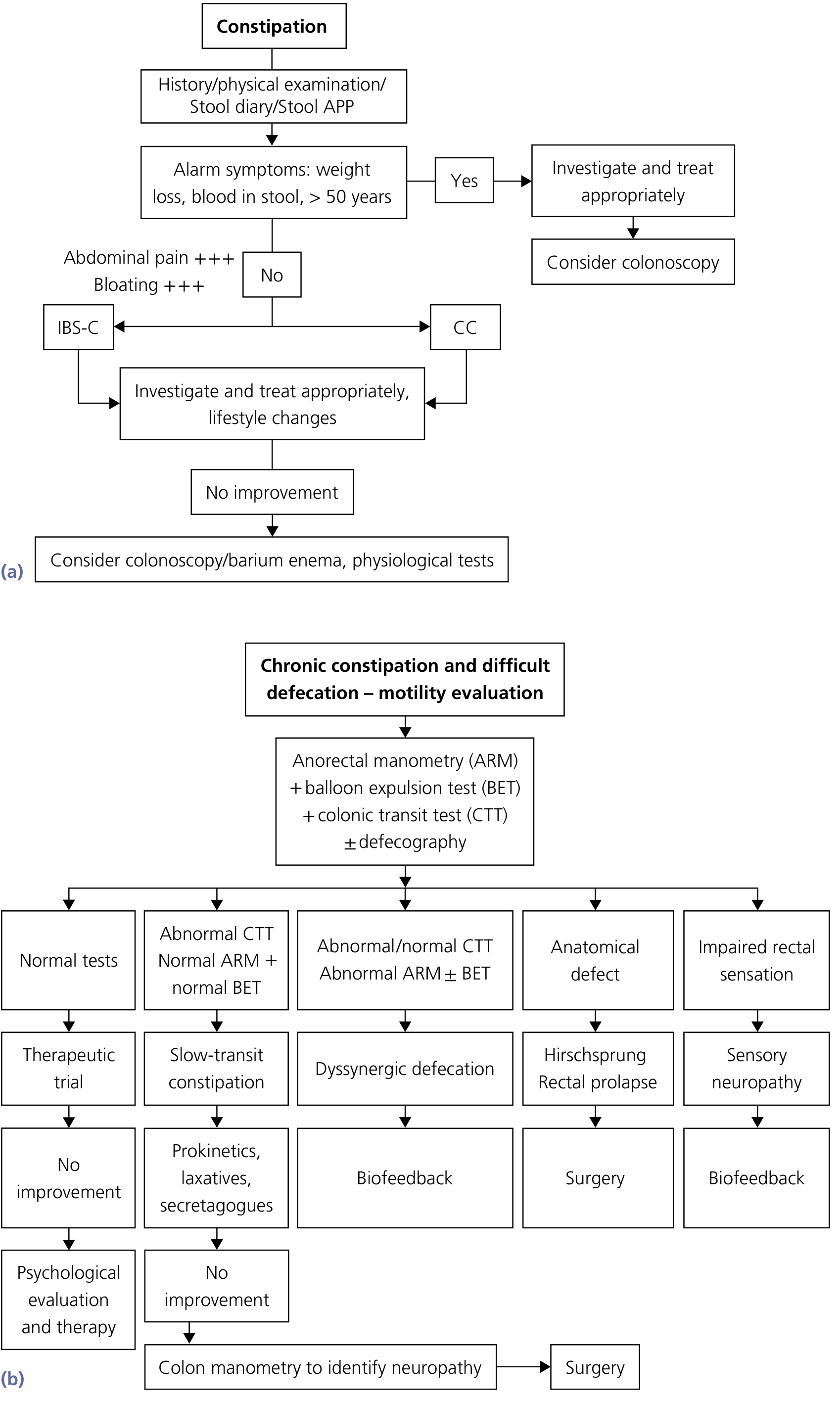
Treatment should be individualized based on the underlying cause (slow transit, dyssynergic defecation, or normal transit) and the patient's comorbidities.
1. Lifestyle Modifications
-
Adequate fluid intake - maintain good hydration throughout the day
-
Regular, non-strenuous exercise - exercise increases propagated colonic contractions; sedentary patients are at much higher risk (relative risk of constipation in bed-bound patients is ~15x that of those who walk daily)
-
Timed toilet training - attempt defecation for ~5 minutes at least twice daily, 30-60 minutes after a meal; never suppress the urge to defecate
-
Optimal timing: the colon is most active in the first 2 hours after waking and after breakfast
-
Yamada's Textbook of Gastroenterology, 7th Ed., p. 747-748
2. Diet and Fiber
-
Target fiber intake of 20-30 g/day
-
Psyllium (ispaghula husk) is the best-evidenced bulk-forming agent - Grade B recommendation from the American College of Gastroenterology; increases stool frequency by ~1.4 bowel movements/week
-
Dried prunes were shown superior to psyllium in mild-to-moderate constipation
-
Note: fiber supplements are less effective in slow-transit constipation or pelvic floor dysfunction
-
Yamada's Textbook of Gastroenterology, 7th Ed., p. 748
3. Laxatives (Step-Up Approach)
| Class | Agent | Mechanism | Notes |
|---|---|---|---|
| Bulk-forming | Psyllium, methylcellulose | Water retention, stool softening | First-line; safe long-term |
| Osmotic | Polyethylene glycol (PEG), lactulose, magnesium hydroxide | Draw water into colon | PEG preferred - well-tolerated, no electrolyte issues |
| Stimulant | Bisacodyl, senna | Stimulate colonic motility | Short-term use; avoid long-term dependency |
| Stool softener | Docusate sodium | Surface tension reduction | Often combined with stimulants |
| Lubricant | Mineral oil | Softens stool | Avoid if aspiration risk (elderly, neurological) |
4. Prescription Medications (for refractory cases)
-
Lubiprostone (Amitiza) - chloride channel (ClC-2) activator; increases intestinal fluid secretion; approved for chronic idiopathic constipation and IBS-C
-
Linaclotide (Linzess) - guanylate cyclase-C (GCC) receptor agonist; stimulates chloride/bicarbonate secretion; effective in RCTs for chronic constipation and IBS-C
-
Plecanatide (Trulance) - also activates GCC receptors; two large RCTs confirmed efficacy at 3 mg daily for 12 weeks
-
Prucalopride - selective 5-HT4 agonist (prokinetic); accelerates colonic transit; approved for chronic idiopathic constipation in women
-
Yamada's Textbook of Gastroenterology, 7th Ed., p. 751-752
5. Treatment of Opioid-Induced Constipation
If constipation is drug-induced (narcotics are a common cause), peripherally acting mu-opioid receptor antagonists (PAMORAs) are indicated:
- Methylnaltrexone (subcutaneous or oral)
- Naloxegol (pegylated naloxone - does not cross blood-brain barrier)
- Naldemedine (Symproic)
6. Dyssynergic Defecation
If anorectal manometry + balloon expulsion testing confirms dyssynergia (pelvic floor dysfunction - failure to relax puborectalis/external sphincter during straining):
- Biofeedback therapy is the primary treatment - instrument-based neuromuscular conditioning to restore coordinated defecation; has strong evidence
- Botulinum toxin injection into the puborectalis has limited efficacy
- Surgery is rarely indicated for this subtype
7. Slow-Transit Constipation
When colonic transit testing confirms slow transit and all pharmacological measures fail:
- Colonic manometry to identify colonic neuropathy
- Subtotal colectomy with ileorectal anastomosis - reserved for severe, refractory cases
Part 2: Anal Fissure (Acute + Chronic, with Bleeding)
An anal fissure is a longitudinal tear in the anoderm of the distal anal canal. It is the classic cause of bright red rectal bleeding with severe, sharp pain during and after defecation. Hard stools from constipation are the primary precipitant.
The cycle of injury: Hard stool -> fissure -> pain -> internal anal sphincter (IAS) spasm -> reduced blood flow to posterior midline -> ischemia -> failure to heal -> chronic fissure.
- Sabiston Textbook of Surgery, 21st Ed., p. (block 23)
Location: 75% posterior midline. Fissures off the midline suggest secondary causes (Crohn's disease, TB, HIV, syphilis, anal cancer).
Conservative Measures (First for Acute Fissures)
Approximately 70% of chronic fissures and the vast majority of acute fissures heal with conservative therapy alone (Fischer's Mastery of Surgery, 8th Ed.).
- Stool softening - the single most important step. Increase fluids + fiber + psyllium/methylcellulose + mild laxative (bisacodyl or docusate). Eliminate straining.
- Sitz baths (warm water soaks, 10-15 min, 2-3x daily) - provide significant pain relief in >90% of patients with acute fissures and promote local vasodilation
- Topical local anesthetics (lidocaine 2-5% ointment) - short-term pain relief, especially for acute fissures
- Topical corticosteroids - reduce local inflammation; available as combination ointments/suppositories
- Anal hygiene - gentle cleansing; avoid aggressive wiping
Specific First-Line Medical Therapy: Sphincter Relaxants
These break the spasm-ischemia cycle that prevents healing:
Option A: Topical Glyceryl Trinitrate (GTN / nitroglycerin 0.2-0.4%)
- Most widely used first-line agent
- Apply over the fissure after defecation and at bedtime; increase to 4x/day if needed
- Achieves pain relief in 60-70% at 4 weeks; healing in 45-60% at 3 months; 60-80% with repeat course
- Main side effect: headache in 30-40% of patients; 20-30% cannot tolerate it long-term (tachyphylaxis usually develops within 5-6 days)
Option B: Topical Calcium Channel Blockers (Diltiazem 2% or Nifedipine 0.2-0.3% cream)
-
Preferred when GTN is not tolerated
-
Apply twice daily up to 4x/day; pain relief at 4 weeks: 60-70%; healing at 3 months: 40-60%
-
Virtually no headache side effects - better tolerability profile than GTN; similar efficacy
-
Note: no commercial formulation available in the US - requires compounding pharmacy
-
Sabiston Textbook of Surgery; Fischer's Mastery of Surgery, 8th Ed., p. 4238-4839
Specific Second-Line Medical Therapy: Botulinum Toxin Injection
When topical therapies fail or fissure recurs:
- Inject 20-100 IU into the internal anal sphincter (intersphincteric plane, typically at 3 and 9 o'clock positions)
- Induces temporary sphincter paralysis lasting ~3 months
- Healing rates: 40-60% as second-line therapy; modest additional benefit after failed topical therapy
- Can be done in-office or as outpatient procedure with sedation
- Side effects: transient flatus incontinence (warn all patients), temporary increased urinary residual volume; hematoma/sepsis are uncommon
A 2024 meta-analysis (PMID: 39579232) compared botulinum toxin vs. lateral internal sphincterotomy across RCTs.
Surgical Treatment: Lateral Internal Sphincterotomy (LIS)
Reserved for patients who fail medical management (sequential trials of topical agents and botulinum toxin):
-
Partial division of the internal anal sphincter (lower one-third), reducing resting anal tone
-
Most effective treatment: healing rates >90% - significantly superior to all medical options
-
Can be done open or closed technique, usually under local anesthesia as an outpatient
-
Main risk: incontinence - minor fecal or flatus incontinence occurs in 0-30% depending on technique; permanent incontinence risk is ~1-2%
-
Because of incontinence risk, surgery is not offered until at least first-line (and often second-line) medical therapy has been attempted first
-
Women, elderly, and those with prior obstetric injuries are at higher risk for post-LIS incontinence
-
Fischer's Mastery of Surgery, 8th Ed., p. 4845; Sabiston Textbook of Surgery
Summary: Stepwise Treatment Plan
STEP 1 (Both conditions simultaneously):
- High-fiber diet (20-30g/day) + increased fluids
- Psyllium or methylcellulose supplement
- Stimulant/osmotic laxative (PEG, bisacodyl) to ensure soft stools
- Sitz baths (3x daily)
- Timed toilet training; never suppress defecation urge
- Topical local anesthetic for pain PRN
STEP 2 (If fissure not healed in 4-8 weeks):
- Add topical GTN 0.2% OR diltiazem 2% cream
- Continue stool softening
STEP 3 (Refractory / 2nd-line):
- Botulinum toxin injection (20-100 IU) into IAS
- For constipation: escalate to linaclotide, prucalopride, or lubiprostone
STEP 4 (Surgical):
- Lateral internal sphincterotomy (LIS) for chronic fissure unresponsive to above
- Subtotal colectomy for severe refractory slow-transit constipation (rare)
Recent evidence notes:
- A 2024 network meta-analysis (PMID: 38693449) found probiotics, prebiotics, and synbiotics provide modest benefit as adjuncts to constipation therapy in adults.
- A 2025 systematic review (PMID: 39531948) confirmed abdominal massage as an effective non-pharmacological intervention for chronic constipation.
- A 2025 systematic review (PMID: 41493321) confirmed conservative approaches have comparable short-term outcomes to surgery for anal fissure, but surgery has superior long-term healing rates.
Important: All treatments listed here are clinical information for educational purposes. Patients should be evaluated individually - especially for alarm symptoms (weight loss, blood in stool, age >50, off-midline fissures) that warrant colonoscopy before assuming a benign cause.
This is a shared conversation. Sign in to Orris to start your own chat.