Nose anatomy clearly with simple way
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the diagrams and comprehensive content. Here is the full, clearly structured anatomy of the nose:
Nose Anatomy - Simple & Clear
1. External Skeleton (What You See From Outside)
The outer nose is supported by a framework of bone and cartilage:
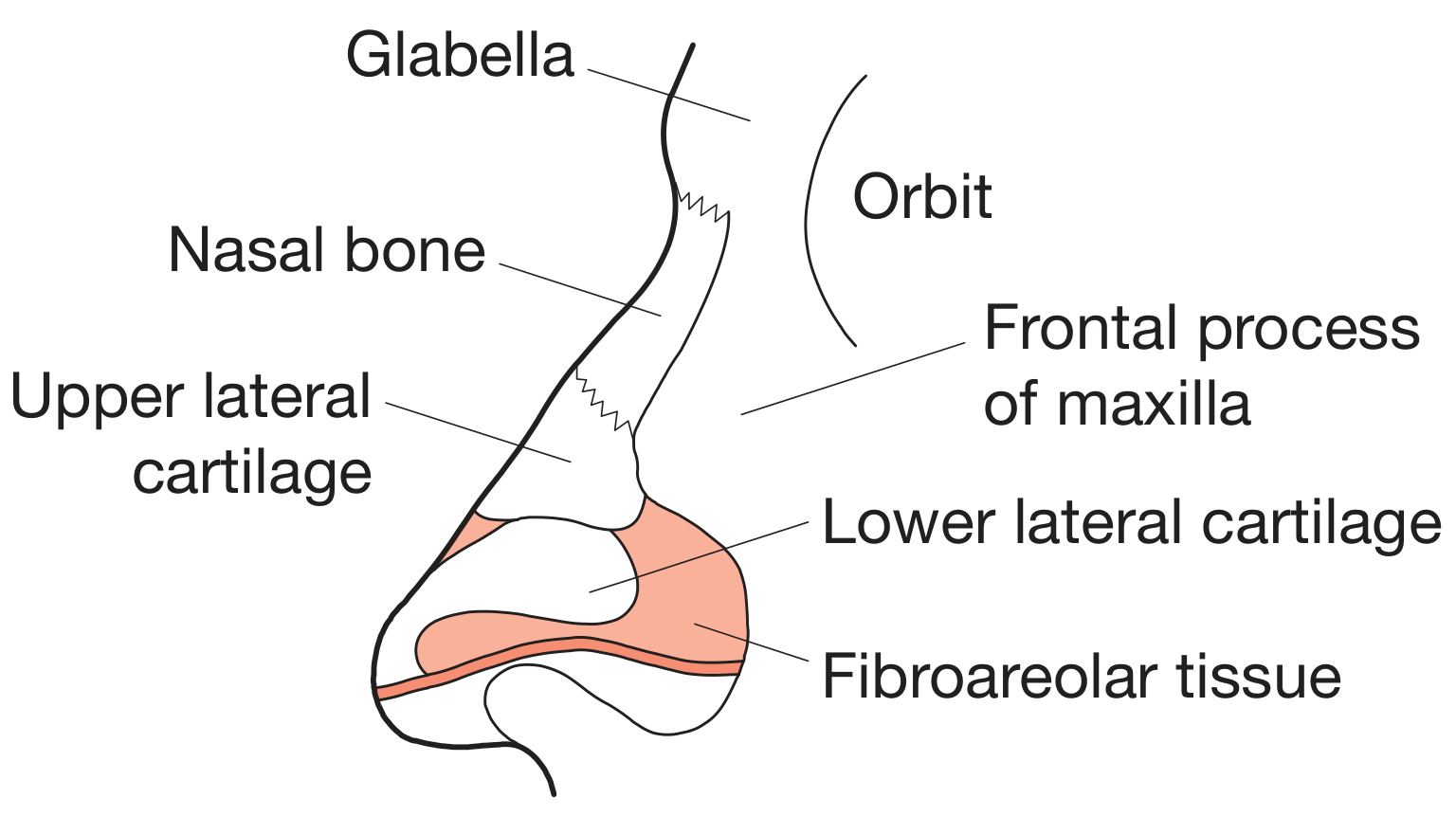
| Part | What It Is |
|---|---|
| Nasal bones (upper 1/3) | Two small bones that form the hard "bridge" of the nose |
| Upper lateral cartilages (middle 1/3) | Paired flat cartilages that form the middle vault |
| Lower lateral cartilages (lower 1/3) | Paired curved cartilages that form the tip and nostrils |
| Fibroareolar tissue | Connects the lower cartilages to fill the alar lobule |
| Glabella | The smooth area between the eyebrows, just above the nose |
| Frontal process of maxilla | The cheekbone contributes to the side of the nose |
Simple rule: Top = bone, middle = upper cartilage, bottom = lower cartilage.
2. The Nasal Septum (Divides Left and Right)
The septum splits the nose into two halves. It has three parts:
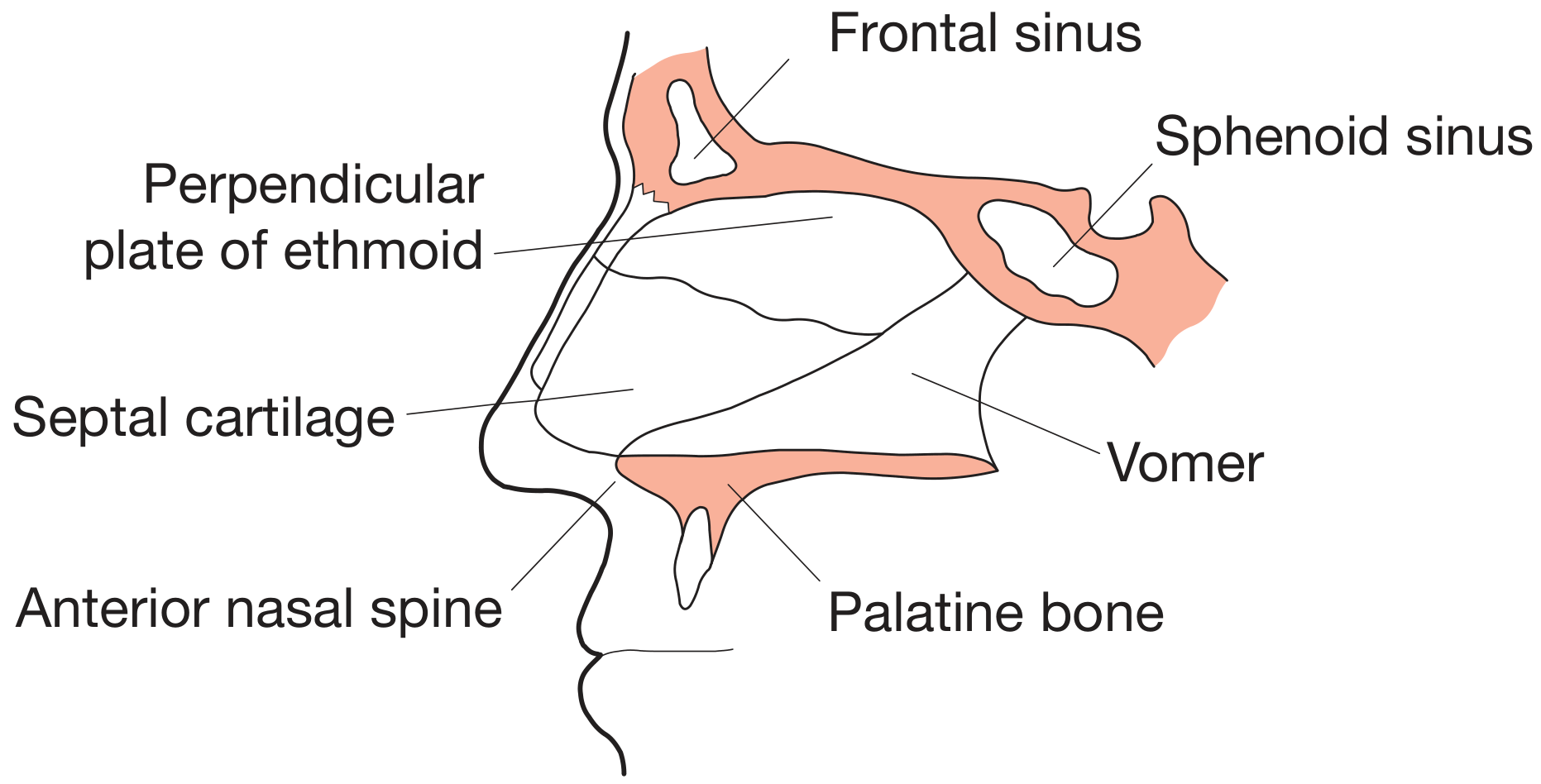
| Part | Location | Material |
|---|---|---|
| Septal (quadrilateral) cartilage | Front portion | Cartilage |
| Perpendicular plate of ethmoid | Upper-back portion | Bone |
| Vomer | Lower-back portion | Bone |
The anterior nasal spine anchors the bottom of the septum to the face. A deviated septum (bent to one side) commonly causes nasal obstruction.
3. The Nasal Cavity (Inside the Nose)
The nasal cavity runs from the nostrils (nares) back to the nasopharynx. Its lateral (outer) wall has three shelf-like projections called turbinates (or conchae):
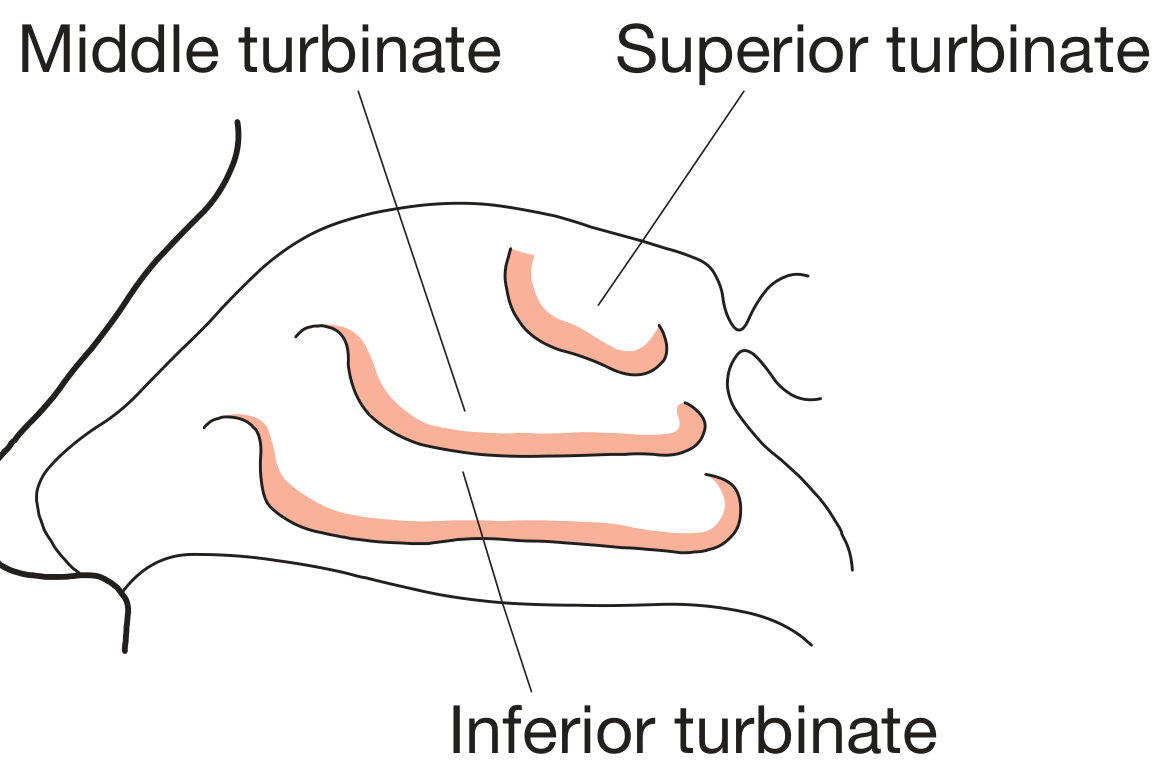
| Turbinate | Main Role |
|---|---|
| Inferior turbinate (largest) | Warms and humidifies inhaled air |
| Middle turbinate | Protects the sinus drainage openings |
| Superior turbinate (smallest) | Located near the olfactory (smell) area |
The space beneath each turbinate is called a meatus:
- Inferior meatus - where the nasolacrimal duct drains (tears from the eye)
- Middle meatus - where the frontal, maxillary, and anterior ethmoid sinuses drain
- Superior meatus - where the posterior ethmoid sinus drains
4. Paranasal Sinuses (Air Spaces Around the Nose)
There are 4 pairs of sinuses, all connected to the nasal cavity:
| Sinus | Location | Drains Into |
|---|---|---|
| Maxillary | Cheekbones | Middle meatus |
| Frontal | Above eyebrows | Middle meatus |
| Ethmoid (anterior) | Between eyes | Middle meatus |
| Ethmoid (posterior) | Between eyes | Superior meatus |
| Sphenoid | Deep, behind nose | Sphenoethmoidal recess |
The sinuses lighten the skull, produce mucus, and give resonance to the voice.
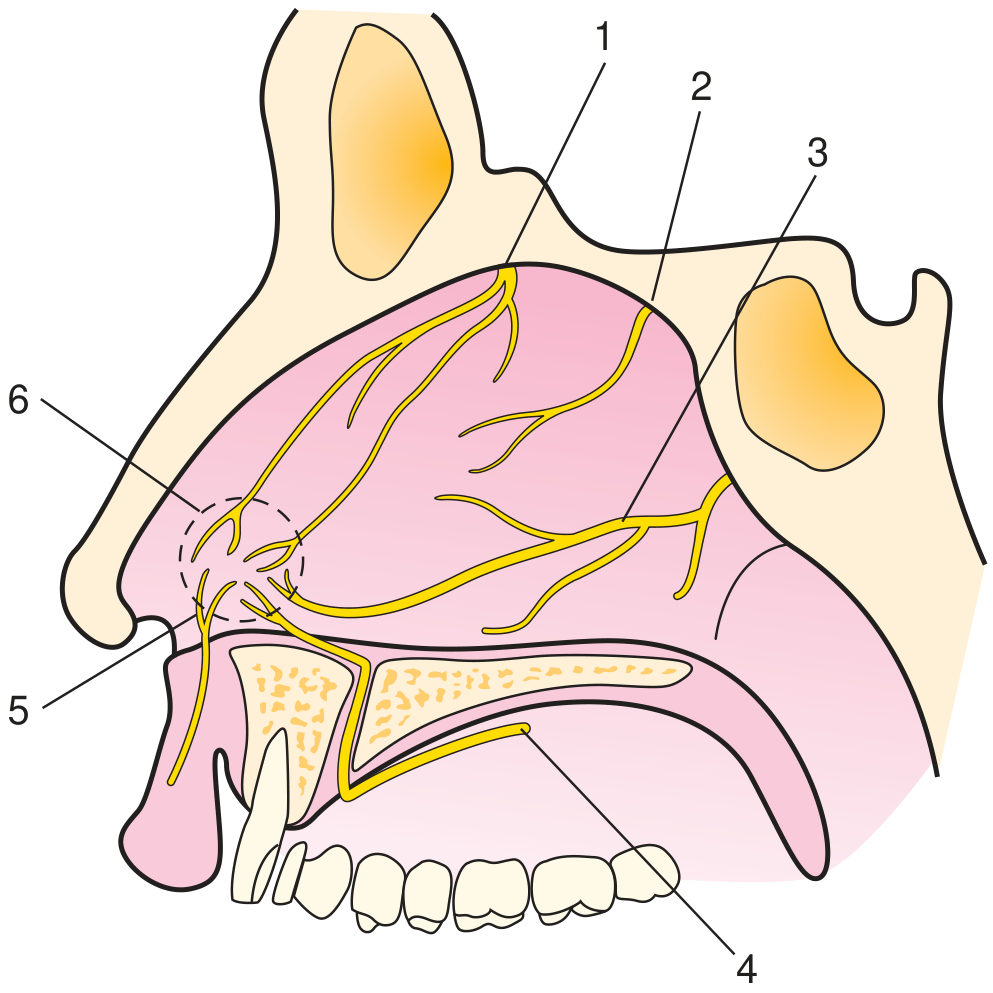
5. Blood Supply (Very Important - Explains Nosebleeds)
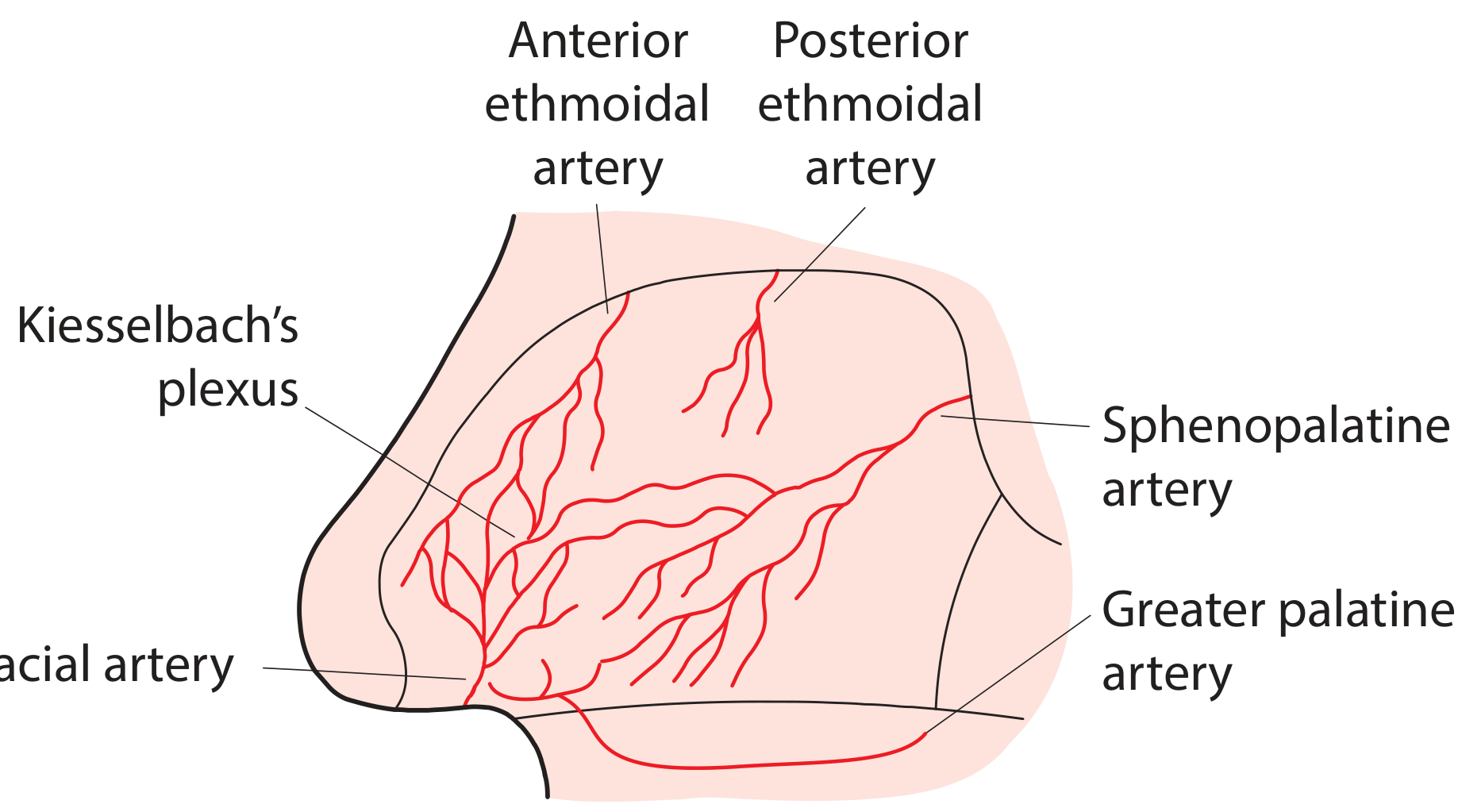
Two main sources supply the nose:
From the External Carotid Artery:
- Sphenopalatine artery (largest supply - supplies the back of the nasal cavity)
- Facial artery
- Greater palatine artery (via incisive canal to the anteroinferior septum)
From the Internal Carotid Artery (via ophthalmic artery):
- Anterior ethmoidal artery
- Posterior ethmoidal artery
All these vessels meet on the front part of the septum to form Kiesselbach's plexus (also called Little's area). This is where ~90% of nosebleeds (epistaxis) come from, because it is so richly supplied and easily traumatized.
6. Overall Relationship to the Head
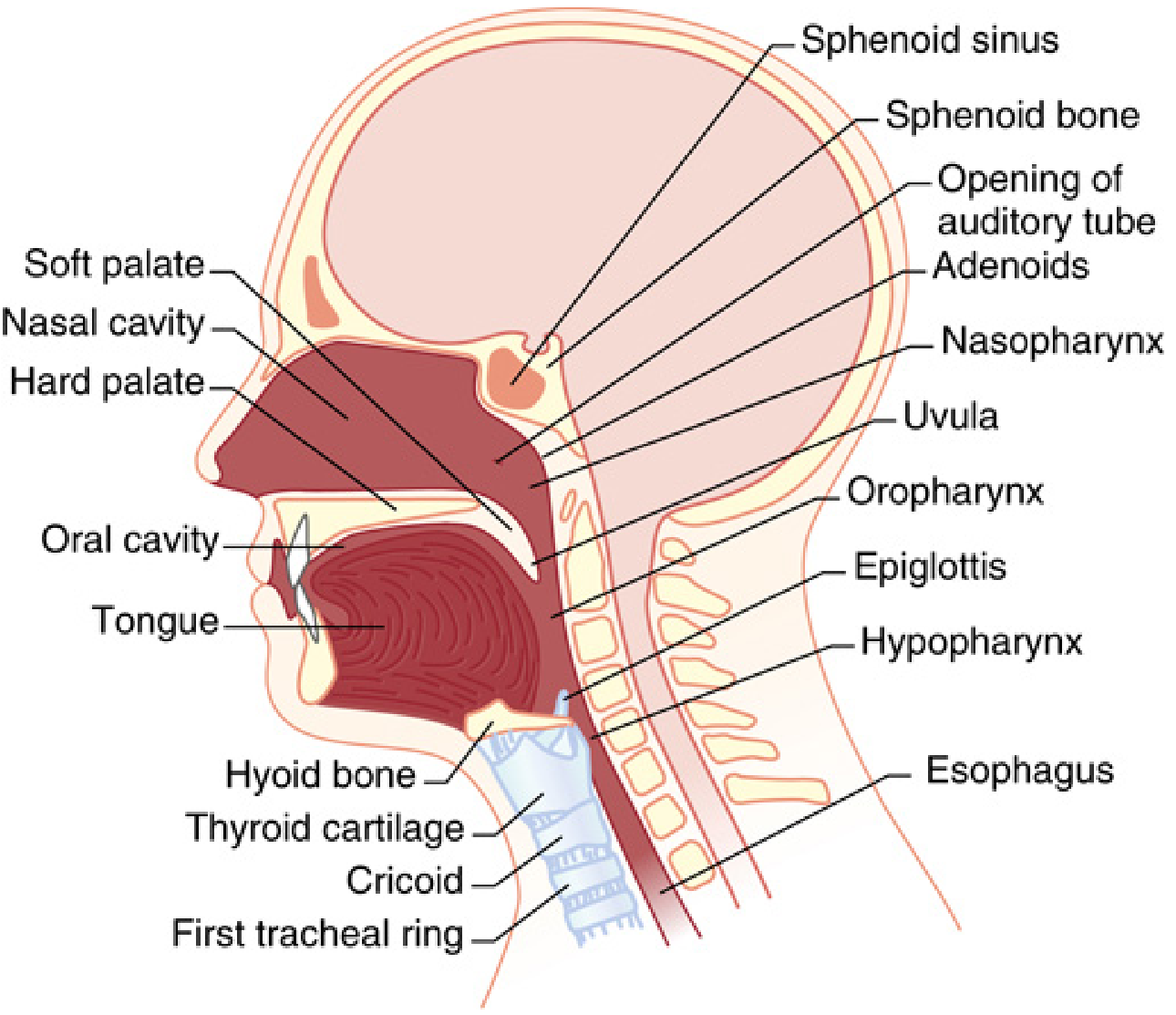
The nasal cavity sits above the hard palate (roof of the mouth) and opens posteriorly into the nasopharynx. Above it lies the skull base. The adenoids sit on the back wall of the nasopharynx.
Quick Summary Table
| Structure | Simple Description |
|---|---|
| Nasal bones | Hard bridge at the top |
| Upper lateral cartilage | Supports the middle of the nose |
| Lower lateral cartilage | Forms the tip and nostrils |
| Nasal septum | Divides left and right - cartilage in front, bone behind |
| Turbinates (3) | Shelves inside that warm and filter air |
| Paranasal sinuses (4) | Air pockets in the skull bones that drain into the nose |
| Kiesselbach's plexus | Main nosebleed site on the front of the septum |
Sources: Bailey and Love's Short Practice of Surgery 28th Edition, p. 785-786; Cummings Otolaryngology Head and Neck Surgery; Miller's Anesthesia 10e
Clinical correlations
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Here are the clinical correlations of nose anatomy, each tied directly to the structure involved:
Clinical Correlations of Nose Anatomy
1. Kiesselbach's Plexus → Epistaxis (Nosebleed)
Anterior epistaxis accounts for 90% of all nosebleeds and almost always involves Kiesselbach's plexus on the anteroinferior septum. It is typically unilateral and easier to control.
Posterior epistaxis (10%) arises from the posterior cavity, mainly the sphenopalatine artery. It is more severe, harder to control, and occurs mostly in older adults with comorbidities.
Risk factors:
- Nose picking / dry air (desiccates mucosa - common in winter)
- Hypertension (associated with persistent bleeding)
- Anticoagulants (aspirin, warfarin, clopidogrel)
- Bleeding disorders (HHT - Hereditary Hemorrhagic Telangiectasia)
- Intranasal tumors
Management:
- Pinch the cartilaginous (soft) part of the nose for 10-15 minutes
- Oxymetazoline spray (vasoconstrictor) before applying pressure
- Chemical cautery if source identified
- Nasal packing for refractory cases
- ENT referral for posterior bleeding
Red flag: An adolescent boy with recurrent epistaxis + nasal obstruction = suspect juvenile nasopharyngeal angiofibroma (benign but locally aggressive tumor).
- Rosen's Emergency Medicine; Textbook of Family Medicine 9e
2. Nasal Septum → Deviated Septum & Septoplasty
Most people have some degree of septal deviation - only symptomatic cases need treatment.
Causes:
- Nasal trauma (most common - even "minor" past trauma)
- Congenital
Symptoms:
- Unilateral or bilateral nasal obstruction
- Mouth breathing (especially at night)
- Recurrent sinusitis (if deviation obstructs the ostiomeatal complex)
- Snoring
Diagnosis: Anterior rhinoscopy; posterior deviations need nasal endoscopy or CT scan.
Treatment - Septoplasty:
- Done through an intranasal incision
- Deviated cartilage/bone is repositioned or removed
- Often combined with turbinate reduction
- Well tolerated as day surgery
- Avoid in children (risk of disrupting nasal/facial growth) unless deviation is severe
- Textbook of Family Medicine 9e, p. 419; Cummings Otolaryngology
3. Turbinates → Turbinate Hypertrophy & "Empty Nose Syndrome"
The inferior turbinate is the most commonly affected. Chronic inflammation from allergy or rhinosinusitis causes it to swell, blocking airflow.
Treatment options (least to most aggressive):
- Topical steroids / antihistamines
- Radiofrequency reduction, cautery, cryotherapy
- Submucosal resection of conchal bone (most effective)
Empty Nose Syndrome - the "too much surgery" complication:
- Overly aggressive turbinate removal leaves the nasal cavity too large and "empty"
- Paradoxically, the patient feels they cannot breathe despite a wide open nose
- Causes: nasal sicca (dryness), crusting, bleeding, discomfort, depression
- Very difficult to treat - conservative surgery is key
- Textbook of Family Medicine 9e
4. Paranasal Sinuses → Sinusitis & Its Complications
Acute sinusitis is most commonly preceded by viral rhinitis (common cold). Mucosal swelling blocks sinus drainage, creating a warm, moist pocket where bacteria thrive. The middle meatus is the most clinically important site as the maxillary, frontal, and anterior ethmoid sinuses all drain there.
Chronic sinusitis - polymicrobial, often with fungi (especially in diabetics - think mucormycosis).
Serious complications of sinusitis (when infection spreads):
| Complication | Mechanism |
|---|---|
| Orbital cellulitis/abscess | Ethmoid sinuses sit directly against the medial orbit - infection spreads easily |
| Osteomyelitis | Bony sinus walls eroded by chronic infection |
| Cavernous sinus thrombosis | Venous drainage from the nose communicates with the ophthalmic vein → cavernous sinus (life-threatening) |
| Meningitis / brain abscess | Direct spread through the skull base (rare but fatal if missed) |
| Mucocele | Blocked frontal/ethmoid sinus fills with mucus, expands slowly, erodes bone |
Kartagener syndrome - inherited ciliary defect causing recurrent sinusitis + bronchiectasis + situs inversus.
- Robbins Pathologic Basis of Disease; Bailey & Love's Surgery
5. Nasal Mucosa / Turbinates → Rhinitis & Common Cold
The nasal mucosa (lining the turbinates and septum) is the first line of defense against inhaled air. Rhinovirus damages the respiratory epithelium, causing the common cold - the most common human infection.
Types of rhinitis:
| Type | Cause | Key Feature |
|---|---|---|
| Acute viral | Rhinovirus (most common) | Self-limiting 7-10 days |
| Allergic | IgE-mediated (pollens, dust mites) | Seasonal or perennial; sneezing, watery discharge |
| Non-allergic | Vasomotor, drugs, hormonal | No allergic trigger identified |
| Drug-induced (Rhinitis medicamentosa) | Rebound from prolonged decongestant use | Worsens with oxymetazoline overuse |
6. Middle Meatus / Sinuses → Nasal Polyps
Nasal polyps are benign, pale gray, translucent swellings arising from chronically inflamed nasal mucosa - they look like peeled grapes on endoscopy.
Associations:
- Chronic rhinosinusitis (most common)
- Asthma (Samter's triad: polyps + asthma + aspirin sensitivity)
- Allergic rhinitis
- Cystic fibrosis - nasal polyps in a child should always prompt CF testing
Symptoms: Progressive nasal blockage + anosmia (loss of smell) - the anosmia is often the clue.
Unilateral polyps = red flag - must rule out tumor or fungal disease.
Treatment: Topical steroids first → endoscopic sinus surgery (ESS) if inadequate. Polyps almost always recur without continued medical treatment post-surgery.
- Goldman-Cecil Medicine; Textbook of Family Medicine 9e; Scott-Brown's Otolaryngology
7. Nasal Bones → Nasal Fracture
The nasal bones are the most commonly fractured bones in the face because they protrude and have no protective musculature.
Clinical signs: Swelling, tenderness, crepitus, visible deformity, epistaxis, septal hematoma.
Septal hematoma - do not miss: Blood collects between the cartilage and its perichondrium. If not drained urgently, it:
- Cuts off blood supply to the cartilage
- Leads to avascular necrosis → saddle nose deformity
- Can get infected → septal abscess
Management of septal hematoma: Immediate surgical drainage + nasal pack to prevent re-accumulation.
8. Nose → Upper Airway Anatomy Relevance (Anesthesia / Intubation)
- The nasal cavity is the preferred route for nasotracheal intubation (jaw trauma, oral surgery cases)
- Risk: epistaxis from turbinate or Kiesselbach trauma during instrumentation
- Nasal surgery (septoplasty, rhinoplasty) can trigger laryngospasm via blood/secretions on the vocal cords - a true anesthetic emergency
- The adenoids in the nasopharynx can cause nasotracheal tube obstruction in children
- Miller's Anesthesia 10e
Quick Clinical Reference Card
| Structure | Condition | Key Clinical Point |
|---|---|---|
| Kiesselbach's plexus | Epistaxis (90%) | Pinch soft nose 10 min; oxymetazoline |
| Nasal septum | Deviated septum | Septoplasty; avoid in children |
| Inferior turbinate | Turbinate hypertrophy | Conservative reduction; avoid empty nose |
| Paranasal sinuses | Sinusitis | Middle meatus is key drainage point |
| Ethmoid sinus | Orbital complications | Sits next to orbit - spreads easily |
| Nasal mucosa | Rhinitis / polyps | Polyps in child → test for CF |
| Nasal bones | Fracture / septal hematoma | Drain hematoma urgently → saddle nose |
| Nasopharynx | Angiofibroma | Teenage boy + recurrent epistaxis |
This is a shared conversation. Sign in to Orris to start your own chat.