Case study of bels palsy
Reading File
Finding Sources
Searching PubMed
"Bell palsy" treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Harrison's (2025), Adams & Victor's Neurology, and Bradley's. Let me compile the full case study.
Bell's Palsy - Comprehensive Case Study
Illustrative Case Presentation
Patient: 38-year-old male, no significant past medical history
Presenting complaint: Sudden-onset right-sided facial weakness, noticed on waking. Unable to close right eye. Mouth drooping to the right. Pain behind the right ear for the past 2 days.
Additional symptoms: Altered taste on the right side of tongue, sounds seem louder in the right ear (hyperacusis), mild facial numbness (subjective)
No: Vesicular rash, limb weakness, speech disturbance, rash, tick bite, recent illness
Definition & Epidemiology
Bell's palsy is the most common peripheral facial nerve (CN VII) palsy. It is defined as an acute, idiopathic, unilateral lower motor neuron (LMN) facial paralysis.
- Annual incidence: ~25 per 100,000 (approximately 1 in 60 persons over a lifetime)
- Affects men and women roughly equally; occurs at all ages
- Risk factors: pregnancy (especially third trimester and first 2 weeks postpartum), diabetes mellitus, hypertension
- Recurrence rate: ~7-8% of cases, interval averaging ~10 years
- Harrison's Principles of Internal Medicine 22E, p. 3597; Adams and Victor's Principles of Neurology 12E, p. 1371
Anatomy & Pathophysiology
The facial nerve (CN VII) exits the brainstem at the pontomedullary junction, travels through the internal auditory canal, geniculate ganglion, and the facial canal in the temporal bone before exiting at the stylomastoid foramen to innervate all muscles of facial expression. It also carries:
- Taste from anterior 2/3 tongue (via chorda tympani)
- Autonomic fibers to lacrimal and salivary glands
- A branch to the stapedius muscle (hearing modulation)
In Bell's palsy, there is inflammation and swelling of the facial nerve, causing compression within the tight bony facial canal. Histology shows mononuclear cell infiltration consistent with viral or immune cause.
Viral etiology:
- HSV-1 reactivation in the geniculate ganglion is the primary cause - HSV-1 DNA was detected in endoneurial fluid and posterior auricular muscle in the majority of Bell's palsy cases
- Varicella-zoster virus (VZV) accounts for up to one-third of cases
- Other viruses (including SARS-CoV-2) implicated less commonly
- Bell's palsy can occur during HIV seroconversion
- Harrison's 22E, p. 3598; Adams and Victor's 12E, p. 1371
Clinical Features
Presentation
| Feature | Detail |
|---|---|
| Onset | Abrupt; 50% reach maximal weakness within 48 h, nearly all within 3-4 days |
| Pain | Retroauricular (behind the ear) - may precede palsy by 1-2 days |
| Facial weakness | ALL ipsilateral facial muscles (forehead AND lower face - LMN pattern) |
| Eye | Cannot close eye (lagophthalmos), Bell's phenomenon (eye rolls up on attempted closure) |
| Mouth | Drooping of ipsilateral corner, drooling, difficulty eating |
| Taste | Impaired on anterior 2/3 of ipsilateral tongue (chorda tympani involvement) |
| Hyperacusis | Ipsilateral - stapedius muscle paralysis |
| Subjective numbness | May occur without objective sensory loss |
Key Clinical Point - LMN vs. UMN Palsy
In Bell's palsy (LMN/peripheral), both the forehead and lower face are equally affected because all facial muscles lose their ipsilateral innervation. In upper motor neuron (central/cortical) lesions, the forehead is spared because upper facial muscles receive bilateral cortical innervation. This distinction is critical in examination.
- Harrison's 22E, p. 3598
MRI Findings
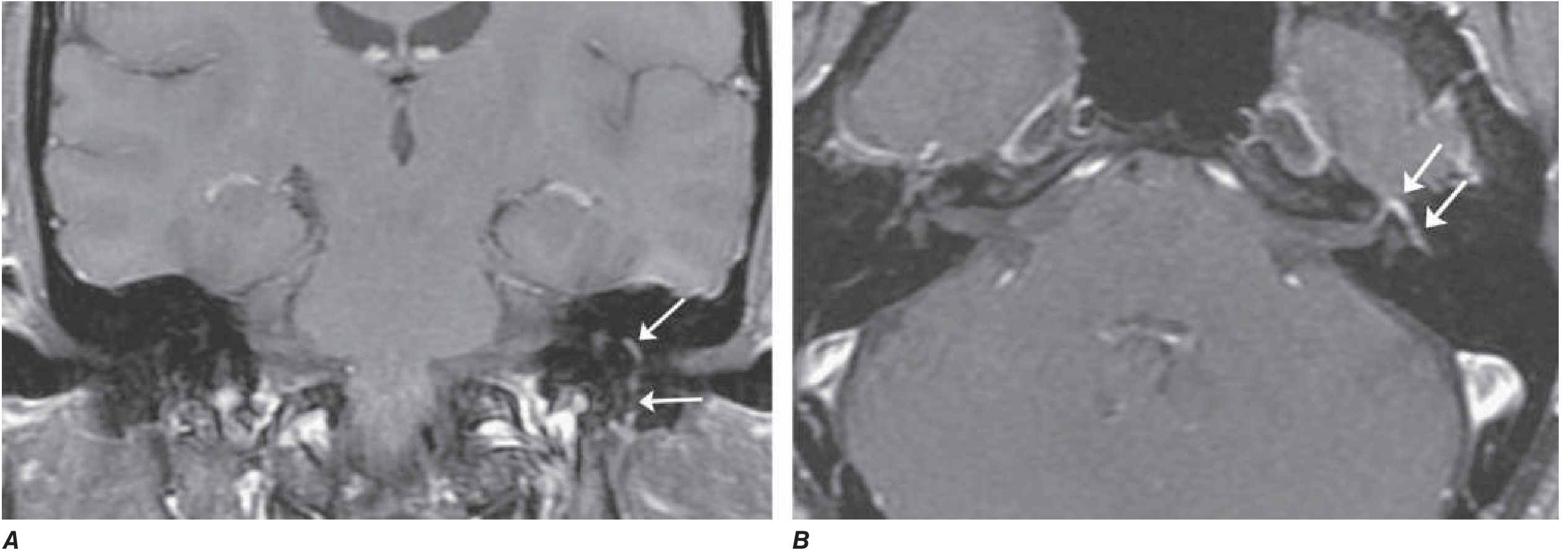
Axial and coronal T1 post-gadolinium MRI with fat suppression showing diffuse smooth linear enhancement of the left facial nerve involving the genu, tympanic, and mastoid segments within the temporal bone (arrows), without mass lesion. This pattern is highly suggestive of Bell's palsy but can also be seen in Lyme disease, sarcoidosis, and perineural malignant spread.
(Harrison's 22E, Fig. 452-4)
Differential Diagnosis
Bell's palsy is a diagnosis of exclusion. The following must be ruled out:
| Condition | Distinguishing Features |
|---|---|
| Ramsay Hunt Syndrome (VZV reactivation) | Vesicular rash in external auditory canal, pharynx, or pinna; CN VIII involvement (hearing loss, vertigo); more severe palsy, worse prognosis |
| Lyme disease | Tick bite history, erythema migrans, arthritis; can cause bilateral facial palsy; CSF pleocytosis; in endemic areas, >10% of facial palsies |
| Sarcoidosis | Bilateral facial palsy, uveoparotid fever (Heerfordt syndrome), elevated ACE, hilar adenopathy on CXR |
| Guillain-Barré syndrome | Bilateral facial palsy, ascending weakness, areflexia, CSF albuminocytologic dissociation |
| Acoustic neuroma / CPA tumor | Slowly progressive palsy, associated hearing loss, no pain behind ear |
| Parotid malignancy | Progressive, painless, no retroauricular pain, mass palpable |
| HIV seroconversion | Risk history, CSF pleocytosis |
| Melkersson-Rosenthal syndrome | Recurrent facial palsy + facial/lip edema + fissured tongue |
| Diabetes mellitus / Hypertension | Risk factor associations |
| Leprosy | Endemic areas, thickened nerve, skin patches |
- Harrison's 22E, p. 3597-3598; Adams and Victor's 12E, p. 1372
Investigations
For typical Bell's palsy with classic presentation and no red flags, the diagnosis is clinical and no investigations are routinely required.
Criteria for clinical diagnosis (all must be met):
- Typical abrupt presentation
- No risk factors or symptoms suggesting another cause
- No vesicles in external ear canal (rules out Ramsay Hunt)
- Normal neurological examination apart from CN VII
Investigations in atypical cases:
- Blood glucose / HbA1c (diabetes)
- ESR / CRP (inflammatory)
- Lyme serology (endemic areas)
- HIV serology
- ACE level + chest imaging (sarcoidosis)
- CSF analysis if Guillain-Barré suspected
- MRI with gadolinium (shows facial nerve enhancement and swelling; excludes mass lesion)
EMG (Electromyography):
- Performed after day 10 if prognosis unclear
- Evidence of denervation after 10 days = axonal degeneration = delayed recovery (months), possibly incomplete
- Incomplete paralysis in the first week = most favorable prognostic sign
Prognosis
- ~80-85% of patients recover near-normal function within weeks to months
- 70% recover completely within 1-2 months
- Recovery of taste in the first week is a good prognostic sign
- Early motor recovery in first 5-7 days = best prognostic sign
- Severe denervation on EMG after 10 days = poor prognosis; regeneration takes months to years and may be incomplete
- Recurrence: ~7-8%, average interval 10 years
- Harrison's 22E, p. 3597; Adams and Victor's 12E, p. 1371
Treatment
1. Eye Care (All Patients - Mandatory)
- Artificial tears during waking hours
- Paper tape / eye pad to keep eyelid closed during sleep (prevent corneal drying and exposure keratopathy)
- Lubricating eye ointment at night
- Sunglasses to protect from wind/dust
2. Corticosteroids (Mainstay of Treatment)
- Prednisone 60-80 mg/day for the first 5 days, then tapered over the next 5 days (total 10-day course)
- Must be started as early as possible (ideally within 72 hours of onset)
- Mechanism: reduces inflammation and swelling of the nerve within the tight facial canal
- Evidence: Shown to modestly shorten recovery and improve functional outcome in randomized controlled trials
3. Antiviral Agents
- Valacyclovir 1000 mg/day for 5-7 days OR Acyclovir 400 mg five times daily for 10 days
- Large controlled trials found no added benefit of antivirals over steroids alone for routine Bell's palsy
- Indication: Use antivirals if vesicular lesions are seen (suggests Ramsay Hunt) or in patients with complete facial palsy where some evidence suggests additive benefit
- Ramsay Hunt syndrome: Antivirals are standard and required
4. Physiotherapy
- Facial muscle massage for weakened muscles
- Mime therapy / neuromuscular retraining in recovery phase
- Recent systematic reviews (2025) support physical therapy for idiopathic facial paralysis
5. Surgical Decompression
- Not recommended - no evidence of benefit, may be harmful
- Cosmetic procedures (e.g., gold weight implant in eyelid, muscle transfer, botulinum toxin) for permanent paralysis as a residual complication
Special Population: Pregnancy
- Bell's palsy is 2-4 times more common in late pregnancy and puerperium (peaks ~35 weeks)
- Prednisone 1 mg/kg for 5 days tapered over 10 days - considered safest if avoided in first trimester
- Antivirals: individually low risk but combination not adequately tested in pregnancy
- Eye patching and lubricating drops are safe
- Harrison's 22E, p. 3598; Adams and Victor's 12E, p. 1372; Creasy & Resnik's Maternal-Fetal Medicine
Complications
| Complication | Description |
|---|---|
| Corneal exposure keratopathy | Lagophthalmos + dry eye -> corneal ulceration if not protected |
| Incomplete recovery | ~15% have residual weakness |
| Synkinesis | Aberrant nerve regeneration - involuntary co-movement (e.g., eye closes when smiling) |
| Hemifacial spasm | Sequela of Bell's palsy - irregular involuntary contractions; can be treated with botulinum toxin |
| Crocodile tears (gustatory lacrimation) | Aberrant regeneration of autonomic fibers - tearing when eating |
| Recurrence | ~7-8%; may represent reactivation of latent herpes virus |
Summary Table
| Feature | Bell's Palsy |
|---|---|
| Nerve affected | CN VII (facial nerve) |
| Type of palsy | Peripheral (LMN) |
| Laterality | Unilateral |
| Forehead involvement | Yes (distinguishes from UMN) |
| Primary cause | HSV-1 reactivation (geniculate ganglion) |
| Onset | Abrupt, maximal in 48-72 h |
| Prognosis | ~80-85% near-complete recovery |
| First-line treatment | Prednisone (60-80 mg/d x 5 days, taper x 5 days) |
| Eye protection | Mandatory (artificial tears, eyelid taping) |
| Antivirals | Only if vesicular rash or complete palsy |
| Surgery | Not recommended |
Recent evidence note: A 2025 systematic review (Varelas et al., PMID 39647183) supports physical therapy for idiopathic facial paralysis. Laser/photobiomodulation therapy has been evaluated in recent systematic reviews (Lin et al., 2024, PMID 39546047) with promising but inconclusive results - standard corticosteroid therapy remains the cornerstone of management.
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Adams and Victor's Principles of Neurology 12E | Creasy & Resnik's Maternal-Fetal Medicine | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.