Brachial artery long answer with clinical correlations
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full long answer.
The Brachial Artery - A Comprehensive Long Answer with Clinical Correlations
1. Introduction
The brachial artery is the principal arterial trunk of the arm. It is the direct continuation of the axillary artery and provides the entire blood supply to the arm, before terminating in the cubital fossa by dividing into the radial and ulnar arteries.
2. Origin
The brachial artery begins at the inferior border of teres major muscle, where the axillary artery becomes the brachial artery. This transition occurs deep and medial to the median nerve.
"The brachial artery is the major arterial supply to the arm and is the continuation of the axillary artery at the inferior margin of the teres major, deep and medial to the median nerve."
- Imaging Anatomy, Vol. 3
3. Course and Relations
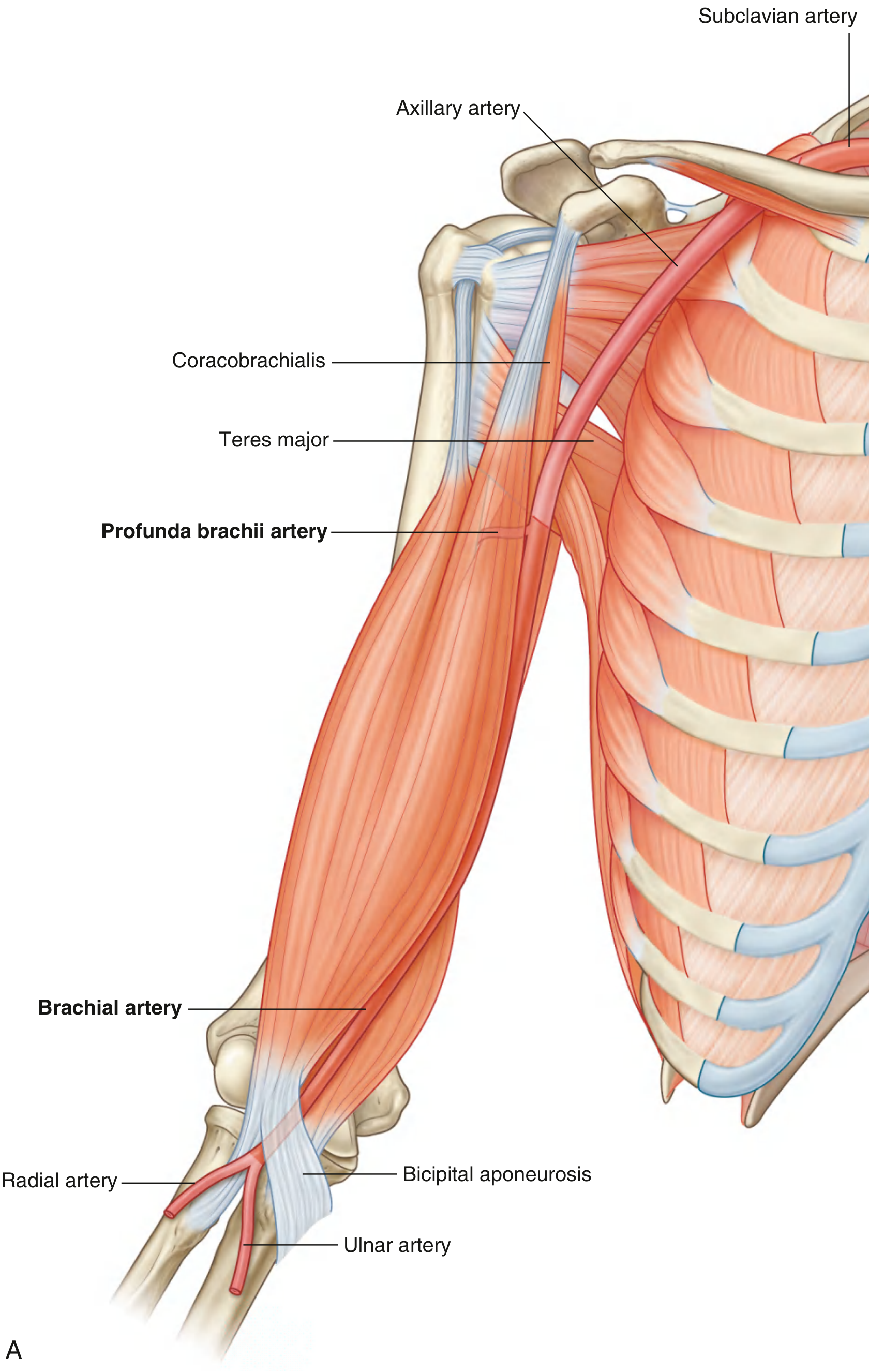
Fig. 7.66A - Brachial artery in context (Gray's Anatomy for Students)
The brachial artery runs in the anterior compartment of the arm. Its course can be described in three segments:
Proximal arm
- Lies on the medial side of the arm, in the medial bicipital groove
- Rests on the medial head of the triceps, then on the coracobrachialis, and finally on the brachialis muscle
- The median nerve lies lateral to the artery at first, then crosses anterior to it at mid-arm to lie medial distally
- The ulnar nerve lies medial initially but deviates posteriorly at mid-arm level, passing posterior to the medial epicondyle (and does NOT pass through the cubital fossa)
- The basilic vein lies parallel to the artery medially
- Paired brachial veins accompany the artery on each side
Distal arm
- Moves anteriorly and laterally to assume a position midway between the medial and lateral epicondyles
- Can be compressed against the medial side of the humerus in the proximal arm
- Lies in the cleft between the biceps brachii and triceps brachii muscles (palpable along its full length)
Cubital fossa
- Enters beneath the bicipital aponeurosis (lacertus fibrosus)
- Lies medial to the biceps tendon and lateral to the median nerve
- The aponeurosis covers and protects both the brachial artery and median nerve
- Terminates at the apex of the cubital fossa by dividing into radial and ulnar arteries at the level of the neck of the radius
"In the proximal arm, the brachial artery lies on the medial side. In the distal arm, it moves laterally to assume a position midway between the lateral epicondyle and the medial epicondyle of the humerus." - Gray's Anatomy for Students
4. Termination
The brachial artery bifurcates into the radial and ulnar arteries at the apex of the cubital fossa, at the level of the neck of the radius (approximately opposite the radial head). This bifurcation normally occurs within the cubital fossa, though in anatomical variants it may occur much higher - even in the axilla.
5. Branches
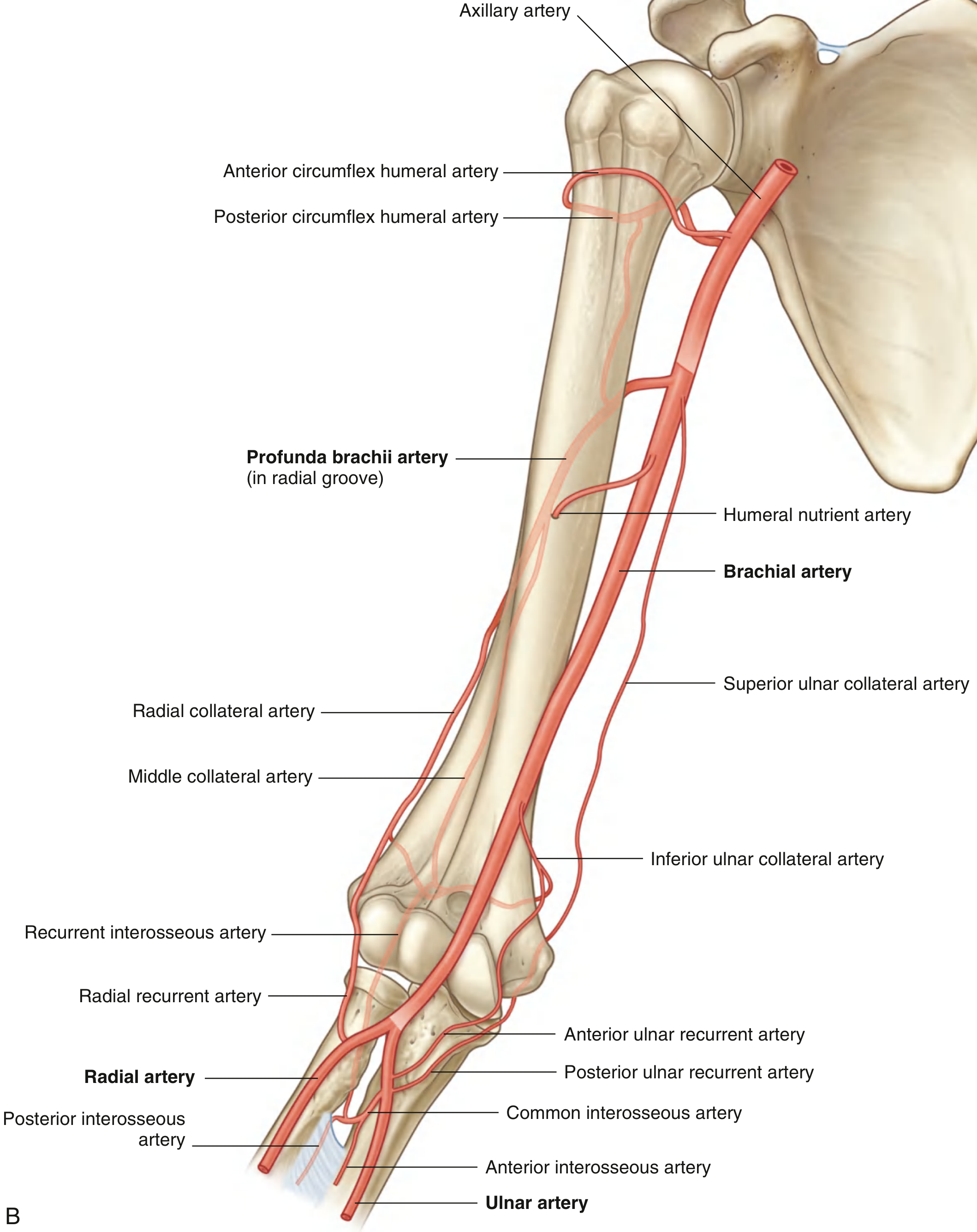
Fig. 7.66B - Branches of the brachial artery (Gray's Anatomy for Students)
(a) Profunda Brachii Artery (Deep Artery of the Arm)
- The largest branch of the brachial artery
- Arises near the origin of the brachial artery, just below the inferior border of teres major
- Passes with the radial nerve through the triangular interval (bounded by the shaft of the humerus, inferior margin of teres major, and lateral margin of the long head of triceps)
- Winds around the posterior surface of the humerus in the radial (spiral) groove, deep to the lateral head of triceps
- Terminates as two collateral vessels:
- Radial collateral artery - anastomoses with the radial recurrent artery
- Middle (medial) collateral artery - anastomoses with the recurrent interosseous artery
(b) Superior Ulnar Collateral Artery
- Arises distal to the origin of the profunda brachii
- Accompanies (runs alongside) the ulnar nerve as it passes posterior to the medial epicondyle
- Anastomoses with the inferior ulnar collateral and posterior ulnar recurrent arteries
(c) Inferior Ulnar Collateral Artery
- Arises above the medial epicondyle
- Anastomoses with the anterior ulnar recurrent artery
(d) Muscular Branches
- Numerous branches to the muscles of the anterior compartment (coracobrachialis, biceps brachii, brachialis)
(e) Nutrient Artery to the Humerus
- Enters through a foramen in the anteromedial surface of the humeral shaft
6. The Cubital (Periarticular Elbow) Anastomosis
This is a rich network of arteries encircling the elbow joint, allowing collateral circulation if the brachial artery is ligated distal to the origin of the profunda brachii.
| Descending vessels (from brachial/profunda) | Ascending vessels (from radial/ulnar) |
|---|---|
| Superior ulnar collateral artery | Anterior ulnar recurrent artery |
| Inferior ulnar collateral artery | Posterior ulnar recurrent artery |
| Radial collateral artery | Radial recurrent artery |
| Middle collateral artery | Recurrent interosseous artery |
"The cubital anastomosis permits ligature of the brachial artery distal to the origin of the deep artery of the arm." - Color Atlas of Human Anatomy, Vol. 2
7. Surface Marking
- A line drawn from the apex of the axilla (arm slightly abducted) to the midpoint between medial and lateral epicondyles of the humerus represents the surface marking of the brachial artery.
- The artery is palpable along this entire course in the medial bicipital groove.
- Pulse point: Easily palpated in the medial bicipital groove, proximal arm, and in the cubital fossa.
8. Anatomical Variations
In approximately 20% of individuals, the brachial artery gives off a superficial brachial artery that courses superficial to (instead of deep to) the median nerve. Three types are recognized (Yang classification):
- Type I: The superficial brachial is dominant and divides into radial and ulnar arteries
- Type II: It runs parallel to the deep brachial artery and continues as the radial artery in the forearm
- Type III: It joins the brachial artery distally
This is clinically important because the superficial course makes it more vulnerable to injury during procedures and venepuncture.
Other recognized variants include a high division of the brachial artery (bifurcation in the arm or axilla) and a duplicated brachial artery.
"In approximately 20% of individuals the brachial artery gives off a superficial brachial artery that courses inferiorly superficial to the median nerve; it can be a high-branching radial artery (10%), high-branching ulnar artery (3%), or divide into radial and ulnar arteries (7%)" - Fischer's Mastery of Surgery, 8th ed.
9. Clinical Correlations
9.1 Blood Pressure Measurement
The brachial artery is the standard site for blood pressure measurement. A sphygmomanometer cuff is applied around the mid-arm, compressing the brachial artery against the humerus. A stethoscope is placed over the brachial artery in the cubital fossa to auscultate Korotkoff sounds:
- When cuff pressure falls just below systolic pressure: sounds appear (systolic reading)
- When cuff pressure falls below diastolic pressure: sounds disappear (diastolic reading)
Normal range: 90-120 mmHg systolic / 60-80 mmHg diastolic.
"The sphygmomanometer is a device that inflates a cuff around the midportion of the arm to compress the brachial artery against the humerus." - Gray's Anatomy for Students
9.2 Brachial Artery Puncture and Cannulation
The brachial artery is used for:
- Arterial blood gas sampling
- Cardiac catheterization (Sones technique - brachial cutdown approach)
- Invasive blood pressure monitoring
The preferred site is at or just proximal to the antecubital fossa. However, the brachial artery is less preferred than the radial or axillary artery because:
- It lacks adequate collateral circulation (unlike the dual supply at the wrist)
- Risk of ischemic complications to the hand if thrombosis occurs
- Requires the arm to be extended, limiting mobility
- A longer catheter (10 cm) is required to traverse the elbow joint
"Although it appears safe for arterial puncture, the brachial artery does not have the anatomic benefit of the collateral circulation that is found in the wrist." - Roberts and Hedges' Clinical Procedures in Emergency Medicine
9.3 Supracondylar Fracture of the Humerus and Brachial Artery Injury
This is the most important clinical correlation of the brachial artery and a classic exam topic.
Mechanism: In a displaced (extension-type) supracondylar fracture in a child, the distal humeral fragment is pulled posteriorly by the triceps muscle. This posterior displacement effectively "bowstrings" the brachial artery over the sharp, irregular proximal fracture fragment, stretching or lacerating it.
Consequences:
- Arterial spasm, thrombosis, or laceration
- Anterior compartment ischemia of the forearm
- If untreated: muscle necrosis replaced by fibrous tissue = Volkmann's Ischemic Contracture
Signs of impending ischemia (the 5 P's):
- Pain - especially with passive finger extension
- Pallor of the hand and forearm
- Pulselessness - absent radial pulse
- Paraesthesia - tingling in the hand
- Paralysis - inability to extend fingers/wrist
"The most serious complication is a compartment syndrome of the forearm, also known as Volkmann's ischemic contracture. This classically occurs following a displaced supracondylar fracture. Post-ischemic swelling increases pressure within the enclosed osteofascial forearm compartment..." - Tintinalli's Emergency Medicine
Management:
- Urgent reduction of the fracture
- If ischemia persists after reduction: emergency surgical exploration of the brachial artery
- Fasciotomy for compartment syndrome
9.4 Volkmann's Ischemic Contracture
The end-stage result of untreated brachial artery injury or forearm compartment syndrome.
- Post-ischemic muscle necrosis of the flexor compartment of the forearm
- Replaced by inelastic fibrotic tissue
- Produces a characteristic flexion contracture of the wrist and fingers with pronation of the forearm
- The median nerve is also compromised (the key nerve and artery involved)
- Prevention: early recognition and treatment is essential - "Extremities with signs of ischemia require emergency orthopedic consultation" (Tintinalli's Emergency Medicine)
9.5 Brachial Artery Injuries
The brachial artery accounts for 14-30% of all arterial injuries and up to 60% of upper extremity arterial injuries. Causes include:
- Penetrating trauma (stab/gunshot wounds)
- Blunt trauma with fracture/dislocation
- Iatrogenic (cardiac catheterization, IV drug injection)
Key surgical considerations (Fischer's Mastery of Surgery):
- Proximal control by compressing the brachial artery against the humerus
- Access via longitudinal incision in the medial bicipital groove
- The median nerve crosses from lateral to medial in the distal arm - must be identified and protected
- Injuries proximal to the profunda brachii origin will compromise collateral circulation and are more likely to cause critical ischemia
- Injuries distal to the profunda brachii origin may be tolerated due to collateral flow
- Always check radial and ulnar pulses by palpation and Doppler before and after repair
9.6 Brachial Artery in the Cubital Fossa - Surgical Significance
The bicipital aponeurosis (lacertus fibrosus) plays a protective and surgical role:
- It covers the brachial artery and median nerve in the distal cubital fossa
- Separates the median cubital vein (used for venepuncture) from these deeper vital structures
- Must be divided when surgically exposing the brachial artery distally
- The aponeurosis prevents laceration of the brachial artery during routine venepuncture at the cubital fossa
9.7 Brachioradialis Arteriovenous Fistula (for Dialysis)
A brachio-cephalic AV fistula is created by anastomosing the cephalic vein to the brachial artery at the antecubital fossa. It is used when a radiocephalic fistula is not feasible. The brachial artery's superficial position in the cubital fossa makes this anastomosis surgically accessible.
9.8 Blood Pressure Discrepancy (Differential Brachial Pressure)
A significant pressure difference (>10-15 mmHg) between the two arms suggests:
- Subclavian artery stenosis (proximal to the brachial artery origin)
- Aortic dissection
- Thoracic outlet syndrome
- Atherosclerotic disease
10. Summary Table
| Feature | Detail |
|---|---|
| Origin | Continuation of axillary artery at inferior border of teres major |
| Termination | Bifurcation into radial and ulnar arteries at apex of cubital fossa (neck of radius) |
| Surface marking | Apex of axilla to midpoint between medial and lateral epicondyles |
| Largest branch | Profunda brachii (deep brachial) artery |
| Accompanies | Median nerve (crosses from lateral to medial at mid-arm) |
| Pulse site | Medial bicipital groove; cubital fossa |
| BP measurement | Sphygmomanometer cuff + stethoscope over brachial artery |
| Key clinical hazard | Supracondylar fracture → ischemia → Volkmann's contracture |
| Collateral pathway | Cubital anastomosis (via profunda brachii + recurrent vessels) |
| Safe ligation site | Distal to origin of profunda brachii (collaterals maintain perfusion) |
| Common variation | Superficial brachial artery (~20%) - superficial to median nerve |
Sources: Gray's Anatomy for Students; Imaging Anatomy Vol. 3; Fischer's Mastery of Surgery 8th ed.; Color Atlas of Human Anatomy Vol. 2; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Tintinalli's Emergency Medicine; S. Das Manual on Clinical Surgery 13th ed.; Campbell's Operative Orthopaedics 15th ed.
This is a shared conversation. Sign in to Orris to start your own chat.