sexual disease in detailed way with image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have excellent clinical images and comprehensive content. Let me write the full detailed answer.
Sexually Transmitted Infections (STIs) - A Comprehensive Overview
Sexually transmitted infections (STIs) are caused by organisms transmitted through intimate contact involving the skin or mucosal surfaces of the oropharynx, vagina, penis, and rectum. They are among the most common infections worldwide. Many are subclinical yet still transmissible - meaning a person can spread infection without knowing they are infected.
The spread of any STI depends on: B (efficiency of transmission) x D (duration of infectiousness) x C (number of sexual partners) = R₀ (basic reproductive rate).
Classification of STIs by Syndrome
| Syndrome | Causative Organism(s) |
|---|---|
| Urethritis (gonococcal) | Neisseria gonorrhoeae |
| Urethritis (non-gonococcal) | Chlamydia trachomatis, Mycoplasma genitalium, Trichomonas vaginalis |
| Genital ulcers | HSV (herpes), T. pallidum (syphilis), H. ducreyi (chancroid) |
| Lymphogranuloma venereum | Chlamydia trachomatis (serovars L1, L2, L3) |
| Genital warts / cervical cancer | Human papillomavirus (HPV) |
| Vaginal discharge | T. vaginalis, Gardnerella, Candida |
| Pelvic inflammatory disease | N. gonorrhoeae, C. trachomatis |
| Ectoparasites | Pthirus pubis (pubic lice), Sarcoptes scabiei (scabies) |
- Goldman-Cecil Medicine, Table 264-1
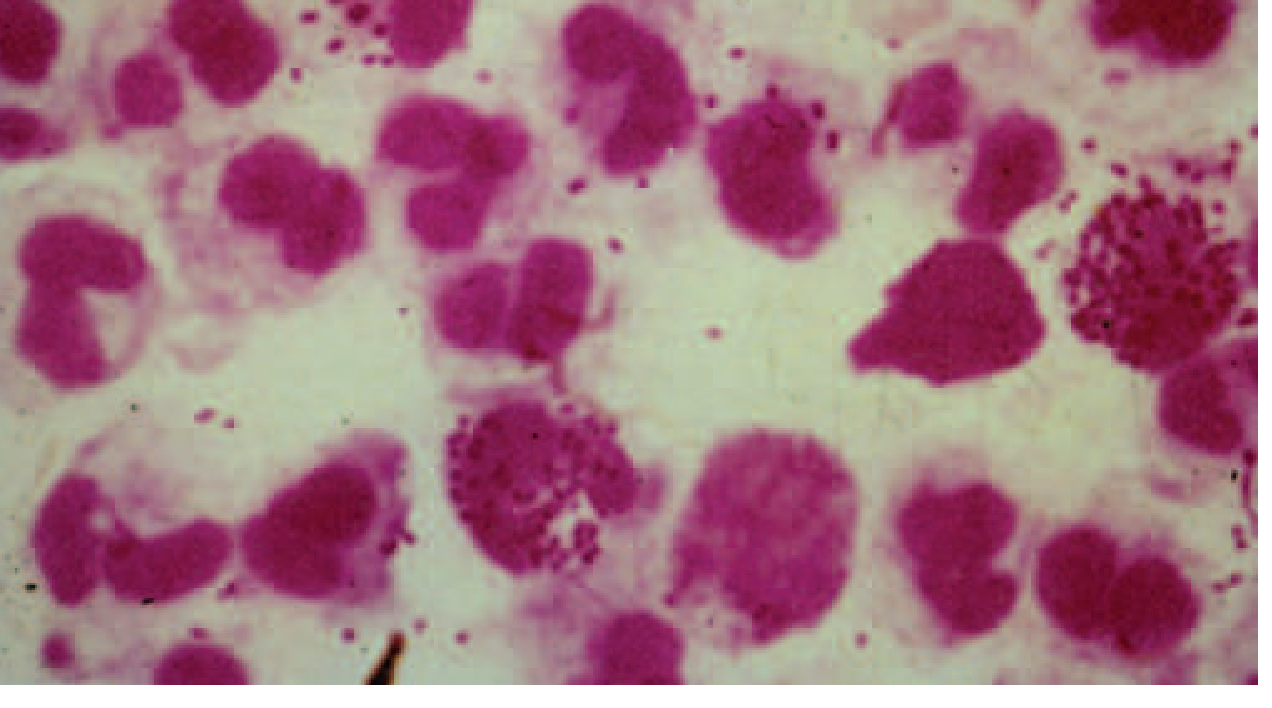
1. Gonorrhea (Neisseria gonorrhoeae)
Pathogen: Gram-negative intracellular diplococcus.
Epidemiology: Overall rate ~150 cases per 100,000 in women; rates in men and women ages 20-24 approach 750 per 100,000. Gonococcal infection of the cervix occurs in about 1% of pregnant women.
Clinical Features:
- Men: Acute urethritis is the most common presentation. Incubation period is 2-7 days. Discharge begins scant and mucoid then becomes profuse and purulent. Dysuria without urinary frequency is typical. Asymptomatic men are a major reservoir of spread.
- Women: Mucopurulent cervicitis, vaginal discharge, dysuria. In the first trimester, ascending infection can cause salpingitis. Disseminated gonococcal infection (arthritis, skin lesions) is more common in pregnant women due to elevated progesterone and increased cervical vascularity.
- Complications: Epididymitis, pelvic inflammatory disease, disseminated gonococcal arthritis, neonatal gonococcal ophthalmia and sepsis.
Diagnosis: Gram stain of urethral discharge showing gram-negative intracellular diplococci within PMNs (see image below); NAAT is the gold standard.
Treatment:
- Ceftriaxone 250 mg IM (single dose); always treat for possible co-existent chlamydia.
- Resistance to azithromycin and cephalosporins is an emerging global concern.
- Harrison's Principles of Internal Medicine 22e; Rosen's Emergency Medicine
2. Chlamydia (Chlamydia trachomatis)
Pathogen: Obligate intracellular bacterium. Most common bacterial STI in the US - prevalence is 3-5 times that of gonorrhea.
Clinical Features:
- Men: Urethritis with mild, watery or mucoid discharge (much less intense than gonorrhea) or completely asymptomatic.
- Women: Cervicitis (often asymptomatic), urethritis, pelvic inflammatory disease, postpartum endometritis, preterm labor in pregnancy.
- Neonates of infected mothers: Conjunctivitis and pneumonitis.
- Lymphogranuloma venereum (LGV): Caused by serovars L1-L3 - painless genital ulcer followed by massive inguinal lymphadenopathy (buboes).
Diagnosis: NAAT on urine or endocervical/urethral swab.
Treatment:
- Standard: Azithromycin 1 g orally (single dose) OR doxycycline 100 mg twice daily x 7 days.
- Pregnancy: Azithromycin 1 g (single dose); amoxicillin 500 mg TID x 7 days is an alternative.
- LGV: Doxycycline 100 mg twice daily x 21 days.
- Rosen's Emergency Medicine; Goldman-Cecil Medicine
3. Syphilis (Treponema pallidum)
Pathogen: A delicate, spiral spirochete 5-20 μm in length with 4-14 spiral coils. It is actively motile, showing rotation, forward movement, and side-to-side bending. It cannot be cultured in vitro and is highly sensitive to temperature. An estimated 12 million people are infected annually worldwide.
Epidemiology: Primary and secondary syphilis rates have increased every year since 2000. Rates in women increased ~150% from 2016-2020; congenital syphilis increased 250% in the same period. Men who have sex with men account for ~60% of male syphilis cases.
Stages of Syphilis
Primary Syphilis:
- Painless, indurated ulcer (chancre) at the inoculation site, appearing 10-90 days after exposure.
- The risk of transmission from a single sexual contact is 16-30%.
- Heals spontaneously in 3-6 weeks even without treatment.
- Diagnosed by dark-field microscopy (finding motile spirochetes) or serologic testing.

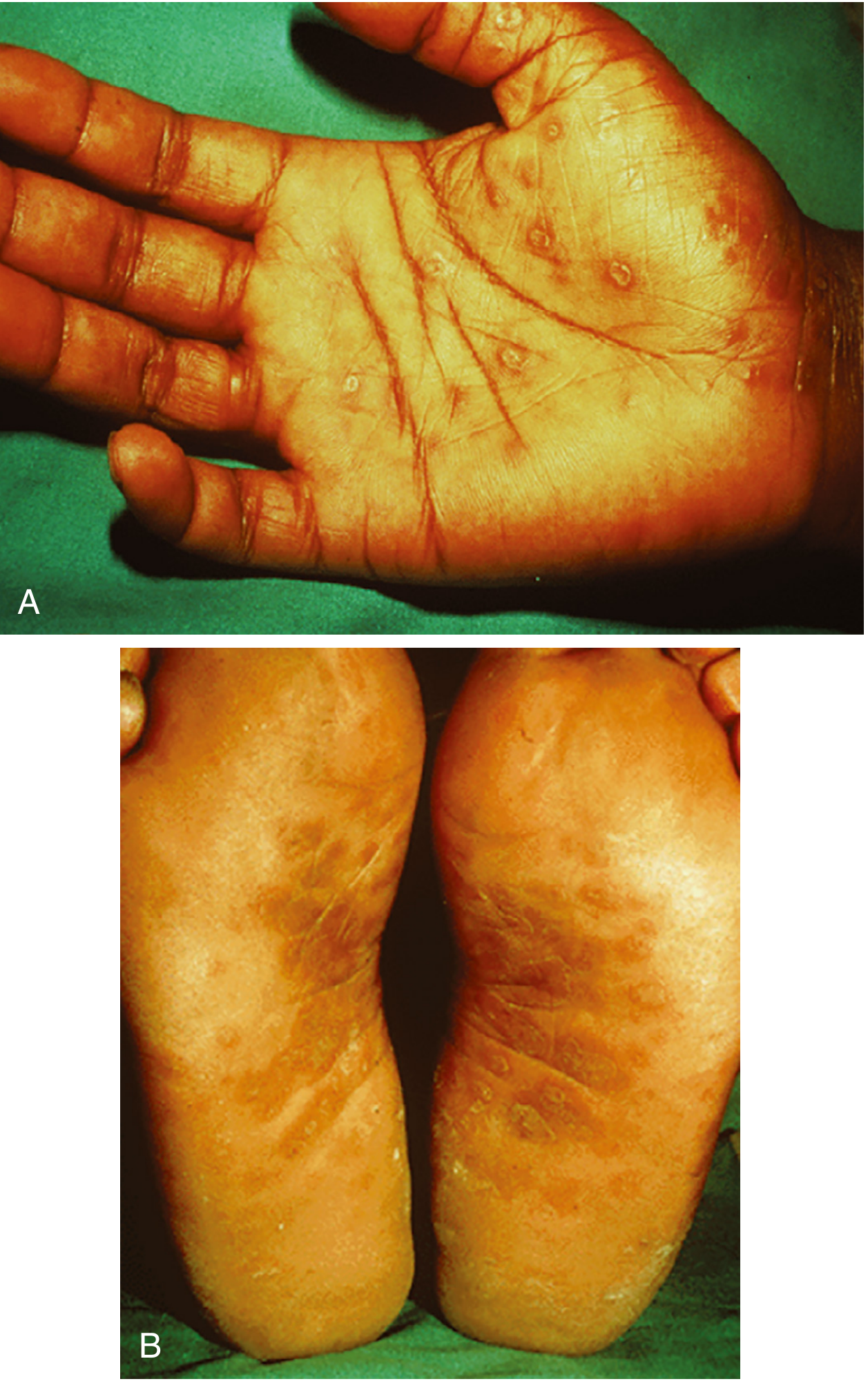
Secondary Syphilis:
- Appears 2-10 weeks after the chancre resolves when spirochetes spread systemically.
- Characteristic maculopapular rash involving palms and soles (highly pathognomonic), face, trunk, and extremities.
- Also causes: mucous patches, condyloma lata (broad moist papules on genitalia), generalized non-tender lymphadenopathy, "moth-eaten" alopecia.
- Systemic symptoms: low-grade fever, malaise, myalgias, headache.
- These mucocutaneous lesions are highly contagious.

Latent Syphilis:
- No clinical manifestations. Early latent = within 12 months; late latent = beyond 12 months.
- Patient is not contagious by sexual transmission in late latent stage, but can still transmit transplacentally.
Tertiary Syphilis: (~1/3 of untreated cases)
- Gummas: Granulomatous lesions of skin, bone, liver.
- Cardiovascular: Aortitis, aortic aneurysm, aortic insufficiency.
- Neurosyphilis: General paresis, tabes dorsalis, Argyll Robertson pupil (accommodates but doesn't react to light - virtually pathognomonic), meningovascular disease, optic atrophy.
Congenital Syphilis: Stillbirth, neonatal death, non-immune hydrops, hepatosplenomegaly, skin lesions. Placental transmission occurs predominantly in the second and third trimesters.
Diagnosis: Non-treponemal tests (RPR, VDRL) + treponemal tests (FTA-ABS, TPPA). Dark-field microscopy for primary lesion exudate.
Treatment:
- Primary/secondary: Benzathine penicillin G 2.4 million units IM single dose.
- Late latent: Benzathine penicillin G 2.4 million units IM x 3 weekly doses (7.2 million units total).
- Neurosyphilis: Aqueous crystalline penicillin G IV x 10-14 days.
- Andrews' Diseases of the Skin; Rosen's Emergency Medicine; Creasy & Resnik's Maternal-Fetal Medicine
4. Genital Herpes (HSV-1 and HSV-2)
Pathogen: Herpes simplex virus - two types: HSV-1 (classically orofacial) and HSV-2 (classically genital). HSV-1 is now an increasingly common cause of genital herpes in young women in the USA. Genital herpes is the most prevalent STI worldwide and the most common cause of ulcerative genital disease.
Epidemiology: HSV-2 antibodies are found in ~12% of Americans aged 14-49. About 35% of non-Hispanic Black Americans are HSV-2 seropositive vs. ~8% of non-Hispanic Whites. Women (16%) are more often seropositive than men (8%). Genital herpes is an important risk factor for acquisition and transmission of HIV.
Clinical Presentations:
- Primary episode (no pre-existing immunity): Severe local symptoms - multiple painful vesicles/ulcers on genitalia or perianal area, fever, malaise, myalgia, inguinal lymphadenopathy. Lasts 2-3 weeks.
- Non-primary first episode (partial immunity): Less severe.
- Recurrent episodes: Generally milder, shorter. Often preceded by a prodrome of tingling/burning.
- Asymptomatic shedding: Most transmissions occur during asymptomatic shedding. Most recurrences are not recognized by the patient.
Complications: Neonatal herpes (disseminated or CNS disease with high morbidity/mortality), HSV encephalitis, keratitis. Women with genital herpes in the third trimester have a 30-50% risk of neonatal transmission vs. 1% in first trimester.
Diagnosis: PCR (most sensitive), viral culture, or type-specific serology (IgG).
Treatment:
- First episode: Acyclovir 400 mg TID x 7-10 days OR valacyclovir 1 g BID x 7-10 days.
- Recurrence: Valacyclovir 500 mg BID x 3-5 days.
- Suppressive therapy: Valacyclovir 1 g daily (reduces frequency of outbreaks and risk of transmission).
- Fitzpatrick's Dermatology; Goldman-Cecil Medicine
5. Human Papillomavirus (HPV)
Pathogen: Double-stranded DNA virus; >100 types identified; ~35-40 primarily infect the genital tract. HPV is the most common sexually transmitted infection overall.
Classification:
- Low-risk types (6, 11, 42, 43, 44): Associated primarily with genital warts (condyloma acuminatum). About 1% of sexually active adults are diagnosed with genital warts annually.
- High-risk types (16, 18, 31, 45, and others): Associated with cervical, anal, oropharyngeal, vulvar, vaginal, and penile cancers. HPV types 16 and 18 account for ~70% of cervical cancers.
Epidemiology: 75% of new HPV infections occur in those aged 15-24. Transmission rate is ~65% among sex partners. Risk factors include: early onset of sexual activity, multiple partners, failure to use condoms, smoking, and immunosuppression.
Clinical Features:
- Most HPV infections (majority) are asymptomatic and self-limiting.
- Condyloma acuminata: soft, skin-colored or pink, cauliflower-like growths on the genitalia, perineum, and perianal area.
- High-risk types cause high-grade squamous intraepithelial neoplasia (CIN) and invasive cervical cancer.
- Laryngeal papillomatosis (caused by HPV 6 and 11) - rare but serious in neonates born to infected mothers.
Diagnosis: Clinical examination for warts; Pap smear + HPV DNA testing for cervical dysplasia; colposcopy and biopsy for high-grade lesions.
Treatment:
- Genital warts: Patient-applied (podophyllotoxin, imiquimod) or provider-applied (trichloroacetic acid, cryotherapy, surgical removal).
- No antiviral drug eliminates HPV itself; treatment targets lesions.
Prevention - Vaccines:
- Gardasil 9 covers HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58. Recommended for all persons through age 26; shared decision-making for ages 27-45.
- Goldman-Cecil Medicine; Creasy & Resnik's Maternal-Fetal Medicine
6. Trichomoniasis (Trichomonas vaginalis)
- The annual global incidence exceeds that of chlamydia and gonorrhea combined.
- Symptoms (women): Purulent, frothy yellow-green vaginal discharge; vulvar irritation; elevated vaginal pH. Pathognomonic finding: "strawberry cervix" (colpitis macularis - punctate microhemorrhages of the ectocervix).
- Men: Usually asymptomatic; may cause urethritis.
- Diagnosis: NAAT (most sensitive); wet mount (motile protozoa with flagella visible).
- Treatment: Metronidazole 500 mg twice daily x 7 days (preferred in women) or 2 g single dose; tinidazole 2 g single dose. Treat sexual partners.
7. Bacterial Vaginosis (BV)
- Caused by overgrowth of Gardnerella vaginalis and anaerobes replacing normal Lactobacillus flora.
- Symptoms: Thin, gray-white discharge with fishy odor; no significant inflammation.
- Diagnosis: Clue cells on wet mount, elevated vaginal pH >4.5, positive whiff test (10% KOH), Amsel's criteria.
- Treatment: Metronidazole 500 mg BID x 7 days or metronidazole gel 0.75% intravaginally.
8. Chancroid (Haemophilus ducreyi)
- Painful genital ulcer(s) (in contrast to the painless chancre of syphilis) with ragged, undermined edges.
- Associated with painful inguinal lymphadenopathy (tender buboes) in ~50% of cases.
- Treatment: Azithromycin 1 g orally single dose OR ceftriaxone 250 mg IM single dose.
General Principles of STI Management
Diagnosis approach:
- Syndromic approach: Empiric treatment based on signs/symptoms - used in resource-limited settings.
- Microbiologic approach: NAAT, culture, and serology - preferred in developed countries; allows resistance monitoring and public health reporting.
Every patient with an STI should be:
- Screened for HIV (early diagnosis has major personal and public health benefits).
- Screened serologically for syphilis.
- Counseled about partner notification and treatment.
- Offered vaccination (hepatitis A, hepatitis B, HPV where applicable).
Special populations:
- Pregnant women: Tetracyclines and quinolones are contraindicated. Treat chlamydia with azithromycin; gonorrhea with ceftriaxone; herpes with acyclovir/valacyclovir (consultation required); syphilis with penicillin.
- Neonates: At risk for conjunctivitis, pneumonitis (chlamydia), ophthalmia and sepsis (gonorrhea), disseminated herpes, and congenital syphilis.
Summary Table
| Disease | Pathogen | Key Feature | Treatment |
|---|---|---|---|
| Gonorrhea | N. gonorrhoeae | Purulent urethral/cervical discharge | Ceftriaxone IM |
| Chlamydia | C. trachomatis | Mild/no discharge, PID, infertility | Azithromycin or doxycycline |
| Syphilis | T. pallidum | Painless chancre → palmar/plantar rash | Benzathine penicillin G |
| Genital Herpes | HSV-1/2 | Painful vesicles/ulcers, recurrent | Acyclovir/valacyclovir |
| HPV | Human papillomavirus | Genital warts, cervical cancer | Topical agents; vaccine |
| Trichomoniasis | T. vaginalis | Frothy discharge, strawberry cervix | Metronidazole |
| Chancroid | H. ducreyi | Painful ulcer + tender bubo | Azithromycin or ceftriaxone |
Sources: Goldman-Cecil Medicine 2-Vol Set; Harrison's Principles of Internal Medicine 22e; Rosen's Emergency Medicine; Andrews' Diseases of the Skin; Fitzpatrick's Dermatology; Creasy & Resnik's Maternal-Fetal Medicine; Washington Manual of Medical Therapeutics - treatment regimens per CDC STI Guidelines 2021.
This is a shared conversation. Sign in to Orris to start your own chat.