IBS
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"irritable bowel syndrome"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough answer on IBS diagnosis. Let me compile the complete response.
IBS: Diagnosis & Investigations
Source: Goldman-Cecil Medicine, Chapter 123
Definition
IBS is a functional bowel disorder characterized by chronic or recurrent abdominal pain associated with alterations in stool form and/or frequency (diarrhea and/or constipation). It is attributable to the middle or lower GI tract, and functional bowel disorders form a spectrum that can transition from one subtype to another over time.
Rome IV Diagnostic Criteria
Criterion A (required): Recurrent abdominal pain, on average at least 1 day per week in the last 3 months, with symptom onset at least 6 months prior, associated with two or more of the following:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
Criterion B - supportive symptoms (not required but strengthen the diagnosis):
| Symptom |
|---|
| Abnormal stool frequency: ≤3 BM/week or >3 BM/day |
| Abnormal stool form: lumpy/hard or loose/watery |
| Defecation straining |
| Urgency |
| Feeling of incomplete bowel movement |
| Passing mucus |
| Bloating or abdominal distention |
IBS Subtypes (via Bristol Stool Form Scale)
- IBS-C - predominant constipation (~25%)
- IBS-D - predominant diarrhea (~35-40%)
- IBS-M - mixed bowel habits (~35-40%)
- IBS-U - unclassified (<5%)
Subtypes can transition in the same patient over time.
Alarm Features (require further investigation if present)
The following features shift the approach away from a positive IBS diagnosis toward targeted workup:
- New-onset symptoms at age ≥50 years
- Unintentional weight loss
- Hematochezia or melena (not related to hemorrhoids)
- Nocturnal diarrhea
- Anemia
- Palpable abdominal mass or lymphadenopathy
- Family history of colorectal cancer, IBD, or celiac disease
Diagnostic Algorithm
The approach is a positive diagnostic strategy - IBS should be diagnosed on its own merits rather than purely by exclusion:
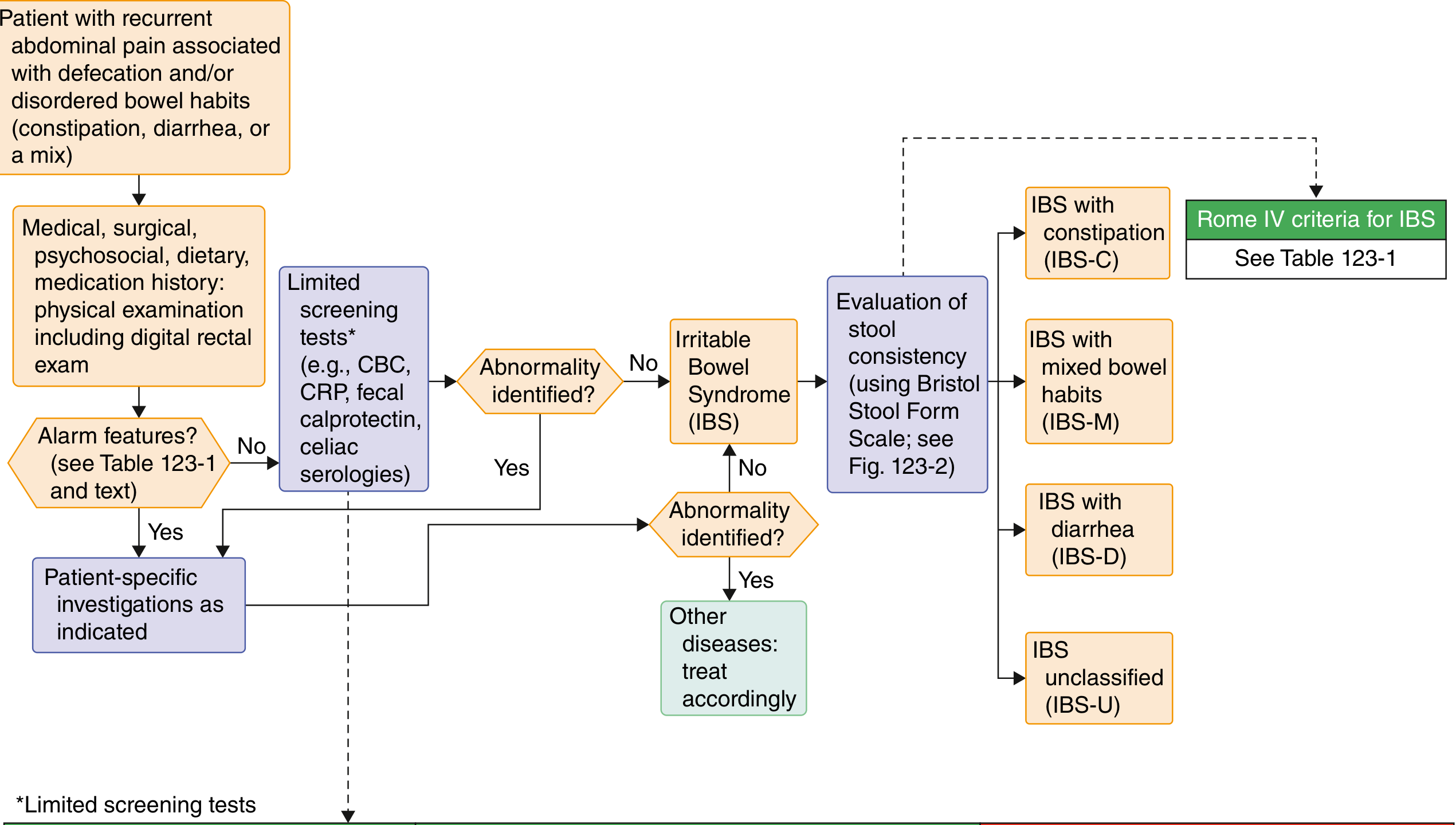
Flow: History + physical exam → check for alarm features → limited screening tests → if no abnormality found and Rome IV criteria met → diagnose IBS → classify subtype by Bristol Stool Form Scale.
Investigations
Generally Recommended
| Test | Population |
|---|---|
| Complete blood count (CBC) | All |
| C-reactive protein (CRP) | All (especially IBS-D) |
| Fecal calprotectin or lactoferrin | All (especially IBS-D) to exclude IBD |
| Celiac serologies (IgA anti-tTG + total IgA) | IBS-D |
| Bile acid diarrhea testing | IBS-D where BAD is suspected |
| Stool Giardia antigen or PCR | IBS-D in endemic areas |
| Stool culture/parasites | Relevant travel history |
| Colonoscopy | New-onset symptoms at age ≥50 years |
| Anorectal physiology testing | Suspected pelvic floor dysfunction or refractory constipation |
Note: In IgA-deficient patients, use serum IgG anti-tTG and/or IgG deaminated gliadin peptide to screen for celiac disease.
NOT Routinely Recommended
| Test | Reason |
|---|---|
| Colonoscopy in age <50 without alarm features | Low yield |
| Routine stool cultures without travel history | Low yield |
| Food allergy or intolerance testing | Not validated |
| Lactose or glucose hydrogen breath testing | Not recommended routinely |
If colonoscopy is performed in diarrheal-predominant IBS, random colon biopsies should be taken to examine for microscopic or collagenous colitis.
Key Diagnostic Principle
IBS is not diagnosed by exclusion alone. A positive diagnostic approach - applying Rome IV criteria combined with targeted limited tests to rule out structural/organic disease - is preferred by current guidelines. Over-investigation with colonoscopy, food allergy panels, and breath tests is neither necessary nor recommended in the absence of alarm features.
- Goldman-Cecil Medicine, Chapter 123 (Lin Chang)
Treatment
Reading File
Searching PubMed
"irritable bowel syndrome"[MeSH Terms] AND "therapeutics"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive treatment answer. Here it is:
IBS: Treatment
Source: Goldman-Cecil Medicine, Chapter 123 (Lin Chang)
Overall Approach
Treatment is stratified by symptom severity:
- Mild - education, reassurance, dietary advice, OTC medications
- Moderate - add pharmacotherapy targeted to predominant symptoms
- Severe / refractory - integrated approach combining pharmacotherapy + behavioral/psychological treatment
Treatment choices are guided by the most bothersome symptom, subtype (IBS-C vs IBS-D), comorbidities, and patient preference.
1. Dietary Therapy (First-Line for All Subtypes)
| Intervention | Evidence/Notes |
|---|---|
| Low-FODMAP diet | First-line; improves global IBS symptoms, especially in IBS-D. Reduces abdominal pain, bloating, and abnormal bowel habits. Best supervised by a trained dietitian. |
| Soluble fiber (psyllium) | 25-35 g/day; most useful in IBS-C. Start low, increase gradually. Soluble (psyllium) recommended; insoluble (wheat bran) is NOT. |
| Gluten-free diet | Less clear benefit; may be tried if gluten consistently triggers symptoms. |
| Food/symptom diary | 1-2 weeks to identify personal trigger foods. |
2. Medications - Active for All Subtypes
Antispasmodics & Peppermint Oil (Pain/Spasm)
| Drug | Dose | Key Side Effects |
|---|---|---|
| Peppermint oil | 1-2 capsules TID or PRN | Heartburn, nausea |
| Hyoscyamine | 0.125 mg TID-QID or PRN | Dry mouth, blurred vision, dizziness, constipation |
| Dicyclomine | 10 mg TID-QID or PRN | Dry mouth, blurred vision, dizziness |
Central Brain-Gut Neuromodulators (Pain)
Used at low doses for their visceral analgesic effects - not necessarily for treating anxiety or depression:
| Drug | Dose | Notes |
|---|---|---|
| Amitriptyline (TCA) | 10-25 mg QHS → up to 100 mg | Sedation, dry mouth; useful in IBS-D (slows transit) |
| Desipramine (TCA) | 10-25 mg QHS → up to 100 mg | Less anticholinergic |
| Nortriptyline (TCA) | 10-25 mg QHS → up to 100 mg | |
| Citalopram (SSRI) | 5-20 mg daily | SSRIs useful in IBS-C (may accelerate transit) |
| Fluoxetine (SSRI) | 20-40 mg daily | Sexual dysfunction, headache, nausea |
| Duloxetine / Venlafaxine (SNRI) | Standard doses | Useful for pain with comorbid anxiety/depression |
Probiotics
Combination probiotic products reduce global IBS symptoms by ~20%. Data from RCTs are mixed. Most useful for patients with persistent bloating. (Recent 2024 network meta-analysis, PMID 38999862 in Nutrients confirms benefit but notes heterogeneity across strains.)
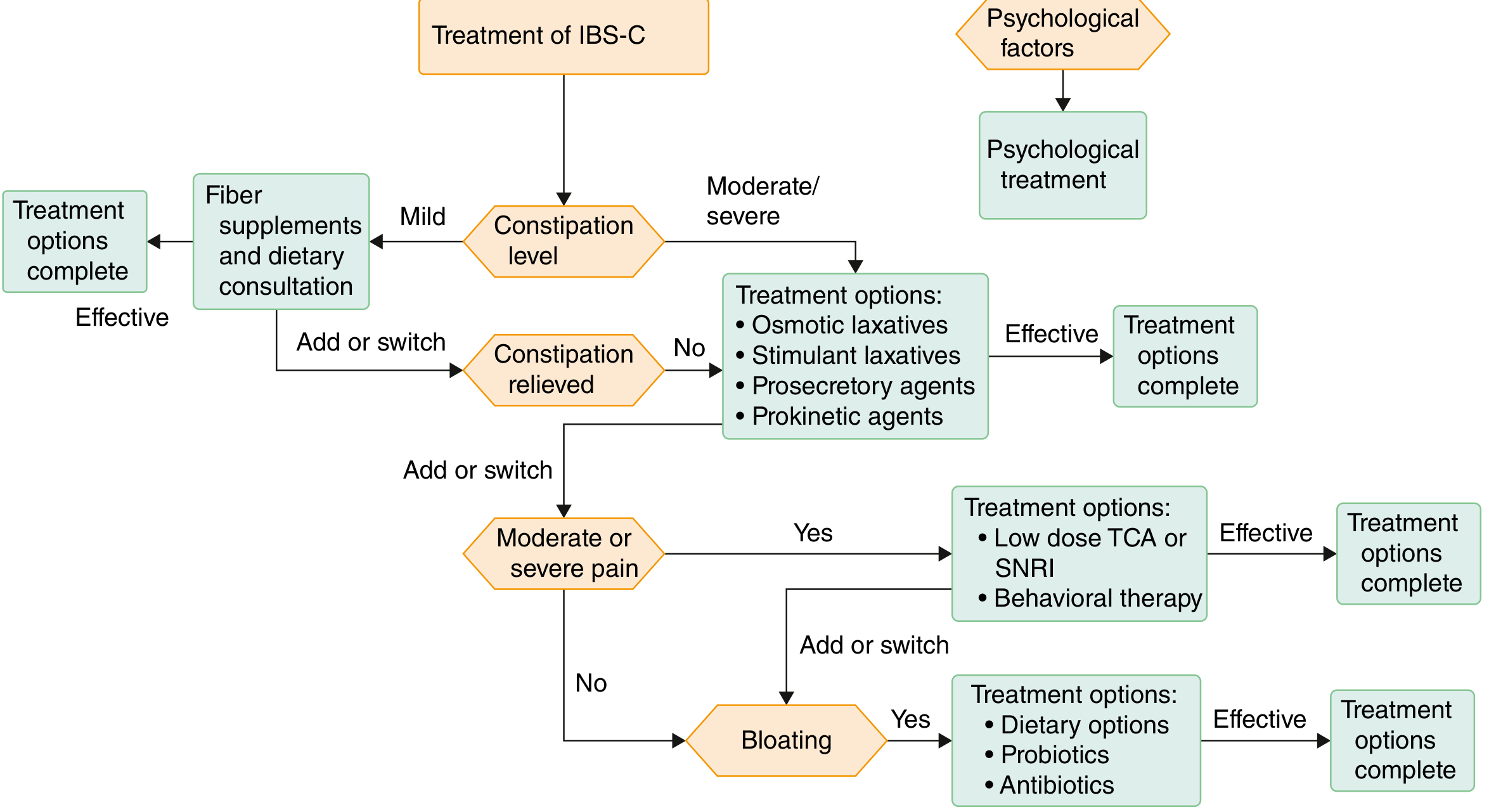
3. IBS-C Specific Pharmacotherapy
Treatment algorithm:
| Drug | Dose | Mechanism | Notes |
|---|---|---|---|
| Osmotic laxatives (PEG, lactulose) | Standard doses | Draws water into lumen | First-line for constipation relief |
| Linaclotide | 290 µg daily | Guanylate cyclase-C agonist → ↑Cl⁻/HCO₃⁻ secretion; also reduces visceral nerve firing → ↓pain | Diarrhea most common SE |
| Plecanatide | 3 mg daily | Same class as linaclotide (GC-C agonist) | Similar efficacy, similar SE profile |
| Tenapanor | 50 mg BID | NHE3 inhibitor → ↓Na⁺/water reabsorption | Diarrhea as common SE |
| Lubiprostone | 8 µg BID | ClC-2 channel activator → ↑intestinal secretion | Nausea common SE |
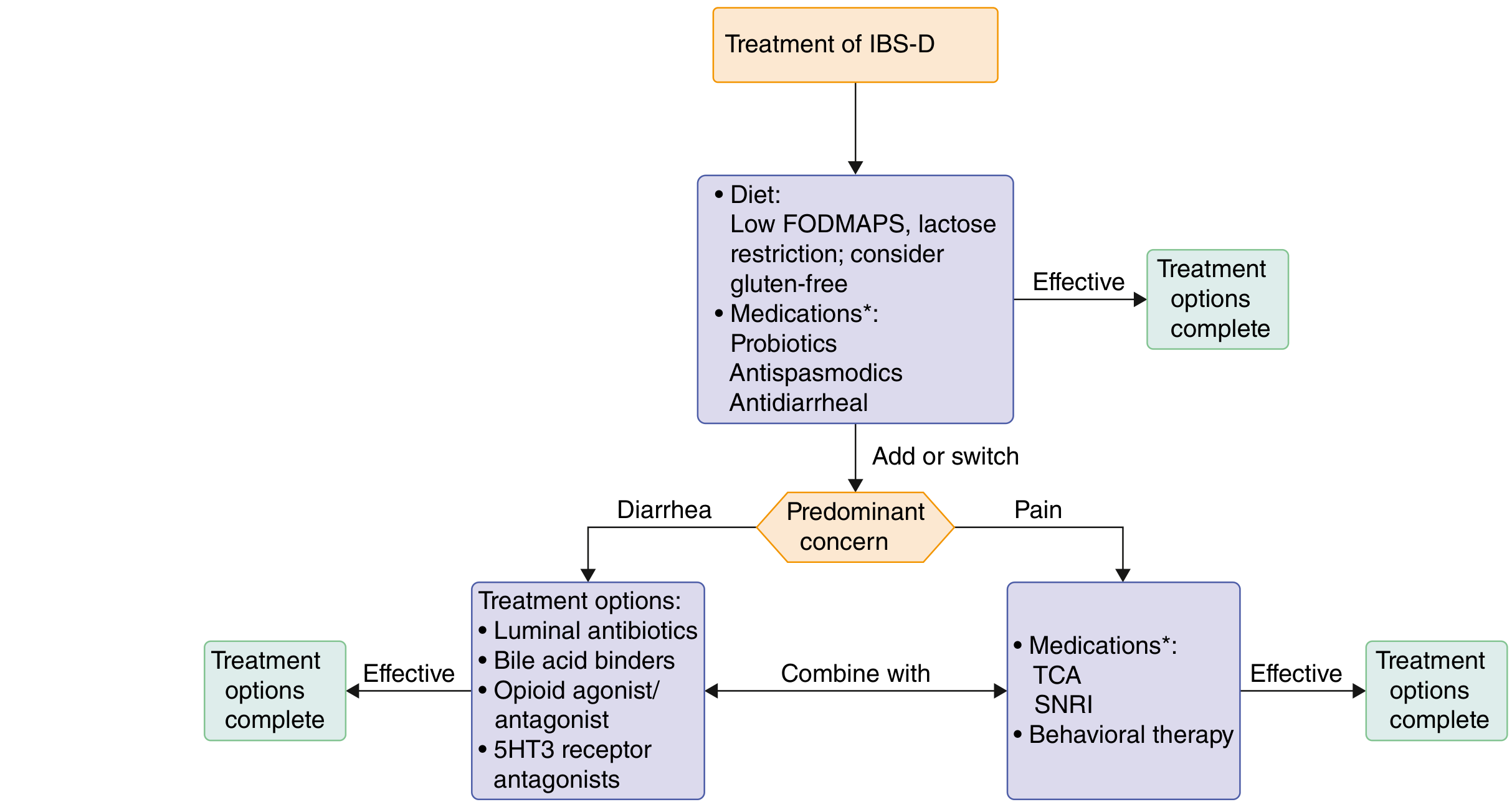
4. IBS-D Specific Pharmacotherapy
Treatment algorithm:
| Drug | Dose | Notes |
|---|---|---|
| Loperamide | PRN | Peripheral opioid agonist; reduces stool frequency but does NOT improve global IBS symptoms or pain. Best for mild-pain IBS-D. |
| Eluxadoline | 100 mg BID (or 75 mg BID if not tolerated) | µ- and κ-opioid agonist + δ-opioid antagonist; reduces diarrhea AND abdominal pain. CI: no gallbladder, hepatic impairment, biliary obstruction, SOD, alcohol use disorder. |
| Rifaximin | 550 mg TID × 14 days | Minimally absorbed antibiotic; approved for IBS-D. Up to 3 retreatment courses effective. |
| Alosetron | Restricted use (REMS program) | 5-HT₃ receptor antagonist; for women with severe IBS-D failing conventional treatment. Risk of ischemic colitis (1.1/1000 patient-years). |
| Bile acid sequestrants (cholestyramine, colestipol) | Standard doses | If bile acid diarrhea confirmed or suspected (affects ~25% of IBS-D). |
5. Psychological / Behavioral Therapies
~30% reduction in IBS symptoms vs. usual care. Recommended for patients who:
- Understand the role of brain-gut behavioral therapy
- Have persistent symptoms despite standard care
- Experience significant avoidance behaviors or distress
| Therapy | Key Focus |
|---|---|
| Cognitive-behavioral therapy (CBT) | Reduces maladaptive thoughts influencing GI symptoms; standard or minimal-contact formats available |
| Gut-directed hypnotherapy | Relaxation + reinterpretation of visceral signals |
| Mindfulness meditation | Stress reduction, symptom acceptance |
| Psychotherapy / relaxation training | Reduces stress-sensitive symptoms |
| Emotional awareness and expression therapy | Addresses suppressed emotional responses that exacerbate gut symptoms |
A 2024 systematic review (PMID 38777133, Gastroenterology) and a 2025 Lancet GH network meta-analysis (PMID 41077057) both confirm brain-gut behavioral therapies reduce abdominal pain and global IBS symptoms significantly.
Summary by Subtype
| Subtype | First-Line | Add if Insufficient |
|---|---|---|
| IBS-C | Low-FODMAP + soluble fiber + osmotic laxatives | Linaclotide / plecanatide / tenapanor; TCA/SNRI for pain |
| IBS-D | Low-FODMAP diet + loperamide or antispasmodic | Rifaximin; eluxadoline; alosetron (refractory women) |
| All | Education + dietary modification | Antispasmodics; probiotics (especially for bloating); psychological therapies for moderate-severe |
Prognosis
30-45% of patients have persistent symptoms for up to 12 years. Worse prognosis is associated with: anxiety, negative perception of stressors, female sex, younger age, and comorbid depression.
- Goldman-Cecil Medicine, Chapter 123 (Lin Chang)
This is a shared conversation. Sign in to Orris to start your own chat.