Haematological changes during pregnancy nots
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full notes.
Haematological Changes During Pregnancy
Sources: Miller's Anesthesia 10e, Creasy & Resnik's Maternal-Fetal Medicine, Medical Physiology (Boron & Boulpaep), Fishman's Pulmonary Diseases, Harrison's Principles of Internal Medicine 22e
1. Blood Volume
Pregnancy produces the most dramatic change in blood volume seen in any normal physiological state.
- Total blood volume rises by ~45-50% in singleton pregnancies; up to 75-100% in twin/triplet pregnancies
- Expansion begins in the first trimester, accelerates rapidly in the second trimester, slows in the third trimester, and plateaus in the last few weeks
- The increase serves to:
- Supply the hypertrophied uterine vasculature
- Protect against impaired venous return (supine/erect positions)
- Buffer against blood loss at delivery (300-500 mL vaginal; 800-1000 mL caesarean)
Figure - Blood volume changes throughout pregnancy:
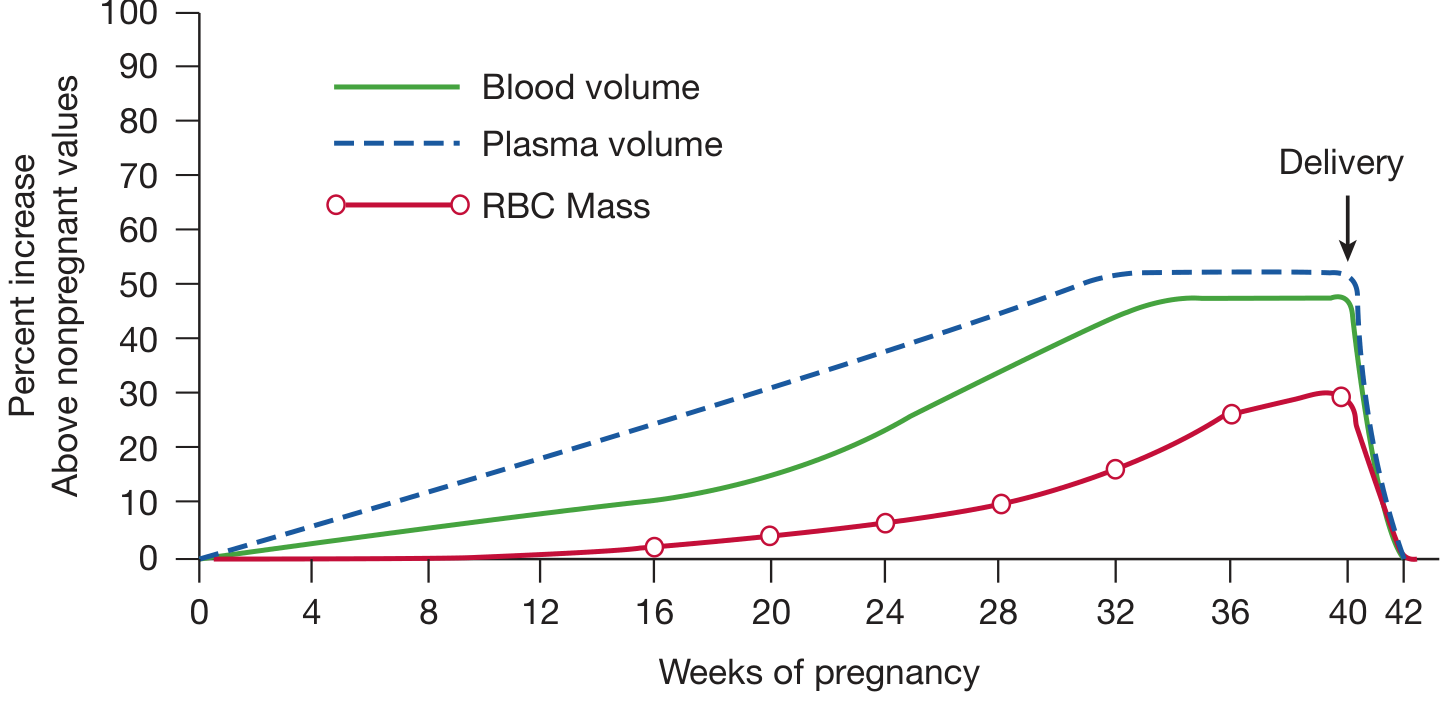
Plasma volume rises ~50% (disproportionately greater than RBC mass ~25-33%), creating the physiologic anaemia of pregnancy. After delivery, all volumes return sharply toward baseline. - Fishman's Pulmonary Diseases
2. Plasma Volume
| Parameter | Change |
|---|---|
| Plasma volume increase | ~50% above pre-pregnancy |
| Onset | Early first trimester |
| Peak | ~30-34 weeks |
| Mechanisms | Steroid hormones, elevated renin-aldosterone axis, RAAS activation, human placental lactogen, atrial natriuretic factor |
-
Progesterone and oestrogen cause peripheral vasodilation and decreased SVR, reducing renal perfusion
-
The RAAS responds with increased aldosterone, augmenting sodium and water reabsorption
-
Renal threshold for AVP shifts leftward (plasma osmolality set-point decreases), further expanding volume
-
After placental delivery, oestrogen/progesterone fall abruptly and a vigorous post-partum diuresis follows
-
Hypervolaemia also occurs with trophoblastic disease (a fetus is not essential for its development)
-
Creasy & Resnik's Maternal-Fetal Medicine; Medical Physiology
3. Red Cell Mass and Haemoglobin
| Parameter | Change |
|---|---|
| RBC mass increase | ~25-33% |
| Haemoglobin at term (normal) | ~11.6 g/dL |
| Haematocrit (acceptable) | ≥33% |
| Haemoglobin below which anaemia is diagnosed | <11 g/dL (any trimester) |
-
Because plasma volume rises more (~50%) than RBC mass (~25%), a dilutional or "physiologic" anaemia develops - this is normal and not pathological
-
Total oxygen delivery is not reduced because cardiac output increases to compensate
-
Iron supplementation corrects the RBC deficit; without it, haemoglobin can fall as low as 11 g/dL and haematocrit to 33%
-
In twin/triplet pregnancies, the plasma expansion is even greater and anaemia more pronounced
-
Miller's Anesthesia 10e; Creasy & Resnik's Maternal-Fetal Medicine
4. Iron and Erythropoiesis
- Pregnancy substantially increases iron demand to support:
- Expanded maternal RBC mass
- Fetal and placental iron requirements
- Erythropoietin levels rise in pregnancy, stimulating erythropoiesis
- Iron deficiency anaemia is the most common cause of true anaemia in pregnancy (haemoglobin <11 g/dL)
- Without supplementation, iron stores are readily depleted, especially in the third trimester
5. White Blood Cells (Leukocytes)
| Parameter | Change |
|---|---|
| Normal non-pregnant WBC | 4,000 - 10,000 /mm³ |
| Normal range in pregnancy | up to 13,000 /mm³ |
| Peak (during labour) | can rise further, proportional to duration of labour |
| Return to normal | first week postpartum, but may take weeks/months |
-
Physiologic leukocytosis is common in pregnancy and is unrelated to infection
-
Predominantly a neutrophilia
-
WBC rises further during labour (proportional to the duration of labour)
-
This physiologic leukocytosis can overlap with SIRS/sepsis criteria, making infection harder to diagnose in pregnancy
-
Miller's Anesthesia 10e
6. Platelets
| Parameter | Change |
|---|---|
| Platelet count | Normal or slightly decreased (~10% dilution at term) |
| Gestational thrombocytopenia | 8% of healthy pregnant women have platelets <150,000/mm³ |
| Floor of gestational thrombocytopenia | Rarely <70,000/mm³ |
-
The mild decrease is due to haemodilution and more rapid platelet turnover
-
Gestational thrombocytopenia is a diagnosis of exclusion - must differentiate from:
- Idiopathic thrombocytopenic purpura (ITP)
- HELLP syndrome (haemolysis, elevated liver enzymes, low platelets)
- Pre-eclampsia
-
Gestational thrombocytopenia is not associated with abnormal bleeding and resolves postpartum
-
Miller's Anesthesia 10e
7. Coagulation - Hypercoagulable State
Pregnancy creates a prothrombotic (hypercoagulable) state - an adaptation to minimise haemorrhage at delivery.
Increased Factors (Pro-coagulant)
| Factor | Change |
|---|---|
| Factor I (Fibrinogen) | Markedly increased (normal in pregnancy: 400-450 mg/dL) |
| Factor VII | Markedly increased |
| Factors II, V, VIII, IX, X, XII | Increased |
| von Willebrand factor | Increased |
Decreased Factors (Anti-coagulant)
| Factor | Change |
|---|---|
| Factor XI | Decreased |
| Factor XIII | Decreased |
| Protein S | Decreased |
| Antithrombin III | Decreased |
| Protein C | Unchanged |
Net Effect
- PT shortened by ~20%
- PTT shortened by ~20%
- Overall: shortened clotting times, promoting haemostasis
Thromboelastography (TEG) at Term
-
Decreased R time (time to start clot formation)
-
Decreased K time (time to specified clot strength)
-
Increased α angle (rate of clot formation)
-
Increased MA (maximum amplitude / clot strength)
-
Changes begin as early as the first trimester
-
Miller's Anesthesia 10e; Harrison's Principles 22e
Clinical implication: This hypercoagulable state, combined with venous stasis and endothelial injury, constitutes Virchow's triad in pregnancy - the basis for a 4-6x increased risk of VTE (venous thromboembolism) during pregnancy and the puerperium.
8. Fibrinogen
-
Normal pregnancy fibrinogen: 400-450 mg/dL (significantly above the normal non-pregnant range of 200-400 mg/dL)
-
Values below 300 mg/dL in pregnancy indicate significant consumption of coagulation factors (e.g. DIC, abruption, HELLP)
-
Oestrogens stimulate hepatic rough endoplasmic reticulum, increasing protein synthesis including fibrinogen, factors VII, VIII, IX, and X
-
Creasy & Resnik's Maternal-Fetal Medicine; Rosen's Emergency Medicine
9. Summary Table
| Parameter | Direction | Magnitude |
|---|---|---|
| Plasma volume | ↑ | ~50% |
| Total blood volume | ↑ | ~45-50% |
| RBC mass | ↑ | ~25-33% |
| Haemoglobin | ↓ (dilutional) | ~11.6 g/dL at term |
| Haematocrit | ↓ (dilutional) | ~33% acceptable floor |
| WBC | ↑ | Up to 13,000/mm³ (labour: higher) |
| Platelets | ↓ slightly | ~10% dilution |
| Fibrinogen | ↑ markedly | 400-450 mg/dL |
| Factors VII, VIII, IX, X, XII | ↑ | Variable |
| Factors XI, XIII | ↓ | Modest |
| Protein S, Antithrombin III | ↓ | Modest |
| PT / PTT | ↓ | ~20% shorter |
10. Key Clinical Points
- Physiologic anaemia is expected - Hb ~11.6 g/dL is normal at term; values below 11 g/dL need investigation
- Leukocytosis up to 13,000/mm³ is normal - do not treat for infection without other evidence
- Mild thrombocytopenia is usually gestational - but HELLP and ITP must be excluded
- Pregnancy is a hypercoagulable state - elevated DVT/PE risk throughout pregnancy and 6 weeks postpartum
- Post-partum autotransfusion - uterine contraction after delivery returns >500 mL blood to circulation, offsetting delivery blood loss
- Iron supplementation is routinely indicated to support the expanded RBC mass and prevent true iron-deficiency anaemia
This is a shared conversation. Sign in to Orris to start your own chat.