Tuberculosis pleural effusion full details for md exam answer 15 marks structured answer
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Running Command
Running Command
Reading File
Running Command
Finding Sources
Running Command
Reading File
Reading File
Running Command
Reading File
Reading File
Loading Image
This is your complete, exam-ready 15-mark structured answer on Tuberculosis Pleural Effusion, compiled from Sharma Mohan's TB textbook, Murray & Nadel's Respiratory Medicine, Harrison's 22E, and Light's Pleural Diseases. Here's a quick map of how marks are distributed:
| Section | Marks |
|---|---|
| Introduction + Epidemiology | 1 |
| Pathogenesis (dual mechanism, spectrum concept) | 2 |
| Clinical Features | 2 |
| Radiology | 1 |
| Pleural Fluid Analysis + Diagnostic Markers | 3 |
| Diagnosis (stepwise approach, gold standard) | 2 |
| Treatment (ATT regimen, steroids, fibrinolytics) | 2 |
| DD of lymphocytic exudate | 1 |
| Complications | 1 |
| Total | 15 |
High-yield points examiners look for:
- Pathogenesis: paucibacillary + delayed hypersensitivity as a spectrum, not two separate disorders
- ADA >40 IU/L in a lymphocytic exudate = key diagnostic pointer
- IFN-γ >140 pg/mL — direct ELISA required (not IGRA)
- Pleural biopsy = gold standard; thoracoscopy = highest yield
- Treatment is identical to pulmonary TB: 2HRZE/4HR
- Paradoxical worsening during ATT is recognized and should not trigger treatment withdrawal
- Corticosteroids: low-quality evidence, always start ATT first
Where is the answer
The full answer is right above this message — scroll up. It's a long, detailed response. Here's the complete content again for convenience:
TUBERCULOSIS PLEURAL EFFUSION
MD Examination Answer — 15 Marks
1. INTRODUCTION & EPIDEMIOLOGY (1 mark)
Tuberculous pleural effusion is the most common cause of an exudative pleural effusion in many parts of the world. In Africa, pleural TB represents >30% of all TB cases (partly due to HIV co-infection). It is relatively uncommon in the US (~3.6% of TB cases). It may represent primary TB (3–6 months after initial infection) or reactivation TB.
2. PATHOGENESIS (2 marks)
Caused by rupture of a subpleural caseous focus into the pleural space, introducing mycobacterial antigens. Two overlapping mechanisms:
A. Delayed Hypersensitivity (Classical)
- Sensitised T-lymphocytes react to mycobacterial proteins → cytokine-driven vascular permeability → exudate
- Explains historically negative culture results (~80%)
B. Paucibacillary Direct Infection (Modern)
- Improved liquid culture + biopsy identifies bacilli in >60% of cases
- Initial neutrophilic acute inflammation → evolves to lymphocyte-driven chronic reaction + granuloma formation
- Lymphocyte activity inversely correlates with culture positivity
- Sufficient lymphocytic activity can sterilise the pleural space → explains spontaneous resolution
TB Pleuritis vs. TB Empyema — a spectrum, not two distinct diseases:
| Feature | TB Pleuritis | TB Empyema |
|---|---|---|
| Mechanism | Paucibacillary + immune reaction | High mycobacterial load |
| Fluid | Serous, lymphocytic exudate | Purulent |
| Culture | Usually negative | Positive |
| Spontaneous resolution | Possible | Unlikely |
In HIV co-infection: more systemic features, culture-positive effusions more common, more prevalent when CD4 >200 cells/μL.
3. CLINICAL FEATURES (2 marks)
Acute presentation (~2/3 cases): cough, pleuritic chest pain (~75%), fever, dyspnea — mimics bacterial pneumonia
Chronic presentation (~1/3 cases): low-grade fever, weakness, weight loss, night sweats
Effusion characteristics:
- Almost always unilateral
- Usually small to moderate in size (occasionally massive)
- Up to 86% have coexisting parenchymal disease — effusion always on the same side
- Even without radiographic parenchymal involvement, induced sputum is positive in ~55%
Rare complications: TB empyema (with pneumothorax + bronchopleural fistula), empyema necessitans, fibrothorax
4. RADIOLOGY (1 mark)
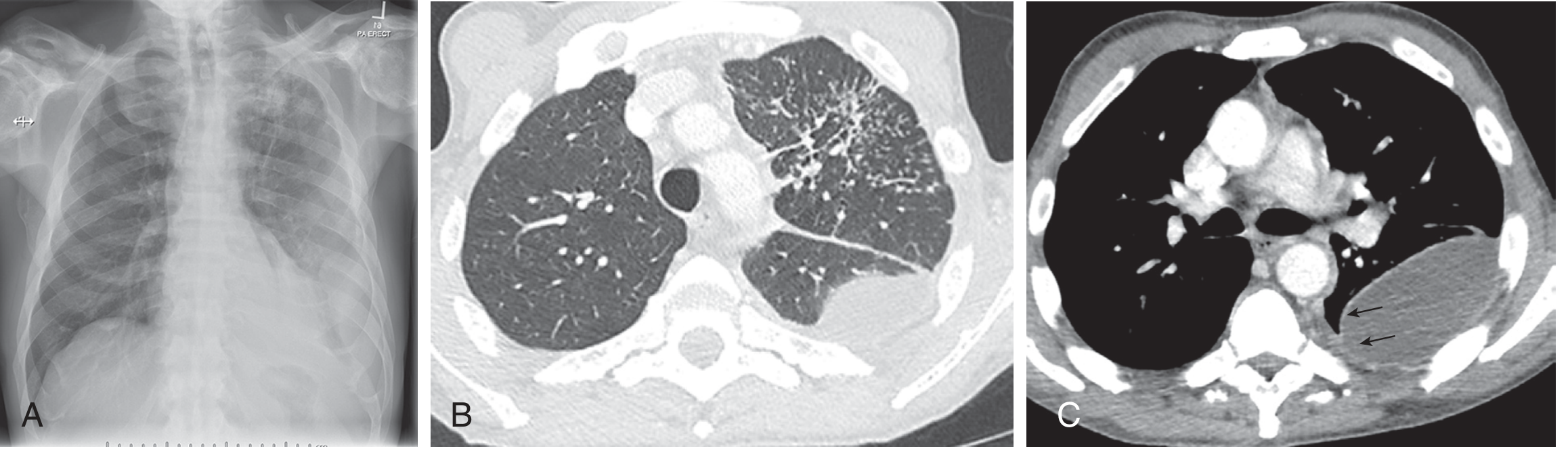
- CXR: unilateral homogeneous opacity; obliterated costophrenic angle; associated apical/upper lobe consolidation
- CT chest: encapsulated/loculated collections; smooth pleural enhancement ("split-pleura" sign); mediastinal lymphadenopathy; tree-in-bud nodules
- Ultrasound: free vs. loculated; guides thoracentesis
5. PLEURAL FLUID ANALYSIS (3 marks)
All TB effusions are exudates by Light's criteria:
- PF protein / serum protein > 0.5
- PF LDH / serum LDH > 0.6
- PF LDH > 2/3 upper limit of normal serum LDH
Biochemistry:
| Parameter | Finding |
|---|---|
| Protein | >3 g/dL; often >5 g/dL (characteristic of TB) |
| LDH | Elevated |
| Glucose | Normal or mildly reduced |
| pH | Normal (reduced in empyema) |
Cytology:
- Lymphocyte-predominant (hallmark) — small mature lymphocytes
- PMN predominance in ~11% (early disease)
- Mesothelial cells: characteristically absent or very sparse
Diagnostic Markers:
| Marker | Cut-off | Notes |
|---|---|---|
| ADA (Adenosine Deaminase) | >40 IU/L | Most clinically useful; released by T-lymphocytes; sensitivity ~90%, specificity ~90% |
| IFN-γ | >140 pg/mL | High accuracy; requires direct ELISA — NOT IGRA (insufficiently sensitive on PF) |
| PCR (mycobacterial DNA) | Positive | Variable sensitivity; high specificity |
| AFB culture (PF) | Positive | Low sensitivity (~30–40%); liquid media improves yield; gold standard if positive |
| AFB smear (PF) | Positive | Very low sensitivity (<20%) |
Key point: ADA + differential cell count + clinical context used in combination substantially improves diagnostic accuracy. ADA >50 IU/L in a lymphocytic exudate (Cecil's cut-off) is strongly suggestive.
6. DIAGNOSIS (2 marks)
Gold standard: Pleural biopsy showing caseating granulomas or positive AFB culture of biopsy tissue.
Stepwise Approach:
Step 1 — Thoracentesis
Send for: biochemistry, cytology + differential, AFB smear & culture, ADA, IFN-γ, PCR
Step 2 — Sputum
Induced sputum AFB smear + culture → positive in ~50% even without radiographic parenchymal involvement
MODS assay: liquid culture with drug susceptibility; faster, cheaper; WHO-approved for resource-limited settings
Step 3 — Pleural Biopsy (if above inconclusive)
- Thoracoscopy (medical / VATS): ideal — highest yield; direct visualization + directed biopsy
- Image-guided percutaneous needle biopsy: replaced closed biopsy in high-income settings
- Blind needle biopsy (Abrams needle): important in high-TB-prevalence/resource-limited settings; combine with ADA + differential; ultrasound guidance improves yield
- Biopsy culture yield > pleural fluid culture yield
Diagnostic criteria (any one):
- Caseating granuloma on pleural biopsy
- Positive AFB culture (fluid / biopsy / sputum)
- ADA >40 IU/L + lymphocytic exudate + compatible clinical picture + exclusion of alternative diagnoses
7. TREATMENT (2 marks)
Antituberculous Therapy (ATT)
Same regimen as pulmonary TB:
| Phase | Duration | Drugs |
|---|---|---|
| Intensive phase | 2 months | HRZE — 2HRZE |
| Continuation phase | 4 months | HR — 4HR |
| Total | 6 months |
(H = Isoniazid, R = Rifampicin, Z = Pyrazinamide, E = Ethambutol)
Response:
- Fever resolves: ~2 weeks
- Effusion resolves: ~6 weeks
- Residual pleural fibrosis: ~50% at 1 year (usually no functional impairment)
Corticosteroids
- May reduce time to resolution and residual fibrosis
- Evidence is low quality; more adverse events
- Always start ATT first, then add steroids if indicated
- Caution in HIV patients (possible Kaposi sarcoma risk)
Therapeutic Thoracentesis
- For large effusions causing significant dyspnea
- Not routinely required for small-moderate effusions on ATT
Intrapleural Fibrinolytics
- May improve drainage and reduce residual thickening
- Clinical benefit uncertain; not routine practice
Paradoxical Worsening
- Effusion worsens after starting ATT or new effusion develops during treatment for pulmonary TB
- First exclude wrong diagnosis; if TB confirmed → continue ATT (immune reconstitution reaction)
8. DIFFERENTIAL DIAGNOSIS OF LYMPHOCYTIC EXUDATE (1 mark)
| Condition | Key Distinguishing Feature |
|---|---|
| Malignant effusion | Positive cytology; low ADA; imaging mass |
| Lymphoma | Very high LDH; CT mediastinal mass |
| Rheumatoid pleurisy | Glucose <30 mg/dL; RF positive; low complement |
| Chylothorax | Triglycerides >110 mg/dL; milky fluid |
| Fungal (Cryptococcus) | Immunocompromised; antigen titre positive |
| Sarcoidosis | Bilateral; hilar lymphadenopathy; ACE elevated |
9. COMPLICATIONS (1 mark)
| Complication | Notes |
|---|---|
| Fibrothorax / Trapped lung | ~50% at 1 year; rarely requires decortication |
| TB Empyema | Purulent, culture positive; requires drainage ± surgery |
| Empyema necessitans | Rare; spontaneous percutaneous decompression |
| Bronchopleural fistula | Complicates TB empyema after lung rupture |
| Paradoxical worsening | During ATT; immune reconstitution |
| MDR-TB | Culture + drug susceptibility testing essential |
RAPID REVISION TABLE
| Feature | TB Pleural Effusion |
|---|---|
| Type | Exudate (Light's criteria) |
| Side | Unilateral (almost always) |
| Cells | Lymphocyte-predominant |
| ADA | >40 IU/L |
| IFN-γ | >140 pg/mL |
| Protein | Often >5 g/dL |
| Gold standard | Pleural biopsy (granuloma/AFB) |
| Treatment | 2HRZE + 4HR |
| Fever resolution | ~2 weeks |
| Effusion resolution | ~6 weeks |
| Residual fibrosis | ~50% at 1 year |
Sources: Murray & Nadel's Respiratory Medicine; Harrison's 22E; Goldman-Cecil Medicine; Sharma SK — Textbook of Tuberculosis & NTM Diseases, 3rd Ed; Light RW — Pleural Diseases
This is a shared conversation. Sign in to Orris to start your own chat.