Gate control theory of pain
Gate control theory of pain for 1st year mbbs physiology
Reading File
Finding Sources
Finding Sources
Searching the Web
gate control theory of pain physiology diagram Melzack Wall
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Searching PubMed
"gate control theory" AND pain
I have excellent textbook content and two clear diagrams. I now have everything needed for a comprehensive 1st-year MBBS answer. Let me compose it.
Gate Control Theory of Pain
Proposed by: Ronald Melzack and Patrick Wall, 1965 (published in Science)
Background - Why This Theory Was Needed
Before 1965, the dominant view was the Specificity Theory - pain fibers simply carried impulses straight to a pain center in the brain. This failed to explain:
- Why rubbing an injured area reduces pain
- Why soldiers in battle feel no pain despite serious wounds
- Why chronic pain persists without tissue damage
- How psychological state influences pain intensity
Melzack and Wall proposed that pain is not simply transmitted - it is modulated at the level of the spinal cord.
Core Concept
The dorsal horn of the spinal cord acts like a "gate" that can either allow or block pain signals from reaching the brain. The state of this gate is determined by the balance of activity between two types of nerve fibers.
Key Components
| Component | Description |
|---|---|
| Small fibers (C fibers / Aδ fibers) | Thin, slow, unmyelinated/lightly myelinated - carry pain (nociceptive) signals |
| Large fibers (Aβ fibers) | Thick, fast, myelinated - carry touch, pressure, vibration (non-nociceptive) |
| Substantia Gelatinosa (SG) | Inhibitory interneurons in the dorsal horn - the "gate" cells |
| Transmission (T) cells | Projection neurons in the dorsal horn - send signals up the anterolateral tract to the brain |
The Gate Mechanism
Diagram 1 - Neuroscience: Exploring the Brain (Bear, Connors, Paradiso):
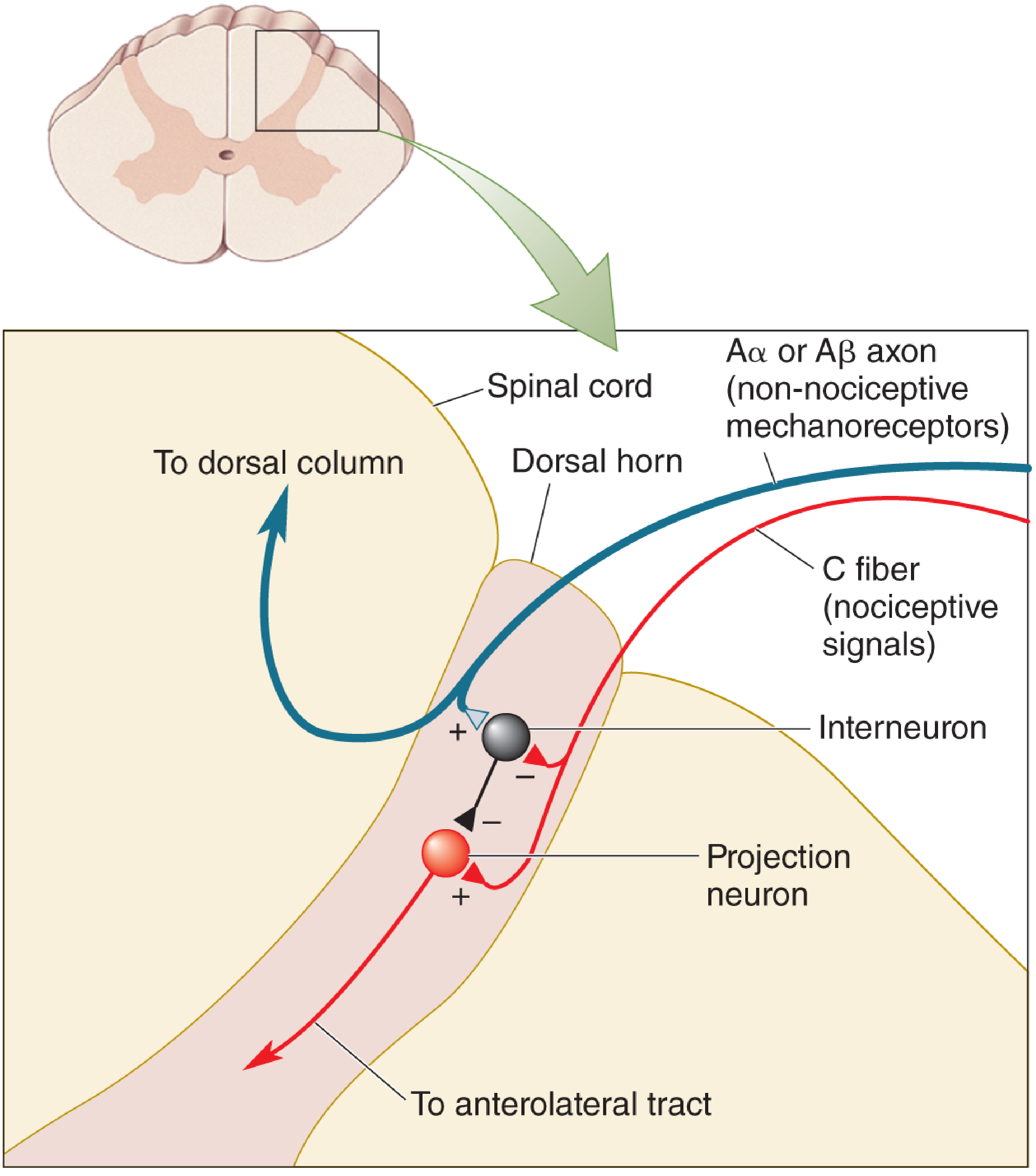
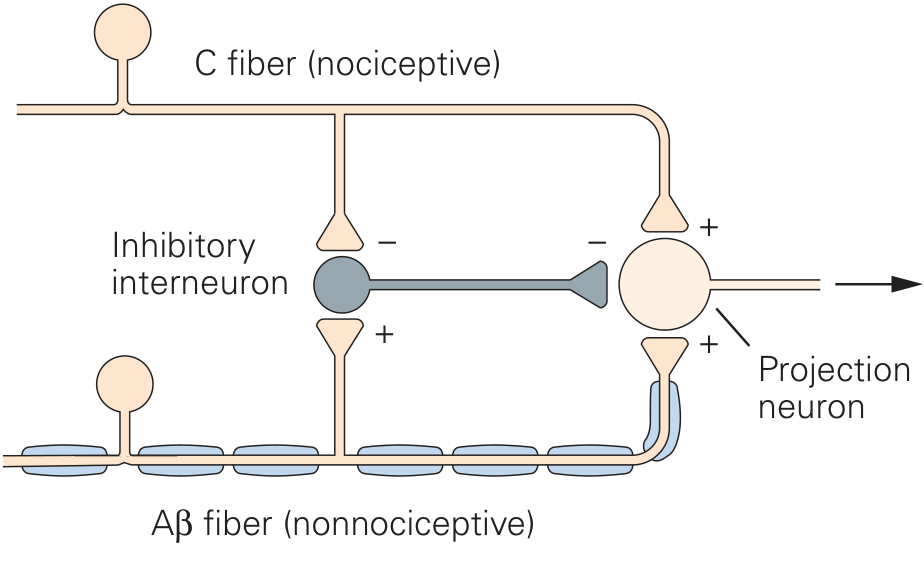
Diagram 2 - Kandel's Principles of Neural Science (6th Edition):
When the Gate is OPEN (Pain is felt)
- C fibers (nociceptive) are active
- C fibers inhibit the inhibitory interneuron (SG cell) - i.e., they remove the brake
- With the interneuron suppressed, the T cell (projection neuron) fires freely
- Nociceptive signals travel up the anterolateral (spinothalamic) tract to the brain
- Result: Pain is perceived
When the Gate is CLOSED (Pain is reduced)
- Aβ fibers (large, non-nociceptive) are active (e.g., due to rubbing, vibration, TENS)
- Aβ fibers excite the inhibitory interneuron (SG cell) - i.e., they activate the brake
- The excited interneuron inhibits the T cell (projection neuron)
- Fewer pain signals reach the brain
- Result: Pain is reduced or blocked
Summary Table
| Condition | Large fiber (Aβ) | Small fiber (C) | Interneuron | T cell | Gate | Pain |
|---|---|---|---|---|---|---|
| Pain only | Low activity | High activity | Inhibited | Fires | Open | Yes |
| Touch + Pain | High activity | Low activity | Excited | Inhibited | Closed | Reduced |
| TENS therapy | Stimulated | Not targeted | Excited | Inhibited | Closed | Reduced |
Third Component - Central (Descending) Control
Melzack and Wall also proposed a central control trigger - signals from the brain (via descending pathways, e.g., from the periaqueductal grey / PAG) can modulate the gate from above. This explains:
- Stress-induced analgesia (soldiers not feeling pain in battle)
- Placebo effects
- How attention, emotion, and expectation alter pain
Clinical Applications
-
TENS (Transcutaneous Electrical Nerve Stimulation): Electrodes placed on skin stimulate Aβ fibers, closing the gate - used for arthritis, tendonitis, chronic back pain. - Neuroscience: Exploring the Brain, 5th Ed., p. 1213
-
Spinal Cord Stimulation (SCS): Implanted electrodes near the dorsal column activate large fibers to close the gate for intractable neuropathic pain. - Kandel's Principles of Neural Science, 6th Ed., p. 535
-
Rubbing an injury: Activating Aβ mechanoreceptors by rubbing closes the gate and transiently reduces pain.
-
Acupuncture: May work partly by stimulating large fibers that close the gate.
-
Distraction and relaxation: Descending cortical pathways can close the gate even without peripheral stimulation.
Limitations of the Original Theory
- The original circuit was oversimplified - interactions also occur at supraspinal (brainstem, thalamus, cortex) relay centers, not just the spinal cord
- Melzack later extended it into the Neuromatrix Theory (1990s), accounting for how the brain creates pain as an output even without peripheral input (e.g., phantom limb pain)
- The exact identity and wiring of the interneurons has been updated by subsequent research
Key Points for Exam
- Proposed by Melzack and Wall, 1965
- Gate is located in the dorsal horn of the spinal cord (substantia gelatinosa)
- Large fibers (Aβ) close the gate - inhibit pain
- Small fibers (C/Aδ) open the gate - facilitate pain
- Inhibitory interneurons are the key mediators
- Descending control from higher brain centers can also modulate the gate
- Clinical basis of TENS, SCS, acupuncture, rubbing
Sources: Neuroscience: Exploring the Brain (5th Ed.), p. 1213-1215; Kandel's Principles of Neural Science (6th Ed.), p. 535; original Melzack & Wall paper, Science, 1965
Gate control theory of pain for 1st year mbbs physiology
Finding Sources
Finding Sources
Searching the Web
gate control theory pain Melzack Wall 1965 MBBS physiology spinal cord mechanism
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed - rich textbook content from Ganong's, Kandel's, and Neuroanatomy through Clinical Cases, plus two high-quality diagrams. Here is the complete, exam-ready answer for 1st year MBBS.
Gate Control Theory of Pain
Proposed by: Ronald Melzack and Patrick Wall | Year: 1965 | Published in: Science
Why This Theory Was Needed
Before 1965, the Specificity Theory held that dedicated pain fibers simply carried impulses to a pain center in the brain - a passive, straight-line system. This failed to explain everyday observations:
- Rubbing a bruised shin reduces pain
- Soldiers in battle feel no pain despite severe injuries
- Minor stimuli can hurt intensely in anxious or depressed individuals
- Chronic pain persists long after tissue healing
Melzack and Wall proposed that pain is not just transmitted - it is actively modulated at the spinal cord before reaching the brain.
Core Concept
The dorsal horn of the spinal cord acts as a "gate" that can either allow or block nociceptive signals from ascending to the brain. The state of the gate depends on the balance of activity between large and small diameter nerve fibers.
- Ganong's Review of Medical Physiology, 26th Ed.
Key Players in the Circuit
| Component | Fiber type | Function |
|---|---|---|
| Large fibers (Aα/Aβ) | Myelinated, fast | Carry touch, pressure, vibration (non-nociceptive) |
| Small fibers (Aδ/C) | Thin, slow, unmyelinated | Carry pain and temperature (nociceptive) |
| Substantia Gelatinosa (SG) | Inhibitory interneurons in dorsal horn | The "gate" - modulate T cell output |
| Transmission (T) cells | Projection neurons in dorsal horn | Relay signals up the anterolateral (spinothalamic) tract to brain |
The Gate Mechanism - Circuit Diagrams
Diagram 1 (from Kandel's Principles of Neural Science, 6th Ed.):
Diagram 2 (from Neuroscience: Exploring the Brain, 5th Ed.):
Gate OPEN - Pain is Felt
- Injury activates small C/Aδ fibers (nociceptive)
- C fibers inhibit the inhibitory interneuron (SG cell) - they remove the brake
- With the interneuron suppressed, the T cell fires freely
- Pain signals travel up the anterolateral (spinothalamic) tract to thalamus and cortex
- Result: Pain is perceived
Gate CLOSED - Pain is Reduced
- Large Aβ fibers are activated (e.g., by rubbing, touch, vibration, TENS)
- Aβ fibers excite the inhibitory interneuron (SG cell) - they turn on the brake
- The active interneuron inhibits the T cell (projection neuron)
- Nociceptive signals cannot efficiently travel to the brain
- Result: Pain perception is reduced or blocked
Summary Table
| Situation | Large fiber (Aβ) activity | Small fiber (C) activity | Interneuron | T cell | Gate state | Pain perceived? |
|---|---|---|---|---|---|---|
| Injury only | Low | High | Inhibited | Fires freely | Open | Yes |
| Rubbing injury | High | Low | Excited | Inhibited | Closed | Reduced |
| TENS applied | Stimulated artificially | Not targeted | Excited | Inhibited | Closed | Reduced |
| Anxiety/fear | Low | High | Relatively suppressed | More active | More open | Increased |
Third Component - Descending (Central) Control
Melzack and Wall added a central control trigger - higher brain centers can descend to modulate the gate independently of peripheral input.
- The periaqueductal grey (PAG) in the midbrain receives inputs from the hypothalamus, amygdala, and cortex
- PAG activates a relay in the rostral ventral medulla (RVM)
- From the RVM, serotonergic (5-HT) fibres of the raphe nuclei descend to inhibit T cells in the dorsal horn
- The RVM also activates the locus coeruleus, which sends noradrenergic (NE) projections to further suppress dorsal horn nociceptive transmission
- Neuroanatomy through Clinical Cases, 3rd Ed.
This explains:
- A soldier in combat feeling no pain (stress/adrenaline activates descending inhibition)
- Placebo analgesia
- How depression or anxiety can worsen chronic pain (reduced descending inhibition)
Role of Endogenous Opioids
The interneurons in the superficial dorsal horn contain enkephalin and dynorphin (endogenous opioid peptides). These act on opioid receptors (presynaptic and postsynaptic) to:
- Decrease Ca²+ influx at nociceptive fiber terminals → less glutamate/substance P release
- Hyperpolarize dorsal horn neurons via increased K+ conductance
This is the same mechanism exploited by morphine and other opioid analgesics. - Ganong's Review of Medical Physiology, 26th Ed.
Clinical Applications
| Application | Mechanism |
|---|---|
| TENS (Transcutaneous Electrical Nerve Stimulation) | Electrodes stimulate Aα/Aβ fibers near injury → gate closes → used for arthritis, back pain, tendonitis |
| Spinal Cord Stimulation (SCS) | Implanted dorsal column electrodes activate large fibers → gate closes → used for intractable neuropathic pain |
| Rubbing an injury | Activates Aβ mechanoreceptors → closes gate temporarily |
| Acupuncture | Possibly activates large Aβ fibers and descending inhibitory pathways |
| Psychological interventions | Cognitive-behavioural therapy, relaxation, distraction → strengthen descending inhibitory control |
| Opioid analgesics | Mimic endogenous enkephalins at dorsal horn opioid receptors |
Limitations of the Original Theory
- The original model was oversimplified - subsequent research showed interactions also occur at supraspinal (thalamic, cortical) levels, not just the spinal cord
- Melzack later revised it into the Neuromatrix Theory (1999), proposing the brain generates pain as an active output based on a body-self "neuromatrix" - explaining phantom limb pain, psychogenic pain, and chronic pain without identifiable tissue damage
- The exact interneuron subtypes and precise wiring have been updated considerably
High-Yield Exam Points
- Proposed by: Melzack and Wall, 1965
- Gate location: Dorsal horn of spinal cord, specifically the substantia gelatinosa
- Large fibers (Aβ) → Close the gate (reduce pain) by exciting inhibitory interneurons
- Small fibers (C/Aδ) → Open the gate (facilitate pain) by inhibiting interneurons
- T cells = transmission neurons = projection neurons of anterolateral tract
- Descending control via PAG → RVM → serotonin/noradrenaline pathways can also close the gate
- Clinical basis of TENS, SCS, rubbing, opioids, psychological pain therapy
- Explains paradoxes: battle analgesia, why rubbing helps, how anxiety worsens pain
Sources: Ganong's Review of Medical Physiology 26th Ed.; Kandel's Principles of Neural Science 6th Ed.; Neuroanatomy through Clinical Cases 3rd Ed.; original Melzack & Wall, Science, 1965
This is a shared conversation. Sign in to Orris to start your own chat.