Pre operative evaluation of respiratory system before surgery full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have all the key content needed for a comprehensive MD exam answer. Let me compile the full answer.
Preoperative Evaluation of the Respiratory System Before Surgery
Introduction
Perioperative pulmonary complications — atelectasis, pneumonia, respiratory failure, prolonged mechanical ventilation — occur in 15–20% of thoracic surgery patients and account for the majority of the expected 3–4% perioperative mortality. For non-thoracic surgery, pulmonary complications remain a leading cause of postoperative morbidity. A structured preoperative respiratory evaluation is therefore mandatory, with goals of:
- Identifying patients at elevated risk
- Stratifying perioperative management
- Focusing resources on high-risk patients
- Optimizing respiratory function before surgery
I. Predisposing Risk Factors for Pulmonary Complications
All patients undergoing non-cardiac surgery should be assessed using established risk factors (Harrison's 22e):
| # | Risk Factor |
|---|---|
| 1 | Upper respiratory tract infection (cough, dyspnoea) |
| 2 | Age >60 years |
| 3 | Chronic obstructive pulmonary disease (COPD) |
| 4 | Cigarette smoking |
| 5 | ASA physical status class ≥ 2 |
| 6 | Functional dependence |
| 7 | Congestive heart failure |
| 8 | Serum albumin <3.5 g/dL |
| 9 | Obstructive sleep apnoea |
| 10 | Impaired sensorium (confusion, delirium) |
| 11 | Abnormal chest examination |
| 12 | Alcohol use |
| 13 | Weight loss |
Surgical risk factors: Emergency surgery, aortic aneurysm repair, vascular surgery, major abdominal/thoracic/neurological/head/neck surgery, and general anaesthesia all confer elevated risk.
ARISCAT Risk Index — includes 7 variables: age, low preoperative SpO₂, respiratory infection within 1 month, upper abdominal or thoracic surgery, surgery lasting >2 hours, Hb <10 g/dL, and emergency surgery.
II. The Three-Legged Stool of Pre-Thoracotomy Respiratory Assessment
For pulmonary resection surgery (and any major thoracic procedure), no single test of respiratory function is adequate. The evaluation must cover three related but independent areas — analogous to a three-legged stool (Miller's Anesthesia, 10e):
1. Respiratory Mechanics (Lung mechanical function)
2. Lung Parenchymal Function (Gas exchange)
3. Cardiopulmonary Interaction (Exercise capacity)
III. Assessment of Respiratory Mechanics
Key test: Predicted Postoperative FEV₁ (ppoFEV₁)
Multiple spirometric parameters correlate with post-thoracotomy outcome: FEV₁, FVC, MVV, RV/TLC ratio. The most valid single predictor is:
$$\text{ppoFEV}_1% = \text{Preoperative FEV}_1% \times \left(1 - \frac{% \text{ functional lung tissue removed}}{100}\right)$$
Using lung segments (19 total — right: upper 3, middle 2, lower 5; left: upper 3, lingula 2, lower 4):
$$\text{epoFEV}_1 = \text{preFEV}_1 \times \frac{19 - \text{segments to be removed}}{19}$$
Risk thresholds:
| ppoFEV₁ | Risk Category |
|---|---|
| >40% | Low risk — can extubate in OR |
| 30–40% | Intermediate risk |
| <30% | High risk of major respiratory complications |
| <20% | Very high risk — consider alternative therapy |
Absolute spirometry values (for lung resection):
- FEV₁ >2 L → can tolerate any resection
- FEV₁ >1.5 L → can tolerate lobectomy
- MVV <50% predicted → high risk
- PEF <100 L/min or <50% predicted → high risk
Note: For VATS (video-assisted thoracoscopic surgery), the risk threshold has shifted from ppoFEV₁ <40% (open thoracotomy) to <30%, reflecting better preservation of function.
IV. Assessment of Lung Parenchymal Function (Gas Exchange)
Key test: Diffusing Capacity for Carbon Monoxide (DLCO)
- DLCO reflects total functioning alveolar-capillary surface area
- Corrected DLCO can also be expressed as ppoDLCO using the same formula as for FEV₁
- ppoDLCO <40% predicted → increased both respiratory and cardiac complications (independent of FEV₁)
- DLCO (but not FEV₁) is negatively affected by preoperative chemotherapy — making it the most important predictor in those patients
Arterial Blood Gas (ABG):
| Value | Significance |
|---|---|
| PaO₂ < 60 mmHg | Warning indicator — increased risk |
| PaCO₂ > 45 mmHg | Warning indicator — CO₂ retention, increased risk |
ABG should be done preoperatively to establish baseline and guide postoperative management.
V. Assessment of Cardiopulmonary Interaction (Exercise Capacity)
Exercise capacity is the final and most important assessment. It is expressed in metabolic equivalents (METs): 1 MET = 3.5 mL O₂/kg/min at rest; climbing 1 flight = 4 METs.
Simple Tests
1. Stair-Climbing Test:
- Minimum: ability to climb 2 flights without stopping (a pragmatic screening test)
2. Six-Minute Walk Test (6MWT):
- Gold standard simple test — correlates excellently with VO₂max
- Estimated VO₂max = 6MWT distance (metres) ÷ 30
- Example: 6MWT of 450 m → VO₂max ≈ 15 mL/kg/min
- 6MWT <400 m → increased risk of postoperative cardiopulmonary complications after lobectomy
- Requires no laboratory equipment
Formal Cardiopulmonary Exercise Testing (CPET)
Gold standard — continuous measurement of respiratory gas exchange (O₂ uptake and CO₂ production) during bicycle or treadmill exercise for 8–12 minutes.
Key parameter: Maximal Oxygen Consumption (VO₂max)
| VO₂max | Risk Level |
|---|---|
| >20 mL/kg/min (>75% predicted) | Low risk — few complications |
| 15–20 mL/kg/min | Moderate — proceed with caution |
| <15 mL/kg/min | High risk |
| <10 mL/kg/min (<35% predicted) | Very high risk — consider alternative therapy |
VI. Preoperative Respiratory Investigation Algorithm
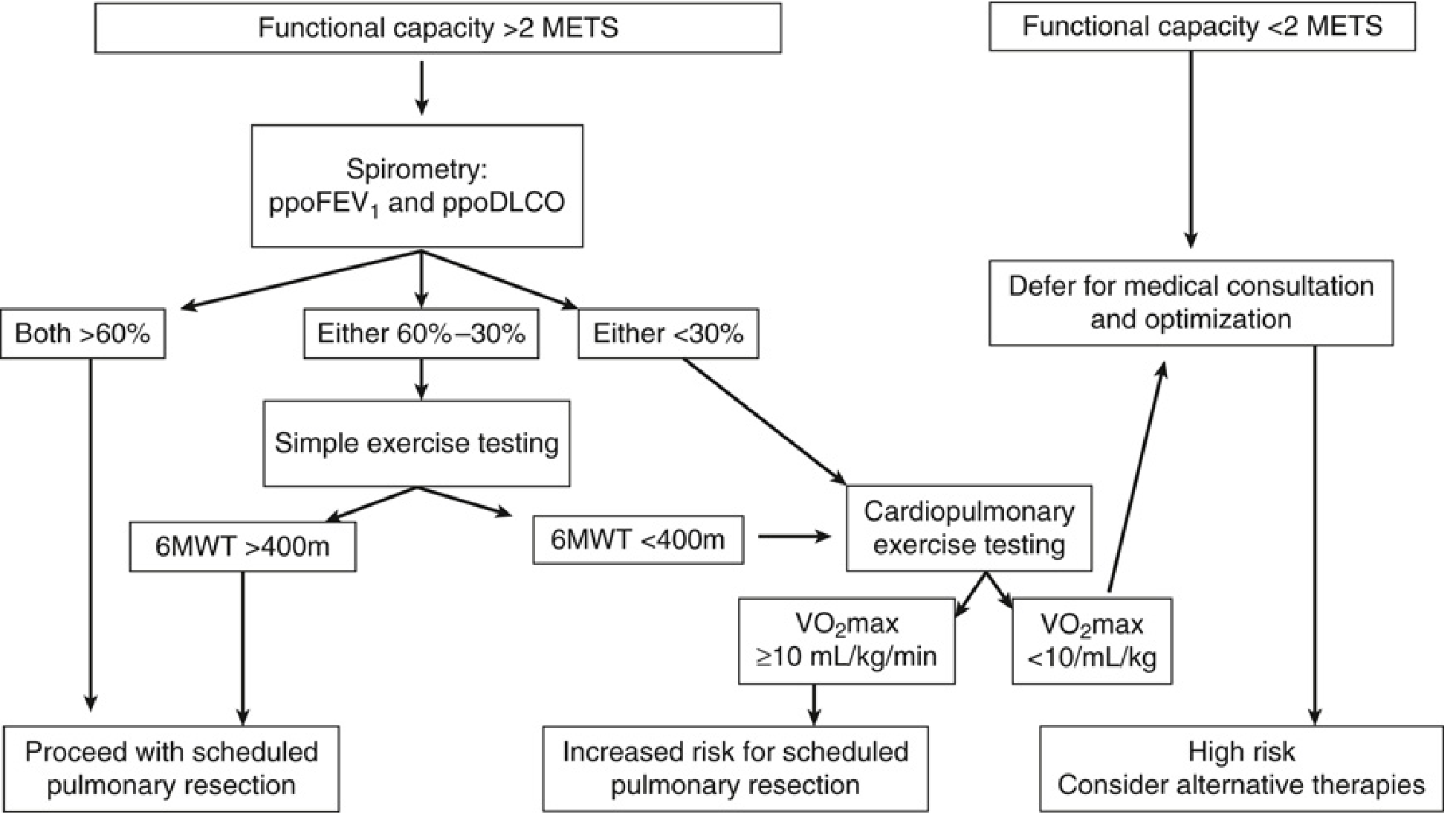
Miller's Anesthesia, 10e — Fig. 49.2: Flow diagram for preoperative respiratory investigation for pulmonary resection
Algorithm Summary:
- Functional capacity >2 METs → Perform spirometry (ppoFEV₁ and ppoDLCO)
- Both >60% → Proceed to surgery
- Either 60–30% → Simple exercise testing (6MWT)
- 6MWT >400 m → Proceed
- 6MWT <400 m → CPET
- Either <30% → CPET
- VO₂max ≥10 mL/kg/min → Increased risk; proceed with optimisation
- VO₂max <10 mL/kg/min → High risk — consider alternative therapies
- Functional capacity <2 METs → Defer for medical consultation and optimisation
VII. Ventilation-Perfusion (V/Q) Scintigraphy
Used when ppoFEV₁ values are borderline (30–40%) to more precisely estimate the contribution of the lobe/lung to be resected. Quantitative V/Q scanning combined with spirometry refines the prediction of postoperative pulmonary function.
Formula:
$$\text{ppoFEV}_1 = \text{preFEV}_1 \times (1 - \text{fractional contribution of resected lung})$$
This allows surgery to be considered in borderline patients whose diseased segment contributes very little to overall function.
VIII. Chest Radiograph and CT Chest
- Routine preoperative CXR is NOT recommended for all patients before non-cardiothoracic surgery
- Appropriate for patients with COPD, asthma, or known pulmonary disease
- HRCT chest is essential for evaluating parenchymal disease, bullae, and surgical planning
- In thoracic cases: CT delineates tumour location, mediastinal involvement, and helps plan resection
IX. Assessment of Specific Conditions
COPD
- Optimise bronchodilator therapy (SABA, LABA, LAMA) before surgery
- Check baseline ABG for CO₂ retention
- Perioperative corticosteroids if severe obstruction
Asthma
- Ensure well-controlled with minimal wheeze
- Continue inhaled corticosteroids; add systemic steroids if needed
- Preoperative peak flow should be >80% of personal best
Obstructive Sleep Apnoea (OSA)
- STOP-BANG questionnaire for screening
- Polysomnography if indicated
- Ensure CPAP therapy compliance
- Impacts post-extubation monitoring plans
Smoking
- All patients should be counselled to stop smoking before surgery
- Meta-analyses have challenged earlier concerns about increased sputum in those who stopped close to surgery
X. Risk Modification — Perioperative Strategies
Preoperatively
- Smoking cessation
- Training in proper lung expansion techniques (incentive spirometry)
- Inhalation bronchodilator and/or corticosteroid therapy when indicated
- Control of infection and secretion
- Weight reduction when appropriate
- Physiotherapy and respiratory exercises
Intraoperatively
- Neuraxial anaesthesia (epidural/spinal) preferred — meta-analyses show lower rates of pneumonia and respiratory failure vs. general anaesthesia
- Limit duration of anaesthesia
- Avoid long-acting neuromuscular blocking drugs
- Prevent aspiration; maintain optimal bronchodilation
- Lung-protective ventilation during OLV (tidal volume 4–6 mL/kg IBW + titrated PEEP)
Postoperatively
- Thoracic epidural analgesia (>24 h) — reduces splinting, aids deep breathing
- Incentive spirometry and deep breathing exercises
- Early ambulation
- Postural drainage, percussion, vibration
- Suctioning and cough encouragement
- Selective nasogastric tube (for symptomatic distension)
- Adequate pain control without excessive opioids
XI. Role of Spirometry Before Non-Thoracic Surgery
According to evidence-based guidelines (American College of Physicians):
- Routine preoperative spirometry is NOT recommended for estimating pulmonary complication risk in non-cardiothoracic surgery
- Spirometry may be appropriate for COPD or asthma patients
- It does not provide a threshold below which extrathoracic surgery risk is unacceptable
- For coronary artery bypass grafting, spirometry is of value in determining candidacy
- For lung resection surgery, spirometry (with ppoFEV₁ calculation) is mandatory
XII. Summary Table — Key Thresholds
| Parameter | Threshold | Implication |
|---|---|---|
| ppoFEV₁ | >40% | Low risk; extubate in OR |
| ppoFEV₁ | 30–40% | Intermediate; further testing |
| ppoFEV₁ | <30% | High risk (open); <20% very high |
| ppoDLCO | <40% | Increased respiratory + cardiac risk |
| PaO₂ | <60 mmHg | Warning indicator |
| PaCO₂ | >45 mmHg | Warning indicator |
| VO₂max | >20 mL/kg/min | Low risk |
| VO₂max | <15 mL/kg/min | High risk |
| VO₂max | <10 mL/kg/min | Very high risk |
| 6MWT | <400 m | Proceed to CPET |
| Albumin | <3.5 g/dL | Independent risk factor |
Conclusion
The preoperative respiratory evaluation is a structured, sequential assessment that begins with clinical history and risk factor identification, proceeds through spirometry (ppoFEV₁, ppoDLCO), gas exchange (ABG), and exercise capacity (6MWT/CPET), and culminates in a risk-stratified management plan. The "three-legged stool" framework — lung mechanics, parenchymal function, and cardiopulmonary interaction — ensures no critical domain is missed. Patients at elevated risk benefit from preoperative optimisation through bronchodilator therapy, physiotherapy, smoking cessation, and careful anaesthetic planning. The advent of VATS and robotic surgery has expanded operability in patients previously deemed inoperable by conventional thresholds.
Sources: Miller's Anesthesia 10e (Slinger P); Harrison's Principles of Internal Medicine 22e; Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.