Hi
Hey! How can I help you today?

Give me these topic from guy ton in an answer format with pictures
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
All 6 topics are covered. Here's a quick summary of what's included:
Topics Covered (All from Guyton):
-
Normal ECG - Waves (P, QRS, T), how it's recorded, all leads (bipolar + augmented + chest), P-R interval significance, and Einthoven's Law (Lead II = Lead I + Lead III) - with labeled ECG diagrams
-
Cardiac Cycle - All 7 phases, pressure/volume changes, ejection fraction formula (normal ~60%), all 4 heart sounds with causes, and Frank-Starling law
-
Cardiac Output & Venous Return - Definition, Fick principle formula, cardiac index, all factors affecting CO and venous return, factors affecting stroke volume - with blood flow distribution diagram
-
Long-term BP Regulation - Full renin-angiotensin cascade, role of JGA (baroreceptor + macula densa), pressure-natriuresis mechanism, aldosterone/ADH - with equilibrium pressure graph
-
Coronary Circulation - All peculiarities (diastolic flow dominance, high O₂ extraction, etc.), metabolic regulation (adenosine), angina types + ECG changes, MI ECG sequence, and full table of cardiorespiratory changes during exercise
-
Circulatory Shock - 4-type classification table, 3 stages with physiological explanation, hypovolemic shock management principles
Glomerular filtration
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have everything needed for a thorough answer. Let me compile it.
Glomerular Filtration
(Guyton and Hall Textbook of Medical Physiology, 14th Edition)
Definition
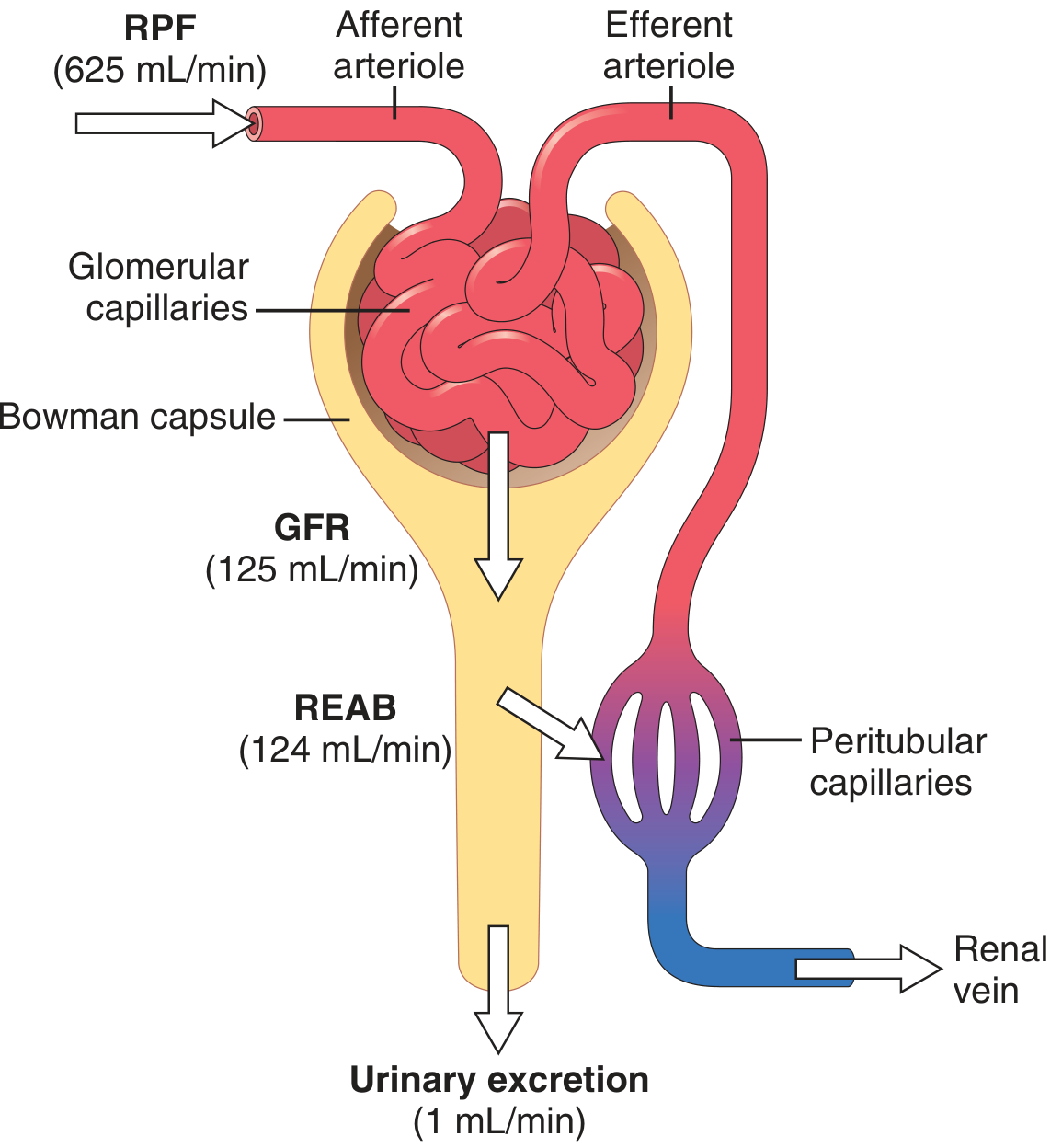
Glomerular filtration is the first step in urine formation - it involves the filtration of large amounts of fluid from the glomerular capillaries into the Bowman capsule. Approximately 180 L/day (125 mL/min) is filtered, of which more than 99% is reabsorbed, leaving only ~1 mL/min as final urine output.
Excretion = Filtration - Reabsorption + Secretion
The Glomerular Filtration Membrane
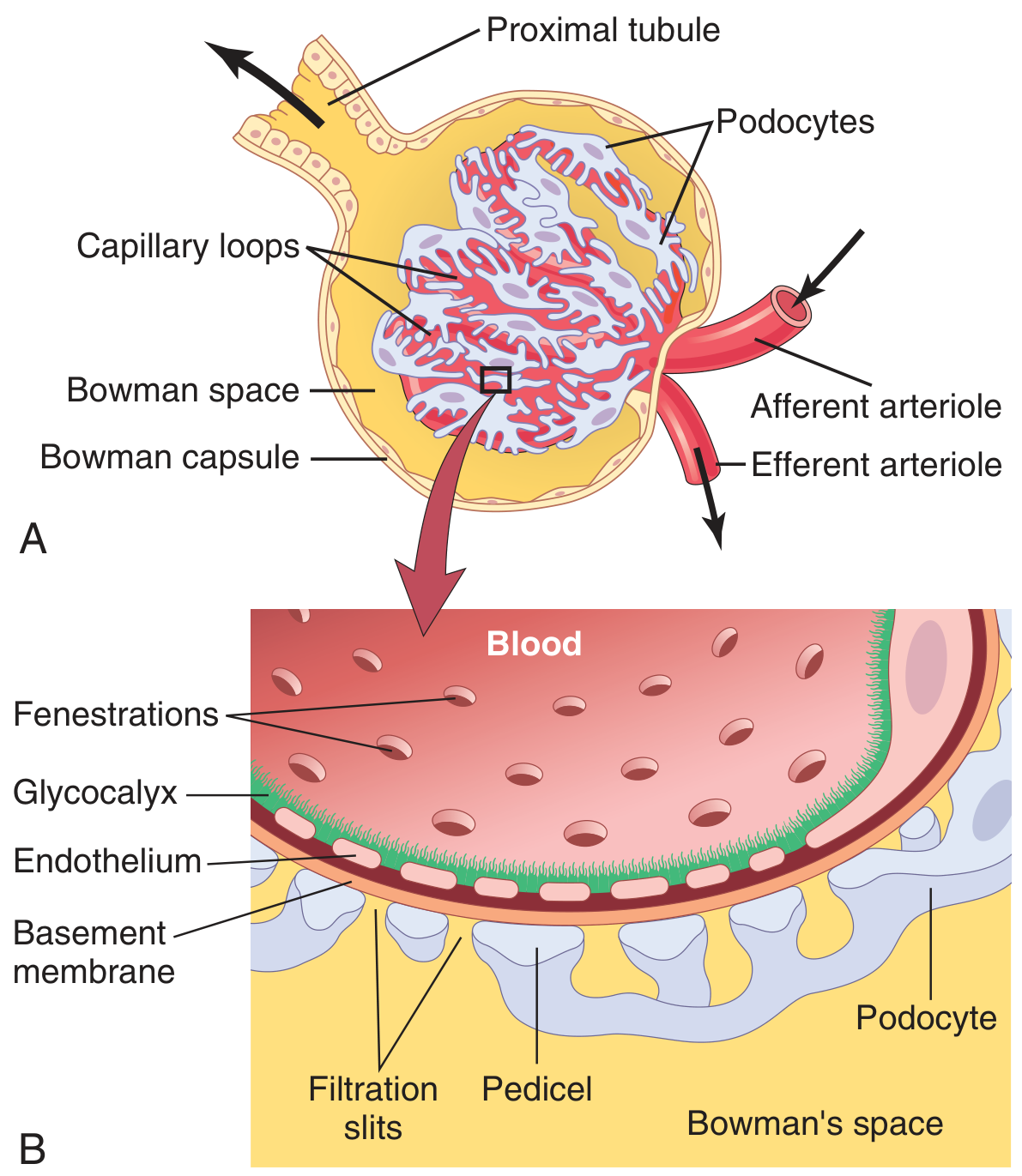
The glomerular capillary membrane has 3 layers, each acting as a filtration barrier:
1. Fenestrated Capillary Endothelium
- Perforated by thousands of tiny holes called fenestrae (~8 nm / 80 Å)
- Allows rapid passage of water and small solutes
- Endothelial proteins carry fixed negative charges (glycocalyx) - repel plasma proteins
2. Glomerular Basement Membrane (GBM)
- A meshwork of collagen and proteoglycan fibrillae
- Large spaces allow water and small solutes to pass freely
- Strongly negatively charged - major barrier to plasma proteins
- Damaged in diseases like diabetes (thickened GBM) and Goodpasture syndrome
3. Epithelial Cell Layer (Podocytes)
- Not a continuous layer; podocytes have long foot processes called pedicels
- Pedicels are separated by filtration slits bridged by thin slit diaphragms
- Slit diaphragm contains proteins nephrin and podocin - critical for preventing proteinuria
- Mutations in nephrin gene → absent filtration slit diaphragms → massive proteinuria
Filterability Table
| Substance | Molecular Weight | Filterability |
|---|---|---|
| Water | 18 | 1.0 (freely filtered) |
| Sodium | 23 | 1.0 |
| Glucose | 180 | 1.0 |
| Inulin | 5,500 | 1.0 |
| Myoglobin | 17,000 | 0.75 |
| Albumin | 69,000 | 0.005 (almost completely restricted) |
Key point: Filterability depends on both molecular size AND electrical charge. Negatively charged molecules are filtered less readily than neutral or positively charged molecules of the same size (because the GBM is negatively charged).
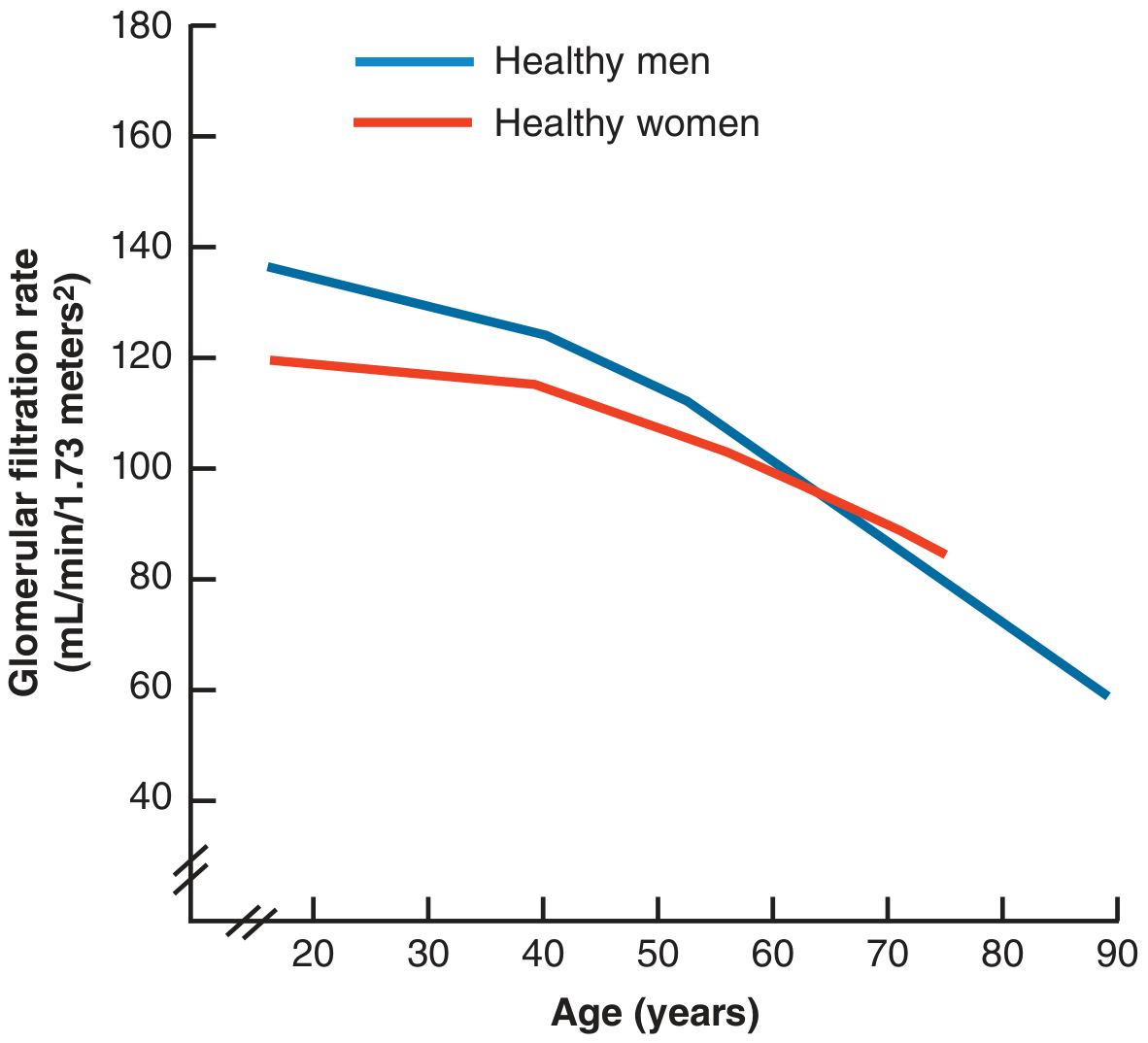
Glomerular Filtration Rate (GFR)
- Normal GFR = 125 mL/min (180 L/day)
- Women: ~10% lower than men
- GFR declines progressively with age (see graph below)
Filtration Fraction
Filtration Fraction = GFR / Renal Plasma Flow = 125 / 625 = ~0.2 (20%)
- ~20% of the plasma flowing through the kidneys is filtered each minute
- The kidneys receive 22% of total cardiac output (~1100 mL/min blood flow, ~625 mL/min plasma flow)
Starling Forces Determining GFR
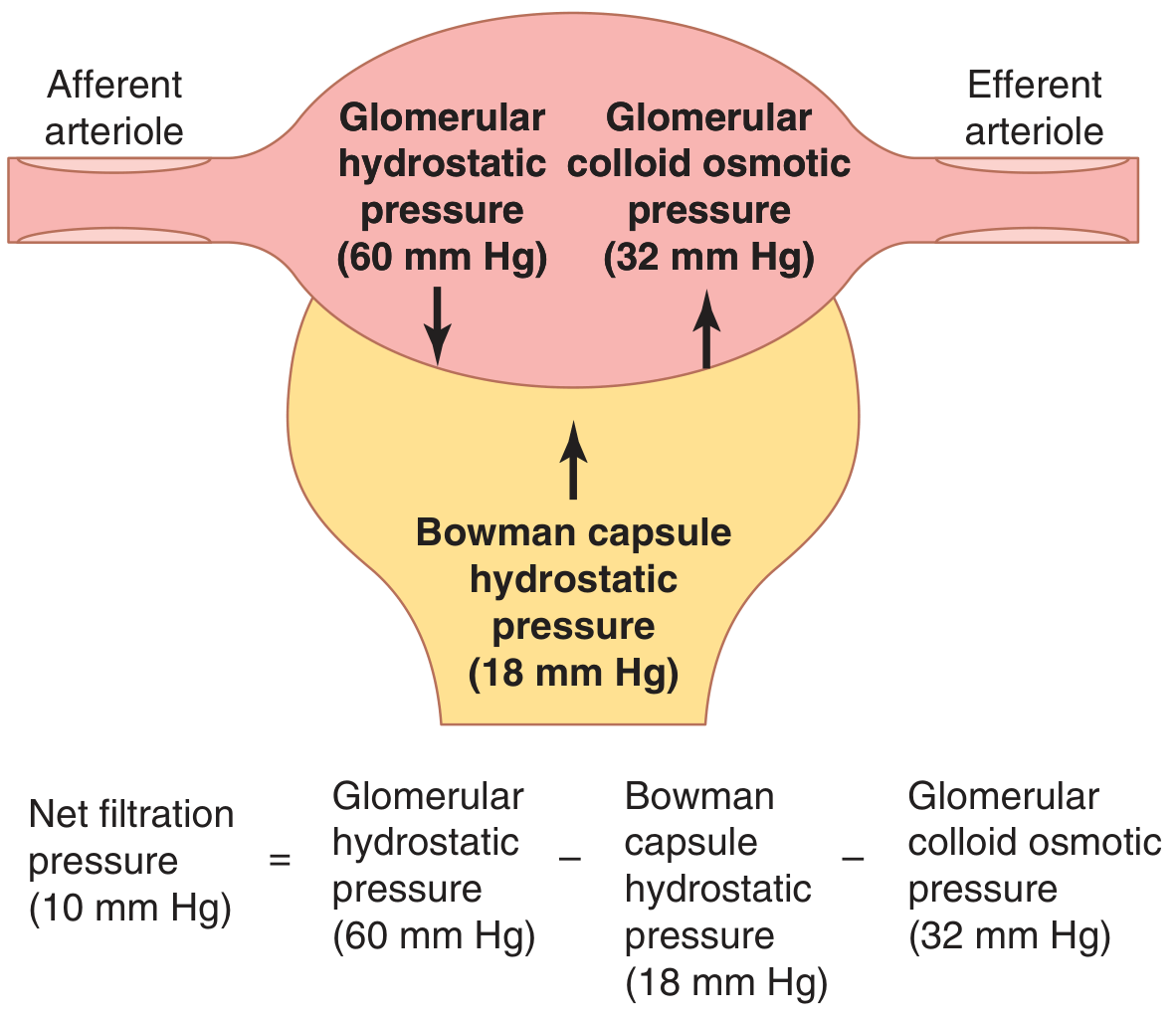
GFR = Kf × Net Filtration Pressure
Where:
| Force | Value (mmHg) | Direction |
|---|---|---|
| Glomerular hydrostatic pressure (PG) | 60 | Favors filtration ↓ |
| Bowman capsule colloid osmotic pressure (πB) | 0 (negligible protein) | Favors filtration |
| Bowman capsule hydrostatic pressure (PB) | 18 | Opposes filtration ↑ |
| Glomerular capillary colloid osmotic pressure (πG) | 32 | Opposes filtration ↑ |
Net Filtration Pressure = 60 - 18 - 32 = +10 mmHg
Filtration Coefficient (Kf)
Kf = GFR / Net filtration pressure = 125 / 10 = 12.5 mL/min/mmHg
- Kf is the product of hydraulic conductivity × filtration surface area
- Glomerular Kf is ~400x higher than in most other capillaries in the body
- Expressed per 100g kidney weight ≈ 4.2 mL/min/mmHg
- Reduced in chronic hypertension and glomerulonephritis (thickened GBM)
Factors Affecting GFR
1. Glomerular Hydrostatic Pressure (PG) - Primary Regulator
Determined by three variables:
| Variable | Effect on PG | Effect on GFR |
|---|---|---|
| ↑ Arterial pressure | ↑ PG | ↑ GFR |
| ↑ Afferent arteriolar resistance | ↓ PG | ↓ GFR |
| ↓ Afferent arteriolar resistance | ↑ PG | ↑ GFR |
| ↑ Efferent arteriolar resistance (mild) | ↑ PG | ↑ GFR |
| ↑ Efferent arteriolar resistance (severe >3x) | ↓ flow so much | ↓ GFR |
2. Bowman Capsule Hydrostatic Pressure (PB)
- Normal = 18 mmHg
- Increased by urinary tract obstruction (e.g., kidney stones, ureteral stones) → ↓ GFR → hydronephrosis if prolonged
3. Glomerular Colloid Osmotic Pressure (πG)
- Normal = 32 mmHg
- As blood passes through glomerular capillaries, ~1/5 of fluid is filtered → proteins concentrate → πG rises along the length of the capillary
- ↑ Plasma proteins → ↑ πG → ↓ GFR
- ↓ Plasma proteins (hypoalbuminemia, e.g., nephrotic syndrome, liver disease) → ↓ πG → ↑ GFR (filtration fraction increases)
- ↑ Renal blood flow → slower concentration of proteins → slower rise in πG → ↑ GFR
4. Filtration Coefficient (Kf)
- Decreased in diseases that reduce glomerular surface area or increase GBM thickness (e.g., chronic hypertension, glomerulonephritis, diabetic nephropathy)
Summary Table: Factors That Decrease GFR
| Factor | Mechanism |
|---|---|
| ↓ Arterial pressure (severe) | ↓ PG |
| ↑ Afferent arteriolar constriction | ↓ PG (angiotensin II, sympathetic stimulation) |
| ↑ Efferent arteriolar dilation | ↓ PG (ACE inhibitors, ARBs) |
| ↑ Bowman capsule pressure | Ureteral obstruction, kidney stones |
| ↑ Plasma protein concentration | ↑ πG |
| ↓ Kf | Glomerulonephritis, diabetes, hypertension |
Measurement of GFR - Inulin Clearance
Inulin is the gold standard for measuring GFR because it is:
- Freely filtered (filterability = 1.0)
- Not reabsorbed, secreted, or metabolized by the tubules
- Therefore: Amount filtered = Amount excreted
GFR = (Urine inulin conc. × Urine flow rate) / Plasma inulin conc.
In clinical practice, creatinine clearance approximates GFR (slightly overestimates because small amounts of creatinine are also secreted by the tubules).
Autoregulation of GFR and Renal Blood Flow
The kidneys maintain a relatively constant GFR over an arterial pressure range of 80-180 mmHg through two mechanisms:
- Myogenic mechanism - increased wall tension in the afferent arteriole causes smooth muscle contraction, reducing diameter and resistance compensation
- Tubuloglomerular feedback (TGF) - via the macula densa; increased NaCl delivery → adenosine and TXA₂ released → afferent arteriolar constriction → ↓ GFR (negative feedback)
All content sourced from Guyton and Hall Textbook of Medical Physiology, 14th Edition, Chapters 26-27.
All clinical cases from guy ton of renal physiology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Guyton covering all the major renal clinical cases. Let me compile the full answer.
All Clinical Cases from Guyton - Renal Physiology
(Guyton and Hall Textbook of Medical Physiology, 14th Edition)
CLINICAL CASE 1: Acute Kidney Injury (AKI)
Definition & Classification
AKI is an abrupt decrease in kidney function resulting in accumulation of waste products. Guyton classifies it into three categories:
| Type | Origin | Examples |
|---|---|---|
| Prerenal AKI | Decreased blood supply to kidneys | Heart failure, hemorrhage, burns, sepsis |
| Intrarenal AKI | Abnormalities within the kidney | Glomerulonephritis, tubular necrosis, toxins |
| Postrenal AKI | Obstruction of urinary tract | Kidney stones, prostatic hypertrophy, ureteral obstruction |
CASE 1A: Prerenal AKI
Causes of Decreased Renal Blood Flow:
| Category | Examples |
|---|---|
| Intravascular volume depletion | Hemorrhage (trauma, surgery, GI bleed, postpartum), diarrhea, vomiting, burns |
| Cardiac failure | Myocardial infarction, valvular damage |
| Peripheral vasodilation + hypotension | Anaphylactic shock, anesthesia, sepsis |
| Primary renal hemodynamic abnormality | Renal artery stenosis, embolism, renal vein thrombosis |
Pathophysiology:
- Normal renal blood flow ~1100 mL/min (~22% of cardiac output)
- As RBF falls → ↓ GFR → ↓ Na⁺ filtered → ↓ tubular reabsorption → ↓ O₂ consumption
- This protective reduction allows the kidney to tolerate reduced blood flow down to ~20-25% of normal without major cellular damage
- Below this level → tubular epithelial cells become hypoxic → cell death → intrarenal AKI
- Oliguria (urine output < fluid intake) develops when RBF is significantly reduced
- Anuria (complete cessation of urine output) may occur with very severe reduction
Clinical key: If the cause is corrected before permanent damage occurs, prerenal AKI is fully reversible. If ischemia persists for hours, it evolves into intrarenal AKI.
CASE 1B: Intrarenal AKI - Acute Glomerulonephritis
Causes of Intrarenal AKI:
Small vessel / glomerular injury: Vasculitis, polyarteritis nodosa, glomerulonephritis
Tubular injury: Acute tubular necrosis (ischemia, nephrotoxins - aminoglycosides, heavy metals, contrast dye)
Interstitial injury: Pyelonephritis, allergic interstitial nephritis (NSAIDs, penicillin)
Acute Glomerulonephritis:
- Most common cause: abnormal immune reaction 1-3 weeks after infection elsewhere in the body (classically Group A beta-hemolytic Streptococcus - post-streptococcal GN)
- Mechanism: antigen-antibody complexes deposit in glomerular capillaries → inflammatory reaction → ↓ GFR
- Features: hematuria, proteinuria, reduced urine output, edema, hypertension
- If the inflammation subsides, most patients recover; if severe/persistent → CKD
CASE 1C: Postrenal AKI
- Obstruction anywhere from the calyces to the bladder outlet
- Most common cause: kidney stones (calcium, urate, or cystine precipitation)
- Obstruction → ↑ Bowman capsule hydrostatic pressure → ↓ net filtration pressure → ↓ GFR → hydronephrosis
- Relief of obstruction usually restores GFR
CLINICAL CASE 2: Chronic Kidney Disease (CKD) and Uremia
Causes of CKD
| Category | Examples |
|---|---|
| Metabolic disorders | Diabetes mellitus (most common), obesity, amyloidosis |
| Hypertension | Nephrosclerosis |
| Immunological | Glomerulonephritis, polyarteritis nodosa, SLE (lupus erythematosus) |
| Infections | Pyelonephritis, tuberculosis |
| Primary tubular | Nephrotoxins (analgesics, heavy metals) |
| Urinary tract obstruction | Renal calculi, prostatic hypertrophy, urethral stricture |
| Congenital | Polycystic kidney disease, renal hypoplasia |
Key principle: Despite the variety of causes, the end result is always the same - progressive loss of functional nephrons.
The kidney can maintain relatively normal blood electrolyte concentrations and body fluid volumes until nephron number falls to less than 20-25% of normal. Below this, clinical uremia develops.
The Vicious Cycle of CKD → ESRD
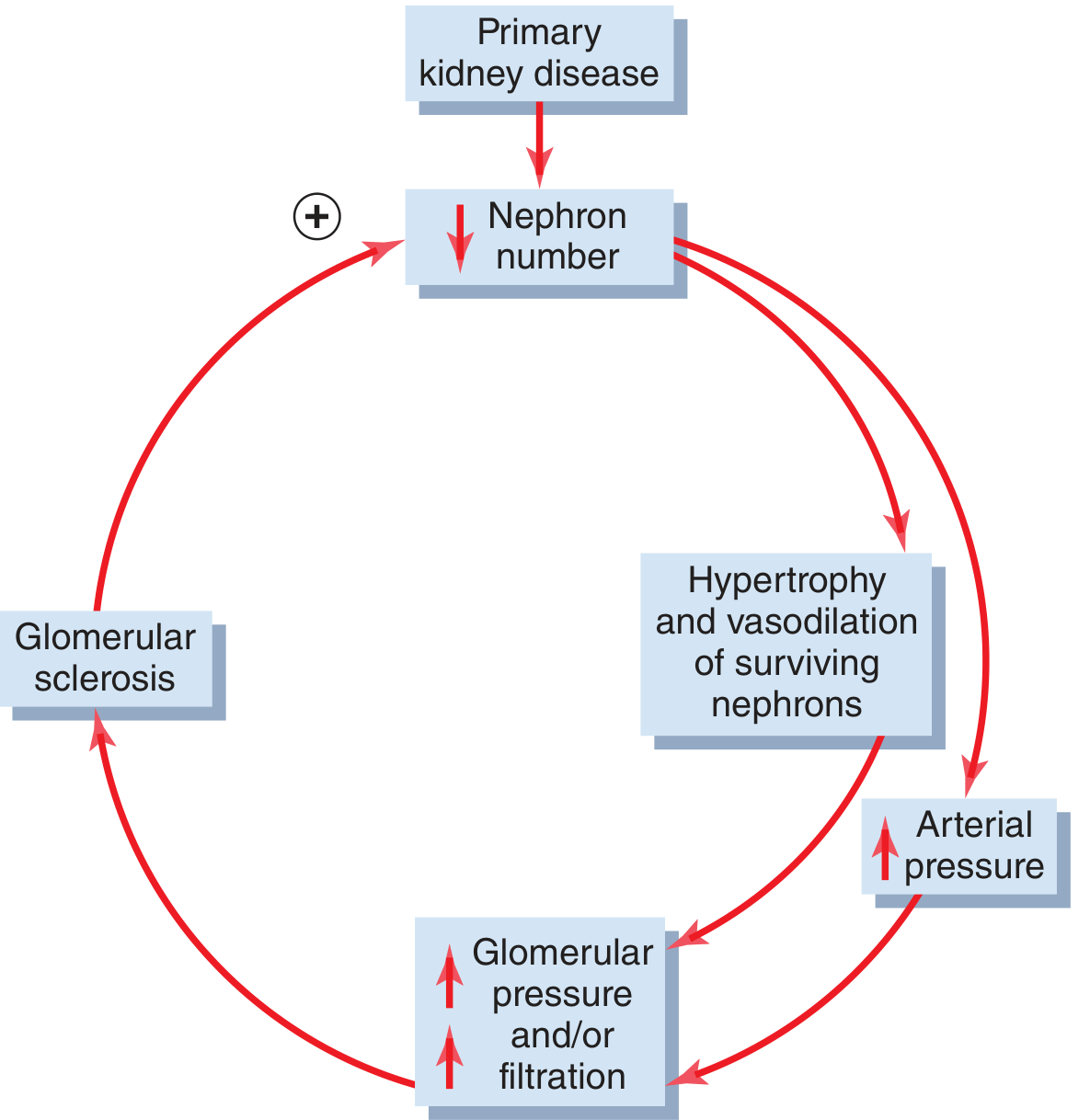
- Surviving nephrons hypertrophy and vasodilate to compensate
- This causes hyperfiltration in remaining nephrons → ↑ glomerular pressure
- Over time, high pressure damages surviving glomeruli → glomerular sclerosis
- This triggers further nephron loss → the cycle continues
- Ultimately leads to end-stage renal disease (ESRD)
Uremia - Effects of Renal Failure on Body Fluids
As renal function deteriorates and GFR approaches zero with continued food/water intake:
| Effect | Mechanism |
|---|---|
| Generalized edema | Water and salt retention (↓ urinary excretion) |
| Metabolic acidosis | Failure to excrete H⁺ and regenerate bicarbonate |
| ↑ BUN, creatinine, uric acid (azotemia) | Failure to excrete metabolic end products of protein |
| Hyperkalemia | Failure to excrete K⁺; life-threatening arrhythmias |
| Hyperphosphatemia | ↓ phosphate excretion → renal osteodystrophy |
| Hypocalcemia | ↓ renal activation of Vitamin D → ↓ Ca²⁺ absorption |
| Hypertension | Na⁺/water retention → ↑ blood volume |
| Anemia | ↓ erythropoietin production |
Isosthenuria - An early clinical sign of CKD: the kidney loses its ability to concentrate OR dilute urine. Urine osmolality approaches the osmolality of the glomerular filtrate (~300 mOsm/L, specific gravity ~1.010). Useful clinical test: water restriction for 12+ hours - inability to concentrate urine is evidence of CKD.
CLINICAL CASE 3: Nephrotic Syndrome
Definition: Massive proteinuria (>3.5 g/day) due to increased glomerular capillary permeability, causing loss of 30-50 g of plasma protein per day in the urine.
Pathophysiology:
- Glomerular capillary permeability ↑ → plasma proteins (especially albumin) leak into filtrate
- Plasma protein concentration falls to <1/3 of normal → plasma colloid osmotic pressure falls markedly
- Capillaries throughout the body filter excess fluid into tissues → massive edema
- Reduced plasma volume activates RAAS and sympathetic nervous system
- Kidneys retain Na⁺ and water → blood volume partially restored
- But proteins remain diluted → plasma oncotic pressure remains low → fluid continues leaking into tissues
- Vicious cycle: more Na⁺/water retention → more dilution of plasma proteins → more edema
Features:
- Massive pitting edema (anasarca)
- Proteinuria >3.5 g/day
- Hypoalbuminemia
- Hyperlipidemia and lipiduria (compensatory liver protein synthesis makes lipoproteins)
- Frothy urine
Causes: Minimal change disease (most common in children), membranous nephropathy, diabetic nephropathy, focal segmental glomerulosclerosis
CLINICAL CASE 4: Renal Interstitial Nephritis and Pyelonephritis
Pyelonephritis
- Bacterial infection of the renal interstitium, most commonly from E. coli (fecal origin)
- Route of infection: bloodstream, or more commonly ascending infection via ureters from bladder
Predisposing conditions:
- Incomplete bladder emptying - residual urine allows bacteria to multiply
- Urinary tract obstruction - impairs flushing of bacteria
- Vesicoureteral reflux - urine propelled back up ureters during micturition, carrying bacteria to the renal pelvis
Sequence: Cystitis (bladder infection) → vesicoureteral reflux → ascending to renal pelvis → pyelonephritis
Clinical effects:
- Primarily affects the medulla initially → impaired countercurrent mechanism → inability to concentrate urine (earliest sign)
- Long-standing pyelonephritis: progressive tubular, glomerular, and interstitial damage throughout the kidney → CKD
CLINICAL CASE 5: Tubular Transport Disorders
Bartter Syndrome
- Autosomal-recessive mutation in Na-K-2Cl transporter in the thick ascending limb of the loop of Henle
- Results in: impaired Na⁺ reabsorption → salt wasting → volume depletion → RAAS activation → hypokalemia, metabolic alkalosis, hyper-reninemia, hyperaldosteronism
- Blood pressure is normal or low (despite high renin/aldosterone) because volume depletion counteracts vasoconstriction
- Treatment: replace NaCl and K⁺; NSAIDs (reduce prostaglandin-mediated vasodilation); spironolactone (aldosterone antagonist)
Gitelman Syndrome
- Autosomal-recessive mutation in thiazide-sensitive NaCl co-transporter in the distal tubule
- Similar to Bartter syndrome but milder: salt wasting, volume depletion, RAAS activation, hypokalemia, metabolic alkalosis
- Also associated with hypomagnesemia (impaired Mg²⁺ reabsorption in distal tubule)
- Treatment: NaCl + K⁺ + Mg²⁺ supplementation; spironolactone
Liddle Syndrome
- Autosomal-dominant gain-of-function mutation in amiloride-sensitive epithelial Na⁺ channel (ENaC) in distal and collecting tubules
- Results in: excessive Na⁺ reabsorption → hypertension, metabolic alkalosis, hypokalemia
- Resembles primary hyperaldosteronism BUT: renin is low, aldosterone is low (because Na⁺ retention suppresses the RAAS)
- Treatment: amiloride (directly blocks ENaC); NOT spironolactone (because aldosterone is not elevated)
CLINICAL CASE 6: Renal Artery Stenosis - Two-Kidney Goldblatt Hypertension
Scenario: Stenosis of ONE renal artery with a normal contralateral kidney.
Mechanism:
- ↓ Pressure in ischemic kidney → ↑ Renin secretion → ↑ Angiotensin II
- Angiotensin II → vasoconstriction → ↑ arterial pressure
- ↑ Arterial pressure → normal kidney increases Na⁺/water excretion (pressure natriuresis)
- The ischemic kidney cannot respond to increased pressure (has low perfusion pressure)
- Net effect: sustained hypertension
- Elevated angiotensin II also causes the normal kidney to retain salt/water → adds to hypertension
Treatment: Revascularization (angioplasty, stenting) or ACE inhibitors/ARBs
Warning: ACE inhibitors in bilateral renal artery stenosis can cause AKI by removing the angiotensin II-driven efferent constriction that maintains GFR.
CLINICAL CASE 7: Treatment of Renal Failure - Dialysis
Indications for Dialysis
- Severe AKI (temporary, until kidney function recovers)
- ESRD (permanent) - over 800,000 patients in the USA are on ESRD therapy
Principles of Dialysis (Artificial Kidney)
- Blood passes through minute channels bounded by a thin semipermeable membrane
- On the other side of the membrane is a dialysate solution with a composition similar to normal plasma
- Small molecules (urea, creatinine, electrolytes) diffuse from blood into dialysate down concentration gradients
- Normal plasma electrolytes are maintained in the dialysate so they are NOT removed
- Larger molecules (proteins) are too big to pass through the membrane
Limitations of Dialysis vs. Transplantation
- Dialysis cannot replace all kidney functions (erythropoietin production, Vitamin D activation, renin-angiotensin regulation)
- Health of dialysis patients remains significantly impaired
- Kidney transplantation restores function more completely and patients live longer with fewer complications
- ~25,000 kidney transplantations are performed per year in the USA
- Requires lifelong immunosuppressive therapy → risk of infections and some cancers
All content from Guyton and Hall Textbook of Medical Physiology, 14th Edition, Chapters 26-32.
This is a shared conversation. Sign in to Orris to start your own chat.