Now I have enough from the library to synthesize a comprehensive, high-yield NEET PG / FMGE-focused answer. Let me compose it from my knowledge base, the textbook snippets, and Goodman & Gilman / Katzung sources retrieved.
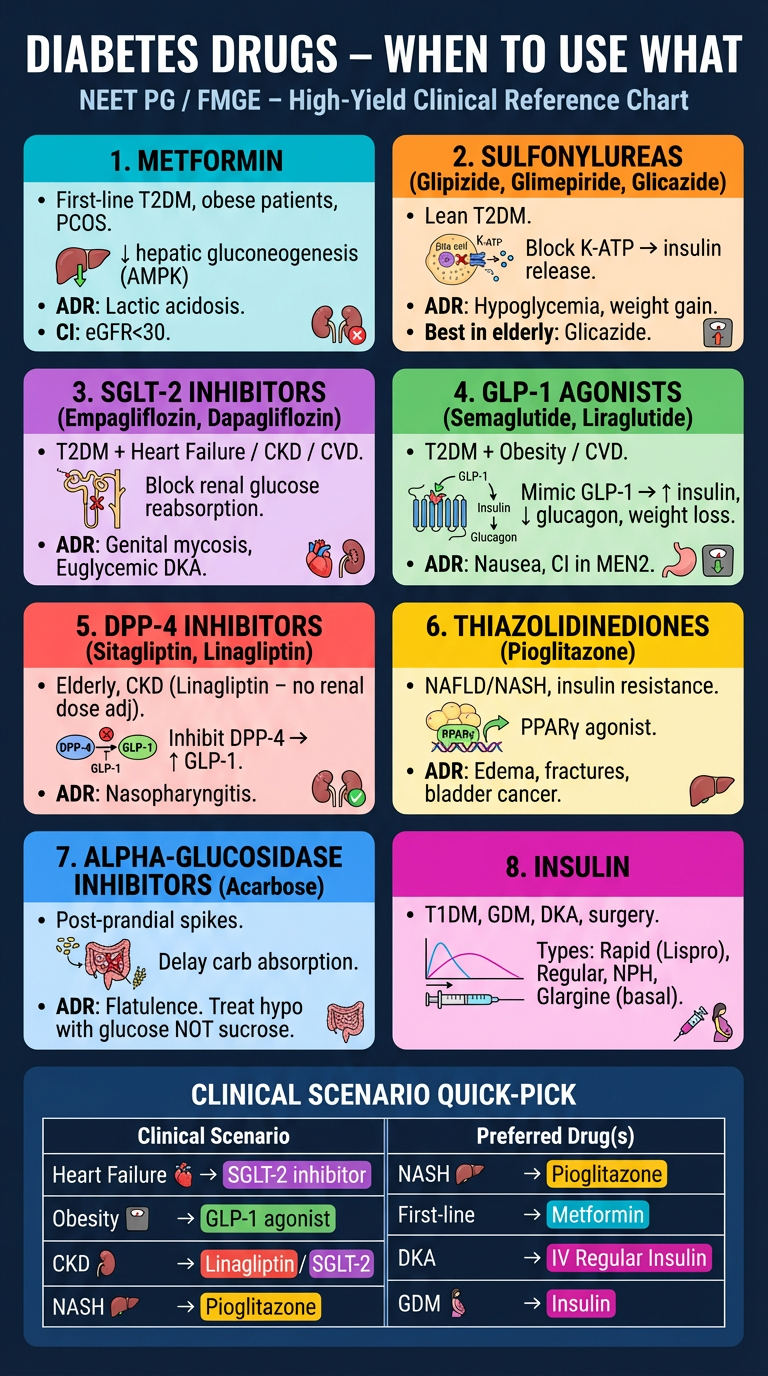
🩺 Diabetes Drugs — When to Use What (Clinical Logic)
High-Yield for NEET PG / FMGE
🔑 The Golden Framework
Every antidiabetic drug has a "clinical niche" — knowing WHEN to use which drug is the examiner's favorite.
1. METFORMIN (Biguanide)
| Feature | Detail |
|---|
| Mechanism | Activates AMPK → ↓ hepatic gluconeogenesis, ↑ peripheral insulin sensitivity |
| First-line for | T2DM — ALL patients unless contraindicated |
| Special merit | Obese T2DM (weight-neutral/↓ weight) |
| Extra indications | PCOS, pre-diabetes, prevention of T2DM |
| No hypoglycemia | ✅ (does not stimulate insulin secretion) |
| Key ADR | Lactic acidosis (rare), GI upset, B12 deficiency |
| Contraindications | eGFR < 30 (hold if < 45 before contrast), hepatic failure, alcoholism, heart failure (relative) |
Exam pearl: Metformin is the only oral antidiabetic proven to ↓ macrovascular events (UKPDS). It is also the drug of choice in obese T2DM patients. — Brenner and Rector's The Kidney
2. SULFONYLUREAS (SU)
Drugs: Glibenclamide (Glyburide) → 1st gen | Glipizide, Glimepiride, Glicazide → 2nd gen
| Feature | Detail |
|---|
| Mechanism | Block ATP-sensitive K⁺ channels on β-cells → depolarization → insulin release |
| Use when | Lean T2DM, elderly (glicazide preferred — lower hypo risk), cost-sensitive patients |
| Key ADR | Hypoglycemia (major concern), weight gain |
| Safest SU in elderly/CKD | Glicazide (hepatic metabolism, inactive metabolites) |
| Avoid in | Renal failure (accumulation → prolonged hypoglycemia), G6PD deficiency (glibenclamide → hemolysis) |
| Pregnancy | Glibenclamide used as alternative to insulin (in some guidelines) |
Exam pearl: Chlorpropamide (1st gen SU) → causes SIADH (dilutional hyponatremia), disulfiram-like reaction with alcohol, longest half-life.
3. THIAZOLIDINEDIONES / GLITAZONES
Drugs: Pioglitazone (in use) | Rosiglitazone (withdrawn in India/Europe)
| Feature | Detail |
|---|
| Mechanism | PPARγ agonist → ↑ insulin sensitivity in adipose/muscle, ↑ GLUT4 |
| Use when | Insulin-resistant T2DM (esp. with NAFLD — pioglitazone is beneficial), PCOS |
| Unique benefit | Pioglitazone ↑ HDL, ↓ TG, improves NASH |
| ADRs | Weight gain, fluid retention/edema, osteoporosis (↑ fracture risk), bladder cancer risk (pioglitazone — long-term) |
| Contraindicated | Heart failure (NYHA III/IV), osteoporosis, active bladder cancer, hepatic disease |
| Onset of action | Slow (weeks) |
Exam pearl: Rosiglitazone was withdrawn due to ↑ MI risk. Pioglitazone is neutral/beneficial for CV. Both ↑ risk of macular edema.
4. ALPHA-GLUCOSIDASE INHIBITORS
Drugs: Acarbose, Miglitol, Voglibose
| Feature | Detail |
|---|
| Mechanism | Inhibit intestinal α-glucosidase → delay carbohydrate digestion/absorption |
| Use when | Post-prandial hyperglycemia (BGpp control), as add-on |
| No hypoglycemia alone | ✅ (peripheral mechanism) |
| ADR | Flatulence, diarrhea, bloating (limits use) |
| Hypoglycemia treatment | Must use glucose (NOT sucrose — sucrase inhibited) |
| Contraindicated | IBD, cirrhosis, renal failure |
5. DPP-4 INHIBITORS ("Gliptins")
Drugs: Sitagliptin, Vildagliptin, Saxagliptin, Alogliptin, Linagliptin
| Feature | Detail |
|---|
| Mechanism | Inhibit DPP-4 enzyme → ↑ active GLP-1 and GIP → glucose-dependent insulin release |
| Use when | Elderly, CKD (linagliptin — entirely biliary excretion, no dose adjustment), add-on to metformin |
| Glucose-dependent | ✅ → minimal hypoglycemia risk |
| ADRs | Nasopharyngitis, pancreatitis (rare), joint pain, saxagliptin → ↑ HF hospitalizations |
| Weight | Neutral |
| Best in CKD | Linagliptin (no renal excretion) |
Exam pearl: Saxagliptin and alogliptin — avoid in heart failure (↑ hospitalization signal in trials).
6. GLP-1 RECEPTOR AGONISTS ("Glutides")
Drugs: Liraglutide, Semaglutide, Exenatide, Dulaglutide, Lixisenatide
| Feature | Detail |
|---|
| Mechanism | Mimic GLP-1 → ↑ insulin (glucose-dependent), ↓ glucagon, ↓ gastric emptying, ↑ satiety |
| Use when | T2DM + Obesity (weight loss), T2DM + CVD (MACE reduction proven) |
| CV benefit | Liraglutide (LEADER trial) & Semaglutide (SUSTAIN-6) → ↓ MACE, ↓ CV death |
| Obesity | Semaglutide (Ozempic/Wegovy) approved for obesity; liraglutide (Saxenda) approved for obesity |
| ADRs | Nausea/vomiting (most common, transient), pancreatitis, thyroid C-cell tumors (animal data, contraindicated in MEN2/medullary thyroid Ca) |
| Weight | ↓↓ (significant) |
| Route | Injectable (mostly); oral semaglutide available |
Exam pearl: GLP-1 agonists slow gastric emptying → useful in post-prandial hyperglycemia; also ↑ natriuresis. Contraindicated in personal/family history of medullary thyroid carcinoma or MEN2. — Katzung's Basic and Clinical Pharmacology
7. SGLT-2 INHIBITORS ("Gliflozins")
Drugs: Empagliflozin, Dapagliflozin, Canagliflozin, Ertugliflozin
| Feature | Detail |
|---|
| Mechanism | Inhibit SGLT-2 in PCT → ↓ glucose reabsorption → glucosuria + natriuresis |
| Use when | T2DM + Heart Failure (HFrEF + HFpEF — empagliflozin), T2DM + CKD (dapagliflozin/canagliflozin — slow progression), T2DM + CVD |
| MACE reduction | Empagliflozin (EMPA-REG), Canagliflozin (CANVAS), Dapagliflozin (DECLARE) |
| Renal protection | Dapagliflozin approved for CKD (even without T2DM) |
| HF | Dapagliflozin (HFrEF), Empagliflozin (both HFrEF + HFpEF) |
| ADRs | Genital mycotic infections (most common), UTI, DKA (euglycemic DKA — rare), Fournier's gangrene, polyuria, dehydration, ↑ fractures/amputations (canagliflozin) |
| Weight | ↓ |
| Contraindicated | eGFR < 45 (for glucose lowering), T1DM (risk of DKA), recurrent UTI |
Exam pearl: SGLT-2 inhibitors cause euglycemic DKA — blood sugar may be near-normal but patient is acidotic. The mechanism involves ↑ glucagon, ↑ ketogenesis. Always suspect in a patient on gliflozins presenting with metabolic acidosis. — Brenner and Rector's The Kidney; Goodman & Gilman's
8. MEGLITINIDES (Glinides)
Drugs: Repaglinide, Nateglinide
| Feature | Detail |
|---|
| Mechanism | Also block K-ATP channels on β-cells (like SU) but different binding site, shorter action |
| Use when | Post-prandial hyperglycemia, irregular meal patterns (taken with meals, skipped if meal skipped) |
| Advantage over SU | Shorter duration → less hypoglycemia |
| Repaglinide | Safe in renal failure (biliary excretion) |
| ADR | Hypoglycemia (less than SU), weight gain |
9. INSULIN
| Indication | Clinical Scenario |
|---|
| T1DM | Mandatory |
| T2DM | When HbA1c > 10%, symptomatic hyperglycemia, oral drugs fail |
| Gestational DM | When diet fails (insulin is first-line pharmacologic tx in GDM) |
| Acute illness | Surgery, infections, MI, ICU |
| DKA / HHS | IV regular insulin |
Types:
| Type | Onset | Duration | When to give |
|---|
| Rapid-acting (Lispro, Aspart, Glulisine) | 5-15 min | 3-5 h | Just before meals |
| Regular (Soluble) | 30-60 min | 6-8 h | 30 min before meals; IV in DKA |
| NPH (Isophane) | 2-4 h | 12-18 h | Intermediate, twice daily |
| Long-acting (Glargine, Detemir) | 1-2 h | 20-24 h | Once daily basal coverage |
| Ultra long-acting (Degludec) | — | >42 h | Once daily; most stable |
Exam pearl: Insulin is the ONLY antidiabetic safe in ALL situations — pregnancy, liver disease, renal failure (dose adjustment needed), surgery. Lispro/Aspart can be used in pregnancy.
🔥 High-Yield Clinical Scenario Table
| Clinical Scenario | Drug of Choice |
|---|
| T2DM, first-line | Metformin |
| T2DM + Obesity | GLP-1 agonist (semaglutide/liraglutide) or SGLT-2 inhibitor |
| T2DM + Heart Failure | SGLT-2 inhibitor (empagliflozin/dapagliflozin) |
| T2DM + CKD (proteinuria) | SGLT-2 inhibitor (+ RAAS blocker) |
| T2DM + ASCVD/CVD | SGLT-2 inhibitor or GLP-1 agonist |
| T2DM + NAFLD/NASH | Pioglitazone |
| T2DM + Elderly (avoid hypo) | Glicazide or DPP-4 inhibitor (linagliptin in CKD) |
| T2DM + Renal failure (dialysis) | Repaglinide, dose-adjusted insulin; linagliptin |
| T2DM + Postprandial spikes | Alpha-glucosidase inhibitor or meglitinide |
| T2DM + Irregular meals | Repaglinide/Nateglinide (eat-skip, take-skip) |
| T2DM + PCOS | Metformin ± pioglitazone |
| Gestational DM (pharmacotherapy) | Insulin (preferred) or metformin/glibenclamide (alternatives) |
| DKA | IV regular insulin + fluids + K⁺ |
| Hyperosmolar Hyperglycemic State | IV regular insulin + aggressive hydration |
⚡ Drug-Specific "Only" Facts (Classic MCQ Traps)
| Fact | Drug |
|---|
| Only antidiabetic proven to ↓ macrovascular events (UKPDS) | Metformin |
| Causes SIADH + disulfiram reaction | Chlorpropamide |
| Euglycemic DKA | SGLT-2 inhibitors |
| Thyroid C-cell tumor risk (contraindicated in MEN2) | GLP-1 agonists |
| Lactic acidosis | Metformin (biguanides) |
| Weight loss + glucose control | GLP-1 agonists > SGLT-2 inhibitors |
| Safe in renal failure (biliary excretion) | Linagliptin, Repaglinide, Pioglitazone |
| ↑ HDL, beneficial in NASH | Pioglitazone |
| Bladder cancer risk | Pioglitazone (long-term) |
| Fracture risk + limb amputation | Canagliflozin |
| Genital fungal infection | SGLT-2 inhibitors |
| Must treat hypoglycemia with glucose (not sucrose) | Acarbose/Miglitol |
| Safe in G6PD deficiency (avoid glibenclamide) | Glicazide |
🧠 Mechanism Summary (1-liner each)
| Drug Class | 1-Line Mechanism |
|---|
| Metformin | ↓ hepatic glucose output via AMPK activation |
| Sulfonylureas | Block K-ATP → ↑ insulin secretion (glucose-independent) |
| Glinides | Same as SU but faster/shorter → meal-time coverage |
| TZDs | PPARγ agonist → ↑ insulin sensitivity |
| α-GI | Delay gut carb absorption |
| DPP-4 inhibitors | ↑ endogenous GLP-1/GIP → glucose-dependent insulin release |
| GLP-1 agonists | Exogenous GLP-1 → ↑ insulin, ↓ glucagon, ↓ appetite, slow gastric emptying |
| SGLT-2 inhibitors | ↓ renal glucose reabsorption → glucosuria + natriuresis |
| Insulin | Direct insulin replacement |
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics; Brenner and Rector's The Kidney; Katzung's Basic and Clinical Pharmacology, 16th Ed.