Explain D-dimer test
Reading File
Finding Sources
Searching PubMed
"D-dimer" AND "venous thromboembolism" AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbook sources along with excellent diagrams. Here is the complete, well-sourced answer:
D-Dimer Test
What Is D-Dimer?
D-dimer is a fibrin degradation product (FDP) - a small protein fragment released into the bloodstream when a blood clot (thrombus) is broken down by fibrinolysis. Its name comes from the two cross-linked "D" domains of fibrin that remain joined after plasmin cleaves the molecule.
Formation - How D-Dimer Is Generated
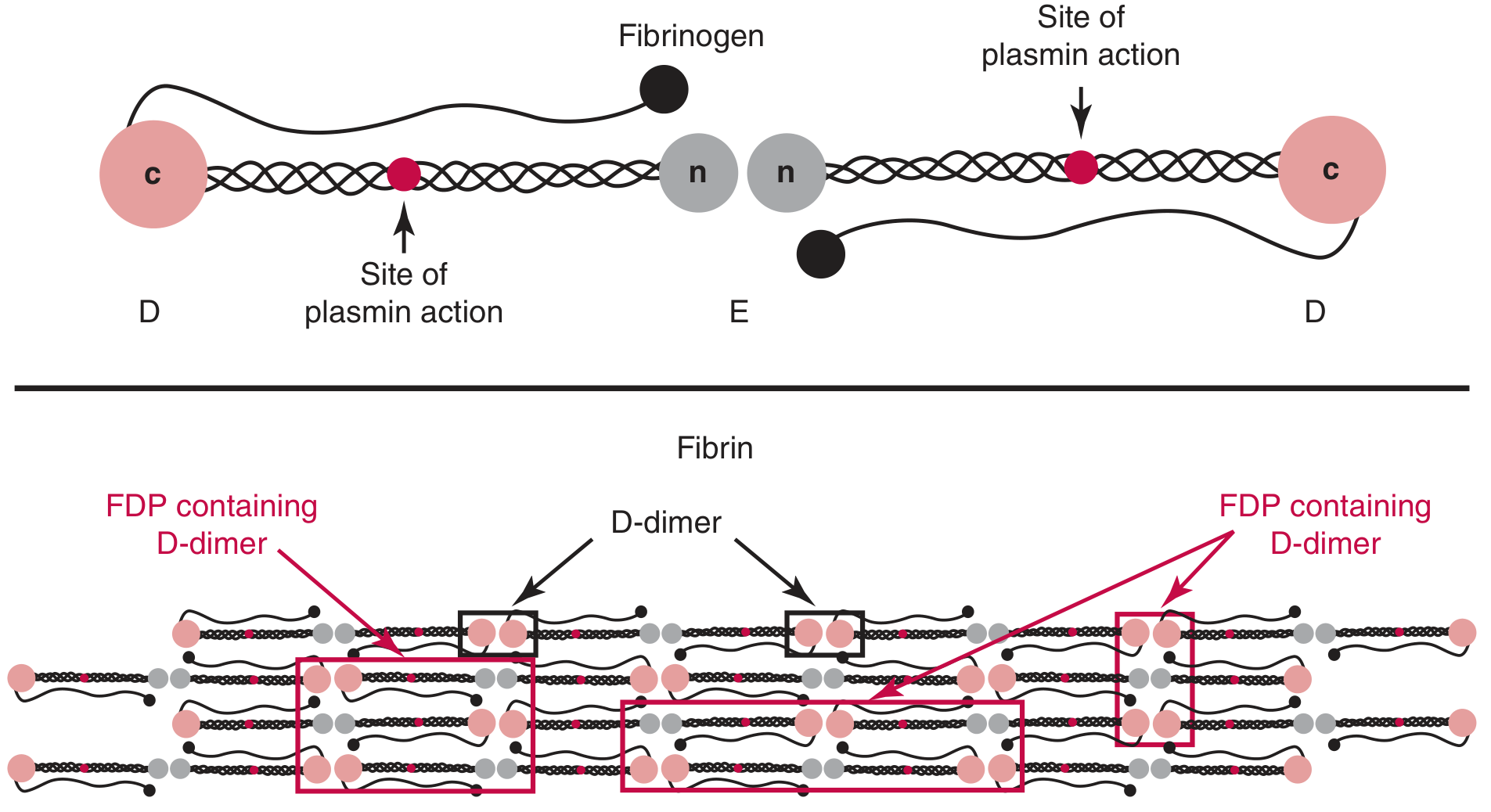
The key steps are:
- Thrombin cleaves fibrinogen (340 kDa) into fibrin monomer
- Fibrin monomers polymerize to form a fibrin network
- Factor XIIIa cross-links the D domains of adjacent fibers, forming the D-D epitope
- Plasmin (the key fibrinolytic enzyme) cleaves the fibrin between D and E domains
- Soluble fibrin degradation products (FDPs) containing the D-dimer moiety are released into plasma
D-dimer is specific to cross-linked fibrin - it is not generated by cleavage of fibrinogen, fibrin monomers, or non-cross-linked fibrin. - Tietz Textbook of Laboratory Medicine, 7th Ed.
Clinical Uses
1. Rule Out Venous Thromboembolism (DVT / PE) - PRIMARY USE
D-dimer is the most extensively studied and best-performing blood test for VTE. It is used as an exclusionary tool, not a confirmatory one.
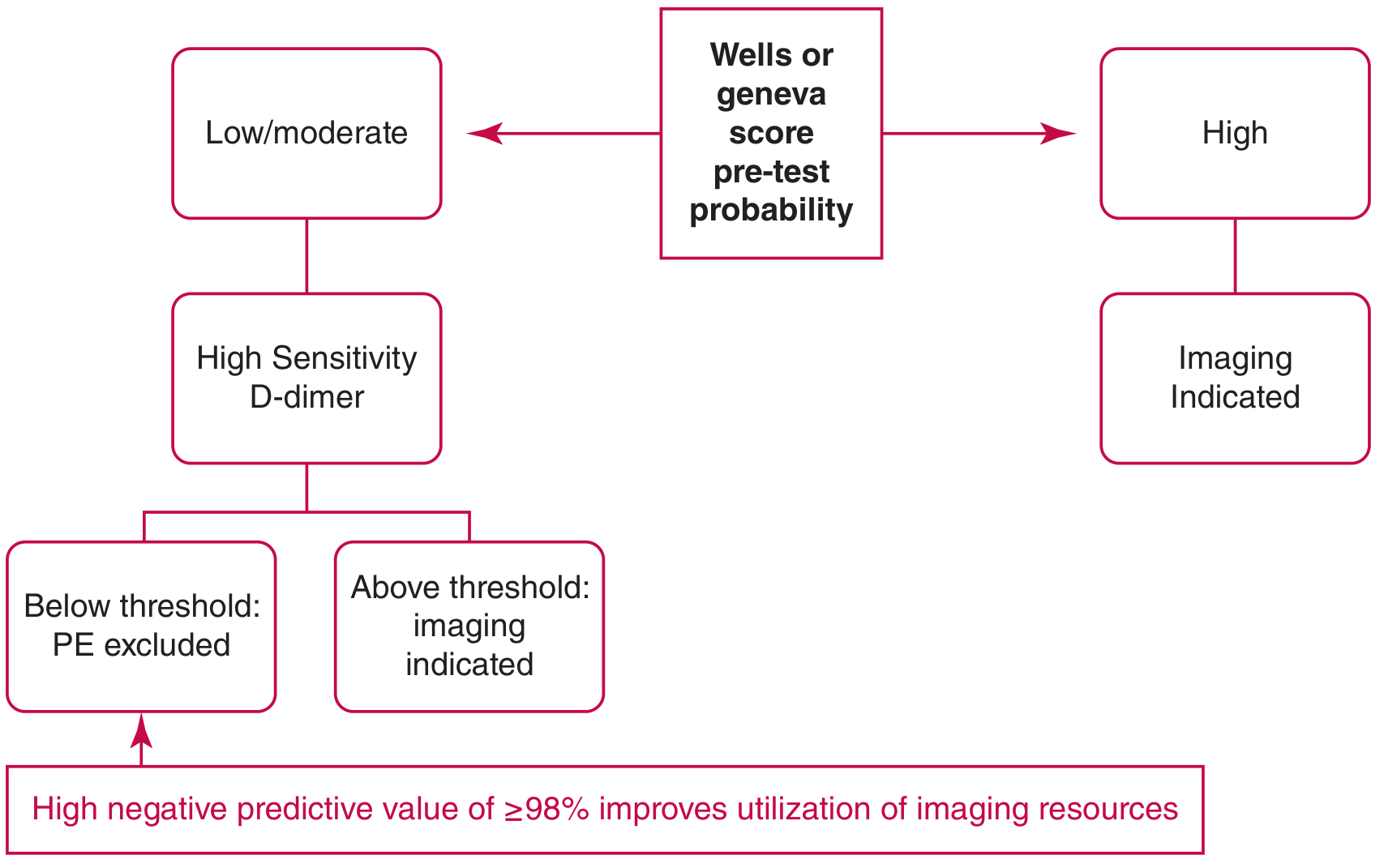
The logic:
- D-dimer below threshold + low/moderate pre-test probability → PE/DVT effectively ruled out; no imaging needed
- D-dimer elevated → Non-specific; imaging (CT pulmonary angiography or ultrasound) is required
- High pre-test probability → Do NOT measure D-dimer; proceed directly to imaging
D-dimer assays for VTE exclusion must meet minimum performance criteria: ≥98% sensitivity and ≥98% negative predictive value (lower CI at 95% and 90% respectively). - Tietz Textbook of Laboratory Medicine, 7th Ed.
2. Disseminated Intravascular Coagulation (DIC)
Quantitative D-dimer is useful in the evaluation of DIC, where simultaneous widespread clot formation and fibrinolysis produce markedly elevated D-dimer levels. - Tietz Textbook of Laboratory Medicine, 7th Ed.
3. Other Contexts
- Aortic dissection (elevated in most cases)
- COVID-19 and sepsis monitoring
- Pregnancy complications (pre-eclampsia, placental abruption)
Test Performance
| Parameter | Value |
|---|---|
| Sensitivity for PE/DVT | 95-98% |
| Specificity | 40-55% (low) |
| Negative predictive value | 99-100% |
D-dimer testing is highly sensitive but not specific. Elevated levels occur in nearly all patients with thromboembolism, but also in a wide range of other conditions. - Rosen's Emergency Medicine; Murray & Nadel's Textbook of Respiratory Medicine
Causes of Elevated D-Dimer (False Positives)
Because specificity is low, D-dimer can be elevated in many conditions besides VTE:
- Advanced age
- Pregnancy
- Surgery / trauma (postoperative period)
- Active malignancy / cancer
- Infection and sepsis
- Inflammatory states (rheumatic diseases, COVID-19)
- Liver disease
- Stroke
- Atrial fibrillation
- Renal failure
Causes of False-Negative D-Dimer
- Subacute or chronic PE (D-dimer has a half-life of < 8 hours in circulation)
- Severe lipemia
- Ongoing warfarin therapy
- Isolated subsegmental PE (small clot burden)
Assay Types and Reporting Units
Several assay formats exist with differing performance:
| Assay Type | Performance |
|---|---|
| ELISA / immunoturbidimetric / LIA | Highly sensitive; suitable for VTE exclusion |
| Latex agglutination (semiquantitative) | Lower sensitivity; NOT appropriate for VTE exclusion |
A critical source of confusion is the reporting units:
- D-Dimer Units (DDU): based on a D-dimer fragment (~185 kDa)
- Fibrinogen Equivalent Units (FEU): based on intact fibrinogen (~340 kDa)
- FEU is approximately twice DDU for the same sample
- Example: 500 ng/mL FEU = 250 ng/mL DDU
Using the wrong units can result in incorrect thresholds and missed diagnoses. Clinicians must know which unit system their lab uses. - Tietz Textbook of Laboratory Medicine, 7th Ed.; Murray & Nadel's Textbook of Respiratory Medicine
Standard Cutoff and Age-Adjusted D-Dimer
Standard cutoff: 500 ng/mL (FEU) is the traditional upper limit of normal.
Problem with elderly patients: D-dimer sensitivity is preserved across age groups, but specificity decreases markedly with age - leading to many false positives and unnecessary CT scans in older patients.
Age-adjusted D-dimer (for patients >50 years with low/intermediate pre-test probability):
Threshold = Age × 10 ng/mL (FEU)
For example, a 70-year-old patient's D-dimer threshold would be 700 ng/mL rather than 500 ng/mL.
This was prospectively validated in the ADJUST-PE trial (2014, Righini et al.), a multicenter multinational study showing:
- Increased percentage of patients in whom PE could be ruled out
- Failure rate of only 0.3% using the age-adjusted threshold
- 10-20% reduction in CT pulmonary angiograms in patients over 70
Note: The age-adjusted D-dimer applies to PE exclusion, not to suspected DVT. - Harrison's Principles of Internal Medicine 22E; Rosen's Emergency Medicine; Murray & Nadel's
Advanced Strategies: Variable Thresholds
YEARS Algorithm
Uses three clinical questions (signs of DVT, hemoptysis, PE as most likely diagnosis) to stratify patients:
- If none of the three are present: D-dimer threshold raised to 1000 ng/mL
- If any are present: standard 500 ng/mL threshold
- Validated in a large multicenter study; reduced need for CTPA by 14%
High Pre-Test Probability (PTP) Caveat
In patients with a HIGH pre-test probability (Wells score ≥6), do not order D-dimer - proceed directly to imaging. D-dimer is only useful when PTP is low or intermediate. A negative D-dimer in a high-PTP patient is unreliable and should not be used to exclude VTE. - Rosen's Emergency Medicine
Wells Score for DVT (Used Alongside D-Dimer)
| Clinical Characteristic | Score |
|---|---|
| Active cancer | +1 |
| Paralysis/paresis or plaster immobilization of legs | +1 |
| Bedridden ≥3 days or major surgery within 12 weeks | +1 |
| Localized tenderness along deep venous distribution | +1 |
| Entire leg swollen | +1 |
| Calf swelling ≥3 cm larger than asymptomatic side | +1 |
| Pitting edema in symptomatic leg only | +1 |
| Collateral superficial veins (non-varicose) | +1 |
| Previously documented DVT | +1 |
| Alternative diagnosis at least as likely as DVT | -2 |
Score <2: DVT unlikely → D-dimer can exclude DVT if negative
Score ≥2: DVT likely → proceed to imaging
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume
Summary
| Feature | Details |
|---|---|
| What it detects | Cross-linked fibrin degradation products |
| Primary use | Rule OUT VTE (DVT/PE) |
| Standard threshold | 500 ng/mL FEU |
| Age-adjusted threshold | Age × 10 ng/mL (for >50 years) |
| Sensitivity | 95-98% |
| Specificity | 40-55% (low) |
| NPV when negative | 99-100% |
| Used alone? | Only in LOW or INTERMEDIATE pre-test probability |
| High pre-test probability | Skip D-dimer; go directly to imaging |
The key clinical rule: A normal D-dimer in a patient with low/moderate pre-test probability effectively rules out VTE with very high confidence (~99-100% NPV) and avoids radiation exposure from CT scanning. A positive D-dimer is non-specific and always requires confirmatory imaging.
Sources: Tietz Textbook of Laboratory Medicine 7th Ed. | Harrison's Principles of Internal Medicine 22E | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases and Disorders | Rosen's Emergency Medicine | Recent evidence: ADJUST-PE validated age-adjusted D-dimer (PMID: 37452732 - van Es N et al., Eur Heart J 2023)
This is a shared conversation. Sign in to Orris to start your own chat.