Hi
Hey! How can I help you today?
DKA
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of DKA pathophysiology based on authoritative medical textbooks.
Diabetic Ketoacidosis (DKA) - Overview & Pathophysiology
Definition
DKA is an acute, life-threatening metabolic emergency defined by three core biochemical features (the "DKA triad"):
- Hyperglycemia - blood glucose >250 mg/dL (or a known history of diabetes)
- Ketonemia/Ketonuria - urinary ketones 2+ or serum ketones ≥3.0 mmol/L
- Metabolic acidosis - arterial/venous pH <7.3 (elevated anion gap)
It occurs predominantly in type 1 diabetes but is increasingly seen in type 2 diabetes, particularly in African Americans and Hispanics (ketosis-prone type 2 DM). - Goldman-Cecil Medicine
Core Mechanism: Insulin Deficiency + Counter-Regulatory Hormone Excess
DKA is fundamentally a state of cellular starvation - despite high blood glucose, cells cannot use it without insulin. The body responds by releasing counter-regulatory (catabolic) hormones.
Counter-regulatory hormones involved:
- Glucagon (primary driver)
- Catecholamines
- Cortisol
- Growth hormone
These four hormones act in concert to worsen the metabolic crisis.
Pathogenesis - Step by Step
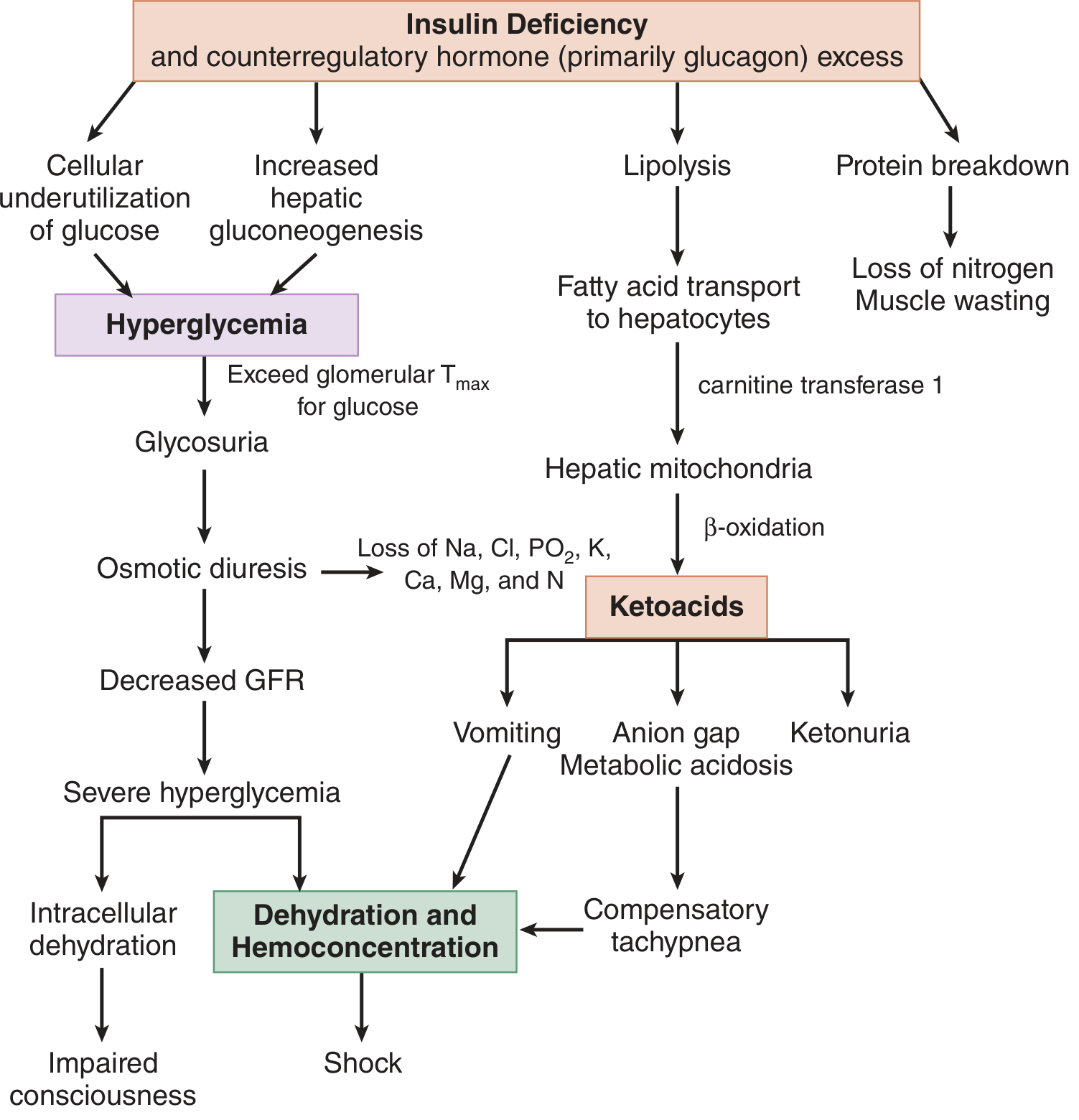
1. Hyperglycemia Pathway
| Insulin Action (Normal) | Effect of Deficiency |
|---|---|
| Promotes hepatic glycogen storage | Uncontrolled glycogenolysis |
| Suppresses gluconeogenesis | Increased hepatic gluconeogenesis (from amino acids, glycerol) |
| Promotes cellular glucose uptake | Cellular underutilization of glucose |
Result: Glucose floods the bloodstream but cannot be used by cells.
2. Osmotic Diuresis
- Hyperglycemia exceeds the renal tubular maximum (Tmax) for glucose reabsorption
- Glucose spills into urine (glycosuria), dragging water and electrolytes with it
- Massive losses of: Na, K, Cl, Mg, Ca, PO₄
- Decreased GFR worsens hyperglycemia further (less glucose filtered/excreted)
3. Ketogenesis Pathway
With insulin absent, adipose tissue undergoes uncontrolled lipolysis:
- Free fatty acids (FFAs) are released and transported to the liver
- FFAs enter hepatic mitochondria via carnitine transferase 1
- Undergo beta-oxidation → produce ketone bodies:
- Beta-hydroxybutyrate (β-HB) - predominant (ratio β-HB:AcAc ~3:1 in DKA)
- Acetoacetate (AcAc)
- Acetone (from spontaneous decarboxylation of AcAc - the fruity breath)
The two main ketones are in equilibrium: AcAc + NADH ⇌ β-HB + NAD⁺
Low/absent insulin also reduces the ability of brain, cardiac, and skeletal muscle to utilize ketones, worsening ketonemia.
4. Metabolic Acidosis
- Accumulation of β-HB and AcAc (both strong acids) causes an elevated anion gap metabolic acidosis
- Acidosis drives compensatory tachypnea (Kussmaul breathing) to blow off CO₂
- Renal loss of ketoanions represents a loss of potential bicarbonate
- In severe ketonuria, a superimposed hyperchloremic (normal anion gap) acidosis also develops as chloride is retained in exchange for excreted ketoanions
5. Protein Catabolism
Counter-regulatory hormones drive proteolysis in muscle:
- Amino acids are released and used as gluconeogenic precursors
- Leads to muscle wasting and nitrogen loss
6. Electrolyte Disturbances
- Potassium: Total body K⁺ is depleted (from osmotic diuresis + aldosterone activation from volume depletion). However, serum K⁺ may appear normal or HIGH initially because acidosis shifts K⁺ out of cells. As insulin is given and acidosis corrects, K⁺ moves back intracellularly - life-threatening hypokalemia can develop rapidly.
- Volume depletion activates the RAAS, which exacerbates renal potassium losses.
- Prostaglandins I₂ and E₂ are produced from adipose breakdown, causing paradoxical vasodilation despite profound volume depletion. - Tintinalli's Emergency Medicine
Why DKA Occurs Primarily in Type 1 vs. Type 2 Diabetes
| Feature | Type 1 DM | Type 2 DM |
|---|---|---|
| Insulin | Absent/severe deficiency | Relative deficiency |
| Residual insulin | None | Some present |
| Lipolysis suppression | Fails completely | Partially maintained |
| Ketosis | Readily develops | Usually suppressed (unless stressed) |
In type 2 DM, even small amounts of residual insulin are often enough to suppress lipolysis and prevent significant ketone production - hence why type 2 DM tends to develop HHS (hyperosmolar hyperglycemic state) rather than DKA. However, a mixed DKA/HHS picture can occur in type 2 with severe counter-regulatory stress. - Goldman-Cecil Medicine
Common Precipitants
Most common:
- Infection (pneumonia, UTI, etc.)
- Inadequate insulin / non-adherence
- New-onset type 1 diabetes
- Acute coronary syndrome
Other precipitants:
- Cerebrovascular accident, pulmonary embolism, pancreatitis
- Drugs: corticosteroids, SGLT-2 inhibitors (can cause euglycemic DKA), antipsychotics (clozapine, olanzapine), cocaine, lithium, thiazides
- Endocrinopathies: Cushing's, thyrotoxicosis, acromegaly, pheochromocytoma
- Pregnancy, major trauma, surgery
Key Summary
The core of DKA pathophysiology is a feed-forward cycle: insulin deficiency → hyperglycemia + lipolysis → osmotic diuresis + ketoacidosis → dehydration → worsening hyperglycemia + electrolyte depletion → shock and impaired consciousness if untreated.
Sources: Tintinalli's Emergency Medicine, 9e | Goldman-Cecil Medicine, International Edition
This is a shared conversation. Sign in to Orris to start your own chat.