reverse shoulder arthroplasty
Reading File
Finding Sources
Finding Sources
Searching PubMed
"reverse shoulder arthroplasty"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"shoulder arthroplasty" AND "reverse total"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
reverse shoulder arthroplasty prosthesis design glenosphere
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of reverse shoulder arthroplasty (RSA / rTSA).
Reverse Shoulder Arthroplasty (RSA)
Concept & Biomechanical Rationale
In a normal shoulder, the rotator cuff compresses and centers the humeral head against the glenoid, providing a stable fulcrum for the deltoid to generate elevation. When the rotator cuff is deficient, this fulcrum is lost and the deltoid can only shear the humeral head superiorly — resulting in pseudoparalysis.
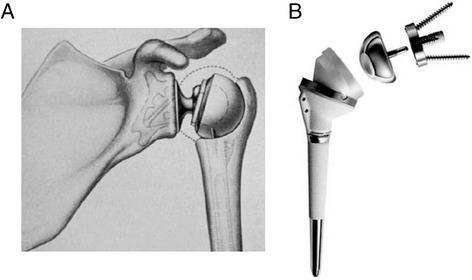
RSA inverts the ball-and-socket relationship: a hemispherical glenosphere (ball) is fixed to the glenoid, and a concave polyethylene socket is mounted on the humeral stem. This "reversal" of anatomy mediates two key effects:
- Medialization and distalization of the center of rotation (COR) — reduces shear stress on the glenoid component and decreases the risk of glenoid loosening
- Distalization of the humerus — increases deltoid tension and moment arm, allowing the deltoid alone to power forward elevation even without a functioning rotator cuff
An intact axillary nerve (and therefore a functional deltoid) is an absolute prerequisite for RSA. — Miller's Review of Orthopaedics, 9th ed.
Implant Components
| Component | Side | Description |
|---|---|---|
| Baseplate (metaglene) | Glenoid | Porous-coated, cementless; secured with central post/screw + peripheral screws |
| Glenosphere | Glenoid | Hemispherical ball attached to baseplate via Morse taper or screw |
| Humeral stem | Humerus | Cemented or press-fit; inserted into medullary canal |
| Humeral tray + polyethylene liner | Humerus | Concave socket that articulates with the glenosphere |
Design Evolution
Grammont "medialized" prosthesis (original):
- COR placed medial to the glenoid-bone interface
- 155° polyethylene opening angle (near-horizontal)
- Humerus positioned more medially and distally
- 0–10° retroversion recommended
Later designs (lateralized):
- Larger sphere, COR shifted more laterally
- 135° or 145° opening angle for better external rotation
- Onlay humeral bearing — lateralizes humerus without changing COR
- Reduced scapular notching and improved external rotation
— Rockwood and Green's Fractures in Adults, 10th ed., 2025
Indications
Primary indications:
- Cuff tear arthropathy (CTA) — the original indication; RSA is now the standard of care
- Massive irreparable rotator cuff tear with pseudoparalysis (without arthritis)
- Displaced proximal humeral fractures in the elderly — now the preferred arthroplasty over hemiarthroplasty; utilization increased from ~26% (2011) to ~67% (2015)
- Proximal humeral nonunion / malunion (especially with failed prior fixation)
- Glenohumeral arthritis with severe rotator cuff deficiency
- Failed anatomic total shoulder arthroplasty with cuff failure
- Severe glenoid retroversion (>15°) where eccentric reaming is inadequate
Key advantage over hemiarthroplasty for fractures:
Even if tuberosity healing fails, the patient retains active elevation/abduction — the deltoid compensates for rotator cuff absence.
Surgical Technique Highlights (Fracture Setting)
- Deltopectoral approach is standard
- Long head of biceps: tenotomy + tenodesis (to conjoined tendon)
- Humeral head excised early to create working space; saved as bone graft
- Glenoid preparation: baseplate placed low on the glenoid face, with ~10° inferior tilt — critical to prevent scapular notching
- Tuberosity reconstruction: repair of greater (and lesser) tuberosity around the stem is recommended for better external rotation and lower dislocation risk
- Tuberosity healing rate: 40–84%; greater tuberosity union correlates with ~40° active external rotation vs. ~28° with nonunion
- Autologous bone graft packed under tuberosities
- Balance between deltoid tension and tuberosity reconstruction is the central technical challenge
Outcomes
| Measure | Typical result (RSA for fracture) |
|---|---|
| Active forward elevation | ~90–110° |
| Active external rotation | ~28–40° (depends on tuberosity healing) |
| Modified Constant score | ~66–86% |
| Subjective satisfaction | ~85–92% |
| Revision rate | Lower than hemiarthroplasty |
RSA produces more reproducible outcomes than hemiarthroplasty because functional recovery is less dependent on tuberosity healing. Results for fracture indications are modestly inferior to RSA for CTA.
Outcomes are worse in patients >80 years. Comparison with nonoperative treatment in elderly displaced fractures shows variable results in the literature.
Component Positioning
| Parameter | Target |
|---|---|
| Glenosphere height | Low/inferior on glenoid face (flush or with inferior overhang) |
| Glenoid tilt | Neutral to 10° inferior |
| Humeral stem version | 25–40° retroversion |
| Glenosphere diameter | Larger = more stable (increases deltoid tension) |
Complications
1. Instability / Dislocation (~9%)
- Most common direction: anterior
- Classic mechanism: pushing up from chair armrests (shoulder hyperextension + external rotation)
- The humeral socket levers posteriorly and dislocates anteriorly
- Risk factors: subscapularis insufficiency (Grammont design), proximal humeral nonunion/bone loss, prior failed arthroplasty, fixed preoperative dislocation
- With lateralized prostheses, subscapularis repair is less critical for stability
2. Scapular Notching
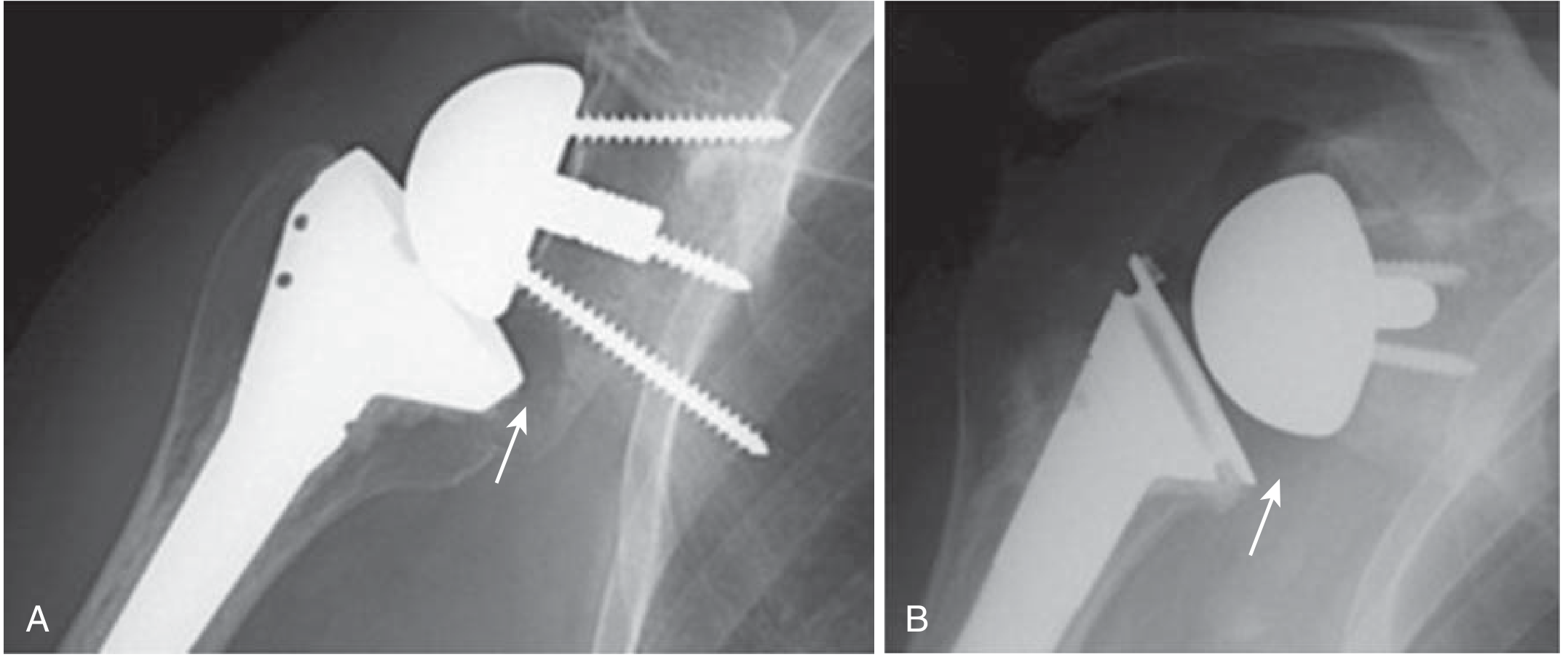
- Erosion of the scapular neck from repeated contact with the humeral tray/PE liner
- Incidence historically 50–90% with Grammont design; reduced significantly with lateralized modern implants
- Caused by 155° (horizontal) neck-shaft angle in Grammont prosthesis
- Consequences: pain, fracture, levering, dislocation
- Minimized by: low glenoid baseplate position, inferior tilt, larger glenosphere
3. Periprosthetic Fractures
- Acromion and scapular spine fractures — due to increased deltoid tension
- Humeral periprosthetic fractures
- Risk is higher with "humeral stem only" configurations
4. Infection
- Propionibacterium acnes and Staphylococcus spp. are most common
- Associated with male sex and younger age
5. Nerve injury
- Axillary nerve injury is catastrophic (eliminates deltoid function)
RSA vs. Other Shoulder Arthroplasty Options
| RSA | Anatomic TSA | Hemiarthroplasty | |
|---|---|---|---|
| Rotator cuff required? | No | Yes (intact cuff) | Preferred intact |
| Glenoid resurfaced? | Yes (reversed) | Yes (anatomic) | No |
| Best indication | CTA, cuff-deficient arthritis, PHF in elderly | Primary OA with intact cuff | AVN, young high-demand patient |
| Deltoid dependency | High | Low | Low |
Recent Evidence
- RSA vs. operative fixation for proximal humerus fractures (2024 systematic review & meta-analysis) — PMID 38038170
- Impact of rTSA on scapulohumeral rhythm (2026 systematic review) — PMID 40976550
Sources: Rockwood and Green's Fractures in Adults, 10th ed. 2025; Miller's Review of Orthopaedics, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.