Everything about bladder cancer in detail with reference to standard textbooks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bladder cancer" AND "urothelial carcinoma"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have extensive, authoritative content from multiple standard textbooks plus excellent visual diagrams. Let me compile the comprehensive answer.
Bladder Cancer - A Comprehensive Review
Sources: Campbell-Walsh-Wein Urology (11e), Goldman-Cecil Medicine, Bailey & Love's Short Practice of Surgery (28e), Gray's Anatomy for Students
1. Definition and Overview
Bladder cancer encompasses a spectrum of tumors arising from the urothelial lining of the bladder, renal pelvis, ureters, and urethra. Over 90% originate in the bladder itself. Transitional cell (urothelial) carcinoma is the most common histologic type. These tumors have a particular tendency for multifocality, high recurrence rates, and potential for progression to higher stages.
They are broadly classified into three categories that differ in clinical behavior, prognosis, and management:
- Non-muscle-invasive bladder cancer (NMIBC) - stages Tis, Ta, T1
- Muscle-invasive bladder cancer (MIBC) - stages T2-T4
- Metastatic disease
Long-term cure ranges from 99% for low-grade Ta tumors to approximately 15% for metastatic disease. - Goldman-Cecil Medicine
2. Epidemiology
| Parameter | Data |
|---|---|
| New US cases/year | ~80,000 |
| US deaths/year | ~17,000 |
| 5-year overall survival | 77% |
| Male:Female ratio | 3:1 |
| Rank in men | 4th most common cancer |
| Lifetime risk (men) | 1 in 27 |
| Lifetime risk (women) | 1 in 89 |
| White:Black prevalence | 2:1 |
| Median age at diagnosis | 73 years |
| Global cases (2015) | ~540,000 |
| Global deaths (2015) | ~188,000 |
Goldman-Cecil Medicine; Bailey & Love's Short Practice of Surgery (28e)
3. Etiology and Risk Factors
Carcinogens and their metabolites excreted in urine act directly on the urothelial lining. The latency period from initial exposure to cancer development is nearly 20 years.
3.1 Cigarette Smoking
- The leading risk factor, contributing to 50% of cancers in men and 25% in women
- Smokers have a 2-4 fold higher relative risk than non-smokers
- Duration of exposure matters more than intensity (cigarettes/day)
- Urothelial cellular atypia found in only 4% of non-smokers vs. 50% of smokers
- Goldman-Cecil Medicine
3.2 Occupational Exposure
- Polycyclic aromatic hydrocarbons: 2-naphthylamine, 4-aminobiphenyl, benzidine, benzene
- Arylamines: metabolically activated to electrophilic compounds by N-hydroxylation via cytochrome P-450 IA2; detoxified by N-acetylation
- Individuals with fast oxidizer + slow acetylator phenotype are at highest risk
- High-risk occupations:
- Dye, rubber, leather manufacturing workers
- Aluminum workers, dry cleaners
- Pesticide applicators, painters, hairdressers, plumbers, tanners
3.3 Chronic Inflammation
- Schistosoma haematobium infection - enhances N-nitroso compound formation; associated primarily with squamous cell carcinoma in endemic areas
- Indwelling catheters, bladder stones, recurrent UTIs - associated with squamous cell carcinoma
- Goldman-Cecil Medicine; Bailey & Love (28e)
3.4 Drugs
- Cyclophosphamide - increases risk 9-fold with chronic use (via acrolein metabolite)
- Phenacetin - associated with renal pelvis and ureteral tumors
3.5 Other Factors
- Pelvic radiotherapy - increased risk
- Arsenic in drinking water
- Genetic susceptibility - GWAS have identified 11+ replicated susceptibility loci including: 1p13.3 (GSTM1), 3q28 (TP63), 4p16.3 (FGFR3), 5p15.33 (hTERT), 8p22 (NAT2), 8q24.21 (MYC), 8q24.3 (PSCA), 19q12 (CCNE1)
- About 15% of patients have germline variants in DNA-damage repair genes (BRCA2, BRCA1, MSH2, CHEK2, ERCC3, NBN, RAD50)
- Campbell-Walsh-Wein Urology; Goldman-Cecil Medicine
4. Pathology and Histological Types
| Histologic Type | Frequency |
|---|---|
| Transitional cell (urothelial) carcinoma | >90% |
| Squamous cell carcinoma | 1-7% |
| Adenocarcinoma | 2% |
| Small cell carcinoma | ~1% |
| Melanoma, lymphoma, sarcoma, pheochromocytoma | <1% |
| Metastatic (colorectal, prostate, kidney, ovary) | <1% |
Bailey & Love (28e); Goldman-Cecil Medicine
4.1 Urothelial (Transitional Cell) Carcinoma
The vast majority. Can show divergent differentiation into squamous, glandular, or neuroendocrine elements.
4.2 Squamous Cell Carcinoma
Occurs secondary to chronic inflammation (indwelling catheter, stones, schistosomiasis, chronic UTI leading to keratinizing squamous metaplasia).
4.3 Adenocarcinoma
Usually originates in the urachus (dome of the bladder) or in those with bowel in the urinary tract (augmentation enterocystoplasty, bladder exstrophy repair).
4.4 Histologic Variants of Urothelial Carcinoma
These variants generally signify aggressive tumours with poorer prognosis than pure urothelial carcinoma:
Micropapillary variant (0.7-2.2% of urothelial tumors)
- Strong male predominance (male:female ratio up to 37:1)
-
50% are stage T3 or T4 at diagnosis
- 5-year and 10-year OS: 51% and 24%
- Progression from NMIBC to MIBC: 70%
- Histologically: small tight clusters or thin papillae with prominent retraction artifact
- BCG therapy is ineffective; early cystectomy is recommended
- Characterized by ERBB2 amplification; evolves through luminal pathway
Other variants: Sarcomatoid, plasmacytoid, nested variant, glandular, squamous
Campbell-Walsh-Wein Urology; Bailey & Love (28e)
5. Molecular Pathobiology
Bladder cancer has a very high somatic mutation rate (7.7 per megabase), exceeded only by lung cancer and melanoma. - Goldman-Cecil Medicine
5.1 Key Molecular Alterations
- EGFR: highly expressed in ~80% of bladder cancers
- HER2/Neu: expressed in ~50-70%; higher expression = more aggressive phenotype
- TP53: mutated in 49% of tumors
- RB1: mutated in 13% of tumors
- Epigenetic modifying genes (MLL2, ARID1A, KDM6A, EP300): ~75% have at least one inactivating mutation
- FGFR, ERBB2, MDM2, EGFR amplifications: minority of tumors; represent therapeutic targets
5.2 Molecular Subtypes (from genome-wide expression studies)
- Luminal phenotype: high levels of FGFR3, GATA3, KRT20, PPARG mutations
- Basal phenotype: squamous differentiation, expression of CK5, CK6, CK14, low FOXA1 and GATA3
5.3 GWAS Pathway Analysis
Susceptibility variants belong to three fundamental cellular processes: metabolic detoxification, mitosis, and chromatin-mediated vesicles. - Campbell-Walsh-Wein Urology
6. Staging
Approximately 70% of tumours are NMIBC at presentation; 30% are MIBC or metastatic. - Bailey & Love (28e)
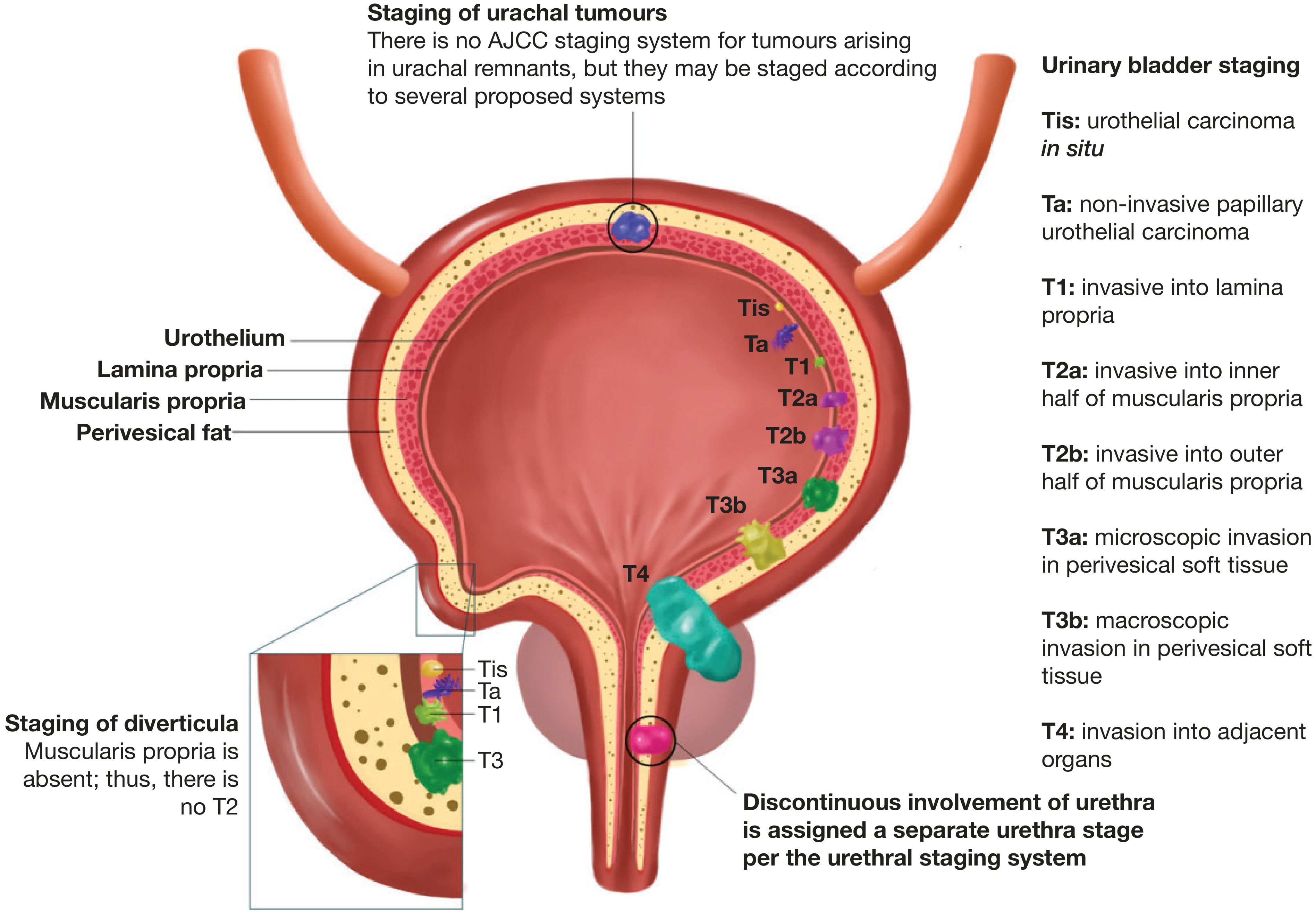
Figure: TNM Staging of Primary Tumour in Bladder Cancer. (Bailey & Love, 28e / Reproduced from Magers et al. Histopathology 2019)
TNM T-Stage Classification
| Stage | Description |
|---|---|
| Tis | Carcinoma in situ (flat, high-grade, non-invasive) |
| Ta | Non-invasive papillary urothelial carcinoma (confined to urothelium) |
| T1 | Invasion into lamina propria (submucosa) |
| T2a | Invasion into inner half of muscularis propria |
| T2b | Invasion into outer half of muscularis propria |
| T3a | Microscopic invasion into perivesical soft tissue |
| T3b | Macroscopic invasion into perivesical soft tissue |
| T4 | Invasion into adjacent organs (prostate, uterus, vagina, pelvic/abdominal wall) |
Note: In diverticula, muscularis propria is absent, so there is no T2 stage.
Grading
- G1: Well differentiated
- G2: Moderately differentiated
- G3: Poorly differentiated
Bailey & Love (28e)
7. Clinical Manifestations
- Painless haematuria - the cardinal symptom, present in 80-90% of bladder cancers
- Storage LUTS - frequency, urgency, dysuria, nocturia (irritative symptoms or reduced bladder capacity)
- Recurrent UTI
- Flank pain - if ureteral orifice obstruction with hydronephrosis
- Lower abdominal pain - from bladder mass
- Pelvic/perineal pain - tumors invading the prostate or pelvis
- Weight loss, anorexia, fatigue - advanced/metastatic disease
- Bone pain, lower limb oedema - metastatic spread
Physical examination is frequently unremarkable in early disease as most patients have organ-confined tumors. - Goldman-Cecil Medicine; Bailey & Love (28e)
8. Diagnosis and Investigation
8.1 Urine Studies
- Urine culture - to exclude infection
- Urinary cytology - identifies malignant cells; high specificity for high-grade tumors
- Urinary biomarkers - panels of epigenetic markers under study; none has surpassed accuracy of cystoscopy for routine use
8.2 Imaging
- CT urography (CTU) - gold standard for upper tract evaluation; detects hydronephrosis and nodal metastases
- MRI bladder - useful for staging the primary tumour, particularly for assessing depth of invasion
- CT chest - complete staging once bladder cancer confirmed
- Important: Imaging should be done before TURBT as post-TURBT oedema can simulate T3 disease on imaging (false-positive overstaging)
8.3 Cystourethroscopy (Key Investigation)
- Flexible cystourethroscopy under local anaesthetic is the mainstay of diagnosis
- Should always be performed in patients with haematuria
- Inspection details: size, number, location, growth pattern (papillary vs. solid) of all lesions
- Blue-light (photodynamic) cystoscopy: hexaminolevulinate (HAL) instilled intravesically; cancer cells accumulate porphyrins and fluoresce pink/red - improves detection of flat lesions (CIS)
- Narrow-band imaging (NBI): enhances vascular contrast - aids detection of flat lesions
8.4 Transurethral Resection of Bladder Tumour (TURBT) - Diagnostic and Therapeutic
- All visible disease undergoes TURBT to determine histologic subtype and depth of invasion
- Muscle must be identified in the pathologic specimen - critical for staging
- Biopsies from areas of erythema to assess for CIS
- Urethra inspected during withdrawal; biopsies taken if clinically indicated
- Patients with positive cytology but no visible tumor in bladder should undergo upper tract evaluation and urethral biopsies
Goldman-Cecil Medicine; Bailey & Love (28e)
9. Management of Non-Muscle-Invasive Bladder Cancer (NMIBC)
Stages: Tis, Ta, T1. Affects ~70% at presentation. Aim: prevent recurrences and progression.
9.1 Risk Stratification (EAU Guidelines)
| Risk Group | Characteristics |
|---|---|
| Low | Single, low-grade Ta, <3 cm, no CIS |
| Intermediate | Multifocal/recurrent low-grade Ta |
| High | T1 high-grade, CIS, multifocal/large high-grade Ta |
9.2 Initial TURBT
All NMIBC is managed with TURBT as the primary treatment.
9.3 Intravesical Mitomycin C (MMC)
- For low- and intermediate-risk tumors
- Single immediate post-operative instillation of MMC recommended within hours of TURBT to destroy circulating tumor cells and implantation
- A 6-week course for intermediate-risk tumors reduces recurrence risk
- Bailey & Love (28e)
9.4 Repeat TURBT
- Mandatory for high-grade or T1 tumors, performed 2-6 weeks after initial TURBT
- Purpose: identify residual tumor, confirm staging
- Upstaging to MIBC found in up to 40% of cases - Bailey & Love (28e)
9.5 Intravesical BCG (Bacillus Calmette-Guérin)
- For high-risk tumors (T1 HG, CIS, multifocal HG Ta)
- Reduces risk of progression to MIBC
- Protocol: 6 weekly instillations (induction), then 3-weekly maintenance every 6 months for 3 years
- Side effects: transient fever, dysuria, BCG sepsis (rare), BCG cystitis (may necessitate cystectomy)
- Bailey & Love (28e)
10. Management of Muscle-Invasive Bladder Cancer (MIBC)
Stages T2-T4. Two primary radical treatment options: radical cystectomy or chemoradiotherapy. 5-year survival with either modality: approximately 60%.
10.1 Neoadjuvant Chemotherapy
- Cisplatin-based chemotherapy given before radical cystectomy
- Improves survival by 5-7% - Bailey & Love (28e)
- Standard regimen: GC (gemcitabine + cisplatin) or MVAC (methotrexate, vinblastine, doxorubicin, cisplatin)
10.2 Radical Cystectomy
The primary surgical radical treatment. Preferred for patients with:
- Poor bladder function
- Significant haematuria
- Upper tract obstruction
- Widespread CIS
- Factors precluding radiotherapy (bilateral hip replacements, inflammatory bowel disease)
Procedure:
- Removal of bladder + pelvic lymphadenectomy (standard)
- In males: removal of prostate, seminal vesicles
- In females: uterus, ovaries, anterior vaginal wall sometimes included
Perioperative morbidity: up to 50% - major surgery requiring thorough anaesthetic assessment.
Sexual function: Male patients should be counselled about erectile dysfunction and anejaculation; nerve-sparing dissection is possible in some.
10.3 Urinary Diversion
After cystectomy, alternative drainage is essential:
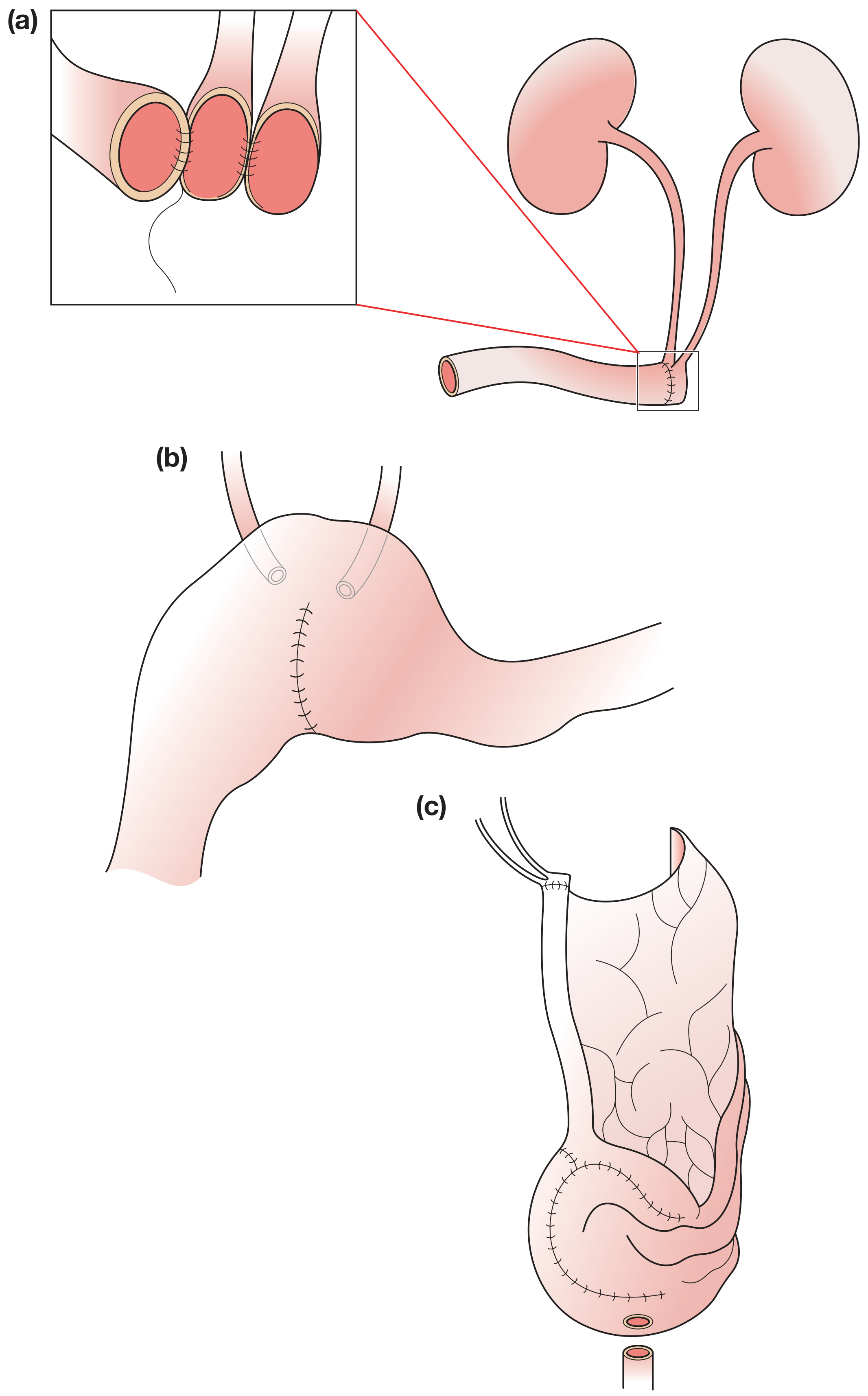
Figure: Techniques of urinary diversion. (a) Ileal conduit - ureters spatulated and anastomosed to ileum; (b) Ureterosigmoidostomy; (c) Ileal neobladder with antireflux long afferent limb. (Bailey & Love 28e)
| Type | Description | Notes |
|---|---|---|
| Ileal conduit | Ureters joined to a loop of ileum brought out as urostomy | Standard; simplest |
| Orthotopic neobladder | Ileal reservoir anastomosed to urethra | Voiding per urethra; nerve preservation needed |
| Heterotopic continent pouch | Ileal reservoir with continent abdominal stoma (e.g. appendicovesicostomy) | Patient self-catheterizes |
| Ureterosigmoidostomy | Ureters implanted into sigmoid colon | Historical; risk of metabolic complications |
Complications of continent pouches:
- Ureteroileal leak or stricture
- Urinary leak from pouch
- Stone formation, UTIs
- Metabolic complications: hyperchloraemic metabolic acidosis
- Adenocarcinoma (5%, rare)
- Stenosis and incontinence (appendicovesicostomy); up to 50% require revision surgery over 5 years
Bailey & Love (28e)
10.4 Radical Radiotherapy
- Option for very elderly or unfit patients unsuitable for radical cystectomy
- Dose: 66 Gy in 30 fractions over 6 weeks
- Long-term urinary and bowel side effects can impair quality of life
- Risk of secondary malignancy and fistula
10.5 Bladder-Preservation Trimodality Therapy
- Radical TURBT + neoadjuvant chemotherapy + chemoradiotherapy
- Being studied for very localised MIBC
- Remains an option only for a very select group - Bailey & Love (28e)
11. Management of Metastatic Bladder Cancer
11.1 First-line Chemotherapy
- GC (gemcitabine + cisplatin) - equivalent efficacy to MVAC with less toxicity; current standard
- MVAC (methotrexate, vinblastine, adriamycin, cisplatin) - older regimen; high-dose MVAC with growth factors also used
- A subset of patients may achieve long-term cure
11.2 Immunotherapy (Checkpoint Inhibitors)
- Antibodies targeting the PD-L1/PD-1 pathway showing promising results in neoadjuvant, adjuvant, and metastatic settings
- Approved agents include pembrolizumab (anti-PD-1), atezolizumab (anti-PD-L1), avelumab, nivolumab, durvalumab
- Bailey & Love (28e); Goldman-Cecil Medicine
11.3 Targeted Therapies
- FGFR inhibitors (e.g., erdafitinib) for FGFR2/FGFR3 mutations
- ERBB2 (HER2)-targeted therapies
- Antibody-drug conjugates (ADCs): enfortumab vedotin (anti-Nectin-4), sacituzumab govitecan - represent major advances in the field
11.4 Upper Tract Urothelial Carcinoma (UTUC)
- Low-grade: endoscopic treatment
- High-grade: nephroureterectomy (ureter also removed due to risk of multifocal disease)
- Adjuvant systemic chemotherapy (cisplatin + gemcitabine or carboplatin + gemcitabine) for high-risk pathologic features
- Goldman-Cecil Medicine
12. Prognosis
| Stage/Grade | 5-year Survival |
|---|---|
| Low-grade Ta | ~99% |
| T1 (NMIBC) | Variable; high risk of recurrence (~70%) and progression |
| T2 (MIBC) | ~60% with radical treatment |
| T3 | ~30-40% |
| T4/Metastatic | ~15% |
Recurrences after therapy are frequent in NMIBC (75-85% of presentations are of superficial type), requiring diligent and lifelong surveillance cystoscopy. - Campbell-Walsh-Wein Urology
13. Surveillance
- Cystoscopy every 3 months for the first 2 years, then 6-monthly, then annually for NMIBC
- Upper tract imaging periodically
- Urinary cytology at each visit
14. Recent Evidence (2024-2026)
Recent systematic reviews highlight evolving approaches:
-
Novel intravesical therapies for NMIBC are expanding beyond BCG, including TAR-200 (intravesical gemcitabine-releasing device), cretostimogene, nadofaragene firadenovec - [Ghodoussipour et al., Eur Urol 2025, PMID 40253283]
-
Mitomycin C in intermediate-risk NMIBC: A 2024 meta-analysis confirms a role for extended MMC instillation in reducing recurrence - [Scilipoti et al., Eur Urol Oncol 2024, PMID 38902138]
-
Nectin-4 (target of enfortumab vedotin) is consistently expressed in urothelial and other genitourinary malignancies - [Crupi et al., JCO Precis Oncol 2024, PMID 39626158]
Summary Table: Key Points
| Feature | Details |
|---|---|
| Most common type | Urothelial (transitional cell) carcinoma >90% |
| Cardinal symptom | Painless haematuria (80-90%) |
| Leading risk factor | Cigarette smoking (2-4x risk) |
| Occupational risk | Aromatic amines (dye, rubber, leather workers) |
| Diagnosis gold standard | Cystoscopy + TURBT |
| Staging tool | CT urography |
| NMIBC treatment | TURBT ± intravesical MMC or BCG |
| MIBC treatment | Neoadjuvant chemo + radical cystectomy |
| Metastatic treatment | GC chemotherapy, checkpoint inhibitors, ADCs |
| Mutation rate | 7.7/Mb (3rd highest of all cancers) |
| Recurrence rate NMIBC | High; lifelong surveillance required |
References:
- Goldman-Cecil Medicine (International Edition, 2-Volume Set), Chapter 100
- Campbell-Walsh-Wein Urology (3-Volume Set), Chapters 33, 75, 84
- Bailey & Love's Short Practice of Surgery (28th Edition), Chapter 83
- Gray's Anatomy for Students
- Scilipoti et al. [Eur Urol Oncol 2024, PMID 38902138]
- Ghodoussipour et al. [Eur Urol 2025, PMID 40253283]
- Crupi et al. [JCO Precis Oncol 2024, PMID 39626158]
This is a shared conversation. Sign in to Orris to start your own chat.