Explain me foetal circulation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here it is:
Foetal Circulation
The foetal cardiovascular system is designed around a fundamental problem: the lungs are non-functional, so gas exchange happens at the placenta. Blood must be routed to the placenta for oxygenation, and the best-oxygenated blood must be directed to the most oxygen-demanding organs (heart and brain). Three shunts make this possible.
The Diagram
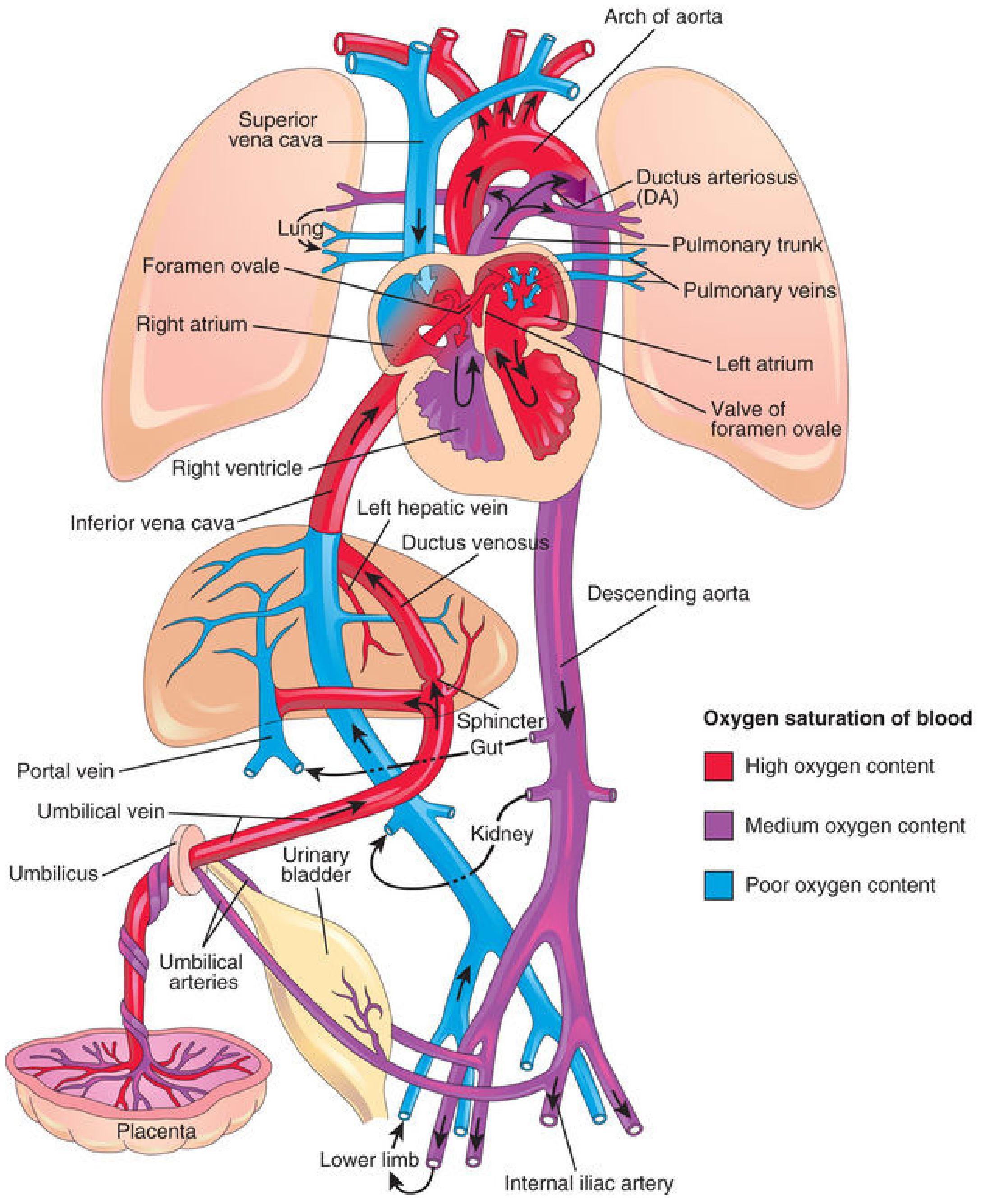
Fetal circulation showing oxygen saturation: red = high O₂, purple = medium O₂, blue = low O₂. Note the three bypass shunts: ductus venosus, foramen ovale, and ductus arteriosus.
Step-by-Step Blood Flow
1. Placenta → Umbilical Vein
- Oxygenated, nutrient-rich blood leaves the placenta via the umbilical vein (~80% O₂ saturation - the highest in the fetal circulation).
- The umbilical vein travels through the umbilical cord and enters the fetal abdomen at the umbilicus.
2. Liver Level - First Shunt: Ductus Venosus
- On reaching the liver, the blood splits:
- ~50% bypasses the liver directly via the ductus venosus → enters the inferior vena cava (IVC).
- ~50% enters the portal system → perfuses hepatic sinusoids → drains via hepatic veins into the IVC.
- A physiologic sphincter near the ductus venosus regulates this split - during uterine contractions (high umbilical flow), the sphincter constricts to prevent cardiac overload.
- In the IVC, this blood mixes with deoxygenated blood from the lower limbs, pelvis, and kidneys - first mixing point (Point II per Langman's).
3. Right Atrium - Second Shunt: Foramen Ovale
- Blood from the IVC enters the right atrium. Here it is guided by the crista dividens (inferior edge of the septum secundum):
- Most of the relatively well-oxygenated IVC blood is directed through the foramen ovale directly into the left atrium, bypassing the lungs entirely.
- A small amount is blocked by the crista dividens and stays in the right atrium, where it mixes with poorly oxygenated blood from the SVC (returning from the head and upper limbs).
4. Left Atrium → Left Ventricle → Ascending Aorta
- Blood from the foramen ovale enters the left atrium, mixes with a small volume of blood from the pulmonary veins (the fetal lungs extract oxygen rather than add it).
- From the left ventricle it enters the ascending aorta.
- The coronary arteries and carotid arteries branch first from the ascending aorta - so the heart and brain receive the best-oxygenated blood available.
5. Right Ventricle - Third Shunt: Ductus Arteriosus
- The small amount of blood remaining in the right atrium (from the SVC + some IVC blood) passes into the right ventricle → into the pulmonary trunk.
- In fetal life, pulmonary vascular resistance is high (hypoxic pulmonary vasoconstriction, fluid-filled lungs). Only ~10% of right ventricular output actually goes to the lungs.
- The rest (>85%) passes through the ductus arteriosus (connecting the pulmonary trunk to the descending aorta), bypassing the lungs.
6. Descending Aorta → Umbilical Arteries → Back to Placenta
- Blood in the descending aorta (now lower O₂ saturation ~58%) supplies the abdominal organs and lower limbs.
- It then flows into the internal iliac arteries → umbilical arteries → back through the umbilical cord → to the placenta for re-oxygenation.
The Three Key Shunts - Summary
| Shunt | Connects | Purpose |
|---|---|---|
| Ductus venosus | Umbilical vein → IVC | Bypasses liver |
| Foramen ovale | Right atrium → Left atrium | Bypasses lungs |
| Ductus arteriosus | Pulmonary trunk → Descending aorta | Bypasses lungs |
Where Mixing Occurs (Langman's 5 Points)
Because pure oxygenated and deoxygenated streams keep merging, foetal blood is never perfectly oxygenated:
- Liver - umbilical vein blood mixes with portal blood
- IVC - mixes with deoxygenated blood from lower limbs
- Right atrium - mixes with SVC blood from head/arms
- Left atrium - mixes with small amount of pulmonary venous blood
- Descending aorta - at the entry of the ductus arteriosus
Changes at Birth (Neonatal Transition)
At birth, two major events trigger a dramatic circulatory reorganisation:
1. Clamping of the Umbilical Cord
- Removes the low-resistance placental circuit → systemic vascular resistance rises sharply.
- Right atrial pressure falls (placental return stops).
2. First Breath - Lung Expansion
- Lungs fill with air → pulmonary vascular resistance drops dramatically (due to mechanical expansion and rise in pO₂).
- Pulmonary blood flow increases markedly → more blood returns to the left atrium → left atrial pressure rises.
Closure of the Shunts
| Shunt | Functional closure | Anatomical closure | Adult remnant |
|---|---|---|---|
| Foramen ovale | At birth (LA pressure > RA) - septum primum presses against septum secundum | Weeks to months | Fossa ovalis |
| Ductus arteriosus | Hours after birth (bradykinin + rise in pO₂ → smooth muscle contraction) | 1-3 months | Ligamentum arteriosum |
| Ductus venosus | Within hours of cord clamping | Few weeks | Ligamentum venosum |
| Umbilical vein | At cord clamping | Few weeks | Ligamentum teres hepatis |
| Umbilical arteries | At cord clamping | Few weeks | Medial umbilical ligaments (proximal parts become superior vesical arteries) |
Neonatal Circulation
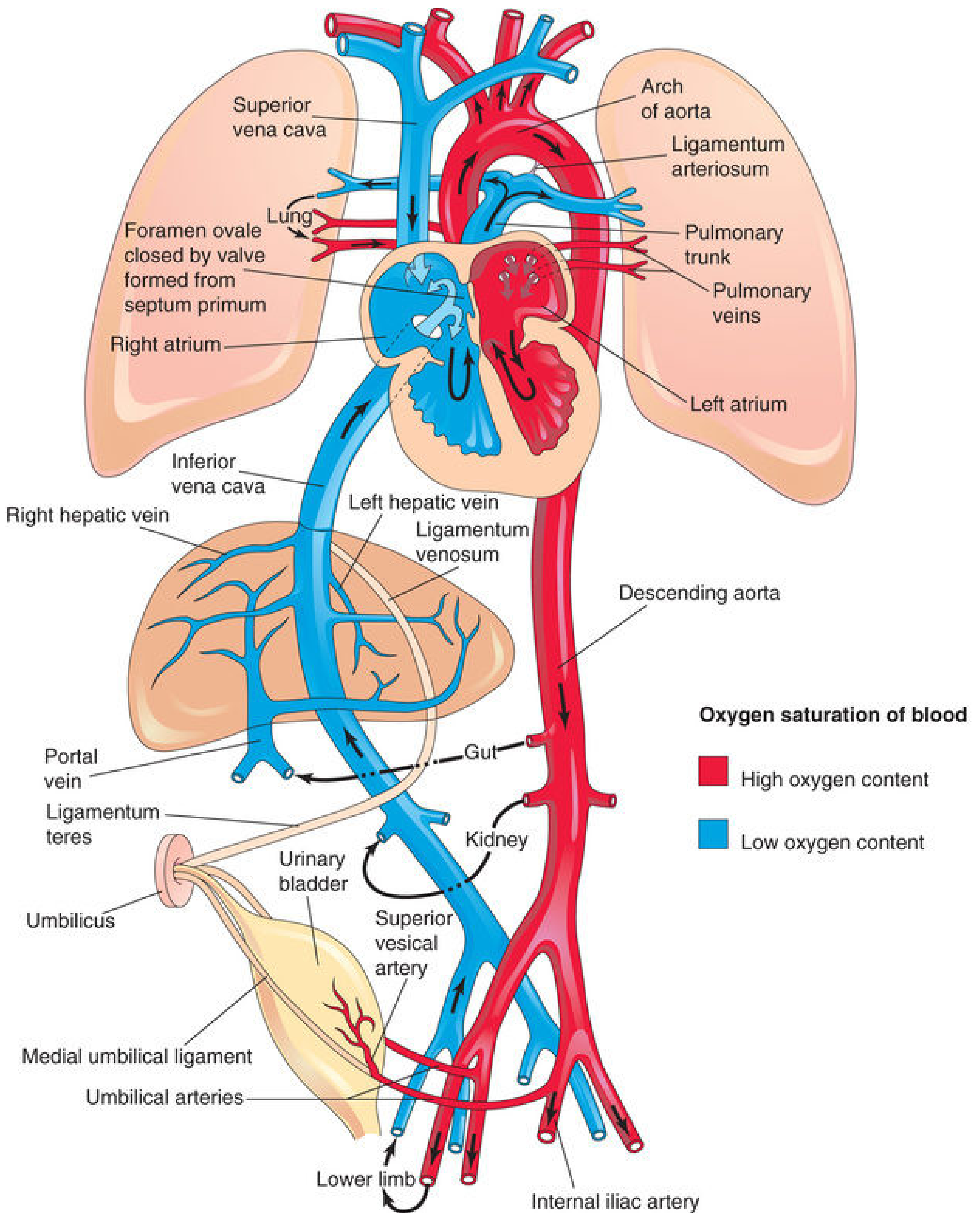
After birth, the three shunts close. Pulmonary and systemic circulations become fully separated. All blood now flows through the lungs for oxygenation.
Why This Design Makes Sense
- The brain and heart need the most oxygen - they receive the best blood (via ascending aorta).
- The lower body and placenta receive mixed/deoxygenated blood - acceptable, since the placenta will re-oxygenate it.
- The liver receives some well-oxygenated blood (for metabolic needs) but also has ~50% bypassed (via ductus venosus) to avoid overloading the heart.
- The lungs are essentially bypassed entirely - no point perfusing them when they are fluid-filled and not exchanging gas.
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.), pp. 869-873 | Langman's Medical Embryology, pp. 236-237 | Ganong's Review of Medical Physiology, 26e, p. 614
And changes occurring at birth
Reading File
Reading File
Finding Sources
I have all the detail needed from both Moore and Langman's. Here is the full dedicated explanation:
Circulatory Changes at Birth
At birth, two simultaneous events restructure the entire circulation: the placenta is cut off and the lungs expand. These two events oppose each other in a perfectly orchestrated way to close all three foetal shunts.
The Two Triggering Events
1. Cessation of Placental Blood Flow
- Cord clamping removes the large, low-resistance placental vascular bed.
- Systemic vascular resistance rises sharply.
- Blood flow returning via the IVC drops → right atrial pressure falls.
2. Lung Expansion (First Breath)
- Aeration of the alveoli causes:
- Dramatic drop in pulmonary vascular resistance (from mechanical stretching of pulmonary arteries + rising O₂ tension causing vasodilation).
- Marked increase in pulmonary blood flow - the pulmonary arteries, which were thick-walled and vasoconstricted in fetal life, progressively thin out.
- More blood now flows through the lungs → more returns to the left atrium → left atrial pressure rises.
The result: left atrial pressure now exceeds right atrial pressure - the reverse of the foetal situation. This pressure reversal is the engine that closes all three shunts.
Closure of Each Shunt
Foramen Ovale
| Foetal | Neonatal | |
|---|---|---|
| RA pressure | Higher than LA | Lower than LA |
| Shunt direction | Right → Left | Reversed pressure closes it |
- The rise in LA pressure presses the septum primum against the septum secundum, like a flap valve snapping shut.
- Functional closure: at birth (within the first breath).
- Anatomical closure: fusion of the two septa over weeks to months (~1 year).
- In 20% of adults, complete anatomical fusion never occurs - this is called a probe patent foramen ovale (PFO), which is usually clinically silent but can be a route for paradoxical embolism.
- In the first few days, crying can momentarily raise RA pressure and cause a brief right-to-left shunt, producing transient cyanosis in the newborn - this is normal.
- Adult remnant: Fossa ovalis
Ductus Arteriosus
| Foetal | Neonatal | |
|---|---|---|
| Pulmonary resistance | High | Falls after first breath |
| Shunt direction | Pulmonary trunk → Descending aorta | Reverses: Aorta → Pulmonary trunk, then closes |
- As pulmonary resistance drops below systemic resistance, blood flow through the ductus reverses direction (now aorta → pulmonary trunk) - this is why left-to-right shunting occurs before it closes.
- Mechanism of closure: The lungs release bradykinin during initial inflation. Bradykinin, combined with the rise in arterial pO₂, causes smooth muscle contraction in the ductus wall.
- Functional closure: within hours of birth.
- At 24 hours: 20% of ducts functionally closed.
- At 48 hours: 82% closed.
- By 96 hours: 100% in full-term neonates.
- Anatomical closure (fibrous obliteration): 1-3 months.
- Premature neonates have immature smooth muscle and are less sensitive to O₂/bradykinin - hence patent ductus arteriosus (PDA) is common in prematurity, treated with indomethacin (prostaglandin inhibitor) or surgical ligation.
- Adult remnant: Ligamentum arteriosum
Ductus Venosus
- The ductus venosus sphincter constricts within hours of cord clamping.
- All portal blood must now pass through the hepatic sinusoids - the liver is no longer partially bypassed.
- Functional closure: within hours of birth.
- Anatomical closure: few weeks.
- Adult remnant: Ligamentum venosum (visible on the visceral surface of the liver, between the left lobe and caudate lobe).
Umbilical Vessels
Umbilical Arteries:
- Close within a few minutes of birth by smooth muscle contraction - triggered by thermal stimuli (cold), mechanical stimuli (handling), and the rise in arterial pO₂.
- Anatomical obliteration by fibrous proliferation: 2-3 months.
- Adult remnants:
- Distal portions → Medial umbilical ligaments (visible on the inner anterior abdominal wall).
- Proximal portions remain patent as the Superior vesical arteries (supplying the bladder).
Umbilical Vein:
- Closes shortly after the umbilical arteries. Blood from the placenta can still enter the newborn for a short time after birth if the cord is not immediately clamped.
- Adult remnant: Ligamentum teres hepatis (round ligament of the liver), running in the free edge of the falciform ligament.
Summary Table - Foetal Structures and Their Adult Derivatives
| Foetal Structure | Closes When | Mechanism | Adult Remnant |
|---|---|---|---|
| Foramen ovale | At birth (functional) | LA > RA pressure | Fossa ovalis |
| Ductus arteriosus | Hours after birth | Bradykinin + ↑pO₂ | Ligamentum arteriosum |
| Ductus venosus | Hours after cord clamping | Sphincter contraction | Ligamentum venosum |
| Umbilical vein | Minutes after birth | Fibrosis | Ligamentum teres hepatis |
| Umbilical arteries (distal) | Minutes after birth | Smooth muscle spasm + fibrosis | Medial umbilical ligaments |
| Umbilical arteries (proximal) | Remain patent | - | Superior vesical arteries |
Ventricular Wall Changes
- In the fetus, the right ventricular wall is thicker than the left - because the RV has been pumping against high pulmonary resistance.
- After birth, the LV now drives the systemic circulation (high resistance) while the RV pumps against the now-low pulmonary resistance.
- By end of the first month: the LV wall becomes thicker than the RV wall.
- The RV wall gradually thins due to its reduced workload.
Clinical Relevance - When Shunts Fail to Close
| Failed closure | Condition | Consequence |
|---|---|---|
| Foramen ovale | Patent foramen ovale (PFO) | Usually silent; risk of paradoxical embolism/stroke |
| Ductus arteriosus | PDA | Left-to-right shunt; pulmonary overcirculation; if large, risk of Eisenmenger syndrome |
| Ductus venosus | Rare | Porto-systemic shunting, hepatic encephalopathy |
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.), pp. 872-876 | Langman's Medical Embryology, pp. 237-238
1. First breath of child
1. First breath of child, 2.flow of blood to lungs, 3.closure of foramen ovale, 4.reversal of blood flow in ductus arteriosus, 5.closure of ductus venosus, 6.closure of ductus arteriosus
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent - I have very rich, detailed content from three authoritative sources. Here is the complete, sequential explanation:
Changes at Birth - A Sequential Physiological Analysis
The transition from foetal to neonatal circulation must be largely completed within minutes of birth - failure means death or permanent neurological damage. The entire sequence is triggered by one event: the first breath.
1. The First Breath
What is in the lungs before birth?
At term, the foetal lungs contain approximately 90 mL of plasma ultrafiltrate (lung liquid), not air. The lungs are fluid-filled, airways are collapsed, and pulmonary vascular resistance is extremely high.
The "Vaginal Squeeze"
During normal vaginal delivery, the forces of the pelvic muscles and birth canal compress the foetal thorax - this squeezes out a large portion of lung fluid. Any remaining fluid is rapidly reabsorbed by pulmonary capillaries and lymphatics. This is why:
- Babies delivered by caesarean section miss this squeeze and retain more lung fluid → Transient Tachypnoea of the Newborn (TTN) is more common.
- Preterm neonates also miss the benefit of full vaginal squeeze.
What triggers breathing?
The stimulus for the first breath is not fully understood, but key triggers include:
- Sensory stimulation: cold air, light, sound, touch, pain, cord clamping
- Mild hypoxia and acidosis from the birth process - act as chemical respiratory stimuli
- Outward recoil of the chest after delivery - the chest wall springs outward, passively drawing air in
- NOT primarily hypoxia in a normal labour (Ganong's)
The mechanics
- The first breath requires a very large negative intrathoracic pressure of -30 to -50 mmHg to overcome:
- Surface tension of fluid in the alveoli
- Resistance of airway fluid
- Elastic recoil of the lungs
- Surfactant is essential here - it reduces alveolar surface tension, prevents alveolar collapse on expiration, and stabilises lung expansion. It is produced from ~30 weeks (adequate amounts by ~34 weeks).
- Respiratory efforts normally begin within 30 seconds of birth and become sustained within 90 seconds.
Immediate result of lung expansion
- Alveolar and arterial pO₂ rises sharply
- This rising O₂ tension is the most potent stimulus for pulmonary arterial vasodilation - mediated through nitric oxide (NO) production
- Pulmonary vascular resistance (PVR) falls to less than 20% of its in utero value after just the first few breaths
2. Flow of Blood to the Lungs
Before birth
Only ~10% of right ventricular output reached the lungs - the rest was diverted via the ductus arteriosus. Pulmonary vessels were thick-walled and vasoconstricted due to:
- Hypoxia (low alveolar pO₂ causes hypoxic pulmonary vasoconstriction)
- High CO₂, low pH
- Physical compression of vessels by fluid-filled alveoli
After first breath
- Lung expansion + rising pO₂ → NO-mediated vasodilation of pulmonary arterioles
- PVR drops dramatically
- Right ventricular output now floods into the pulmonary circulation
- Pulmonary blood flow increases 4-5 fold within minutes
- Pulmonary artery walls progressively thin out (from mechanical stretching by the expanded lungs)
- More blood returns to the left atrium via the pulmonary veins → left atrial pressure rises
This shift - PVR falling below systemic vascular resistance (SVR) - is the key that drives all subsequent closures.
3. Closure of the Foramen Ovale
Foetal state
- RA pressure > LA pressure (because the IVC delivers large volumes of oxygenated umbilical blood to the right side)
- This pressure gradient holds the foramen ovale open, directing blood left-to-right (RA → LA)
At birth - two simultaneous pressure changes
| Event | Effect on pressure |
|---|---|
| Cord clamping - loss of umbilical return | RA pressure falls |
| Increased pulmonary venous return to LA | LA pressure rises |
- LA pressure now exceeds RA pressure
- The septum primum (which acts as a flap valve) is pushed against the septum secundum from the left side, mechanically sealing the foramen ovale shut
- Functional closure: at birth, with the first few breaths
- Anatomical closure: weeks to months (fusion of septa); takes up to 1 year
- In 20% of adults: complete anatomical fusion never occurs → probe patent foramen ovale (PFO) - usually silent, but risk of paradoxical embolism/cryptogenic stroke
- In the first days of life, crying briefly raises RA pressure, temporarily reopening the foramen → physiological transient cyanosis in newborns
4. Reversal of Blood Flow in the Ductus Arteriosus
Foetal direction
- Pulmonary trunk → Descending aorta (right-to-left)
- Driven because PVR > SVR, so blood took the path of least resistance away from the lungs
At birth - pressure reversal
- PVR drops dramatically (first breath)
- SVR rises (cord clamping removes low-resistance placenta)
- Now SVR > PVR → blood flow in the ductus arteriosus reverses
- New direction: Aorta → Pulmonary trunk (left-to-right)
- This left-to-right shunt persists briefly while the ductus remains open
- The right ventricle's output now flows preferentially into the pulmonary trunk rather than the aorta
This reversal phase is transient - the ductus then constricts and closes (see step 6).
5. Closure of the Ductus Venosus
Mechanism
- Cord clamping removes umbilical venous return - there is no longer high-pressure blood flowing from the placenta
- The physiologic sphincter at the ductus venosus constricts almost immediately
- All portal blood must now pass through the hepatic sinusoids - the liver loses its partial bypass
- Functional closure: within hours of cord clamping
- Anatomical closure: 1-3 weeks (fibrotic obliteration)
- Adult remnant: Ligamentum venosum (visible in the groove between the left lobe and caudate lobe of the liver)
The ductus venosus closes largely passively - it depends on umbilical flow being cut off rather than an active chemical trigger.
6. Closure of the Ductus Arteriosus
This is the most complex and pharmacologically important closure.
What keeps it open in foetal life?
Two mechanisms maintain ductal patency in utero:
- Low pO₂ of blood flowing through it (foetal blood is relatively hypoxic)
- Prostaglandins - locally produced PGE₂ and prostacyclin (PGI₂) cause smooth muscle relaxation and keep the ductus open. Hypoxia promotes their local synthesis.
What triggers closure at birth?
Primary trigger - Rise in arterial pO₂:
- When pO₂ of blood passing through the ductus reaches ~50 mmHg, smooth muscle of the ductus wall contracts
- O₂ acts both directly on smooth muscle and indirectly by:
- Stimulating release of bradykinin from the newly inflated lungs
- Suppressing local PGE₂ synthesis (O₂ inhibits cyclooxygenase activity)
Bradykinin:
- Released from the lungs during initial inflation
- Has potent contractile effects on ductal smooth muscle
- Its action is dependent on the high O₂ content of aortic blood
Prostaglandin withdrawal:
- Birth inhibits cyclooxygenase → PGE₂ and PGI₂ synthesis falls → vasodilatory tone is lost
- This is why indomethacin (COX inhibitor) closes a PDA in premature neonates
Other mediators: acetylcholine, TGF-β (involved in anatomical closure)
Timeline of closure
| Time | Status |
|---|---|
| Birth | Begins constricting; brief left-to-right shunt |
| 24 hours | 20% functionally closed |
| 48 hours | ~80% functionally closed |
| 96 hours | 100% functionally closed (full-term) |
| 1-3 months | Anatomical (fibrous) obliteration complete |
- Adult remnant: Ligamentum arteriosum (connects pulmonary trunk to aortic arch)
Why prematurity causes PDA
- Immature smooth muscle is less responsive to O₂ and bradykinin
- PGE₂ production is higher relative to ductal responsiveness
- Treatment: indomethacin or ibuprofen (COX inhibitors) - block PGE₂ → ductal constriction
- If medical treatment fails: surgical/catheter ligation
The Full Sequence as a Timeline
Birth
│
├─ Vaginal squeeze clears lung fluid
│
├─ Sensory stimuli + mild hypoxia → FIRST BREATH (within 30 sec)
│ │
│ ├─ pO₂ rises → NO production → pulmonary vasodilation
│ ├─ PVR falls to <20% of fetal value
│ │
│ ├─ PULMONARY BLOOD FLOW ↑↑↑ (4-5×)
│ │ └─ LA pressure rises
│ │
│ ├─ Cord clamping → umbilical return lost → RA pressure falls
│ │
│ ├─ LA > RA pressure → FORAMEN OVALE closes (functional)
│ │
│ ├─ PVR < SVR → DA flow REVERSES (aorta → pulmonary trunk)
│ │
│ ├─ ↑pO₂ + bradykinin (from inflated lungs) → DUCTUS ARTERIOSUS constricts
│ │ + PGE₂ synthesis falls (COX inhibited) → closes over hours-days
│ │
│ └─ Umbilical flow stops → DUCTUS VENOSUS sphincter constricts → closes
│
└─ Result: Parallel (fetal) circulation → Serial (adult) circulation
What Happens if This Transition Fails?
If the baby is hypoxic or acidotic during the transition:
- Hypoxia maintains high PVR
- PGE₂ production continues → ductus stays open
- Right-to-left shunting persists → more hypoxia → more shunting
- This vicious cycle is Persistent Pulmonary Hypertension of the Newborn (PPHN) - a life-threatening emergency
- Treatment: O₂, inhaled NO, surfactant, possibly ECMO
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.), pp. 875-876 | Langman's Medical Embryology, pp. 237-238 | Ganong's Review of Medical Physiology 26e, pp. 615-616 | Morgan & Mikhail's Clinical Anesthesiology 7e, pp. 1595-1596
Try again
Asking for Preferences
Loading Image
Loading Image
Here is the redesigned, simpler version:
Changes at Birth - Before vs After
BEFORE birth → AFTER birth
The Big Picture First
| In the Womb | At Birth |
|---|---|
| Placenta = oxygen source | Lungs = oxygen source |
| Lungs are bypassed | Lungs receive full blood flow |
| 3 shunts are open | All 3 shunts close |
| Right & left heart pump in parallel | Right & left heart pump in series |
1. 🫁 The First Breath
What's in the lungs before birth?
- ~90 mL of fluid (not air)
- Pulmonary vessels tightly squeezed shut (high resistance)
What triggers breathing?
- Cold air on skin, touch, sound, light
- Mild drop in O₂ at delivery
- The chest wall springs outward after the baby exits → passively sucks air in
- Requires a strong suction effort: -30 to -50 mmHg (much greater than normal adult breathing)
What happens when air enters the lungs?
- Alveoli expand → lung fluid is squeezed out (or reabsorbed)
- O₂ rises in the blood → pulmonary blood vessels relax and open up
- Pulmonary vascular resistance (PVR) falls to <20% of foetal levels in just a few breaths
⚠️ C-section babies miss the "vaginal squeeze" that clears lung fluid → more prone to Transient Tachypnoea of the Newborn (TTN)⚠️ Premature babies lack surfactant (produced from ~34 weeks) → alveoli collapse after each breath → Respiratory Distress Syndrome (RDS)
2. 🩸 Blood Flow to the Lungs
Before birth:
- Only ~10% of blood went to the lungs
- 90% bypassed via the ductus arteriosus
After first breath:
Lungs expand
↓
O₂ rises → Nitric Oxide released → pulmonary vessels DILATE
↓
Pulmonary resistance falls sharply
↓
Blood FLOODS the lungs (4-5× increase)
↓
More blood returns to LEFT ATRIUM via pulmonary veins
↓
LEFT ATRIAL PRESSURE RISES ← this drives the next two closures
3. ❤️ Closure of the Foramen Ovale
What it is: A flap-valve hole in the wall between the two upper chambers (atria).
Why it was open in the womb:
- Right atrium had higher pressure than left (IVC delivering lots of umbilical blood)
- Blood pushed the flap open: RA → LA
Why it closes at birth:
| Event | Pressure change |
|---|---|
| Cord clamped → umbilical flow stops | RA pressure falls |
| More blood returns from lungs | LA pressure rises |
- LA pressure now > RA pressure
- The flap (septum primum) gets pushed shut from the left side - like a door blown closed by wind
- Functional closure: minutes after birth
- Permanent fusion: weeks to months
⚠️ In 20% of people, the flap never fully fuses → Patent Foramen Ovale (PFO) - usually harmless, but can allow blood clots to cross from right to left → stroke
4. 🔄 Reversal of Blood Flow in the Ductus Arteriosus
What it is: A short vessel connecting the pulmonary artery to the aorta.
Blood flow direction:
| When | Direction | Why |
|---|---|---|
| In womb | Pulmonary artery → Aorta (R→L) | Lung resistance HIGH, easier to bypass |
| At birth | Aorta → Pulmonary artery (L→R) | Lung resistance now LOW, blood flows toward lungs |
- This reversal is temporary - it lasts only while the ductus is still open
- It actually helps send more blood to the lungs during the transition
- Then the ductus constricts and closes (step 6)
5. 🏥 Closure of the Ductus Venosus
What it is: A bypass channel that let blood skip the liver in the womb.
Why it closes:
- Cord is clamped → high-pressure umbilical blood flow stops
- No flow = no reason to stay open
- The sphincter at its entrance constricts
- All blood from the gut must now pass through the liver
| Timing | |
|---|---|
| Functional closure | Hours after cord clamping |
| Anatomical closure | 1-3 weeks |
| Adult remnant | Ligamentum venosum (scar tissue on the liver) |
6. 🔒 Closure of the Ductus Arteriosus
This is the most complex one - it involves active chemical signals.
What kept it OPEN in the womb?
- Low O₂ in foetal blood
- Prostaglandins (PGE₂, PGI₂) - these relax the duct wall and keep it open
What CLOSES it at birth?
First breath
↓
O₂ in blood RISES
↓
Two effects:
① O₂ directly contracts the duct wall muscle
② O₂ triggers release of BRADYKININ from lungs
→ bradykinin = powerful muscle contractor
↓
Also: Prostaglandin production FALLS
(O₂ inhibits the enzymes that make PGE₂)
↓
Ductus arteriosus CONSTRICTS and closes
Timeline:
| Time after birth | Status |
|---|---|
| First few hours | Constricting; small left-to-right shunt still present |
| 24 hours | 20% fully closed |
| 48 hours | 80% closed |
| 96 hours | 100% closed (full-term) |
| 1-3 months | Permanent fibrous scar forms |
Adult remnant: Ligamentum arteriosum
⚠️ Premature babies: Duct muscle is immature → doesn't respond to O₂/bradykinin → Patent Ductus Arteriosus (PDA)
- Hear a continuous "machinery murmur"
- Treatment: Indomethacin (blocks prostaglandin → duct constricts) or surgical ligation
All 6 Events as One Flowchart
BIRTH
│
▼
① FIRST BREATH
- Sensory triggers + mild hypoxia
- -30 to -50 mmHg effort
- Alveoli open, O₂ rises, NO released
│
▼
② BLOOD FLOWS TO LUNGS
- PVR falls <20% of foetal value
- Pulmonary blood flow ↑↑↑
- LA pressure rises
│
├──────────────────────────────┐
▼ ▼
③ FORAMEN OVALE CLOSES Cord clamped → RA pressure falls
(LA > RA pressure; same pressure reversal seals the flap
septum primum flaps shut)
│
▼
④ DUCTUS ARTERIOSUS FLOW REVERSES
(now Aorta → Pulmonary artery, briefly)
│
▼
⑤ DUCTUS VENOSUS CLOSES
(no more umbilical flow, sphincter constricts)
│
▼
⑥ DUCTUS ARTERIOSUS CLOSES
(↑O₂ + bradykinin contract the wall;
PGE₂ falls; complete in 96 hours)
│
▼
ADULT SERIAL CIRCULATION ESTABLISHED
Quick Reference - Adult Remnants
| Foetal Structure | Closes When | Becomes |
|---|---|---|
| Foramen ovale | Minutes | Fossa ovalis |
| Ductus arteriosus | 96 hours | Ligamentum arteriosum |
| Ductus venosus | Hours | Ligamentum venosum |
| Umbilical vein | Minutes | Ligamentum teres hepatis |
| Umbilical arteries (distal) | Minutes | Medial umbilical ligaments |
| Umbilical arteries (proximal) | Stay open | Superior vesical arteries |
Sources: The Developing Human (Moore et al.) pp. 875-876 | Langman's Medical Embryology pp. 237-238 | Ganong's Physiology 26e pp. 615-616 | Morgan & Mikhail's Clinical Anaesthesiology 7e pp. 1595-1596
This is a shared conversation. Sign in to Orris to start your own chat.