Give essay answer on atelectasis of middle ear , grades presentation investigations and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
atelectasis middle ear tympanic membrane retraction
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive content from Cummings Otolaryngology plus the key images. Let me now compose the full essay answer.
Atelectasis of the Middle Ear
Definition
Middle ear atelectasis is a condition in which the tympanic membrane becomes progressively retracted into the middle ear cavity due to longstanding negative middle ear pressure, resulting from eustachian tube dysfunction. The middle ear space is partially or completely obliterated, but — crucially — the tympanic membrane remains non-adherent to the medial wall, and the mucosal lining of the middle ear is preserved. This distinguishes it from adhesive otitis media, where the tympanic membrane is fully adherent to the ossicles and promontory with loss of the mucosal surfaces.
Pathophysiology
The principal driving mechanism is eustachian tube dysfunction (ETD). The eustachian tube serves three functions: ventilation, mucociliary drainage, and protection. Intermittent opening of the tube allows gas exchange between the nasopharynx and middle ear, equalising atmospheric pressure. The gas composition of the middle ear normally resembles that of venous blood; bilateral diffusion between the middle ear cavity and the blood further contributes to relative negative pressure in the presence of inadequate ventilation.
When the tube fails to open adequately:
- Negative middle ear pressure develops
- The tympanic membrane is progressively drawn medially
- Repeated bouts of acute otitis media (AOM) lead to collagen destruction and thinning of the fibrous layer of the tympanic membrane (demonstrated by Sadé and Berco), reducing its structural resistance to inward retraction
- The tympanic membrane drapes progressively over the ossicles and onto the promontory
Predisposing factors include recurrent AOM, chronic otitis media with effusion (OME), cleft palate, Down's syndrome, nasopharyngeal pathology, post-irradiation sequelae, and paranasal sinus disease in adults. Reflux of gastric contents (with detection of Helicobacter pylori in middle ear effusions) has been implicated in OME in children. There is also hereditary predisposition — mastoid hypopneumatisation reduces the gas reservoir and worsens negative pressure dynamics.
Grading / Classification
The most widely used system is the Sadé and Berco classification (1976), later described by Sadé and Tos, which stages retraction of the tympanic membrane on a spectrum culminating in adhesive otitis media:
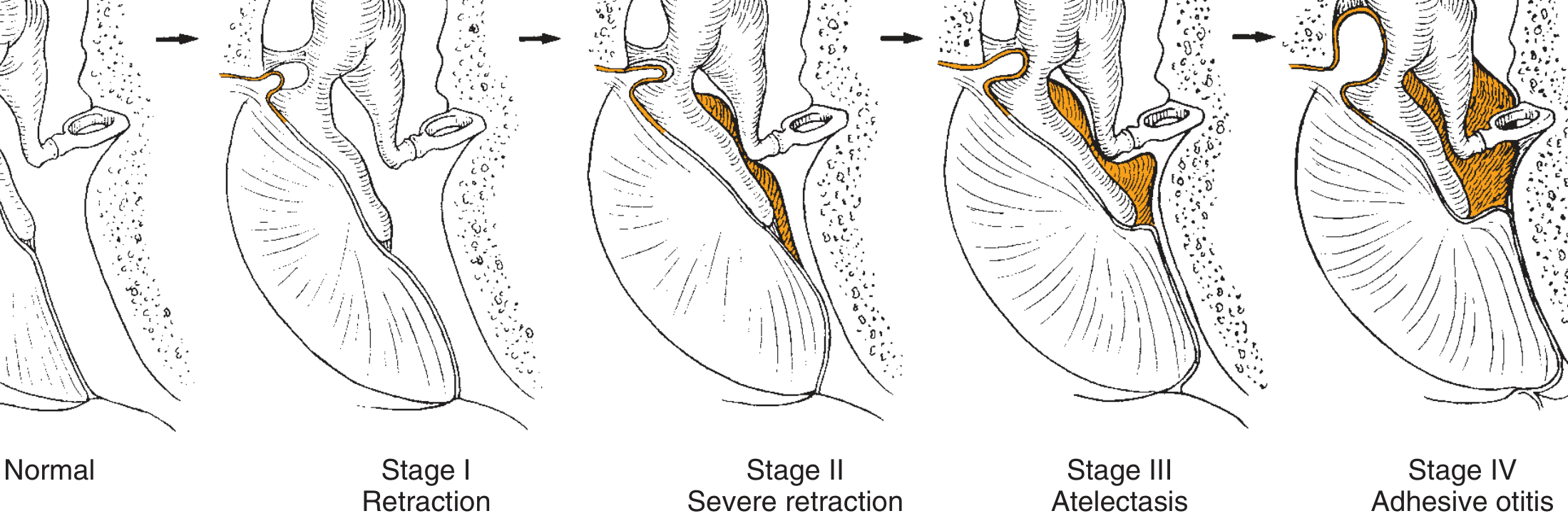
Fig. 140.3 — The four stages of middle ear atelectasis (Sadé & Berco, 1976; adapted from Cummings Otolaryngology)
| Stage | Description |
|---|---|
| Stage I | Retracted tympanic membrane — mild inward bowing, but membrane still mobile and not in contact with ossicles |
| Stage II | Severe retraction — tympanic membrane in contact with the incus (long process) but middle ear space not fully obliterated |
| Stage III | True middle ear atelectasis — tympanic membrane lies on the promontory; middle ear space partially or completely obliterated; membrane still not adherent; mucosa intact |
| Stage IV | Adhesive otitis media — total obliteration of middle ear space; tympanic membrane adherent to ossicles and promontory; mucosal surfaces lost on both medial side of TM and middle ear lining |
Additional classifications used in clinical practice:
- Deguine classification (pars tensa retraction)
- Tos classification (pars flaccida retractions, particularly relevant to cholesteatoma precursor pockets)
Clinical Presentation
Symptoms
- Hearing loss — typically conductive, slowly progressive; due to obliteration of the middle ear space and, in advanced stages, ossicular erosion (particularly the long process of incus)
- Aural fullness — sensation of blocked ear
- Autophony in some patients
- Recurrent otorrhoea — if co-existing OME or secondary infection occurs
- Otalgia — usually mild or absent; significant pain suggests secondary infection
- In many patients, particularly children, the condition is asymptomatic and detected incidentally on otoscopy
Signs on Otoscopy
| Finding | Stage |
|---|---|
| Slightly dull, indrawn pars tensa | Stage I |
| TM touching long process of incus; incus may appear prominently through the membrane | Stage II |
| TM draped over promontory; "disappearing" middle ear space; TM moves toward the medial wall on Valsalva, not away | Stage III |
| Flat, featureless TM plastered to ossicles and promontory; no middle ear space | Stage IV (adhesive OM) |
Additional otoscopic findings:
- Tympanosclerosis (white chalky plaques)
- Amber/dull appearance if OME is co-existing
- Retraction pockets in pars tensa or pars flaccida — the most dangerous finding as they represent precursors to primary acquired cholesteatoma

Fig. 140.1 — Middle ear atelectasis with effusion (Cummings Otolaryngology)
Investigations
1. Otoscopy / Endoscopy / Pneumatoscopy
- Gold standard for diagnosis and staging
- Pneumatoscopy (Siegle speculum) assesses TM mobility — reduced or absent in atelectasis
- Endoscopic otoscopy provides magnification and enables staging
- Retraction pockets must be assessed: are they self-cleaning (keratin naturally migrates out) or progressive/non-cleaning (keratin accumulates — cholesteatoma precursor)?
2. Audiological Assessment
- Pure tone audiogram (PTA) — typically shows conductive hearing loss (air-bone gap); degree correlates with stage
- Tympanometry — type B (flat) curve if effusion present; type C (negative peak) if ETD without effusion
- Stapedial reflex testing — absent in significant conductive loss
3. Eustachian Tube Function Tests
- Toynbee test, Valsalva manoeuvre — clinical assessment of tube patency
- Sonotubometry or tubomanometry — objective measures used in research and some centres
4. Imaging
- High-resolution CT (HRCT) of the temporal bone — indicated when:
- Ossicular erosion is suspected (particularly incus long process)
- Retraction pocket depth cannot be fully assessed
- Cholesteatoma is a differential diagnosis
- Pre-operative planning for surgical management
- Shows degree of middle ear space obliteration, ossicular chain integrity, mastoid pneumatisation
- MRI (non-EPI DWI sequences) — increasingly used to differentiate cholesteatoma from inflammatory tissue, particularly when recurrence after surgery is suspected
5. Examination Under Microscope / Microlaryngoscopy
- Allows precise assessment of retraction pockets and their extent
- Essential pre-operatively
Management
Management is guided by stage, rate of progression, degree of hearing loss, and presence of cholesteatoma risk.
Conservative (Stages I–II, Early Stage III)
1. Treatment of underlying eustachian tube dysfunction
- Treatment of contributing upper respiratory conditions: allergic rhinitis, adenoidal hypertrophy, chronic rhinosinusitis
- Nasal corticosteroid sprays for allergic rhinitis
- Autoinflation (Otovent balloon) — may improve ETD and partially reverse early retraction
- Hearing aids as a temporising measure in bilateral disease with hearing loss
2. Watchful waiting with surveillance
- Early-stage retractions that are fully visible and self-cleaning may be monitored with regular otoendoscopy (3–6 monthly intervals)
- Serial audiograms to detect progression
Surgical Management
A. Ventilation (Grommet/Tympanostomy) Tubes
- Indicated for Stages I–III when ETD is the main driver and the TM is not yet adherent
- Sadé (1992) demonstrated improvement in atelectatic ears following ventilation tube insertion
- Graham and Knight reported reversal of atelectasis with grommets in selected cases
- Tubes bypass the dysfunctional eustachian tube, restore positive middle ear pressure, and allow the TM to return toward a more normal position
- Repeated insertion may be required; longer-term T-tubes are preferred in refractory cases
B. Myringoplasty / Tympanoplasty
- Indicated in Stage III–IV when:
- Significant hearing loss or ossicular erosion is present
- Retraction pocket is progressive or non-self-cleaning
- After grommet insertion has failed to reverse atelectasis
- Goal: reinforcement of the atelectatic/thinned tympanic membrane
- Techniques include cartilage tympanoplasty (cartilage shield or palisade) — cartilage is rigid and resists re-retraction; provides durable repair
- Temporalis fascia, perichondrium, or tragal cartilage may be used
- Cummings notes that myringoplasty for reinforcement of the atelectatic TM is indicated in extreme cases with hearing loss or ossicular erosion
C. Ossiculoplasty
- When ossicular erosion has occurred (typically long process of incus or stapes superstructure)
- Performed concurrently with tympanoplasty
- Options: partial ossicular replacement prosthesis (PORP), total ossicular replacement prosthesis (TORP), incus interposition
D. Management of Retraction Pockets (Cholesteatoma Precursors)
- Self-cleaning and stable: surveillance
- Progressive, non-self-cleaning, or keratin-accumulating: surgical excision with reconstruction
- The approach escalates to canal wall down or canal wall up mastoidectomy if cholesteatoma has developed
E. Mastoidectomy
- Indicated when cholesteatoma has developed from an atelectatic retraction pocket
- Also used in combination with tympanoplasty in cases of poor mastoid pneumatisation to improve the long-term ventilation reservoir for the middle ear
Complications
| Complication | Mechanism |
|---|---|
| Adhesive otitis media | End-stage atelectasis (Stage IV) |
| Conductive hearing loss | Obliteration of middle ear space + ossicular erosion |
| Sensorineural hearing loss | Chronic middle ear inflammation extending to inner ear |
| Primary acquired cholesteatoma | Keratin accumulation in non-self-cleaning retraction pocket |
| Ossicular erosion | Pressure necrosis from retracted TM; incus long process most vulnerable |
| Tympanosclerosis | Collagen destruction and calcification within TM |
| Labyrinthine fistula | From cholesteatoma erosion of lateral semicircular canal |
| Facial nerve paralysis | Cholesteatoma extending to fallopian canal |
| Intracranial infection | Advanced cholesteatoma |
Summary
Middle ear atelectasis is a progressive complication of eustachian tube dysfunction, representing the medial collapse of the tympanic membrane into the middle ear cleft. Using the Sadé-Berco classification (Stages I–IV), it spans a spectrum from simple retraction to full adhesive otitis media. The transition from reversible atelectasis (Stage III) to irreversible adhesion (Stage IV) and to cholesteatoma is the central clinical concern. Management hinges on addressing underlying ETD, ventilation tube insertion for early-to-moderate disease, and cartilage tympanoplasty with or without ossiculoplasty for advanced disease. Early diagnosis and regular surveillance are critical to preventing cholesteatoma formation.
Sources: Cummings Otolaryngology Head and Neck Surgery, Chapter 140 (Complications of Otitis Media); K. J. Lee's Essential Otolaryngology — Cummings Otolaryngology Head and Neck Surgery, pp. 2681–2683
Make it into pdf please
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your PDF is ready (688 KB). Download it here:
Atelectasis Middle Ear
PDF Document · PDF
What's included in the PDF:
- Formatted title banner with subtitle
- All 8 sections: Definition, Pathophysiology, Grading, Clinical Presentation, Investigations, Management, Complications, Summary
- Two clinical images embedded — the Sadé-Berco staging diagram and the otoscopic photo of atelectasis with effusion
- Colour-coded tables (navy headers, alternating rows) for easy reading
- Full source citations at the bottom
This is a shared conversation. Sign in to Orris to start your own chat.