I m preparing for Ini ss cardiology how can u help me prepare
Asking for Preferences
Here's a clear plan for how I can help you prepare for INI-SS Cardiology, starting with ECG & Arrhythmias:
How I Can Help You - Full Preparation Plan
1. Topic Explanations & Notes
I'll pull content from authoritative cardiology textbooks in my library and give you structured, high-yield notes on any topic you ask. For ECG & Arrhythmias, I can cover:
- ECG basics - intervals, axes, waveforms
- Arrhythmia classification (supraventricular vs ventricular)
- AF, AFL, SVT, WPW, VT, VF - mechanisms, ECG features, management
- Heart blocks (1st, 2nd Mobitz I/II, 3rd degree)
- Channelopathies - Brugada, Long QT, CPVT
- Pacemakers and device therapy
2. MCQ Practice & Quizzes
After any topic, I can generate INI-SS style MCQs with explanations - the kind that test clinical reasoning, not just recall.
3. High-Yield Topic List for INI-SS Cardiology
INI-SS is a superspecialty entrance, so the focus is on:
- Applied clinical cardiology (ECG interpretation, hemodynamics)
- Interventional concepts (PCI, EP procedures, devices)
- Guidelines-based management (ACC/AHA, ESC)
- Recent trial data (ISCHEMIA, EMPEROR, DAPA-HF, GWTG, etc.)
How to Use Me Most Effectively
Just tell me one of the following at any time:
| Command | What I'll do |
|---|---|
| "Explain [topic]" | Detailed notes from textbooks + key points |
| "MCQs on [topic]" | 5-10 INI-SS style questions with answers |
| "High-yield points on [topic]" | Bullet-point revision summary |
| "What's new in [topic]" | Recent trial/guideline updates |
| "ECG quiz" | I'll describe an ECG scenario and ask you to interpret |
Let's Start Now - ECG & Arrhythmias
Since you picked ECG & Arrhythmias as your starting point, here's what I suggest:
Option A - Ask me: "Give me high-yield notes on AF management"
Option B - Ask me: "Give me 10 MCQs on heart blocks"
Option C - Ask me: "Explain WPW syndrome with ECG features"
Just fire away with any topic or question - I'm ready to go deep on whatever you need. What would you like to tackle first?
Explain atrial fibrillation: pathophysiology, ECG, and INI-SS management approach
Reading File
Finding Sources
Searching PubMed
"atrial fibrillation"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed to write a complete, INI-SS grade answer. Here it is:
Atrial Fibrillation - Complete INI-SS Guide
1. PATHOPHYSIOLOGY
Triggers - Where AF Starts
AF is triggered most commonly by rapid firing ectopic foci in the pulmonary veins (PVs). Sleeves of atrial cardiomyocytes extend 1-3 cm into the PV walls and can fire at rates up to 300-600/min. A PAC (premature atrial contraction) from these foci can initiate the arrhythmia.

(From Morgan & Mikhail's Clinical Anesthesiology / Braunwald's Heart Disease)
Two Main Electrophysiological Mechanisms
| Mechanism | Description | Relevance |
|---|---|---|
| Focal activation | Ectopic focus (usually at PV ostia) fires rapidly, creating fibrillatory wavelets spreading outward | Basis for PV isolation ablation |
| Multiple wavelet reentry | Wavelets randomly reenter previously activated tissue; self-perpetuating chaos | Atrial size matters - bigger atrium = more wavelets = more stable AF |
The Substrate - "AF Begets AF"
The atrial substrate is as important as the trigger:
- Structural remodeling - Atrial fibrosis, dilatation (from hypertension, valvular disease, HF), inflammation - all create patchy conduction slow zones ideal for reentry.
- Electrical remodeling - Sustained AF shortens the atrial effective refractory period (ERP), making it harder to cardiovert and easier to sustain. This is why chronic AF is harder to revert than paroxysmal AF.
- Calcium overload - Rapid firing causes intracellular Ca²+ overload, which further impairs atrial mechanical function and promotes triggered activity.
- Autonomic influences - Vagal predominance (during sleep, post-prandial) shortens ERP heterogeneously; sympathetic excess (stress, thyrotoxicosis) also triggers AF.
INI-SS Pearl: "AF begets AF" is Wijffels' concept - the longer AF persists, the more the atrium remodels to sustain it. This is why early rhythm control (EAST-AFNET 4 trial) is now preferred.
Key Associations (Know These for MCQs)
- Hypertension - Most common cause overall
- Rheumatic mitral stenosis - LA pressure + stretch + inflammation; highest thromboembolic risk (warfarin mandatory, DOACs not used)
- Thyrotoxicosis - Must rule out in new AF; treat thyroid first
- Post-cardiac surgery - Up to 35% incidence; usually self-limiting
- Lone AF - No structural heart disease; younger patients; good prognosis
- Sleep apnea, obesity - Increasingly recognized as modifiable risk factors
2. ECG FEATURES
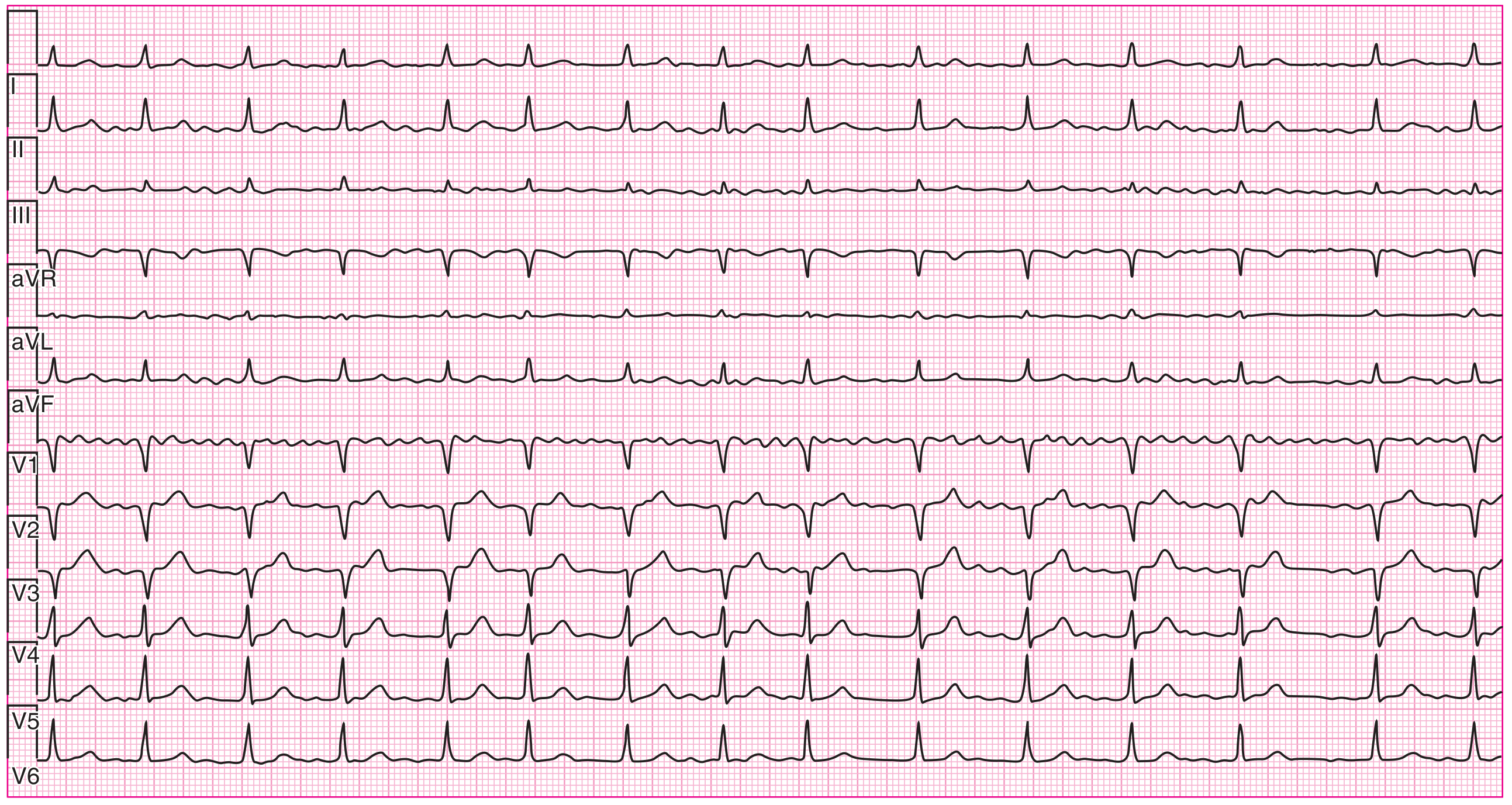
(Harrison's Principles of Internal Medicine, 22e - ECG of irregularly irregular heart rhythm. Disorganized atrial activation best seen in lead V1)
The Classic ECG Triad
| Feature | Detail |
|---|---|
| No P waves | Replaced by fibrillatory (f) baseline - chaotic, irregular undulations. Best seen in V1 and inferior leads |
| Irregularly irregular R-R intervals | This is the hallmark. No two R-R intervals are equal |
| Narrow QRS complexes | Usually - unless aberrant conduction (BBB) or pre-excitation (WPW) |
Rate Ranges
- Atrial rate: 350-700 bpm (chaotic, not measurable as discrete waves)
- Ventricular rate (uncontrolled): 120-170 bpm in untreated AF (AV node acts as the "gatekeeper")
- Rapid ventricular response >200 bpm = suspect WPW with accessory pathway! (Wide, bizarre QRS pattern - "FBI" - Fast, Broad, Irregular)
Key ECG Differentials for INI-SS
| Feature | AF | Atrial Flutter | MAT |
|---|---|---|---|
| Rhythm | Irregularly irregular | Regular (or regularly irregular) | Irregularly irregular |
| P waves | Absent; fibrillatory baseline | Sawtooth flutter waves, 300 bpm | ≥3 distinct P wave morphologies |
| Ventricular rate | Variable | Usually 150 bpm (2:1 block) | 100-180 bpm |
| Best seen in | V1 | Inferior leads + V1 | Any lead |
3. CLASSIFICATION - Know This Cold
| Type | Duration | Key Point |
|---|---|---|
| Paroxysmal | Self-terminating <7 days (usually <48 h) | Higher ablation success rate |
| Persistent | >7 days, requires intervention to terminate | Cardioversion needed |
| Long-standing persistent | >12 months, yet rhythm control attempted | Reduced ablation success |
| Permanent | Rate control accepted; rhythm control abandoned | No cardioversion attempted |
| First detected | First episode regardless of duration | May be paroxysmal or persistent |
4. INI-SS MANAGEMENT APPROACH
The framework is four pillars: Anticoagulation + Blood pressure/risk factor control + Cardioversion/rhythm vs. rate control + Device therapy (ablation).
PILLAR 1: ANTICOAGULATION (Thromboembolic Prevention)
CHA₂DS₂-VASc Score
| Criterion | Points |
|---|---|
| Congestive heart failure | 1 |
| Hypertension | 1 |
| Age ≥75 years | 2 |
| Diabetes mellitus | 1 |
| Stroke/TIA/TE | 2 |
| Vascular disease (CAD/PAD) | 1 |
| Age 65-74 years | 1 |
| Sex (female) | 1 |
| Max | 9 |
Decision rule (2023 ACC/AHA Guideline):
- Score 0 (male) / 1 (female): No anticoagulation
- Score 1 (male): Consider anticoagulation
- Score ≥2 (male) / ≥3 (female): Anticoagulate
Drug Choice
| Situation | Drug |
|---|---|
| Non-valvular AF | DOAC preferred (apixaban > rivaroxaban > dabigatran) |
| Valvular AF (rheumatic MS, mechanical valve) | Warfarin ONLY (DOACs contraindicated) |
| CKD (CrCl <15 mL/min) | Warfarin (DOACs mostly not studied; apixaban has most data) |
| Stable CAD + AF | DOAC alone (drop antiplatelet after 12 months) |
INI-SS Exam Trap: Valvular AF + DOAC = wrong answer. Warfarin is mandatory in rheumatic mitral stenosis and mechanical prosthetic valves.
HAS-BLED Score (Bleeding Risk)
Used to identify and correct modifiable bleeding risks - not to withhold anticoagulation if CHA₂DS₂-VASc is high.
PILLAR 2: RATE CONTROL
Target: Resting HR <80-110 bpm (lenient rate control is acceptable per RACE II trial - target <110 acceptable in asymptomatic patients)
| Drug | Use When | Avoid When |
|---|---|---|
| Beta-blockers (metoprolol, bisoprolol) | AF + HFrEF, post-MI, thyrotoxicosis | Severe bronchospasm, hemodynamic instability |
| Non-DHP CCBs (diltiazem, verapamil) | AF + preserved EF; best for acute rate control | AF + HFrEF (negative inotrope) |
| Digoxin | AF + HFrEF, sedentary patients; add-on | Lone AF, vagotonic AF; narrow therapeutic window |
| Amiodarone | Refractory cases, critically ill | Long-term: thyroid/pulmonary/hepatic toxicity |
INI-SS Trap: Never give verapamil/diltiazem in AF + WPW - they block the AV node, forcing all impulses down the accessory pathway → VF risk.
PILLAR 3: RHYTHM CONTROL
When to choose rhythm over rate control:
- Symptomatic despite rate control
- First episode, young patient
- AF precipitating HF (tachycardia-mediated cardiomyopathy)
- Patient preference
- EAST-AFNET 4 (2020): Early rhythm control within 1 year of diagnosis reduced cardiovascular death/stroke/HF hospitalization (HR 0.79)
Cardioversion Protocol
Key rule: If AF >48 hours (or unknown duration) - 3 weeks anticoagulation BEFORE cardioversion, then 4 weeks AFTER (to cover "atrial stunning").
- Shortcut: TEE-guided cardioversion if immediate CV needed (rule out LA appendage thrombus first).
| Method | Details |
|---|---|
| Electrical (DC) cardioversion | 150-200 J biphasic; synchronized; preferred for hemodynamically unstable |
| Pharmacological cardioversion | Flecanide/propafenone (Pill-in-the-pocket) - only in structurally normal heart; ibutilide; amiodarone (slower) |
"Pill-in-the-pocket": Flecanide 200-300 mg or propafenone 450-600 mg as a single oral dose for patient-initiated cardioversion in paroxysmal AF without structural heart disease. Must pre-test in hospital setting.
Antiarrhythmic Drugs (AADs) for Maintenance of Sinus Rhythm
| Drug | Use In | Avoid In |
|---|---|---|
| Flecanide / Propafenone | No structural heart disease | CAD, HFrEF, LVH |
| Sotalol | Mild-moderate structural disease, normal QTc | QT prolongation, renal failure |
| Amiodarone | HFrEF, severe structural disease; most effective | Long-term toxicity (thyroid, lung, liver, cornea) |
| Dofetilide | HFrEF | QT prolongation; requires in-hospital initiation |
| Dronedarone | Mild structural disease | HFrEF (↑ mortality), permanent AF |
PILLAR 4: CATHETER ABLATION (INI-SS Superspecialty Focus)
Pulmonary vein isolation (PVI) is the cornerstone procedure.
- Mechanism: Electrically isolate PV ostia from LA to eliminate the trigger foci
- Indication (2023 ACC/AHA Class I): Symptomatic paroxysmal AF failing ≥1 AAD; also reasonable as first-line (Class IIa)
- Success rates: ~70-80% for paroxysmal AF; lower for persistent AF (more substrate-dependent)
- CABANA trial: Ablation reduced AF recurrence and improved QoL vs. drug therapy; borderline mortality benefit
- Complications: PV stenosis, atrio-esophageal fistula (rare but fatal), phrenic nerve palsy, cardiac tamponade, stroke
Advanced ablation targets beyond PVI:
- CFAE (Complex Fractionated Atrial Electrograms) - areas of slow conduction
- Posterior wall isolation
- Linear lesions (roof line, mitral isthmus)
- Left atrial appendage (LAA) exclusion - for anticoagulation-intolerant patients (WATCHMAN device)
SPECIAL SITUATIONS (High-Yield for INI-SS)
| Scenario | Management |
|---|---|
| Hemodynamically unstable AF | Immediate DC cardioversion (don't wait for anticoagulation) |
| AF + WPW | IV procainamide or ibutilide; DC cardioversion if unstable. NEVER adenosine, digoxin, verapamil, diltiazem, beta-blockers |
| AF + Acute MI | Heparin + rate control; cardioversion if unstable; beware DOAC + dual antiplatelet bleeding risk |
| AF + Thyrotoxicosis | Treat thyroid first; beta-blockers for rate; spontaneous cardioversion common after euthyroid |
| Postoperative AF | Usually self-limiting; rate control first; cardiovert if >48h or symptomatic |
| Pregnancy + AF | Digoxin or beta-blocker (metoprolol) for rate; heparin/LMWH (DOACs contraindicated); quinidine for rhythm |
| AF + HFrEF | Beta-blocker + digoxin for rate; amiodarone if rhythm control; ablation shown to improve EF (CASTLE-AF) |
5. RECENT GUIDELINES UPDATE (2023 ACC/AHA + 2024 ESC)
The 2023 ACC/AHA AF guideline and 2024 ESC AF guideline introduced key updates:
- "ABC" pathway (ESC 2024): Anticoagulation + Better symptom management (rate/rhythm) + Cardiovascular risk factor and comorbidity management
- Catheter ablation upgraded to Class I for symptomatic paroxysmal AF (was IIa)
- Early rhythm control is preferred (not just rate control) - within 1 year of diagnosis
- Risk factor modification (weight loss, BP control, sleep apnea treatment, exercise) is now a formal part of AF management, not just an afterthought
- DOACs remain preferred over warfarin for non-valvular AF; anti-Xa agents (apixaban, rivaroxaban) preferred over dabigatran in elderly/renal impairment
QUICK RECALL TABLE - INI-SS Mnemonics
CHA₂DS₂-VASc = CHF, HTN, Age≥75 (×2), DM, Stroke (×2), Vascular, Age 65-74, Sex(F)
HAS-BLED = HTN uncontrolled, Abnormal renal/liver, Stroke, Bleeding, Labile INR, Elderly (>65), Drugs/alcohol
AAD choice memory: "No structural disease = Flecanide/No coronary disease = Propafenone / CAD = Sotalol / HF = Amiodarone"
Sources: Braunwald's Heart Disease (11e), Harrison's Principles of Internal Medicine (22e), Tintinalli's Emergency Medicine, Morgan & Mikhail's Clinical Anesthesiology | 2023 ACC/AHA AF Guideline (Circulation, 2024) | 2024 ESC AF Guideline (Eur Heart J, 2024)
Want me to now generate 10 INI-SS style MCQs on AF to test your understanding of this material?
Compare rhythm control vs rate control trials (AFFIRM, RACE, EAST-AFNET)
Finding Sources
Searching PubMed
"EAST-AFNET 4" AND "atrial fibrillation" AND "early rhythm control"
Searching PubMed
AFFIRM trial "atrial fibrillation" AND "rate control" AND "rhythm control"
Reading File
Reading Article
PMID: 32865375
Reading Article
PMID: 12466506
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have all the data needed. Let me compile the complete, INI-SS-grade trial comparison.
Rhythm Control vs. Rate Control in AF - Trial Deep Dive
The Central Question
Does restoring and maintaining sinus rhythm (rhythm control) improve outcomes compared to simply controlling heart rate and letting AF persist (rate control)?
The answer changed dramatically over 20 years:
2002: "Rate control is fine - rhythm control offers no survival benefit and more harm" 2020: "Early rhythm control reduces cardiovascular death and stroke - paradigm shift"
TRIAL 1: AFFIRM (2002)
Atrial Fibrillation Follow-up Investigation of Rhythm Management
| Parameter | Detail |
|---|---|
| Published | N Engl J Med, December 2002 (PMID 12466506) |
| Design | Randomized, multicenter, open-label RCT |
| N | 4,060 patients |
| Population | AF + high risk of stroke or death; mean age 69.7 years; 70.8% hypertensive; 38.2% CAD; 64.7% dilated LA |
| Duration | Up to 5 years follow-up |
| Primary endpoint | Overall mortality |
Arms
| Rate Control | Rhythm Control |
|---|---|
| AV nodal blockers (BB, CCB, digoxin) | Antiarrhythmic drugs (AADs: amiodarone, sotalol, flecanide, propafenone) + repeated DC cardioversion |
| Warfarin continued in ALL patients | Warfarin continued in ALL patients |
Key Results
| Outcome | Rate Control | Rhythm Control | p-value |
|---|---|---|---|
| 5-year mortality | 21.3% | 23.8% | 0.08 (NS, trend favored rate control) |
| Hospitalizations | Lower | Higher | Significant |
| Adverse drug effects | Lower | Higher | Significant |
| Stroke rate | Similar | Similar | NS |
Hazard ratio for death with rhythm vs. rate control: 1.15 (95% CI 0.99-1.34)
The Paradox Within AFFIRM
An "on-treatment" sub-analysis showed:
- Patients who achieved sinus rhythm had better survival than those in AF
- But patients on AADs did NOT have better survival
- Conclusion: AADs negated the benefit of sinus rhythm with their toxicity/proarrhythmia
This suggested: "Sinus rhythm is good; old AADs are the problem" - setting the stage for ablation trials.
Another key finding: The majority of strokes in BOTH groups occurred after warfarin was stopped or the INR was subtherapeutic. This proved anticoagulation must NOT be stopped just because sinus rhythm is achieved.
AFFIRM Limitations
- Old drugs: Amiodarone, sotalol, flecanide/propafenone - all have significant toxicity. No ablation in this era.
- Old, high-risk population (mean age 69.7): Less likely to benefit from rhythm control
- Late diagnosis: Patients often had AF for years before enrollment - heavy atrial remodeling already present
- Cross-over: Many rate-control patients spontaneously stayed in sinus rhythm; rhythm-control patients crossed to AF - contaminated results
TRIAL 2: RACE (2002)
Rate Control versus Electrical Cardioversion for Persistent AF
| Parameter | Detail |
|---|---|
| Published | N Engl J Med, 2002 |
| Design | Randomized, multicenter RCT |
| N | 522 patients |
| Population | Persistent AF after ≥1 cardioversion; had been on anticoagulation for ≥1 year |
| Duration | 2.3 years median |
| Primary endpoint | Composite: cardiovascular death, HF, thromboembolic events, bleeding, pacemaker implantation, serious drug adverse effects |
Key Results
| Outcome | Rate Control | Rhythm Control |
|---|---|---|
| Primary composite | 17.2% | 22.6% |
| Trend | Favored rate control | NS (p=0.11) |
| QoL | Similar | Similar |
| AF recurrence in rhythm arm | ~50% | - |
RACE Conclusion
Rate control was non-inferior to rhythm control for the composite endpoint. Fewer adverse drug events with rate control.
RACE II (2010) - Lenient vs. Strict Rate Control
A follow-up study that tested:
- Strict rate control - resting HR <80 bpm + exercise HR <110 bpm
- Lenient rate control - resting HR <110 bpm
Result: Outcomes were similar. Lenient rate control was easier to achieve and just as safe - now forms the basis of the "HR <110 bpm at rest is acceptable" guideline recommendation.
TRIAL 3: EAST-AFNET 4 (2020) - The Game Changer
Early Treatment of Atrial Fibrillation for Stroke Prevention Trial
| Parameter | Detail |
|---|---|
| Published | N Engl J Med, October 2020 (PMID 32865375) |
| Design | International, investigator-initiated, parallel-group, open, blinded-outcome-assessment RCT |
| N | 2,789 patients; 135 centers |
| Population | AF diagnosed ≤1 year before enrollment + ≥1 cardiovascular condition (HTN, CKD, EF<50%, DM, age≥75, stroke, HF, PAD) |
| Median time since AF diagnosis | 36 days (very early enrollment) |
| Duration | Stopped early for efficacy at interim analysis; median 5.1 years follow-up |
| Primary endpoint 1 | Composite: CV death + stroke + hospitalization for worsening HF or acute coronary syndrome |
| Primary endpoint 2 | Nights in hospital per year |
Arms
| Early Rhythm Control | Usual Care |
|---|---|
| AADs and/or catheter ablation from the start | Rhythm control permitted only for symptom management |
| All patients anticoagulated | All patients anticoagulated |
Key Results
| Outcome | Early RC | Usual Care | Result |
|---|---|---|---|
| Primary composite (per 100 person-years) | 3.9 | 5.0 | HR 0.79 (96% CI 0.66-0.94; p=0.005) |
| Nights in hospital/year | 5.8 | 5.1 | No significant difference |
| Sinus rhythm at 2 years | ~83% | ~60% | Higher in early RC arm |
| Serious adverse events from RC therapy | 4.9% | 1.4% | Higher in early RC |
21% relative risk reduction in the primary composite endpoint with early rhythm control
Why EAST-AFNET 4 Succeeded Where AFFIRM "Failed"
| Factor | AFFIRM | EAST-AFNET 4 |
|---|---|---|
| AF duration at enrollment | Months to years | Median 36 days |
| Patient age | Mean 69.7 yr (older, sicker) | Mixed; more representative |
| Rhythm tools | Mainly AADs | AADs + catheter ablation |
| Goal | Maintain sinus rhythm at all costs | Early, systematic rhythm control |
| AF burden at baseline | Heavy remodeling present | Minimal structural remodeling |
| Primary endpoint | Mortality alone | Composite (CV death + stroke + HF hospitalization + ACS) |
The core insight: The benefit of rhythm control is TIME-DEPENDENT. Intervening early, before atrial remodeling becomes irreversible, prevents downstream events. AF causes stroke, HF, and cognitive decline not just through fast rates but through ongoing atrial remodeling and thrombogenesis even during "controlled" AF.
Head-to-Head Trial Comparison Table
| Feature | AFFIRM (2002) | RACE (2002) | EAST-AFNET 4 (2020) |
|---|---|---|---|
| N | 4,060 | 522 | 2,789 |
| AF duration at entry | Months-years | Persistent AF | ≤1 year (median 36 days) |
| Rhythm control method | AADs + DCCV | DCCV + AADs | AADs + catheter ablation |
| Primary endpoint | Mortality | CV composite | CV death + stroke + HF/ACS hospitalization |
| Result | Rate = Rhythm (NS) | Rate ≈ Rhythm (NS) | Early rhythm control superior (HR 0.79, p=0.005) |
| Trial stopped | Completed | Completed | Stopped early for efficacy |
| Hospitalizations | More in rhythm arm | Similar | Similar (nights in hospital NS) |
| Adverse drug effects | More in rhythm arm | More in rhythm arm | Small excess in RC arm (4.9% vs 1.4%) |
| Stroke finding | Most strokes when anticoagulation stopped | - | Benefit regardless of symptoms |
| Key message | Rate control is simpler, non-inferior | Rate control non-inferior | Treat early, treat rhythm |
Related Ablation Trials (INI-SS Must-Know)
CABANA (2019) - Ablation vs. Drug Therapy
- N: 2,204 patients
- Result: In the intention-to-treat analysis, ablation did NOT significantly reduce the primary composite (death, disabling stroke, serious bleeding, cardiac arrest) vs. drug therapy (HR 0.86, p=0.15)
- BUT: Per-protocol and on-treatment analyses showed benefit; subgroup with HF (similar to CASTLE-AF) showed mortality reduction
- Bottom line: CABANA = ablation improves QoL and reduces AF burden; no clear all-cause mortality benefit in unselected patients
CASTLE-AF (2018) - Ablation in HFrEF + AF
- N: 363 patients; AF + EF <35% + ICD/CRT-D
- Primary endpoint: All-cause death + worsening HF hospitalization
- Result: Ablation 28.5% vs. 44.6% with medical therapy (HR 0.62, p=0.007)
- Key message: Catheter ablation in AF + HFrEF REDUCES MORTALITY - this is a Class IIa indication now
The "Paradigm Shift" Summary for INI-SS
2002 (AFFIRM/RACE):
Rate control = Rhythm control → "Keep it simple, control rate"
2020 (EAST-AFNET 4):
Early rhythm control < 1 year > Rate control → "Treat early, prevent remodeling"
2024 ESC Guidelines (current):
Early rhythm control is now the PREFERRED strategy in eligible patients
Catheter ablation is Class I for symptomatic paroxysmal AF
Why this matters clinically
- Anticoagulation is NEVER stopped based on sinus rhythm achievement (AFFIRM lesson - most strokes occurred when warfarin was inappropriately stopped)
- Rhythm control benefit is time-dependent - early intervention before atrial fibrosis sets in is key
- Ablation changed the equation - AFFIRM used toxic old drugs; modern ablation + safer AADs tip the balance toward rhythm control
- Asymptomatic AF still needs rhythm control (EAST-AFNET 4 enrolled both symptomatic and asymptomatic patients; benefit was similar in both)
High-Yield INI-SS MCQ Concepts from These Trials
| Question | Answer |
|---|---|
| AFFIRM primary endpoint? | Overall mortality |
| AFFIRM result? | No significant difference (HR 1.15, p=0.08) |
| Which AFFIRM sub-analysis showed sinus rhythm is beneficial? | "On-treatment" analysis - sinus rhythm itself reduced mortality, but AADs negated benefit |
| AFFIRM: when did most strokes occur? | After warfarin was stopped/INR subtherapeutic |
| RACE primary endpoint? | CV composite (death, HF, TE, bleeding, pacemaker, drug AE) |
| RACE result? | Non-inferior (favored rate control trend) |
| EAST-AFNET 4: enrollment window? | ≤1 year after AF diagnosis |
| EAST-AFNET 4: primary result? | HR 0.79; 21% RRR in CV composite; p=0.005 |
| Why was EAST-AFNET 4 stopped? | Stopped early for efficacy at interim analysis |
| CASTLE-AF: in which patient subgroup does ablation reduce mortality? | AF + HFrEF (EF <35%) |
| CABANA: ITT result? | No significant difference; per-protocol showed benefit |
Sources: Braunwald's Heart Disease (11e), Fuster & Hurst's The Heart (15e), Textbook of Family Medicine (9e) | AFFIRM trial (NEJM 2002) | EAST-AFNET 4 (NEJM 2020) | 2023 ACC/AHA AF Guideline
Ready for the next topic? I can do:
- 10 MCQs based on these trials (exam-style)
- Heart failure + AF - CASTLE-AF deep dive + management
- Catheter ablation - indications, technique, complications
- Any other arrhythmia topic
This is a shared conversation. Sign in to Orris to start your own chat.