BMD PG level Physiotherapy assessment & management
Reading File
Finding Sources
Finding Sources
Searching the Web
BMD bone mineral density physiotherapy assessment management PG level
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
osteoporosis exercise physiotherapy bone mineral density
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have sufficient comprehensive content. Let me compile the full PG-level physiotherapy response.
BMD (Bone Mineral Density) - PG Level Physiotherapy: Assessment & Management
1. DEFINITION & OVERVIEW
Bone Mineral Density (BMD) is the amount of bone mineral (primarily calcium hydroxyapatite) per unit area or volume of bone tissue, expressed as g/cm². It is the most clinically important parameter for diagnosing osteoporosis, monitoring treatment response, and predicting fracture risk.
WHO Classification (based on DXA T-score):
| Category | T-score |
|---|---|
| Normal | ≥ -1.0 |
| Low bone density (Osteopenia) | -1.0 to -2.5 |
| Osteoporosis | ≤ -2.5 |
| Severe osteoporosis | ≤ -2.5 + fragility fracture |
T-score = SD difference from young normal peak BMD (20-29 year NHANES reference)
Z-score = SD difference from age-matched peers; used in premenopausal women and men <50 years; Z-score ≤ -2.0 = "below expected range for age"
Each 1 SD decrease in T-score increases fracture risk by 1.5-2x; risk increases exponentially below -2.5. - Goldman-Cecil Medicine, p. 2622
2. MEASUREMENT TECHNIQUES
2a. Gold Standard: Dual-Energy X-ray Absorptiometry (DXA)
- Measures areal BMD (g/cm²) at lumbar spine (L1-L4), proximal femur (total hip, femoral neck), and distal radius
- Low radiation dose (~1-10 µSv)
- Preferred sites: lumbar spine AND hip (both should be measured)
- Femoral neck and total hip are the best overall predictors of hip fracture
- Total hip preferred for monitoring (less affected by positioning, OA changes)
- Limitations: Cannot distinguish low BMD from osteomalacia; degenerative changes (facet OA, aortic calcification) can spuriously elevate lumbar spine BMD
2b. Quantitative Computed Tomography (QCT)
- Provides true volumetric BMD
- Can be equivalent to DXA hip measurements; may use WHO T-score criteria
- FDA-approved Biomechanical CT (BCT) assesses bone strength via finite element analysis
- Most useful when DXA is not possible (bilateral hip prostheses, prior lumbar fusion)
- Spinal QCT provides fracture risk data but WHO T-score criteria cannot be applied
2c. Quantitative Ultrasound (QUS)
- Measures bone at calcaneus - attenuation and speed of sound
- No radiation; cheaper; portable
- Cannot diagnose osteoporosis by WHO criteria
- Useful as a screening/triage tool in resource-limited settings
2d. High-Resolution pQCT (HRpQCT) & micro-MRI
- Research tools; may further refine fracture risk prediction
- Not used clinically for routine BMD diagnosis
2e. Trabecular Bone Score (TBS)
- A textural index derived from DXA lumbar spine image
- Reflects bone microarchitecture quality independent of BMD
- Poor TBS (≤1.23) = degraded microarchitecture; Intermediate (1.23-1.31); Normal (≥1.31)
- Can significantly add to FRAX fracture risk estimation
- Used as adjunct, not replacement, for BMD
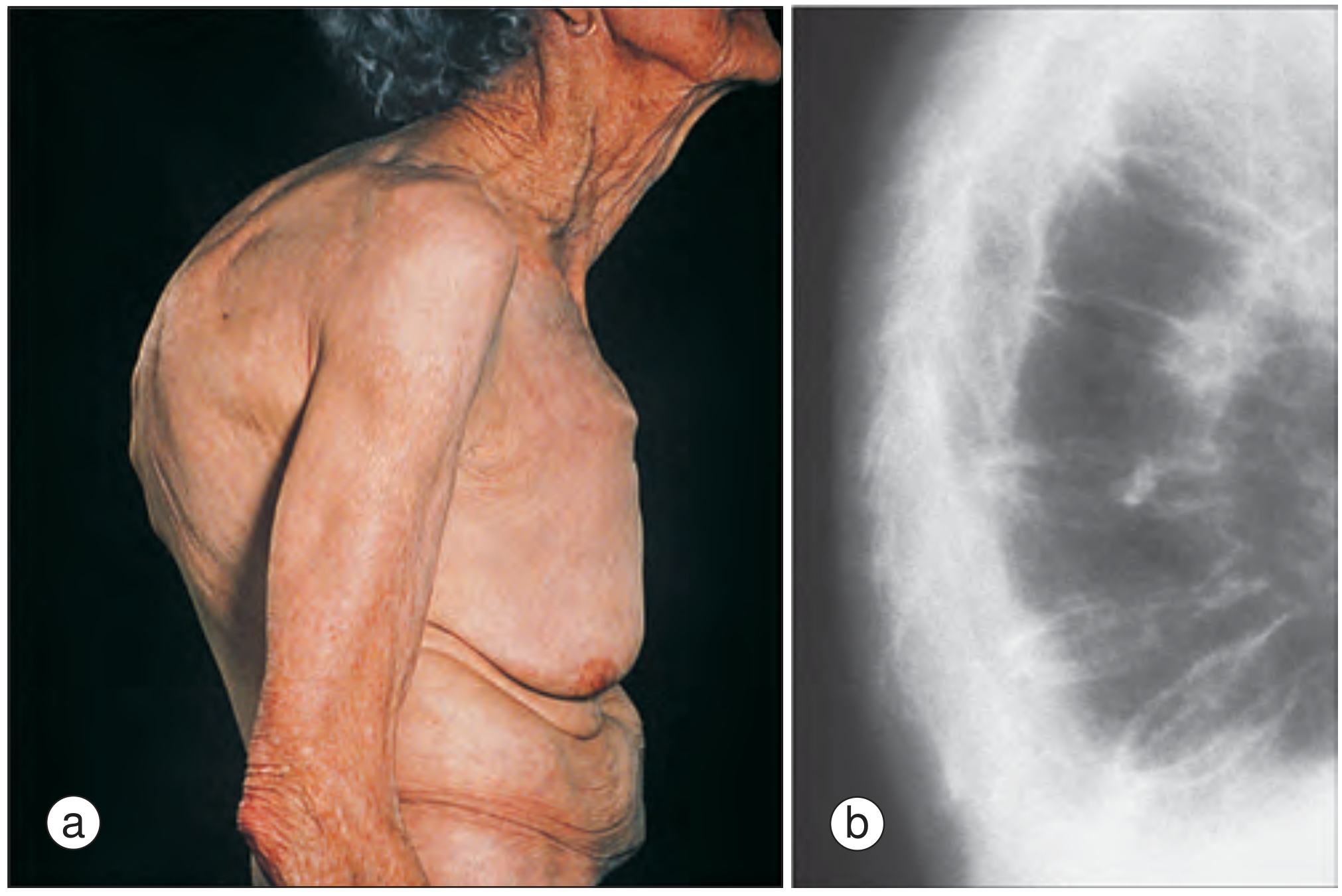
Dowager's hump: marked thoracic kyphosis due to multiple osteoporotic vertebral fractures (Rheumatology, 2-Vol Set, 2022)
3. PHYSIOTHERAPY ASSESSMENT
3a. Indications for BMD Testing (ISCD 2019 Guidelines)
- All women ≥65 years and men ≥70 years regardless of risk factors
- Postmenopausal women and men aged 50-70 with risk factors present
- Women in menopausal transition with low body weight, prior low-trauma fracture, or high-risk medications
- Adults with fragility fracture
- Adults on medications causing bone loss (glucocorticoids, aromatase inhibitors, anticonvulsants, GnRH analogues, PPIs, SSRIs, thiazolidinediones)
- Anyone being considered for or currently on pharmacological therapy
- Patients with spinal cord injury, undergoing orthopaedic procedures, or transgender patients
- Rheumatology 2-Vol Set, p. 4157
OST Screening Tool (Osteoporosis Self-Assessment Tool): Score = (Weight in kg - Age) × 0.2; threshold <2 indicates high risk; simple, validated tool for identifying BMD T ≤ -2.5 in younger postmenopausal women.
3b. Physiotherapy History & Risk Factor Assessment
Modifiable Risk Factors:
- Sedentary lifestyle / physical inactivity
- Smoking, alcohol excess (>3 units/day)
- Low calcium/vitamin D intake
- Low body weight (BMI <20)
- Falls history and fall risk factors
Non-Modifiable Risk Factors:
- Age, female sex, white/Asian ethnicity
- Premature menopause (<45 years), primary hypogonadism
- Family history of hip fracture (parental)
- Prior fragility fracture
Secondary Causes (PT must screen for):
- Glucocorticoid use (≥5 mg prednisone/day ≥3 months)
- Rheumatoid arthritis, IBD, coeliac disease
- Hyperparathyroidism, hyperthyroidism
- Chronic kidney disease, liver disease
- Immobilisation, paralysis
3c. Physiotherapy Physical Assessment
Postural Assessment:
- Thoracic kyphosis (Dowager's hump), forward head posture
- Height loss measurement (>4 cm loss is a red flag for silent vertebral fracture)
- Wall-occiput distance (normal = 0; >5 cm suggests thoracic kyphosis)
- Rib-pelvis distance (normal ≥2 fingers; reduced in vertebral fractures)
Balance & Fall Risk Assessment:
- Berg Balance Scale (BBS)
- Timed Up and Go test (TUG) - >12 seconds = increased fall risk
- Four Test Balance Scale
- Functional Reach Test
- Single Leg Stand test
Muscle Strength:
- Manual Muscle Testing (MMT)
- Grip dynamometry (low grip = surrogate for low bone mass)
- Core and paraspinal muscle endurance (Sorensen Test, McGill battery)
Gait Analysis:
- Gait speed, stride length, cadence
- Slow gait speed (<0.8 m/s) is associated with fracture risk
Functional Tests:
- 30-second Chair Stand Test (lower limb power)
- 6-Minute Walk Test (aerobic capacity)
- FRAX Tool: 10-year probability of major osteoporotic fracture and hip fracture using clinical risk factors ± BMD
Pain Assessment:
- VAS/NRS for back pain
- Identify acute vertebral fracture (sudden severe mid-thoracic/lumbar pain, kyphotic deformity, height loss)
Quality of Life:
- QUALEFFO (Quality of Life questionnaire for Osteoporosis)
- ECOS-16 (Assessment of Health-Related Quality of Life in Osteoporosis)
- OPAQ (Osteoporosis Assessment Questionnaire)
4. PHYSIOTHERAPY MANAGEMENT
4a. Goals of Physiotherapy
- Prevent further BMD loss or stimulate bone formation
- Reduce fracture risk (especially hip and vertebral)
- Fall prevention
- Improve posture, balance, and functional capacity
- Pain management (in acute vertebral fracture)
- Patient education and self-management
4b. Exercise Prescription for BMD
Exercise is the cornerstone of physiotherapy management. Effects require long duration (6 months to 4+ years) to produce measurable changes in BMD. (APTA/SIGN Clinical Practice Guideline, Grade B evidence)
i. Weight-Bearing Impact Exercise
- Walking, jogging, aerobics, dancing, stair climbing
- Mechanical loading through the skeleton stimulates osteoblast activity (Wolff's Law)
- Moderate-impact activities: jogging, hiking
- High-impact activities: jumping, hopping (contraindicated in severe osteoporosis/recent fracture)
- Recommendation (SIGN/APTA CPG): Static weight-bearing (SWB) exercises such as single-leg standing slow BMD decline at the hip in postmenopausal women (Grade B)
ii. Progressive Resistance Strength Training (PRST)
- Most evidence-based intervention for femoral neck BMD
- Systematic review (Hsu et al., 2024, PM&R): Moderate, statistically significant benefit on femoral neck BMD (Hedges' g = 0.583; 95% CI 0.031-1.135); no significant effect on lumbar spine BMD (g = 0.190)
- Optimal Parameters (Zhao et al., 2025, J Orthop Surg Res - Meta-analysis):
- Frequency: 3×/week
- Intensity: 60-85% 1RM
- Duration: ≥6 months
- Include major muscle groups: quadriceps, hip abductors/extensors, paraspinals, upper back
- Key exercises: Squats, lunges, deadlifts, leg press, hip extension, seated row, lat pulldown
iii. Balance and Proprioception Training
- Reduces fall risk independent of BMD effects
- Tai Chi: reduces fall risk and improves BMD; meta-analysis (Zhang & Chen, 2024, J Orthop Surg Res) confirms beneficial effects on bone health and fall prevention
- Balance board, perturbation training, dynamic balance activities
- Progress from static (double-leg stand) → semi-dynamic → dynamic tasks
iv. Postural Correction & Spinal Extension Exercises
- Targets thoracic kyphosis (key deformity)
- Spinal extension exercises (McKenzie extension, prone press-ups, thoracic extension over foam roller)
- Evidence: Spinal extension exercises reduce risk of new vertebral fractures
- Avoid spinal flexion exercises (sit-ups, crunches, rowing in flexion) - flexion loading increases vertebral compression fracture risk
- Posture retraining with scapular retraction, thoracic extension, core stabilization
v. Traditional Chinese/Mind-Body Exercises
- Tai Chi (Yang style): Best evidence among mind-body approaches; reduces falls, improves balance, mild positive effect on BMD (femoral neck)
- Qigong, Wushu: Emerging evidence; systematic reviews (Hou et al., 2024; Liu et al., 2024) show beneficial effects on BMD in menopausal women
- Yoga: Improves flexibility and balance; some evidence for positive effects on lumbar spine BMD
4c. FITT Principle for Osteoporosis Exercise
| Parameter | Recommendation |
|---|---|
| Frequency | Weight-bearing: 4-5×/week; Resistance: 2-3×/week; Balance: Daily |
| Intensity | Moderate-high (RPE 12-16/20); Resistance at 60-85% 1RM |
| Time | 30-60 min/session; minimum 6 months for BMD effects |
| Type | Weight-bearing impact + Resistance training + Balance exercises |
4d. Fall Prevention Programme
Falls are the proximate cause of most osteoporotic fractures. PT-led fall prevention is a direct injury-prevention strategy.
Components:
- Environmental modification - remove trip hazards, improve lighting, grab rails
- Footwear assessment - thin, hard-soled shoes improve proprioception
- Hip protectors - worn during high-risk activities (evidence limited but practical)
- Medication review referral - identify polypharmacy, sedatives, antihypertensives (fall-risk drugs)
- Assistive devices - walking sticks, frames when appropriate
- Multifactorial balance training - as above (Tai Chi, single-leg stance, perturbation training)
- Vision referral - impaired vision is an independent fall risk factor
4e. Pain Management (Acute Vertebral Fracture)
- Relative rest in acute phase (1-2 weeks), then graded mobilization
- Positioning in mild extension / prone lying
- TENS, heat therapy for pain modulation
- Thoracolumbosacral orthosis (TLSO) - spinal brace can reduce pain, improve posture, and prevent further collapse
- Graduated walking programme
- Gentle isometric paraspinal exercises when pain allows
- Hydrotherapy (aquatic physiotherapy): offloads spine, allows early mobilization, reduces pain
4f. Non-Exercise Physiotherapy Interventions
| Modality | Role |
|---|---|
| Hydrotherapy | Pain relief, early post-fracture mobilisation, aerobic exercise with reduced loading |
| TENS | Pain management in vertebral fracture |
| Whole Body Vibration (WBV) | Mechanical stimulus for bone; emerging evidence, particularly for hip BMD |
| Ultrasound therapy | Low-intensity pulsed US (LIPUS) - bone healing post-fracture |
| Orthotics | Spinal orthoses for vertebral fracture; footwear for fall prevention |
| Patient education | Fall prevention, home exercise programme, activity modification |
4g. Non-Pharmacological Nutritional Guidance (PT referral / advice)
- Calcium: 1000-1200 mg/day (dairy, leafy greens, fortified foods)
- Vitamin D: 800-2000 IU/day (sunlight exposure + supplements); critical for calcium absorption and muscle function
- Adequate protein intake (1.0-1.2 g/kg/day in older adults)
- Limit alcohol (<2 units/day), eliminate smoking, limit caffeine
4h. Pharmacological Management (for PT awareness)
Physiotherapists must understand medications to monitor response (serial BMD) and understand drug-exercise interactions:
| Drug Class | Example | Mechanism |
|---|---|---|
| Bisphosphonates (1st line) | Alendronate, risedronate, zoledronate | Inhibit osteoclast-mediated bone resorption |
| RANKL inhibitor | Denosumab | Anti-RANKL antibody, reduces osteoclast activity |
| SERMs | Raloxifene | Estrogen receptor modulator, reduces vertebral fractures |
| Anabolic agents | Teriparatide (PTH 1-34), abaloparatide | Stimulate bone formation |
| Sclerostin inhibitor | Romosozumab | Dual action: increases formation + reduces resorption |
| Hormone therapy | Estrogen/HRT | Anti-resorptive; postmenopausal |
| Testosterone | In men with hypogonadism (T <200 ng/dL) | Improves BMD |
Pharmacotherapy alone reduces fracture risk by ~50%; combined with physiotherapy-led exercise, outcomes are optimized.
5. VERTEBRAL FRACTURE ASSESSMENT (VFA) in Physiotherapy Context
Indications for VFA referral (from physiotherapy assessment):
- T-score < -1.0 AND any of:
- Women ≥70 / Men ≥80 years
- Historical height loss >4 cm (>1.5 inches)
- Self-reported undocumented prior vertebral fracture
- Glucocorticoid therapy ≥5 mg prednisone/day
- Rheumatology 2-Vol Set, p. 4206
VFA by DXA: lower cost, lower radiation than plain radiographs; point-of-care imaging of T4-L4.
6. SERIAL BMD MONITORING IN PHYSIOTHERAPY
- Baseline BMD before starting exercise programme
- Repeat DXA at 1-2 years after starting treatment (pharmacological or exercise)
- Always measure at same DXA machine (inter-machine variability confounds results)
- Monitoring tracks treatment response, adherence, and secondary causes of ongoing bone loss
- Least Significant Change (LSC): Statistical threshold to distinguish true BMD change from measurement error (typically 2-3% at spine, 3-5% at hip); only changes exceeding LSC are clinically significant
7. SPECIAL POPULATIONS IN PHYSIOTHERAPY
| Population | Key Considerations |
|---|---|
| Premenopausal women | Z-score used; high-impact exercise most beneficial to maximize peak BMD |
| Postmenopausal women | Greatest risk group; PRST + weight-bearing impact; falls prevention priority |
| Men (>70 years) | DXA indicated; bisphosphonates effective; check testosterone |
| Glucocorticoid-induced osteoporosis | Rapid bone loss; early physiotherapy intervention; annual DXA |
| Spinal cord injury | Immobilisation-related bone loss; NMES, standing programmes, FES cycling |
| Paediatric/Adolescent | Focus on maximizing peak BMD through sport, weight-bearing, calcium intake |
8. PHYSIOTHERAPY OUTCOME MEASURES SUMMARY
| Domain | Tool |
|---|---|
| BMD | DXA T-score/Z-score |
| Fracture risk | FRAX score (10-year probability) |
| Balance | BBS, TUG, Functional Reach, Single Leg Stand |
| Strength | Grip dynamometry, 30s Chair Stand, MMT |
| Functional capacity | 6MWT, gait speed |
| Posture | Wall-occiput distance, rib-pelvis gap |
| Pain | NRS/VAS |
| Quality of life | QUALEFFO, OPAQ, ECOS-16 |
| Fall risk | Falls Efficacy Scale (FES-I) |
Recent Evidence Updates (PubMed, 2024-2025)
- Optimal resistance training parameters for BMD in postmenopausal women (Zhao F et al., 2025, J Orthop Surg Res - Meta-analysis; PMID: 40420105): 3×/week, 60-85% 1RM, ≥6 months duration produces significant BMD gains at femoral neck
- Exercise effects on BMD in postmenopausal women (Hsu HH et al., 2024, PM&R - Systematic review/Meta-analysis; PMID: 39032163): Significant benefit at femoral neck (g=0.583); combined resistance + impact exercise most effective
- Tai Chi for bone health and fall prevention (Zhang Y & Chen H, 2024, J Orthop Surg Res - Meta-analysis; PMID: 39127644): Tai Chi improves both BMD and fall risk in postmenopausal women
- Traditional Chinese exercises and BMD (Hou J et al., 2024 - Network meta-analysis; PMID: 39328990): Multiple modalities (Baduanjin, Wuqinxi, Tai Chi) improve BMD; Baduanjin may be most effective
Key Clinical Pearls for PG Physiotherapy
- Exercise must be long-term (≥6 months for BMD, ≥1 year for fracture reduction) - set realistic patient expectations
- Combine modalities: Resistance + weight-bearing impact + balance training is superior to any single type
- Avoid spinal flexion in osteoporotic patients - increases vertebral compression fracture risk
- Falls prevention = fracture prevention - even without BMD change, reducing falls directly reduces fractures
- FRAX tool should guide intervention intensity - patients with >20% 10-year major fracture risk need both pharmacotherapy and physiotherapy
- Height loss >4 cm or new back pain = suspect vertebral fracture; refer for VFA/imaging before progressing exercise
- Whole-body vibration (WBV) may be useful when weight-bearing exercise is not feasible (frail/severe osteoporosis)
- Aquatic therapy is safe for severe osteoporosis where land-based impact exercise is contraindicated, but does NOT stimulate bone formation (non-weight-bearing medium)
Sources: Rheumatology 2-Volume Set (Elsevier, 2022); Goldman-Cecil Medicine International Edition (2-Volume, Elsevier); APTA Academy of Geriatric Physical Therapy Clinical Practice Guideline (2022); ISCD Official Positions (2019); PubMed meta-analyses (2024-2025)
Beaker's musclulo dystrophy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
Becker muscular dystrophy physiotherapy management exercise
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
Becker muscular dystrophy physiotherapy assessment management clinical guidelines 2024
I now have comprehensive content from multiple authoritative sources. Let me compile the full PG-level answer.
Becker's Muscular Dystrophy (BMD) - PG Level Physiotherapy: Assessment & Management
1. DEFINITION
Becker's Muscular Dystrophy (BMD) is an X-linked recessive dystrophinopathy characterised by slowly progressive proximal muscle weakness due to production of a reduced quantity or abnormally sized (truncated), but partially functional dystrophin protein. It is less severe and later-onset than Duchenne Muscular Dystrophy (DMD).
- First described by Becker and Kiener (1955)
- Incidence: ~2.3-5 per 100,000 male births
- BMD accounts for ~15% of all dystrophinopathy variants
- Most BMD patients survive into their 4th-5th decade or longer
2. GENETICS & MOLECULAR PATHOGENESIS
Gene
- Dystrophin gene (DMD gene) - largest known human gene
- Located at Xp21 locus on the short arm of the X chromosome
- Spans >2 million base pairs (>2 Mb), contains 79 exons
- Encodes dystrophin: a large 427 kDa structural protein
Molecular Basis: The Reading Frame Rule
- In BMD: mutations are "in-frame" - maintain the translational reading frame → truncated but partially functional dystrophin is produced
- In DMD: mutations cause "out-of-frame" deletions → frameshifts → premature stop codon → complete absence of dystrophin
- This reading frame difference explains why BMD is clinically milder
- Common mutations: deletions (60%), duplications, point mutations - clustered in 5' half or central region of the gene
Dystrophin-Glycoprotein Complex (DGC)
Dystrophin is the core structural linker protein:
Actin (cytoskeleton) → Dystrophin → Dystroglycans + Sarcoglycans → Basement membrane (laminin)
- DGC provides mechanical stability to myofiber membrane during contraction
- Defective/reduced dystrophin → membrane micro-tears during contraction → uncontrolled Ca²⁺ influx → proteolysis, necrosis → fibrosis and fatty replacement
- DGC is also essential in cardiac myocytes → dilated cardiomyopathy
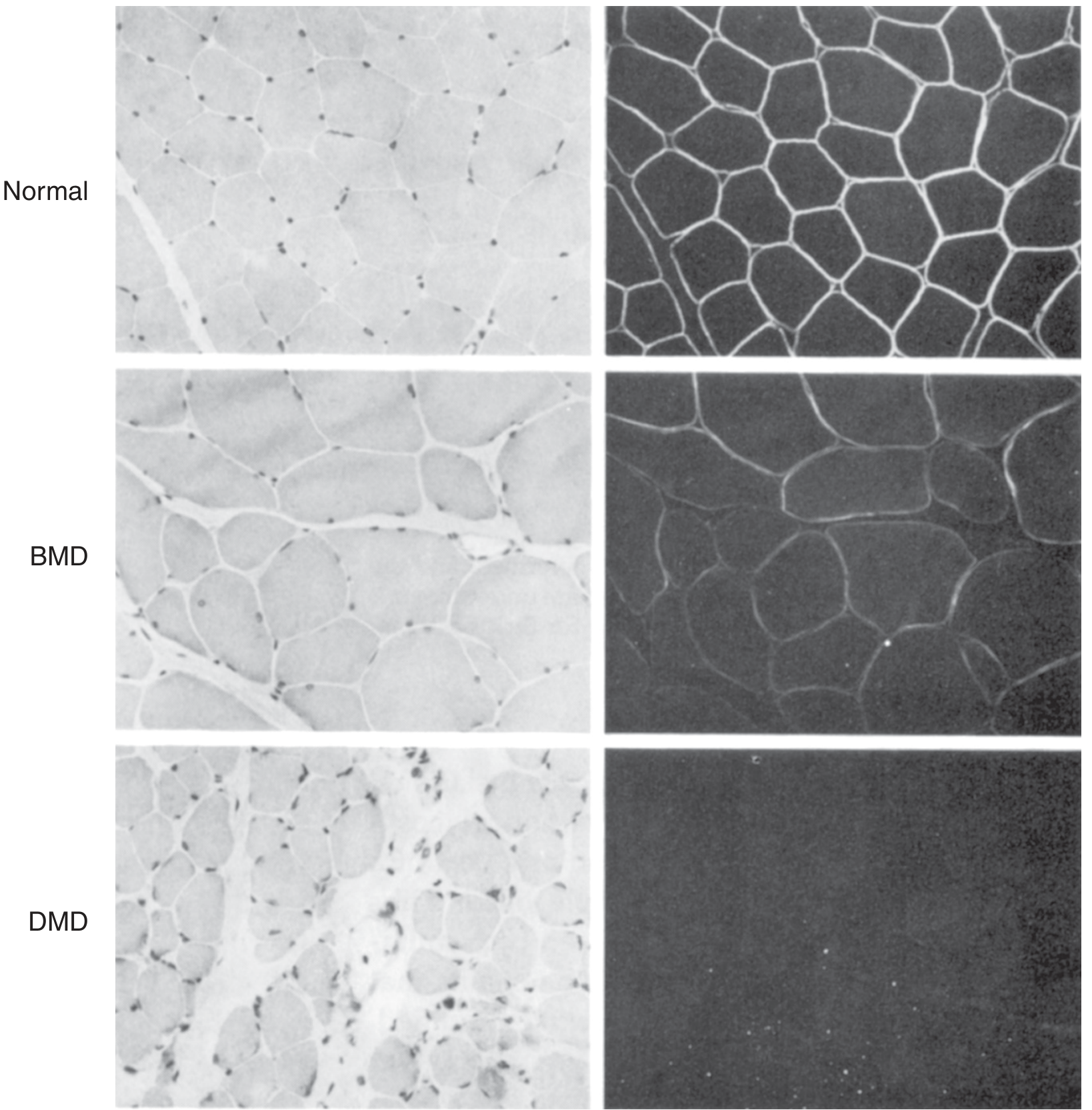
Histology and immunofluorescence: Normal (full membrane dystrophin), BMD (reduced), DMD (absent). Note increased connective tissue in DMD. - Thompson & Thompson Genetics and Genomics in Medicine, 9th Ed.
Inheritance
- X-linked recessive: almost exclusively affects males
- Female carriers: ~70% have elevated CK; ~20% have mild weakness; ~8% develop life-threatening cardiomyopathy (manifesting carriers)
- Reproductive fitness of BMD males is ~70% of normal (vs. DMD which is a genetic lethal)
- Only ~10% of BMD cases are new mutations; most are inherited (contrast with DMD where 1/3 are new mutations)
3. CLINICAL FEATURES
Onset & Natural History
| Feature | BMD | DMD |
|---|---|---|
| Onset | Usually 5-15 years (can be 3rd-4th decade) | <5 years |
| Loss of ambulation | Never before 3rd decade (often maintained much longer) | Early teens |
| Survival | 4th-5th decade or later | 20s-30s (with support) |
| Dystrophin | Reduced/truncated (partially functional) | Absent |
| CK levels | 10-20× normal (often highest before weakness appears) | Very high |
Muscle Involvement
- Proximal muscles predominantly affected, especially lower limbs
- Difficulty climbing stairs, rising from floor, walking up slopes
- Pseudohypertrophy of calves (early and prominent sign) - due to fat/fibrous tissue replacing muscle
- Progressive weakness: hip flexors → hip extensors → shoulder girdle → distal (later)
- Scoliosis is not common (unlike DMD)
- Gowers' sign may be present (though less dramatic than in DMD)
- Toe walking, lumbar lordosis, waddling gait (Trendelenburg gait)
Cardiac Involvement
- Leading cause of death in BMD
- Dilated cardiomyopathy (DCM) - often more severe than skeletal muscle involvement
- Severity of cardiac involvement is independent of skeletal muscle severity
- Some BMD patients present initially with only heart failure (minimal skeletal muscle weakness)
- Right ventricular involvement can be the initial finding → progresses to biventricular DCM
- ECG abnormalities: increased R wave in V1, lateral Q waves
- X-linked dilated cardiomyopathy (XLDCM) is a related allelic condition with predominant cardiac involvement
Respiratory Involvement
- Later and less severe than in DMD, but occurs with disease progression
- Nocturnal hypoventilation → morning headache, fatigue, daytime sleepiness
- Reduced FVC (forced vital capacity); FEV1 decline
- Cough weakness → mucus accumulation → recurrent chest infections
- BiPAP (bilevel positive airway pressure) may be required
Other Features
- Myalgia and cramps (exercise-induced; particularly in early/mild BMD)
- Myoglobinuria (dark urine after exercise) - in ~10-15%
- Intellectual disability: possible but less common than in DMD
- Asymptomatic hyper-CK-emia (can be the only presentation in some)
- Joint contractures: ankle, knee, hip flexors - develop with disease progression
- Pes cavus (in some cases)
4. INVESTIGATIONS
Serum Creatine Kinase (CK)
- 10-20 times normal (can be highest before clinical weakness is apparent)
- First-line screening test
- Lower CK does not exclude BMD but very high CK at presentation is characteristic
Genetic Testing (Gold Standard)
- Multiplex Ligation-dependent Probe Amplification (MLPA) or Next-Generation Sequencing (NGS) from peripheral blood leukocytes
- Detects deletions, duplications, point mutations in the dystrophin gene
- Muscle biopsy is now rarely required when genetic testing is available
Muscle Biopsy (when genetic testing inconclusive)
- H&E: variation in fiber size, fibre necrosis, regeneration, fibrosis, fatty infiltration
- Immunohistochemistry/Immunofluorescence: reduced, irregular, or patchy dystrophin staining at membrane (absent in DMD; normal bright ring in normal muscle)
- Western blot: reduced dystrophin quantity or abnormal size (truncated protein)
EMG/NCS
- Myopathic pattern: short-duration, polyphasic, low-amplitude motor unit potentials
Cardiac Investigations (mandatory at diagnosis)
- 12-lead ECG: Q waves (lateral leads), tall R in V1, conduction abnormalities
- Echocardiography or cardiac MRI: assess LV/RV function, ejection fraction
- Annual monitoring recommended from diagnosis
Respiratory Function Tests
- Spirometry: FVC, FEV1 (FVC <50% predicted = significant impairment)
- Overnight oximetry / polysomnography for nocturnal hypoventilation
- Peak cough flow (PCF): <160 L/min = inadequate cough
5. PHYSIOTHERAPY ASSESSMENT
5a. History Taking
- Age of onset of symptoms; initial presenting complaint (calf enlargement, difficulty running, cramps, myoglobinuria)
- Current functional abilities and limitations
- Falls history; frequency, circumstances, injuries
- Exercise intolerance, fatigue pattern
- Cardiac symptoms: dyspnoea, palpitations, orthopnea, ankle swelling
- Respiratory symptoms: morning headache, daytime sleepiness, recurrent chest infections
- Pain: muscle cramps, joint pain
- Medications: current corticosteroids (deflazacort, prednisolone)
- Psychosocial history: school/work participation, home environment, assistive devices
5b. Musculoskeletal Assessment
Muscle Strength:
- Medical Research Council (MRC) Scale (0-5) for individual muscle groups
- Proximal groups first: hip flexors, extensors, abductors; knee extensors/flexors; shoulder abductors, elbow flexors
- Handheld dynamometry (HHD) for quantitative strength testing
- Myometry for serial monitoring
Range of Motion & Contractures:
- Goniometric measurement of:
- Ankle dorsiflexion (first to become limited - heel cord tightness)
- Hip flexors (Thomas test), knee flexors, ITB (Ober test)
- Shoulder, elbow, wrist
- Identify heel cord contractures, iliotibial band tightness
Postural Assessment:
- Lumbar lordosis (compensatory for weak hip extensors)
- Scoliosis (less common in BMD than DMD)
- Scapular winging, thoracic kyphosis
5c. Functional Assessment
| Test | Purpose |
|---|---|
| Timed Up and Go (TUG) | Mobility and balance |
| 10-Metre Walk Test | Gait speed |
| 6-Minute Walk Test (6MWT) | Exercise capacity and endurance |
| North Star Ambulatory Assessment (NSAA) | DMD/BMD functional motor scale (17 items) |
| 30-Second Chair Stand Test | Lower limb power |
| Gowers' Maneuver timing | Functional lower limb strength |
| Stair climbing test | Functional lower limb strength |
| Performance of Upper Limb (PUL) scale | Upper limb function in non-ambulant patients |
5d. Gait Analysis
- Waddling gait (Trendelenburg) due to weak hip abductors
- Toe walking (shortened Achilles tendon)
- Lumbar hyperlordosis (compensation for weak glutes)
- Reduced stride length, increased base of support
- Increased lateral trunk sway
5e. Respiratory Assessment
- Chest expansion measurement
- Diaphragmatic breathing assessment
- Peak Cough Flow (PCF) - normal >360 L/min; <160 L/min = ineffective cough
- Pulmonary function tests (FVC - lifespan marker; <50% = significant)
- Signs of nocturnal hypoventilation
- Auscultation: basal crepitations, reduced air entry
5f. Cardiac Assessment (Physiotherapy screening)
- Resting heart rate and blood pressure
- Assessment of dyspnoea at rest and with minimal exertion
- Ankle/sacral oedema
- Exercise tolerance modification (adjust intensity per cardiac status)
- Refer to cardiologist if signs of heart failure: ECG, echo, MRI
5g. Outcome Measures Summary
| Domain | Tool |
|---|---|
| Muscle strength | MRC Scale, Handheld dynamometry |
| Functional mobility | NSAA, TUG, 10MWT |
| Exercise capacity | 6MWT |
| Upper limb | PUL 2.0 |
| Respiratory | FVC, PCF, overnight oximetry |
| Pain | NRS/VAS |
| Quality of life | PROMIS, SF-36, PedsQL (paediatric) |
| Falls/balance | BBS, Modified Falls Efficacy Scale |
| Fatigue | Fatigue Severity Scale (FSS) |
6. PHYSIOTHERAPY MANAGEMENT
6a. Goals
- Maintain/prolong functional ambulation
- Prevent or delay joint contractures
- Maintain respiratory function and cough effectiveness
- Preserve upper limb function
- Prevent disuse weakness and secondary deconditioning
- Pain management (cramps, myalgia)
- Optimise quality of life, independence, and participation
6b. Exercise Prescription
Guiding Principles (Medscape/French BMD Guidelines 2023):
- Sessions: twice weekly, 30-45 minutes each
- Avoid high-intensity eccentric contractions (most damaging to dystrophic muscle - causes membrane micro-tears)
- Avoid overwork weakness: muscles scoring <4/5 MRC are at risk from excessive loading
- Promote aerobic metabolism over anaerobic; low to moderate intensity
- Submaximal exercise is safe and beneficial; preserves muscle function and prolongs walking
- Rest between sets; avoid fatigue
i. Aerobic/Cardiovascular Exercise
- Swimming/hydrotherapy: preferred - eliminates gravity, protects joints, allows aerobic exercise with minimal eccentric loading
- Stationary cycling (low resistance)
- Walking at comfortable pace
- Intensity: 40-65% peak VO₂ or RPE 11-13 (Borg 6-20 scale)
- Benefits: cardiovascular fitness, respiratory muscle endurance, mood
ii. Strengthening Exercise
- Low-resistance, high-repetition resistive exercise for muscle groups scoring ≥4/5 MRC
- Avoid maximal eccentric loading (e.g., slow lowering phases with heavy weights)
- Functional strengthening: sit-to-stand, step-ups (modified), supported squats
- Progressive resistance training (submaximal): shown to be safe and beneficial in BMD
- Core strengthening: transversus abdominis, paraspinals (protects lumbar lordosis)
- Upper limb: theraband, light weights for shoulder/elbow muscles
iii. Stretching & Flexibility
- Daily passive/active-assisted stretching of:
- Ankle plantar flexors (Achilles tendon) - most important
- Hip flexors, ITB, hamstrings
- Shoulder girdle, elbow flexors
- Standing programmes: prolonged standing (with or without a standing frame) stretches plantar flexors and maintains bone density
- Hold 30-60 seconds; 3-5 repetitions per muscle group
6c. Contracture Prevention & Management
Priority areas:
- Ankle plantar flexors (most common; leads to toe walking, falls, reduced ambulation)
- Hip flexors and ITB
- Hamstrings (knee flexion contractures)
Methods:
- Daily stretching programme (as above)
- Night splints / Ankle-Foot Orthoses (AFO):
- Worn during sleep to maintain ankle dorsiflexion
- Prescribed early, before significant contracture develops
- Improves foot clearance during gait
- Knee-Ankle-Foot Orthoses (KAFO): for significant knee + ankle contractures; may prolong ambulation
- Serial casting: for established contractures (gentle progressive casting)
- Surgical release (Achilles tendon lengthening ± posterior ankle capsulotomy, ± tibialis posterior transfer) when severe contractures limit ambulation - orthopaedic referral
Orthopaedic management (Campbell's Operative Orthopaedics, 15th Ed.):
"The orthopaedic treatment of Becker muscular dystrophy depends on the severity of the disease. In patients with large amounts of functional dystrophin, orthopaedic procedures are frequently not required until after childhood, and in patients with more severe forms, treatment consideration is the same as for Duchenne muscular dystrophy."
6d. Respiratory Physiotherapy
- Breathing exercises: diaphragmatic breathing, thoracic expansion exercises, pursed lip breathing
- Incentive spirometry: maintains lung volumes, prevents microatelectasis
- Airway clearance techniques:
- Active Cycle of Breathing Technique (ACBT)
- Autogenic drainage
- Percussion and postural drainage (if secretion retention)
- Mechanical Insufflation-Exsufflation (Cough Assist device): indicated when PCF <270 L/min or FVC <50%; generates assisted cough to clear secretions
- Ventilatory support referral:
- BiPAP (non-invasive positive pressure ventilation - NIPPV): for nocturnal hypoventilation (SpO₂ <92% overnight, or symptoms)
- Progresses to full-time NIV in advanced disease
- Annual respiratory review; spirometry 6-12 monthly
6e. Assistive Devices & Orthotics
| Stage | Device |
|---|---|
| Early ambulation | AFOs (ankle-foot orthoses), walking shoes with rigid sole |
| Gait difficulty | Rollator frame, forearm crutches |
| Near loss of ambulation | KAFOs (knee-ankle-foot orthoses) to extend walking |
| Non-ambulant | Powered/manual wheelchair (power preferred for energy conservation) |
| Respiratory | BiPAP, cough assist device |
| Upper limb weakness | Overhead slings, wrist supports, environmental control systems |
| Standing | Standing frame (prolongs stretch, maintains bone density) |
6f. Pain Management
- Cramps and myalgia: common in BMD (more than in DMD)
- Warm-up before exercise; cool-down after
- Heat therapy (warm bath/shower before activity)
- TENS: for pain modulation
- Hydrotherapy (warmth + buoyancy)
- Activity modification: avoid sustained isometric contractions, prolonged walking
- Medication referral: quinine sulfate, magnesium, muscle relaxants (for cramps)
6g. Cardiac Physiotherapy Considerations
- Exercise is safe in BMD patients with mild-moderate cardiac involvement if medically stable
- Avoid isometric exercise and Valsalva maneuver (raises cardiac afterload)
- Monitor heart rate and SpO₂ during exercise; stop if dyspnoea, chest pain, palpitations
- Keep exercise intensity moderate (not maximal)
- Patients on ACE inhibitors/beta-blockers: may have attenuated heart rate response; RPE-based intensity preferred
- Cardiac transplantation: some BMD patients with severe DCM undergo heart transplantation; post-transplant cardiac rehabilitation required
6h. Multidisciplinary Team (MDT) Approach
BMD requires lifelong, coordinated MDT care:
| Specialty | Role |
|---|---|
| Physiotherapist | Exercise prescription, stretching, respiratory PT, orthotics |
| Occupational Therapist | ADL adaptations, assistive devices, home/school modifications |
| Neurologist | Disease monitoring, genetic counselling |
| Cardiologist | ECG, echo, DCM management (ACE inhibitors, beta-blockers) |
| Pulmonologist/Respiratory therapist | Ventilatory support, respiratory monitoring |
| Orthopaedic Surgeon | Contracture release, scoliosis management |
| Dietitian | Nutritional management, obesity prevention (steroid side effects) |
| Neuropsychologist | Cognitive assessment (every 2-3 years in children) |
| Social Worker / Psychologist | Mental health support, school/work reintegration |
| Genetic Counsellor | Family counselling, carrier testing |
7. PHARMACOLOGICAL MANAGEMENT (PT Awareness)
Corticosteroids
- Deflazacort / Prednisolone: evidence-based use (primarily in DMD; role in BMD is debated but used in more severe BMD phenotypes)
- Slows muscle deterioration, preserves ambulation
- PT complications to monitor: weight gain, osteoporosis (→ falls risk, fracture risk), Cushing's features, glucose intolerance, behavioural changes
Cardiac Medications
- ACE inhibitors (perindopril, enalapril): early initiation in BMD (even before symptomatic DCM) slows cardiac deterioration
- Beta-blockers: for established DCM
- Aldosterone antagonists (spironolactone/eplerenone): adjunct
- ICD/CRT: in advanced DCM with arrhythmias
Emerging/Investigational Therapies (2024-2026)
- Exon skipping (antisense oligonucleotides): for specific exon deletion subsets
- Gene therapy (adeno-associated viral vectors expressing mini/microdystrophin): clinical trials ongoing
- Myostatin inhibitors (e.g., apitegromab): aimed at preserving muscle mass
- Edgewise Therapeutics' EDG-5506: targets fast skeletal muscle troponin; Phase 2/3 trials in BMD
8. PHYSIOTHERAPY STAGE-WISE APPROACH
Stage 1 - Ambulatory (Independent Walking)
- Aerobic exercise, submaximal strengthening
- Daily stretching programme (especially Achilles)
- Night AFOs
- Gait training and balance exercises
- Education (energy conservation, activity pacing)
- Annual respiratory review
Stage 2 - Ambulatory with Difficulty (Walking Aids)
- As above + assistive devices (rollators, crutches)
- KAFO assessment to prolong walking
- Increased respiratory physiotherapy
- Hydrotherapy as primary exercise modality
- Referral for contracture surgical review if indicated
Stage 3 - Non-Ambulant (Wheelchair-Dependent)
- Pressure relief and seating assessment
- Postural support (custom wheelchair/seating)
- Upper limb exercise programme (PUL scale monitoring)
- Intensive respiratory physiotherapy + mechanical cough assist
- NIV (BiPAP) initiation
- Prevention of scoliosis (spinal supports)
- Home exercise programme; telerehabilitation (emerging evidence - PMID: 41343252)
Stage 4 - Advanced Disease
- Palliation-focused: comfort, pain management
- NIV optimisation
- Family/caregiver training
- Assistive technology for communication and environment control
9. BMD vs DMD: Key Physiotherapy Differences
| Feature | BMD | DMD |
|---|---|---|
| Age of PT onset | Adolescence/adulthood | Childhood (2-5 yrs) |
| Ambulation loss | >30 years of age | ~12 years |
| Exercise tolerance | Better tolerated | Very limited |
| Cardiac prominence | High (can be the main feature) | Present but overshadowed by skeletal |
| Scoliosis | Uncommon | Common (with loss of ambulation) |
| Corticosteroid role | Less clear evidence | Strong evidence |
| Contractures | Less severe, ankle primarily | Severe, multiple joints |
| Respiratory failure | Later-onset, gradual | Progressive from mid-teens |
10. RECENT EVIDENCE
- Leone E et al. (2024), J Neurol Neurosurg Psychiatry (PMID: 38124127) - Systematic review and meta-analysis of conservative non-pharmacological interventions in muscular dystrophies: supports the role of exercise therapy, respiratory physiotherapy, and stretching in maintaining function
- Vinolo-Gil MJ et al. (2026), Disabil Rehabil (PMID: 41343252) - Telerehabilitation is effective for motor and respiratory function in DMD/BMD; useful for remote delivery of home exercise programmes
- French BMD Working Group Guidelines (Magot A et al., J Neurol. 2023): multidisciplinary evaluation; neuropsychological assessment every 2-3 years in children; annual cardiac ECG + echo; respiratory monitoring; recommendations for physiotherapy in prevention and management of musculoskeletal complications
Key Clinical Pearls for PG Physiotherapy
- Eccentric exercise is the most damaging to dystrophic muscle - always minimise eccentric loading
- Overwork weakness is real - muscles below MRC 4/5 should not be worked to fatigue; submaximal exercise is the rule
- Cardiac involvement can exceed skeletal involvement - always assess cardiac status before exercise prescription in BMD
- Swimming and hydrotherapy are ideal exercise modalities - aerobic, low-eccentric, joint-protective
- Start AFOs early (before contracture is established) - better to prevent than treat heel cord contractures
- PCF <160 L/min = refer for mechanical cough assist device; do not wait for respiratory failure
- Annual respiratory review is mandatory even in mildly affected patients
- Telerehabilitation is emerging as a valid delivery model for BMD home exercise programmes
- Cardioprotection (ACE inhibitors) should begin early in all BMD patients, even before symptomatic DCM
- BMD is never cured - physiotherapy is lifelong and goals shift from performance-based to quality-of-life and function-preservation as disease progresses
Sources: Harrison's Principles of Internal Medicine 22E (2025); Braunwald's Heart Disease 2-Vol Set; Robbins & Kumar Basic Pathology; Campbell's Operative Orthopaedics 15th Ed 2026; Thompson & Thompson Genetics and Genomics in Medicine 9th Ed; French BMD Working Group Guidelines (J Neurol 2023); PubMed meta-analyses (2024-2026)
Give me detailed classification of stroke including all the types & then detailed about circle of willi's - PG level answer with using textbook like Susan B O sullivan
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
I now have comprehensive textbook content. Let me compile the full PG-level answer.
STROKE - Detailed Classification & Circle of Willis
PG Level Physiotherapy Answer
PART 1: CLASSIFICATION OF STROKE
Definition
A stroke (cerebrovascular accident - CVA) is defined as a sudden-onset neurological deficit caused by disruption of blood supply to the brain, either through ischaemia (insufficient blood flow) or haemorrhage (bleeding into or around brain tissue), producing focal brain damage that persists beyond 24 hours. When deficits resolve within 24 hours, it is termed a Transient Ischaemic Attack (TIA).
As noted in Neuroanatomy through Clinical Cases (3rd Ed.): TIAs are "a neurologic emergency akin to acute coronary disease or unstable angina. Approximately 10% of patients with TIAs will have a stroke causing persistent deficits within 3 months, and about half of these strokes occur within the first 48 hours."
MASTER CLASSIFICATION FRAMEWORK
STROKE
├── I. ISCHAEMIC STROKE (~85%)
│ ├── A. Thrombotic
│ │ ├── Large vessel (atherothrombotic)
│ │ └── Small vessel (lacunar)
│ ├── B. Embolic
│ │ ├── Cardioembolic
│ │ └── Artery-to-artery embolism
│ ├── C. Cryptogenic (undetermined cause)
│ └── D. Other determined cause
│ ├── Vasculitis
│ ├── Dissection
│ ├── Hypercoagulable states
│ └── Others
└── II. HAEMORRHAGIC STROKE (~15%)
├── A. Intracerebral Haemorrhage (ICH)
│ ├── Primary (hypertensive / CAA)
│ └── Secondary (AVM, tumour, coagulopathy)
└── B. Subarachnoid Haemorrhage (SAH)
├── Aneurysmal
└── Non-aneurysmal
I. ISCHAEMIC STROKE (~85% of all strokes)
Caused by interruption of blood supply resulting in infarction of brain tissue. Subdivided by the TOAST Classification (Trial of Org 10172 in Acute Stroke Treatment):
A. Thrombotic Stroke
i. Large Vessel (Atherothrombotic) Stroke
- Mechanism: Atherosclerotic plaque formation in large cerebral arteries (ICA, MCA, vertebrobasilar system) → plaque rupture → superimposed thrombus → arterial occlusion
- Common sites: Internal carotid artery (ICA) bifurcation, origin of MCA, vertebral artery origin, basilar artery
- Characteristics: Often preceded by TIAs; stepwise progression; symptoms may fluctuate (stuttering onset); maximal deficit often at onset
- Risk factors: Hypertension, hyperlipidaemia, diabetes mellitus, smoking, age
- Imaging: CT/MRI shows large cortical or subcortical infarct; carotid Doppler, CT angiography confirms stenosis
ii. Small Vessel (Lacunar) Stroke
- Mechanism: Lipohyalinosis or microatheroma in small perforating arteries (<400 µm diameter) supplying deep structures
- Arteries involved: Lenticulostriate arteries (from MCA), thalamoperforating arteries (from PCA/basilar), pontine perforating arteries
- Classic lacunar syndromes (Susan O'Sullivan/Stroke rehabilitation context):
| Syndrome | Location | Deficits |
|---|---|---|
| Pure motor hemiplegia | Posterior limb of internal capsule / pons | Contralateral face, arm, leg weakness; NO sensory loss, no cortical signs |
| Pure sensory stroke | Thalamus (VPL nucleus) | Contralateral hemisensory loss only |
| Sensorimotor stroke | Internal capsule / thalamus junction | Combined weakness + sensory loss |
| Ataxic hemiparesis | Pons or posterior internal capsule | Ipsilateral ataxia + contralateral hemiparesis (disproportionate in leg) |
| Clumsy hand-dysarthria syndrome | Basis pontis / genu internal capsule | Dysarthria + unilateral hand clumsiness |
- Characteristics: No cortical signs (no aphasia, no neglect, no hemianopia); small infarcts <15 mm on MRI; good prognosis with recovery
- Imaging: CT may be normal; MRI DWI shows small deep infarct
B. Embolic Stroke
i. Cardioembolic Stroke
- Mechanism: Thrombus/embolus formed in the heart travels to cerebral arteries → sudden occlusion
- Major cardiac sources:
- Atrial fibrillation (most common; causes 15-20% of all ischaemic strokes)
- Valvular heart disease (mitral stenosis, prosthetic valves)
- Recent MI with mural thrombus
- Dilated cardiomyopathy
- Patent foramen ovale (paradoxical embolism)
- Infective endocarditis
- Left ventricular aneurysm
- Characteristics: Abrupt onset, maximal deficit at onset; often affects multiple vascular territories; haemorrhagic transformation common (emboli fragment, reperfuse infarcted area)
- Preferred territory: MCA (most common embolic target)
ii. Artery-to-Artery Embolism
- Atherosclerotic plaque in proximal artery (e.g., carotid) → thrombus/platelet aggregate → embolises distally
- Common in carotid stenosis (symptomatic amaurosis fugax, retinal artery occlusion, MCA territory TIA)
C. Cryptogenic Stroke
- Ischaemic stroke with no identified cause despite thorough evaluation
- Accounts for 25-30% of ischaemic strokes
- ESUS (Embolic Stroke of Undetermined Source): newer subcategory - non-lacunar, no identified proximal source
D. Stroke of Other Determined Aetiology
| Cause | Details |
|---|---|
| Cerebral venous sinus thrombosis (CVST) | Thrombosis of dural venous sinuses (sagittal sinus most common); presents with headache, papilloedema, focal deficits, seizures |
| Dissection of carotid/vertebral artery | Trauma, spontaneous (connective tissue disorder); intimal tear → intramural haematoma → stenosis/occlusion or embolism; neck pain + Horner's + ipsilateral stroke |
| Vasculitis | Inflammatory narrowing of cerebral vessels (SLE, PAN, primary CNS vasculitis, drug-induced) |
| Hypercoagulable states | Antiphospholipid syndrome, protein C/S deficiency, factor V Leiden, polycythaemia vera |
| CADASIL | Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy; NOTCH3 gene mutation; recurrent lacunar strokes, migraine, dementia |
| Sickle cell disease | Large vessel occlusion in children |
| Drug-induced | Cocaine, amphetamines (haemorrhagic and ischaemic); oral contraceptives (increased thrombosis risk) |
II. HAEMORRHAGIC STROKE (~15% of all strokes)
A. Intracerebral Haemorrhage (ICH) (~10%)
Spontaneous bleeding directly into brain parenchyma.
i. Primary ICH (Hypertensive / CAA)
Hypertensive ICH:
- Mechanism: Chronic hypertension → lipohyalinosis and microaneurysm formation (Charcot-Bouchard aneurysms) in small perforating arteries → rupture
- Classic locations (in order of frequency):
- Putamen (most common - 35%) - lenticulostriate artery rupture
- Thalamus (15%) - thalamoperforating arteries
- Cerebellum (15%) - cerebellar arteries
- Pons (10%) - pontine perforating arteries
- Lobar cortex (20%) - less typical for hypertension; consider CAA
- Clinical features: Sudden severe headache, vomiting, progressive deterioration of consciousness, focal neurological deficit
Cerebral Amyloid Angiopathy (CAA):
- Amyloid-beta deposited in walls of small to medium cortical and leptomeningeal arteries → fragility → rupture
- Location: Lobar (cortical and subcortical) - different from hypertensive ICH
- Common in elderly (>70 years); recurrent lobar haemorrhages; associated with cognitive decline
- MRI gradient echo (GRE)/SWI shows multiple microhaemorrhages (haemosiderin deposits) - "microbleeds"
ii. Secondary ICH
- Arteriovenous malformation (AVM): Abnormal tangle of vessels without capillary bed; high-pressure arterial blood → venous side; most common cause of ICH in young adults (<40 years)
- Intracranial aneurysm rupture: Haemorrhage into parenchyma (rather than subarachnoid space)
- Haemorrhagic transformation of ischaemic infarct: Reperfusion into infarcted tissue → petechial or confluent haemorrhage
- Coagulopathy: Anticoagulant therapy (warfarin, NOACs), haemophilia, thrombocytopenia
- Tumour-related: Primary brain tumours (GBM) or metastases (melanoma, renal cell, choriocarcinoma, thyroid - highly vascular)
- Venous sinus thrombosis: Venous congestion → haemorrhagic infarction
B. Subarachnoid Haemorrhage (SAH) (~5%)
Bleeding into the subarachnoid space (between pia mater and arachnoid mater).
i. Aneurysmal SAH (85% of SAH)
- Cause: Rupture of saccular (berry) aneurysms
- Classic locations:
- Anterior communicating artery (AComm) - most common (30-35%)
- Posterior communicating artery (PComm) - (25-30%) (compresses CN III → ipsilateral fixed dilated pupil)
- MCA bifurcation (20%)
- Basilar tip (10%) - "top of the basilar" aneurysm
- ICA bifurcation, PICA, SCA
- Classic presentation: "Worst headache of my life" (thunderclap headache), sudden onset, meningism, photophobia, vomiting, loss of consciousness
- Complications: Rebleeding (highest in first 24h), vasospasm (days 3-14 → delayed ischaemic deficit), hydrocephalus, hyponatraemia (SIADH/cerebral salt wasting)
- Diagnosis: CT brain (90% sensitive in first 24h) → if negative, lumbar puncture for xanthochromia → CT angiography/conventional angiography
ii. Non-Aneurysmal SAH
- Perimesencephalic SAH: Venous bleed near brainstem; benign prognosis; no aneurysm found
- Vascular malformations: AVM, cavernoma rupture
- Cocaine, sympathomimetics
ADDITIONAL CLASSIFICATION SYSTEMS
By Time Course (Clinical Evolution)
| Type | Duration | Notes |
|---|---|---|
| TIA | <24 h (typically <10 min) | Warning sign; 10% stroke risk in 3 months |
| RIND (Reversible Ischaemic Neurological Deficit) | 24h-3 weeks | Full recovery; older term, less used now |
| Progressing stroke / Stroke-in-evolution | Worsening over hours-days | Active treatment needed; basilar thrombosis classic example |
| Completed stroke | Stable deficits | Rehabilitation focus |
By Anatomy (Vascular Territory)
| Territory | Artery | Key Deficits |
|---|---|---|
| Anterior circulation | ICA, ACA, MCA | Contralateral hemiplegia, hemisensory loss, aphasia (dominant), neglect (non-dominant), hemianopia |
| Posterior circulation | Vertebral, basilar, PCA | Diplopia, dysphagia, dysarthria, ataxia, crossed deficits, vertigo, locked-in syndrome |
By Severity
- NIHSS (National Institutes of Health Stroke Scale): 0 = no stroke; 1-4 = minor; 5-15 = moderate; 16-20 = moderate-severe; 21-42 = severe
- Modified Rankin Scale (mRS): 0-6 scale of functional disability (0 = no symptoms; 6 = death)
- Barthel Index: Functional independence in ADL (0-100)
PART 2: CIRCLE OF WILLIS - DETAILED ANATOMY
The Circle of Willis (Circulus Arteriosus Cerebri) is the principal anastomotic ring at the base of the brain, providing collateral circulation between the anterior and posterior cerebral circulations.
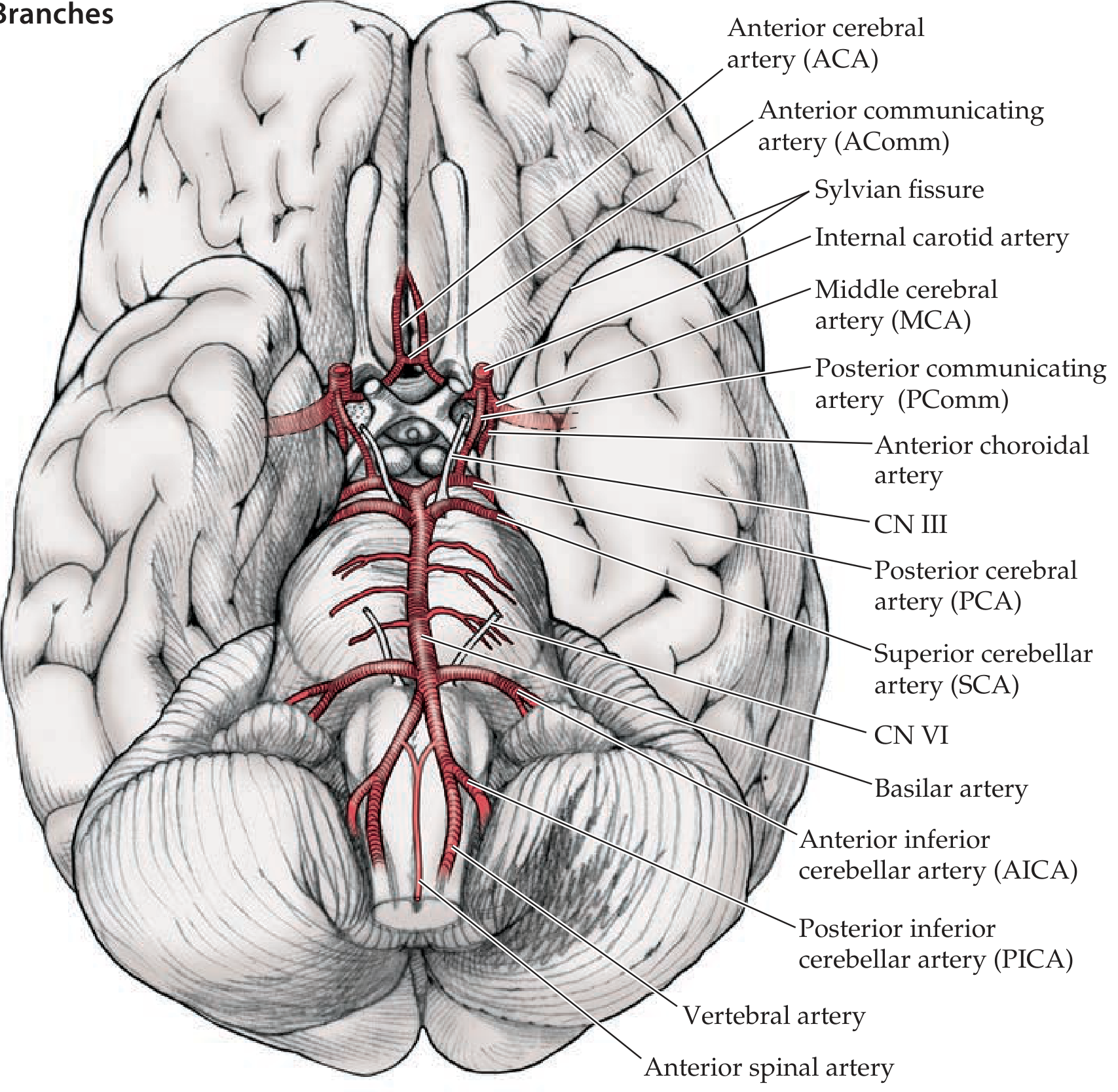
Figure 10.3 - Circle of Willis and Its Main Branches (Inferior view). - Neuroanatomy through Clinical Cases, 3rd Edition
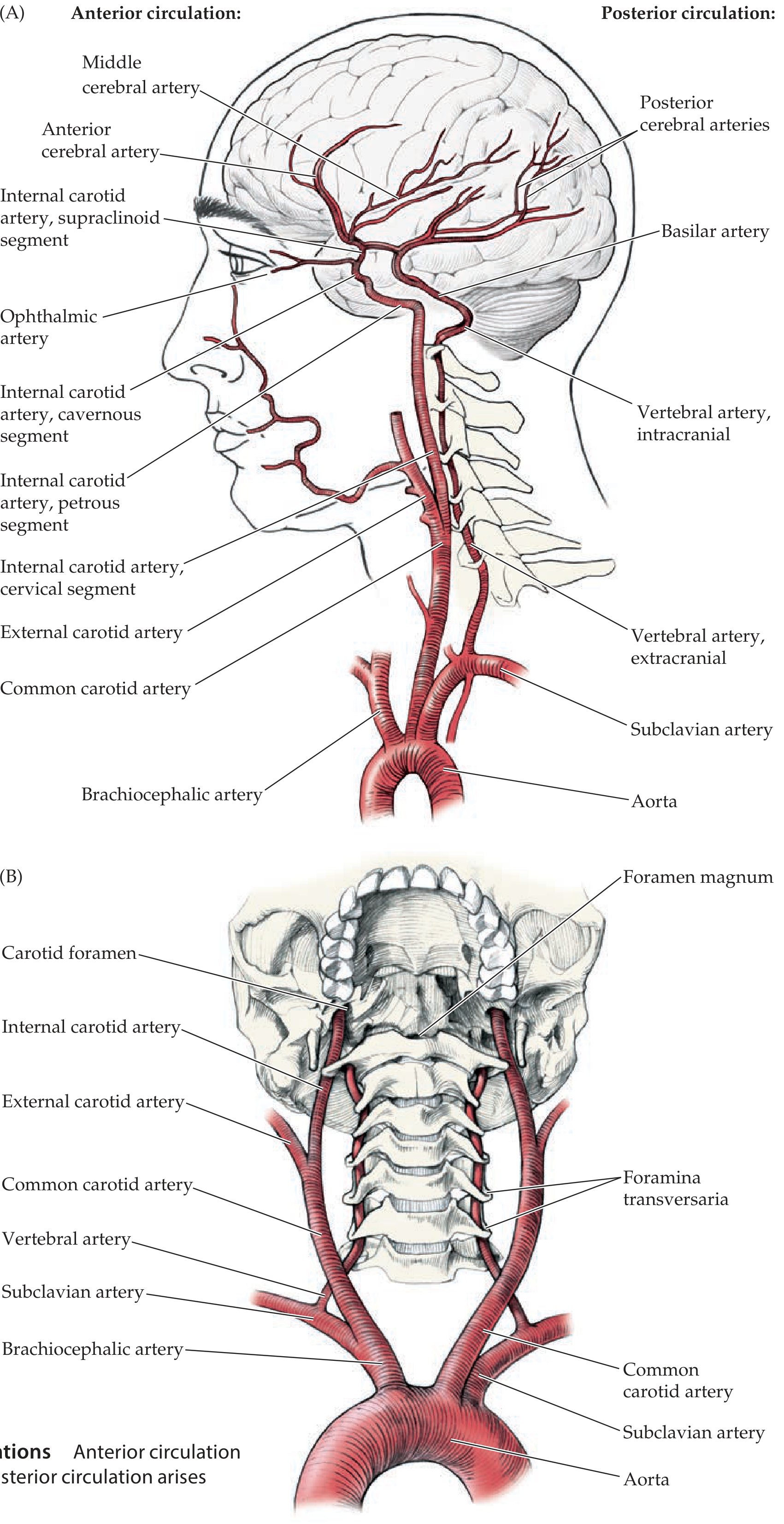
Figure 10.2 - Anterior and Posterior Circulations. Anterior circulation arises from the internal carotid arteries; posterior circulation arises from the vertebral arteries. - Neuroanatomy through Clinical Cases, 3rd Edition
1. LOCATION
- Lies in the interpeduncular cistern at the base of the brain (floor of the cranial vault)
- Surrounds the optic chiasm, pituitary stalk, and hypothalamus
- Sits in the subarachnoid space
- Roughly hexagonal/circular shape when viewed from below
2. COMPONENTS OF THE CIRCLE OF WILLIS
The circle is formed by 9 arterial segments (6 contributing arteries + 3 communicating segments):
ANTERIOR CIRCULATION (Carotid System)
Internal Carotid Artery (ICA) - Supraclinoid Segment (bilateral)
-
Arises from Common Carotid Artery at the carotid bifurcation (C3-C4 level)
-
Segments of ICA (mnemonic: Clean People Can Sit = Cervical → Petrous → Cavernous → Supraclinoid):
- Cervical segment: In neck; no branches
- Petrous segment: Enters carotid canal of temporal bone; horizontal course
- Cavernous segment: S-shaped "carotid siphon" within cavernous sinus
- Supraclinoid (intracranial) segment: Passes anterior clinoid; pierces dura; enters subarachnoid space
-
Main branches of supraclinoid ICA - mnemonic OPAAM:
- Ophthalmic artery
- Posterior communicating artery (PComm)
- Anterior choroidal artery
- Anterior cerebral artery (ACA)
- Middle cerebral artery (MCA)
Anterior Cerebral Artery (ACA) (bilateral)
- Terminal branch of ICA
- Courses anteriorly and medially over the corpus callosum (interhemispheric fissure)
- Segments: A1 (pre-communicating), A2 (post-communicating), A3, A4, A5
- Main branches: Pericallosal artery, Callosomarginal artery
- Territory: Medial surface of frontal and parietal lobes, including the medial sensorimotor cortex (leg area)
- Clinical: ACA infarct → contralateral leg > arm weakness (paraplegia if bilateral)
Anterior Communicating Artery (AComm)
- Connects the two ACAs (A1 segments)
- Short vessel (~2-3 mm); allows cross-circulation between hemispheres
- Most common site of intracranial aneurysm (30-35% of all berry aneurysms)
- Single component; completes the anterior arch of the circle
Middle Cerebral Artery (MCA) (bilateral)
- The largest and most clinically important branch of the ICA
- Turns laterally into the Sylvian (lateral) fissure
- Segments: M1 (horizontal/sphenoidal), M2 (insular), M3 (opercular), M4 (cortical)
- Bifurcates into superior division and inferior division within the Sylvian fissure
- Deep branches (lenticulostriate arteries): Arise from M1 → supply internal capsule, basal ganglia (putamen, caudate head)
- Territory (lateral surface):
- Superior division: Frontal lobe, superior parietal, Rolandic area
- Inferior division: Temporal lobe, inferior parietal (Wernicke's area in dominant hemisphere)
- Clinical: MCA infarct (dominant hemisphere) → contralateral hemiplegia (face + arm > leg), hemisensory loss, hemianopia + aphasia (Broca's if superior, Wernicke's if inferior, global if complete); non-dominant → hemineglect, anosognosia
POSTERIOR COMMUNICATING ARTERY (PComm) (bilateral)
- Arises from ICA (just before its bifurcation)
- Connects ICA to the posterior cerebral artery (PCA) on each side
- Key link between anterior and posterior circulations
- CN III (oculomotor nerve) runs adjacent → PComm aneurysm → ipsilateral CN III palsy (fixed dilated pupil + ptosis + "down and out" eye)
- When PComm is large = "fetal PCA" variant (PCA primarily supplied by ICA, not basilar)
POSTERIOR CIRCULATION (Vertebrobasilar System)
Vertebral Arteries (bilateral)
- Arise from subclavian arteries
- Ascend through foramina transversaria (C6-C1 transverse processes)
- Enter skull through foramen magnum
- Merge at pontomedullary junction to form the basilar artery
- Key branches of vertebral artery:
- PICA (Posterior Inferior Cerebellar Artery): Most important branch; supplies lateral medulla and inferior cerebellum; occlusion → Lateral Medullary (Wallenberg) Syndrome
- Anterior spinal artery (bilateral vertebrals contribute)
- Posterior spinal artery
Basilar Artery
- Formed by union of two vertebral arteries at pontomedullary junction
- Ascends along the ventral pons in the basilar groove
- Branches:
- AICA (Anterior Inferior Cerebellar Artery): Supplies lateral pons + anterior inferior cerebellum; facial nerve nucleus; occlusion → AICA syndrome (facial palsy, ipsilateral hearing loss, ataxia, contralateral sensory loss)
- Pontine perforating arteries: Multiple small arteries supplying basis pontis and tegmentum
- SCA (Superior Cerebellar Artery): Supplies superior cerebellum, lateral tegmentum of upper pons
- Posterior Cerebral Arteries (PCA): Terminal bifurcation of basilar at upper pons/midbrain junction ("top of the basilar")
Posterior Cerebral Artery (PCA) (bilateral)
- Arise as terminal bifurcation of basilar artery (at midbrain-pons junction)
- Connected to ICA via PComm
- Segments: P1 (pre-communicating/mesencephalic), P2 (ambient), P3 (quadrigeminal), P4 (calcarine)
- Deep branches: Thalamoperforating arteries, thalamogeniculate arteries → supply thalamus
- Superficial territory: Occipital lobe (visual cortex), medial temporal lobe (hippocampus), posterior inferior parietal lobe
- Clinical: PCA infarct → contralateral homonymous hemianopia (macular sparing), memory deficits, thalamic pain, alexia without agraphia (left PCA)
3. COMPLETE SCHEMATIC OF THE CIRCLE OF WILLIS
[ACA-L] ——[AComm]—— [ACA-R]
| |
[ICA-L] [ICA-R]
| |
[PComm-L] [PComm-R]
| |
[PCA-L] ←—— [Basilar] ——→ [PCA-R]
|
[VA-L] + [VA-R]
(L = left, R = right; MCA arises from ICA laterally - not part of the ring itself)
The ring structure: ACA (bilateral) → AComm → ICA (bilateral) → PComm (bilateral) → PCA (bilateral) → basilar → vertebrals
4. ANATOMICAL VARIATIONS (Clinically Important)
| Variation | Frequency | Clinical Significance |
|---|---|---|
| Complete full-caliber circle | ~34% only | Most individuals have at least one variant |
| Fetal PCA (PCA arising from ICA via large PComm) | 20-30% | PCA territory at risk with ICA occlusion; protective in basilar disease |
| Hypoplastic A1 segment (one ACA) | 10-15% | AComm aneurysm risk; bilateral ACA territory from one ICA |
| Hypoplastic PComm | 30% | Limits collateral between anterior and posterior circulations |
| Azygos ACA (single midline ACA) | Rare | Bilateral ACA territory infarct with single occlusion |
| Duplicated or fenestrated basilar | Rare | Aneurysm risk |
"A complete full-caliber ring is present in only approximately 34% of individuals." - Neuroanatomy through Clinical Cases, 3rd Ed.
5. DEEP PERFORATING VESSELS FROM THE CIRCLE OF WILLIS
These are critical for understanding lacunar strokes:
| Vessel | Origin | Structures Supplied |
|---|---|---|
| Lenticulostriate arteries (medial + lateral) | M1 segment of MCA | Putamen, globus pallidus, head of caudate, most of internal capsule (posterior limb) |
| Thalamoperforating arteries | P1 segment of PCA (also from basilar tip = "artery of Percheron") | Thalamus (anterior, medial), subthalamus |
| Thalamogeniculate arteries | P2 segment of PCA | Thalamus (ventral posterior, pulvinar) |
| Anterior choroidal artery | ICA (just before bifurcation) | Posterior limb internal capsule, optic tract, medial temporal, choroid plexus |
| Recurrent artery of Heubner | A1-A2 junction of ACA | Head of caudate, anterior internal capsule, anterior putamen |
| Pontine perforating arteries | Basilar artery | Basis pontis, corticospinal/corticobulbar tracts, cranial nerve nuclei |
These small vessels are the ones affected in lacunar infarcts and are the primary targets of lipohyalinosis in hypertension.
6. COLLATERAL CIRCULATION & PHYSIOLOGICAL SIGNIFICANCE
The circle of Willis provides collateral flow when one major vessel is occluded:
- Unilateral ICA occlusion: Flow can reach ipsilateral hemisphere via AComm (from contralateral ICA via ACA) and via PComm (from PCA/basilar)
- Basilar occlusion: Bilateral PCommm arteries can provide retrograde filling to PCA territories from the carotid system
- Subclavian steal syndrome: Proximal subclavian stenosis → reversal of vertebral artery flow to supply arm → posterior circulation ischaemia with arm exercise
- However, collateral effectiveness depends on the completeness of the ring and adequacy of communicating vessel calibre
7. CLINICAL CORRELATIONS (Circle of Willis & Stroke Syndromes)
| Aneurysm Location | Clinical Presentation |
|---|---|
| AComm | Bilateral leg weakness (ACA territory), personality change, abulia, amnesia |
| PComm | CN III palsy (ipsilateral fixed dilated pupil + down-and-out eye), headache |
| MCA bifurcation | Hemiplegia, aphasia or neglect |
| Basilar tip | Bilateral PCA infarcts, quadriplegia, coma, CN III palsy |
| PICA / vertebral | Wallenberg syndrome, ataxia, bulbar symptoms |
PHYSIOTHERAPY RELEVANCE (Susan O'Sullivan Framework)
Stroke Assessment (as per O'Sullivan's Physical Rehabilitation)
Impairment Level (Body Structure/Function):
- Tone assessment (MAS - Modified Ashworth Scale)
- Muscle strength (MRC Scale)
- Sensory testing (light touch, proprioception, pain, temperature)
- Perceptual/cognitive assessment (neglect, apraxia, visuospatial)
- Speech/language screening
- Cranial nerve assessment
- Coordination, balance (Berg Balance Scale)
Activity Level:
- Functional Independence Measure (FIM)
- Barthel Index
- Fugl-Meyer Assessment (motor recovery)
- Wolf Motor Function Test (upper limb)
- 10MWT, 6MWT
Participation Level:
- Modified Rankin Scale
- Quality of life measures
Key Stroke Syndrome → Physiotherapy Implications
| Stroke Site | Deficits | PT Priority |
|---|---|---|
| MCA (dominant) | Hemiplegia (face+arm>leg), aphasia, hemianopia | Communication strategies, UL rehab, gait |
| MCA (non-dominant) | Hemiplegia, neglect, anosognosia | Neglect training, safety awareness |
| ACA | Leg > arm weakness, frontal lobe behaviour | Gait training, balance, behavioural management |
| PCA | Hemianopia, memory, thalamic pain | Visual compensation, pain management |
| Lacunar | Pure motor / pure sensory / ataxic hemiparesis | Targeted motor retraining, balance |
| Brainstem | Cranial nerve deficits, crossed signs, locked-in | Dysphagia, respiratory, communication, positioning |
| Cerebellar | Ataxia, dysmetria, nystagmus | Balance, coordination, vestibular rehab |
QUICK SUMMARY TABLE
| Parameter | Ischaemic (~85%) | ICH (~10%) | SAH (~5%) |
|---|---|---|---|
| Onset | Variable (stepwise/abrupt) | Sudden, progressive | Sudden ("thunderclap headache") |
| Headache | Uncommon | Common (severe) | Severe ("worst of life") |
| LOC | Uncommon | Common | Common |
| CT appearance | Hypodense (>24h) | Hyperdense (acute) | Hyperdense in cisterns |
| Vomiting | Uncommon | Common | Common |
| Meningism | Absent | Absent | Present |
| BP | Variable | Very high | High |
| Treatment | tPA (within 4.5h), thrombectomy | Surgical if large/accessible | Coiling/clipping, nimodipine |
| Prognosis | Varies by territory | Worse than ischaemic | Depends on aneurysm; high early mortality |
Sources: Neuroanatomy through Clinical Cases, 3rd Edition (Blumenfeld); Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine International Edition; Medical Physiology (Boron & Boulpaep); Susan B. O'Sullivan's Physical Rehabilitation framework principles
This is a shared conversation. Sign in to Orris to start your own chat.