Here is a comprehensive overview of Nasopharyngeal Carcinoma (NPC) drawn from multiple authoritative textbooks.
Nasopharyngeal Carcinoma (NPC)
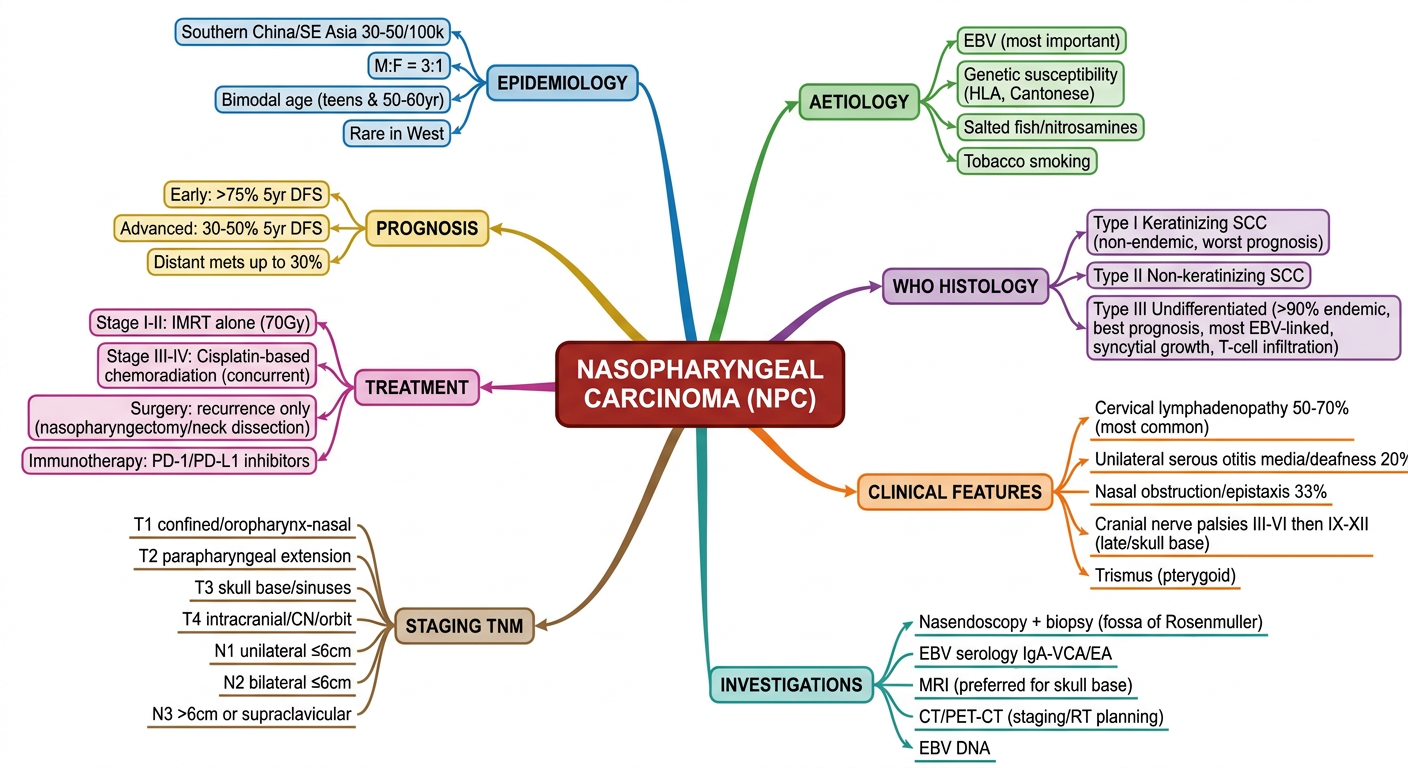
Epidemiology
NPC has a strikingly uneven global distribution. It is rare in most parts of the world (annual incidence ~1 per 100,000), but among southern Chinese (Cantonese) populations the rate rises to 30-50 per 100,000. It also has elevated incidence in Southeast Asia, North Africa, and among Inuit populations. The male-to-female ratio is approximately 3:1. A bimodal age distribution is seen - a peak in teenagers/young adults and again in the 50-60 year age group.
- Bailey and Love's Short Practice of Surgery, p. 805
- Mulholland and Greenfield's Surgery, p. 1999
Aetiology (Multifactorial)
| Factor | Detail |
|---|
| EBV infection | Most important causal factor; EBV genomes found in tumor cells |
| Genetic susceptibility | HLA gene associations; Cantonese/southern Chinese ancestry |
| Diet | Consumption of salted/preserved fish (nitrosamines) |
| Tobacco smoking | Independent risk factor |
EBV infects nasopharyngeal epithelium and, in susceptible individuals, transforms the epithelial cells. The tumor cells express latent membrane protein-1 (LMP1), which activates the NF-kB pathway generating oncogenic signals.
- Robbins & Kumar Basic Pathology, p. (block5)
- Bailey and Love's, p. 805
WHO Histological Classification
| Type | Description | Notes |
|---|
| Type I | Keratinizing squamous cell carcinoma | More common in non-endemic areas; worst prognosis |
| Type II | Non-keratinizing squamous cell carcinoma | Intermediate |
| Type III | Undifferentiated carcinoma | >90% in endemic areas; most common; best prognosis; most strongly EBV-linked |
Type III (undifferentiated) consists of large epithelial cells with indistinct borders ("syncytial" growth), prominent eosinophilic nucleoli, and heavy T-cell infiltration (responding to viral antigens). Rare variants include adenocarcinoma and adenoid cystic carcinoma from minor salivary glands. B- and T-cell lymphomas also occur in the nasopharynx and must be distinguished.
- Robbins & Kumar Basic Pathology
- Mulholland & Greenfield's Surgery, p. 1999
Clinical Features
Symptoms relate to the tumor position and degree of spread. Early symptoms are often minimal, leading to late diagnosis.
~50% of patients present with cervical lymphadenopathy alone - this mandates immediate nasopharyngeal examination.
Presenting Complaints
| Category | Symptoms |
|---|
| Regional | Cervical lymphadenopathy (most common initial presentation) |
| Aural | Unilateral serous otitis media/deafness (~20%) - due to Eustachian tube obstruction |
| Nasal | Obstruction, rhinorrhoea, epistaxis (~1/3 of patients) |
| Neurological | Cranial nerve palsies (III-VI then IX-XII) from skull base invasion - late, poor prognostic sign |
| Other | Trismus (pterygoid muscle involvement) |
Key clinical pearl: Unilateral otitis media in an adult should always prompt nasopharyngoscopy to exclude NPC.
Supraclavicular node involvement (N3 disease) carries a worse prognosis than bulky but lower cervical nodal disease - this is unique to NPC's nodal staging paradigm.
- Bailey and Love's, p. 806
- Mulholland & Greenfield's Surgery, p. 1999
Investigations
- Nasendoscopy + biopsy - flexible or rigid scope; biopsy of fossa of Rosenmüller even if mucosa looks normal; EBV staining of nodes or biopsy specimen is key
- Serology - IgA anti-viral capsid antigen (VCA) antibody and early antigen (EA) antibody; used for mass screening in endemic areas
- MRI (preferred) - for staging skull base, cavernous sinus, cranial foramina, and treatment planning
- CT / PET-CT - for radiotherapy planning, response assessment, detecting recurrence and distant metastases
In ~5% of patients the nasopharynx may appear normal clinically and radiologically, yet biopsy reveals submucosal NPC.
Staging
NPC uses a separate nodal staging paradigm from other head and neck cancers because large-volume cervical nodes alone are less prognostic; what matters is supraclavicular involvement.
Treatment
Primary Treatment: Non-surgical (NPC is highly radiosensitive)
| Stage | Treatment |
|---|
| Stage I-II (Early) | IMRT (Intensity-Modulated Radiotherapy) alone |
| Stage III-IV (Locally advanced) | Concurrent cisplatin-based chemoradiotherapy (CRT) |
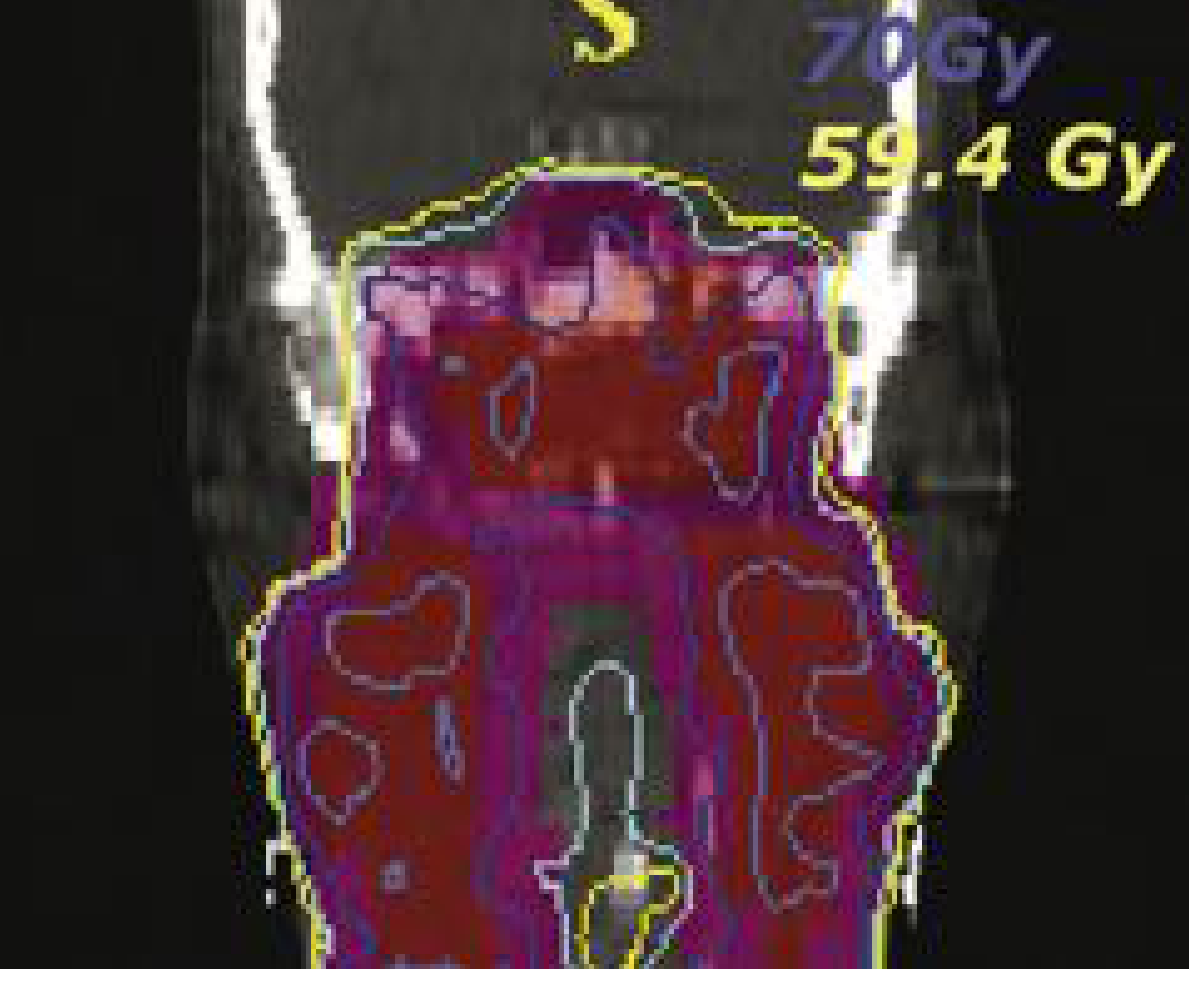
IMRT is now the standard radiation technique - it delivers high conformally shaped doses while sparing critical structures (brainstem, chiasm, parotid glands). Local progression-free rates of 90-97% have been reported.
IMRT plan for T4N2 NPC: the red area = gross tumor volume; magenta = subclinical disease region. The 70-Gy and 59.4-Gy isodose lines conform tightly around target volumes while sparing the parotid glands (mean dose ~28 Gy). - Cummings Otolaryngology
Surgery
Reserved for recurrent or persistent disease only:
- Nasopharyngectomy (transoral robotic, transnasal endoscopic, or open)
- Neck dissection for regional recurrence
Proton beam therapy - promising results with fewer adverse effects in ongoing trials.
Emerging: Immunotherapy
Responses to
immune checkpoint inhibitors (anti-PD-1/PD-L1) have been reported, providing a new strategy for refractory tumors. A
2026 meta-analysis (PMID 41861185) confirmed PD-1/PD-L1 inhibitor benefit in recurrent/metastatic NPC, and a
2025 meta-analysis of toripalimab (PMID 40749515) showed efficacy and safety in NPC specifically.
Prognosis
| Stage | 5-Year Survival |
|---|
| Early disease (I-II) | >75% disease-free survival |
| Advanced disease (III-IV) | 30-50% disease-free survival |
| General (even advanced) | ~50% 5-year OS reported (radiosensitive) |
Distant metastasis rates can reach up to 30% even with IMRT, meaning OS has not dramatically changed with modern RT vs. conventional RT.
- Cummings Otolaryngology, p. 2279
- Bailey and Love's, p. 806
Recent guideline update (2025): The
Lancet Oncology radiotherapy contouring guidelines (PMID 40907526) - a joint CSTRO/CACA/CSCO/HNCIG/ESTRO/ASTRO consensus - updated primary target volume delineation for NPC radiotherapy, reflecting the latest evidence on IMRT field design.