anatomy and physiology of Neuromuscular Junction & neuromuscular transmission with its anaesthetic relevant pharmacology, Factors affecting neuromuscular blockage and monitoring of neuromuscular blockage MD ANAESTHESIA PG EXAM ANSWER
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Miller's Anesthesia and Barash's Clinical Anesthesia. I have everything needed to write a complete MD Anaesthesia PG exam answer. Let me compose the full answer now.
Neuromuscular Junction: Anatomy, Physiology, Anaesthetic Pharmacology, Factors Affecting Blockade & Monitoring
Sources: Miller's Anesthesia 10e (Barash-NMJ p.1156-1184), Barash's Clinical Anesthesia 9e (Ch.21), Goodman & Gilman's Pharmacological Basis of Therapeutics
PART 1: ANATOMY OF THE NEUROMUSCULAR JUNCTION
Structural Components
The NMJ consists of three anatomically distinct zones:
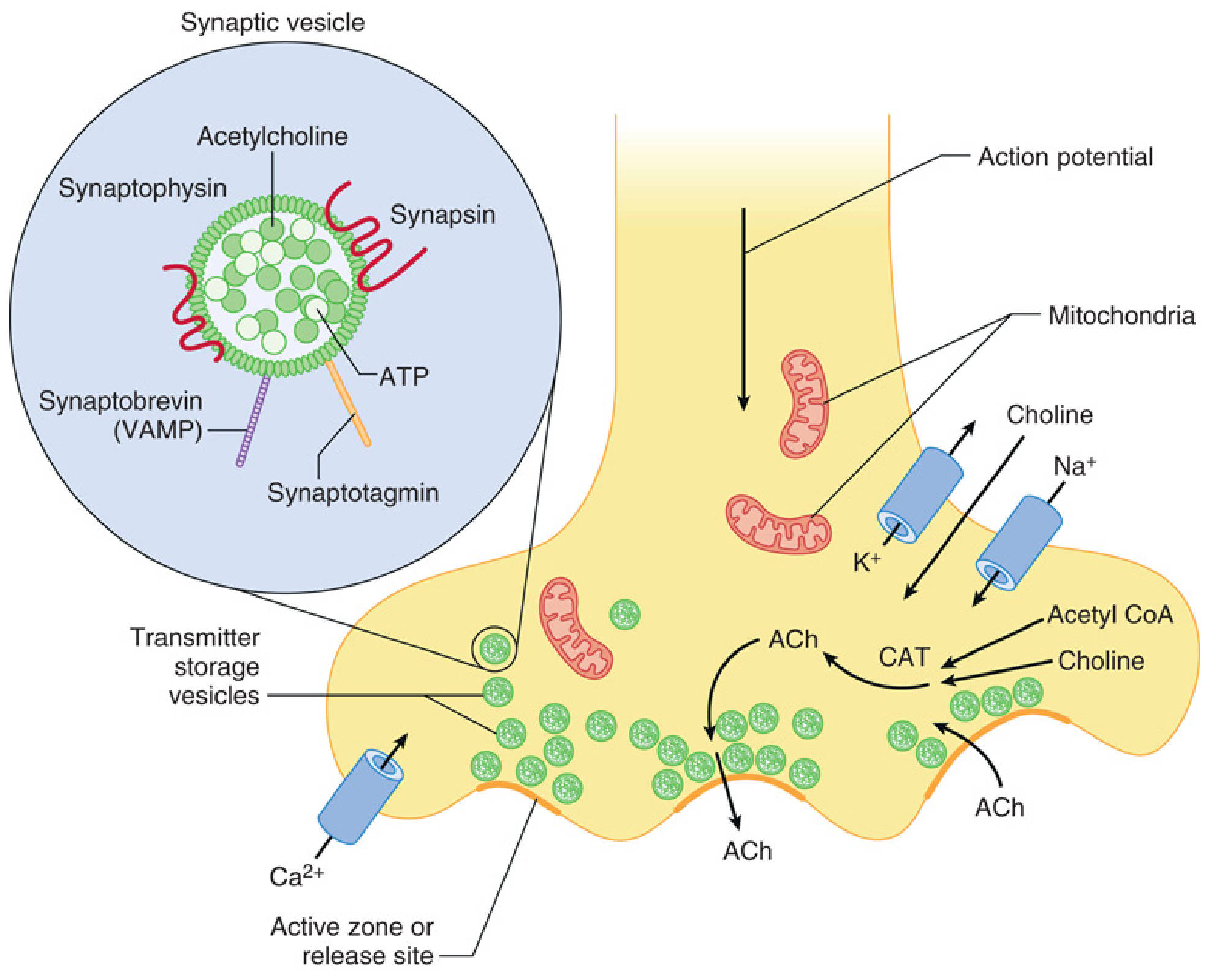
1. Presynaptic (Motor Nerve Terminal)
- The axon of the alpha-motor neuron loses its myelin sheath as it approaches the muscle and terminates in a bulb-shaped nerve ending
- The nerve terminal contains mitochondria (energy supply), choline acetyltransferase (CAT), and numerous synaptic vesicles
- Each vesicle contains approximately 5,000-10,000 molecules of ACh stored as "quanta"
- Vesicle membrane proteins: synaptophysin (glycoprotein), synaptotagmin (Ca2+ sensor), synapsin (vesicular trafficking), synaptobrevin/VAMP (SNARE protein for membrane fusion)
- Voltage-gated Ca2+ channels and K+ channels are present on the presynaptic membrane
- Active zones - specialized release sites directly opposite postjunctional receptor clusters
2. Synaptic Cleft
- Width: 50-70 nm
- Contains acetylcholinesterase (AChE) embedded in the basement membrane - this enzyme rapidly hydrolyzes ACh into choline + acetic acid
- Choline is recycled back into the presynaptic terminal via a sodium-linked active transporter
3. Postsynaptic (Motor End Plate)
- The muscle membrane is thrown into junctional folds (secondary clefts), which increase surface area
- Nicotinic acetylcholine receptors (nAChR) are concentrated at the crests of these folds at high density (~10,000 receptors/µm²)
- Deep in the folds: voltage-gated Na+ channels responsible for propagating the muscle action potential
- The NMJ occupies only 0.1% of the total muscle surface area
PART 2: PHYSIOLOGY OF NEUROMUSCULAR TRANSMISSION
Steps in Neuromuscular Transmission
| Step | Event |
|---|---|
| 1 | Action potential propagates down motor nerve |
| 2 | Depolarization opens voltage-gated Ca2+ channels at active zone |
| 3 | Ca2+ influx triggers vesicle migration, docking (SNARE complex), and exocytosis |
| 4 | ~200 quanta (~1 million ACh molecules) released per nerve impulse |
| 5 | ACh diffuses across 50-70 nm synaptic cleft |
| 6 | ACh binds to both alpha-subunits of nAChR simultaneously |
| 7 | Conformational change opens central ion channel (Na+ in, K+ out, some Ca2+ in) |
| 8 | End-plate potential (EPP) generated (threshold ~-55 mV) |
| 9 | EPP triggers voltage-gated Na+ channels on perijunctional membrane → muscle action potential |
| 10 | Excitation-contraction coupling via T-tubules → Ca2+ release from SR → muscle contraction |
| 11 | AChE rapidly hydrolyzes ACh (lifetime of free ACh ~200 µs) |
The Nicotinic Acetylcholine Receptor (nAChR)
The nAChR is a ligand-gated ion channel made of five protein subunits arranged as a rosette around a central cation pore:
| Feature | Immature (Fetal/Extrajunctional) | Mature (Junctional) |
|---|---|---|
| Subunits | α₁-α₁-β₁-δ-γ | α₁-α₁-β₁-δ-ε |
| Channel open time | 10x longer | Shorter |
| Channel conductance | Lower | Higher |
| Location | Spread over entire muscle | 90% at NMJ |
| Response to depolarizing drugs | Sensitive | Less sensitive |
| Response to non-depolarizing drugs | Resistant | Sensitive |
Key point: Binding of ACh to both alpha subunits is required to open the channel. A nondepolarizing muscle relaxant (NDMR) blocking just one alpha subunit is sufficient to prevent channel opening.
Safety Margin of Neuromuscular Transmission
The NMJ has a remarkable safety margin:
- ACh released (~200 quanta) greatly exceeds the minimum needed
- ~500,000 receptors are activated per nerve impulse
- Only a small fraction of available vesicles/receptors are used per signal
- ~70-80% of receptors must be blocked before any clinical weakness is apparent
- >90-95% must be blocked for complete paralysis (detectable by TOF count = 0)
Miniature End-Plate Potentials (MEPPs)
- Spontaneous, random release of single ACh quanta at rest
- Amplitude ~1/100 of evoked EPP - too small to trigger action potential
- First described by Fatt & Katz (1952) - established the quantal theory of ACh release
Post-Tetanic Potentiation (PTP)
- High-frequency nerve stimulation → Ca2+ accumulates in nerve terminal (enters faster than it can be extruded)
- The nerve terminal is transiently "calcium-loaded" → increased ACh release on subsequent stimuli
- Clinically: after tetanic stimulation during NDMR blockade, the next single twitch is temporarily augmented (post-tetanic count)
PART 3: ANAESTHETIC PHARMACOLOGY OF NEUROMUSCULAR BLOCKING DRUGS
Classification
Neuromuscular Blocking Drugs
├── Depolarizing
│ └── Succinylcholine (suxamethonium)
└── Non-depolarizing (NDMRs)
├── Benzylisoquinoliniums
│ ├── Short: Mivacurium
│ ├── Intermediate: Atracurium, Cisatracurium
│ └── Long: d-Tubocurarine, Pancuronium, Doxacurium
└── Aminosteroids
├── Intermediate: Vecuronium, Rocuronium
└── Long: Pancuronium
A. DEPOLARIZING MUSCLE RELAXANTS - SUCCINYLCHOLINE
Mechanism: Succinylcholine is structurally two ACh molecules joined at their acetyl ends. It acts as an ACh agonist - binds to nAChR, opens channels, and depolarizes the end plate. Unlike ACh, it is not hydrolyzed by AChE, so it persists in the cleft and causes sustained depolarization.
Biphasic Block:
Phase I Block (Depolarizing Block)
- Continuous depolarization keeps perijunctional Na+ channels in the inactivated state (voltage-gated Na+ channels cannot reopen during sustained depolarization)
- Manifests as: initial fasciculations → sustained paralysis
- Characteristics:
- TOF: fade absent (all 4 twitches equally depressed)
- Tetanic stimulation: no fade, no PTP
- Not reversed by anticholinesterases (neostigmine worsens it)
- Potentiated by: volatile agents, prior NDMR administration
Phase II Block (Desensitization Block)
- Occurs with large or repeated doses of succinylcholine (>4-6 mg/kg cumulative)
- The receptor shifts to a "desensitized" state despite depolarization
- Characteristics:
- TOF: fade present (resembles NDMR block)
- Tetanic stimulation: fade present + PTP present
- May be partially reversible with neostigmine
- Mechanism: receptor phosphorylation, ion channel block, receptor desensitization
Pharmacokinetics of Succinylcholine:
- Dose: 1-1.5 mg/kg IV (children: 1.5-2 mg/kg; infants up to 3 mg/kg)
- Onset: 60-90 seconds
- Duration: 5-10 minutes (shortest-acting NMBD)
- Metabolism: rapidly hydrolyzed by plasma (pseudo)cholinesterase (butyrylcholinesterase) in plasma - NOT at the NMJ itself
- Metabolites: succinylmonocholine → succinic acid + choline (inactive)
Dibucaine Number & Pseudocholinesterase Variants:
| Genotype | Dibucaine Number | Incidence | Block Duration |
|---|---|---|---|
| Normal homozygous (Eu/Eu) | 80 | Normal | 5-10 min |
| Heterozygous atypical (Eu/Ea) | 40-60 | 1/480 | 20-30 min |
| Homozygous atypical (Ea/Ea) | ~20 | 1/3200 | 2-3 hours |
- Dibucaine (local anaesthetic) inhibits normal pseudocholinesterase by ~80%, but inhibits atypical enzyme by only ~20%
- Neostigmine also inhibits pseudocholinesterase - avoid succinylcholine immediately after neostigmine
Side Effects of Succinylcholine (Important for Exam):
- Hyperkalaemia - K+ rises ~0.5 mEq/L normally; can be catastrophic in burns (>48h), prolonged immobilization, upper/lower motor neuron injuries, crush injuries (due to upregulated extrajunctional receptors)
- Bradycardia - especially with repeated doses; due to muscarinic receptor stimulation
- Fasciculations - may cause myalgia, increased IOP, ICP, and intragastric pressure
- Malignant hyperthermia - succinylcholine is a potent MH trigger
- Masseter muscle spasm - may herald MH
- Increased IOP - contraindicated in open eye injury
- Anaphylaxis - most common drug cause of anaphylaxis in anaesthesia
B. NON-DEPOLARIZING MUSCLE RELAXANTS (NDMRs)
Mechanism: Competitive antagonists at nAChR - bind to one or both alpha subunits without activating the channel. They compete with ACh for binding. Because antagonist binding increases the square of concentration needed of ACh to maintain activity, doubling the NDMR concentration requires a fourfold increase in ACh concentration.
Presynaptic effects: NDMRs also block presynaptic α3β2 nAChRs, which normally provide positive feedback to enhance ACh mobilization. Blocking these leads to fade on repetitive stimulation - the hallmark of NDMR block.
Characteristics of NDMR Block:
- TOF: fade (T4 < T1, TOF ratio < 1.0)
- Tetanic stimulation: fade + post-tetanic potentiation (PTP)
- Reversed by anticholinesterases (neostigmine, edrophonium, pyridostigmine)
- Reversed by sugammadex (aminosteroid NDMRs only)
Comparison of Key NDMRs:
| Drug | Class | ED95 (mg/kg) | Intubation Dose | Onset | Duration | Elimination |
|---|---|---|---|---|---|---|
| Rocuronium | Aminosteroid | 0.3 | 0.6 mg/kg (RSI: 1.2) | 60-90 s | 30-60 min | Hepatic/biliary |
| Vecuronium | Aminosteroid | 0.05 | 0.1 mg/kg | 3-5 min | 25-40 min | Hepatic (80%), renal (20%) |
| Cisatracurium | Benzylisoquinolinium | 0.05 | 0.15-0.2 mg/kg | 5-7 min | 45-75 min | Hofmann elimination |
| Atracurium | Benzylisoquinolinium | 0.23 | 0.5 mg/kg | 3-5 min | 25-35 min | Hofmann + ester hydrolysis |
| Pancuronium | Aminosteroid | 0.07 | 0.1 mg/kg | 4-6 min | 90-100 min | Renal (80%) |
| Mivacurium | Benzylisoquinolinium | 0.08 | 0.15-0.2 mg/kg | 3-5 min | 12-20 min | Pseudocholinesterase |
Hofmann Elimination: Spontaneous, non-enzymatic degradation at physiological pH and temperature - independent of renal/hepatic function. Atracurium and cisatracurium undergo this route. Laudanosine is a CNS-active metabolite (concern with high-dose atracurium in ICU).
Cardiovascular Effects:
- Pancuronium: vagolytic (tachycardia, hypertension) - blocks muscarinic receptors
- Atracurium: histamine release (hypotension, tachycardia) at rapid/high doses
- Vecuronium, rocuronium, cisatracurium: essentially cardiovascularly neutral
C. REVERSAL AGENTS
Anticholinesterases (Indirect antagonism)
| Drug | Mechanism | Dose | Onset | Duration |
|---|---|---|---|---|
| Neostigmine | Carbamylates AChE (reversible) | 0.04-0.07 mg/kg (max 5 mg) | 7-11 min | 60-90 min |
| Edrophonium | Electrostatic + H-bond to AChE | 0.5-1.0 mg/kg | 1-2 min | 30-60 min |
| Pyridostigmine | Carbamylates AChE | 0.1-0.25 mg/kg | 12-16 min | 90-120 min |
- Must always be given with glycopyrrolate (with neostigmine/pyridostigmine) or atropine (with edrophonium) to prevent muscarinic side effects
- Most effective when TOF ratio >0.1-0.2 (i.e., at least 2-3 twitches present)
- Cannot effectively reverse deep block - must wait for spontaneous partial recovery
- Neostigmine also inhibits pseudocholinesterase → prolongs succinylcholine and mivacurium
Selective Relaxant Binding Agent - Sugammadex
- Modified gamma-cyclodextrin that encapsulates aminosteroid NDMRs (rocuronium > vecuronium >> pancuronium) in a 1:1 complex
- Works at any depth of block - unique advantage over anticholinesterases
- Doses:
- Routine reversal (TOF≥2): 2 mg/kg
- Deep block (PTC 1-2): 4 mg/kg
- Immediate reversal (RSI, 3 min post-rocuronium 1.2 mg/kg): 16 mg/kg
- Does NOT affect muscarinic receptors - no need for anticholinergic pretreatment
- Key interactions: may affect hormonal contraceptives (progestogen binding) - advise alternative contraception for 7 days
PART 4: FACTORS AFFECTING NEUROMUSCULAR BLOCKADE
A. Patient-Related Factors
1. Age
- Neonates/Infants: Higher sensitivity to NDMRs per unit muscle mass but higher volume of distribution → doses on mg/kg basis similar to adults. Succinylcholine dose higher (1.5-2 mg/kg in children, 2-3 mg/kg in infants). Immature nAChRs with gamma subunits resistant to NDMRs but sensitive to depolarizing drugs.
- Elderly: Reduced cardiac output → slower onset. Reduced renal/hepatic function → prolonged duration of renally/hepatically eliminated drugs. Decreased muscle mass.
2. Genetics/Pseudocholinesterase variants (see Dibucaine number above)
3. Neuromuscular Disease
- Myasthenia Gravis: Autoimmune destruction of postjunctional nAChRs → profound sensitivity to NDMRs (reduce dose by 50-75%), resistance to succinylcholine
- Lambert-Eaton Myasthenic Syndrome: Antibodies against presynaptic voltage-gated Ca2+ channels → sensitivity to both NDMRs and depolarizing agents; augmented with repeated stimulation (unlike MG)
- Muscular Dystrophies: Avoid succinylcholine (rhabdomyolysis risk)
- UMN/LMN lesions (>24h): Upregulated extrajunctional receptors → life-threatening hyperkalaemia with succinylcholine; resistance to NDMRs
4. Acid-Base Status
- Respiratory acidosis (↑ pCO2): Potentiates NDMR block, impairs reversal
- Metabolic alkalosis: Potentiates NDMR block
- Metabolic acidosis: Antagonizes some NDMR block
5. Electrolytes
- Hypokalaemia: Potentiates NDMR block (widens resting membrane potential, more negative)
- Hypercalcaemia: Antagonizes NDMR block (increases ACh release)
- Hypocalcaemia: Potentiates NDMR block
- Hypomagnesaemia: Antagonizes (Mg2+ competes with Ca2+ at presynaptic Ca2+ channels → decreases ACh release)
- Hypermagnesaemia: Potentiates NDMR block significantly
- Lithium: Potentiates both depolarizing and non-depolarizing block
6. Temperature
- Hypothermia: Potentiates NDMR block (reduces hepatic/renal metabolism, slows Hofmann elimination, reduces protein binding, shifts ACh quantal content)
7. Burns
- Acute phase (<48h): Sensitive to NDMRs (loss of receptor-rich membrane)
- Post-acute phase (>48h): AVOID succinylcholine (hyperkalaemia from upregulated extrajunctional receptors); resistant to NDMRs
B. Drug Interactions
| Drug Class | Effect on NDMR Block |
|---|---|
| Volatile anaesthetic agents (isoflurane, sevoflurane, desflurane) | Potentiate (enhance end-plate membrane stabilization, possibly presynaptic effects) |
| Aminoglycosides (gentamicin, neomycin) | Potentiate (decrease presynaptic ACh release, stabilize postsynaptic membrane) |
| Polypeptide antibiotics (polymyxin B, colistin) | Potentiate (block ion channels) |
| Tetracyclines | Mildly potentiate |
| Clindamycin, lincomycin | Potentiate (presynaptic ACh release reduction) |
| Local anaesthetics (high dose) | Potentiate (membrane stabilization) |
| Calcium channel blockers (verapamil, nifedipine) | Potentiate (reduce presynaptic Ca2+ entry → reduced ACh release) |
| Beta-blockers (propranolol) | Mild potentiation |
| Lithium | Potentiates both depolarizing and non-depolarizing |
| Furosemide (low dose) | Potentiates |
| Furosemide (high dose) | Antagonizes (via cAMP-mediated increase in ACh release) |
| Phenytoin, carbamazepine (chronic) | Antagonize NDMRs (upregulate ACh receptors) |
| Azathioprine | Antagonizes (mild PDE inhibition) |
| Ecothiopate (organophosphate eye drops) | Prolongs succinylcholine (irreversible AChE inhibition) |
PART 5: MONITORING OF NEUROMUSCULAR BLOCKADE
Why Monitor?
- NDMRs do not alter consciousness - a paralyzed patient may be awake
- Residual paralysis occurs in 30-40% of patients reversed with neostigmine
- Clinical assessment is inadequate: even 5-second head lift can be performed at TOF ratio <0.5
- Guidelines from multiple countries (Canada, France, UK, Australia, Japan, USA) now mandate quantitative monitoring
Nerve Stimulation - Basic Principles
A peripheral nerve stimulator delivers a supramaximal stimulus (20-25% above the threshold to activate all motor fibres in the nerve - typically 40-60 mA for 0.2 ms duration) to a peripheral nerve. The muscle response is measured.
Standard site: Ulnar nerve at wrist → adductor pollicis muscle
- Electrode placement: negative electrode distal, positive electrode proximal
- Alternative sites: facial nerve → orbicularis oculi; peroneal nerve → foot
Patterns of Stimulation
1. Single Twitch (ST)
- Single supramaximal stimulus at 0.1-1 Hz
- Compares response to a baseline (control) twitch
- Can detect 75-80% receptor occupancy before significant depression
- Not useful for monitoring depth of block without a pre-block control
2. Train-of-Four (TOF) - Most Commonly Used
Four successive supramaximal stimuli at 2 Hz (every 0.5s), repeated every 10-12 seconds.
TOF Count (TOFC) - number of twitches visible/palpable:
| TOFC | Approximate Receptor Occupancy | Clinical State |
|---|---|---|
| 0 | >95% | Deep/profound block (excellent intubating/surgical conditions) |
| 1 | ~90% | Deep block |
| 2 | ~85% | Deep block |
| 3 | ~80% | Moderate block |
| 4 (with fade) | ~70-75% | Moderate block |
| 4 (no fade) | <70% | Recovering; need ratio assessment |
TOF Ratio (TOFR) = T4/T1 amplitude ratio:
- Normal = 1.0
- <0.9: Residual paralysis - associated with postoperative respiratory complications
- <0.7: Significant weakness (unable to sustain 5-second head lift in some patients)
- <0.4: Unable to maintain airway, severe hypoventilation
TOF fade occurs because:
- NDMRs block presynaptic α3β2 nAChRs (which normally mobilize ACh vesicles with repetitive stimulation)
- With repeated stimuli, fewer ACh quanta are released → T4 < T3 < T2 < T1
- This presynaptic block is the basis of fade with NDMRs
3. Tetanic Stimulation
- Sustained stimulation at 50 Hz (5 s) or 100 Hz (2 s)
- Sustained tetanus = no residual NDMR blockade
- Fade during tetanus = NDMR block present
- Post-tetanic potentiation (PTP): twitch augmented for 1-2 minutes after tetanic stimulation due to Ca2+ accumulation in nerve terminal
- Should NOT be used repeatedly - painful, can unmask residual block (PTP confounds subsequent TOF)
4. Post-Tetanic Count (PTC)
- Used in deep block when TOF count = 0 and no single twitches visible
- Apply tetanic stimulation (50 Hz, 5s) → wait 3 seconds → count number of single twitches (1 Hz)
- PTC 1-2 = very deep block; PTC 5-10 = deep block recovering; PTC >10 = first TOF twitch about to return
| PTC | Expected TOFC appearance |
|---|---|
| 1-5 | TOF twitch in ~20-40 min |
| 6-10 | TOF twitch in ~10-20 min |
| >15-20 | TOF twitches imminent |
5. Double Burst Stimulation (DBS)
- Two short bursts of 50 Hz tetanic stimulation separated by 750 ms
- DBS₃,₃: 3 pulses at 50 Hz, 750 ms gap, 3 pulses at 50 Hz
- The ratio of second burst to first burst correlates with TOF ratio
- More sensitive than TOF for detecting residual fade by tactile/visual assessment - fade detectable at lower levels of block
- Useful when TOFR is 0.6-0.9 (tactile fade in TOF is unreliable in this range)
Quantitative Monitoring Modalities
| Method | Principle | Cutoff for Extubation |
|---|---|---|
| Mechanomyography (MMG) | Force transducer measures muscle contraction force; gold standard | TOFR ≥ 0.9 |
| Acceleromyography (AMG) | Piezoelectric sensor detects acceleration of thumb; most common clinically | TOFR ≥ 0.9-1.0 (AMG overestimates MMG values) |
| Electromyography (EMG) | Measures compound muscle action potential amplitude | TOFR ≥ 0.9 |
| Kinemyography (KMG) | Piezoelectric sensor detects bending movement | TOFR ≥ 0.9 |
| Phonomyography | Acoustic detection of low-frequency muscle sounds | Investigational |
Key clinical point: AMG values are systematically higher than MMG/EMG values. Therefore, when using non-normalized AMG, the ideal goal is TOFR 0.95-1.0 (not just 0.9) to ensure true adequate recovery.
Differential Muscle Sensitivity to NDMR Block
| Muscle | Sensitivity | Note |
|---|---|---|
| Adductor pollicis (thumb) | Most sensitive | Reference standard for monitoring |
| Corrugator supercilii | Very sensitive | Close to diaphragm resistance pattern |
| Orbicularis oculi | Moderately sensitive | Slightly less sensitive than adductor pollicis |
| Diaphragm | Relatively resistant | 1.5-2x more resistant than adductor pollicis; recovers faster |
| Laryngeal adductors | Moderately resistant | Recovers before adductor pollicis |
| Abdominal muscles | Moderately resistant | Also recover before thumb |
Clinical implication: Even when adductor pollicis TOF count = 0, intubating conditions may be adequate (laryngeal muscles have faster onset and are moderately resistant). However, the adductor pollicis is the best site for assessing safe extubation (it is the most sensitive, last to recover).
Residual Neuromuscular Blockade
- Defined as TOFR < 0.9 at the time of tracheal extubation
- Incidence: ~30-40% with neostigmine reversal alone; ~5% with sugammadex
- Consequences: impaired hypoxic ventilatory response, pharyngeal dysfunction (aspiration risk), upper airway obstruction, critical respiratory events in PACU
- Neither clinical signs nor time from last dose are reliable predictors
- Quantitative monitoring is the only reliable method to rule out residual paralysis
Summary Table: Key Points for MD Anaesthesia Exam
| Topic | Key Fact |
|---|---|
| ACh synthesis | Choline + Acetyl-CoA → ACh via choline acetyltransferase |
| Vesicle release | ~200 quanta (5000 molecules each) per nerve impulse |
| Ca2+ role | Essential for vesicle fusion; doubled Ca2+ = 16-fold increase in quantal content |
| nAChR - mature | α₁α₁β₁δε; requires both α subunits occupied for channel opening |
| nAChR - fetal | α₁α₁β₁δγ; resistant to NDMRs, sensitive to depolarizing drugs |
| Safety margin | 70-80% receptors blocked before clinical weakness; >90-95% for complete block |
| Succinylcholine | Phase I = TOF no fade; Phase II = TOF fade, PTP present |
| NDMR hallmark | TOF fade + PTP = presynaptic mechanism |
| Hofmann elimination | Temperature/pH-dependent, organ-independent (atracurium, cisatracurium) |
| Dibucaine number | Normal >70; Heterozygous 40-60; Homozygous atypical ~20 |
| Sugammadex 16 mg/kg | Immediate reversal 3 min after rocuronium 1.2 mg/kg |
| TOF ratio for extubation | ≥0.9 (MMG/EMG); ≥0.95-1.0 (non-normalized AMG) |
| PTC = 0 | Cannot give sugammadex 4 mg/kg effectively - may need 8 mg/kg or more |
| Most sensitive muscle | Adductor pollicis - best for monitoring safe extubation |
| Most resistant muscle | Diaphragm - resists block, recovers fastest |
| MH triggers | Succinylcholine + volatile halogenated agents |
| Hyperkalaemia risk | Succinylcholine in burns >48h, UMN/LMN lesions, prolonged immobility |
References: Miller's Anesthesia 10e, Chapter 11 (Neuromuscular Physiology and Pharmacology); Barash's Clinical Anesthesia 9e, Chapter 21 (Neuromuscular Blocking Drugs); Goodman & Gilman's Pharmacological Basis of Therapeutics 14e, Chapter 11 (Anti-Cholinesterase Agents)
This is a shared conversation. Sign in to Orris to start your own chat.