Hordeolum
Reading File
Finding Sources
Finding Sources
Searching PubMed
hordeolum stye eyelid treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of Hordeolum (Stye):
Hordeolum (Stye)
Definition & Classification
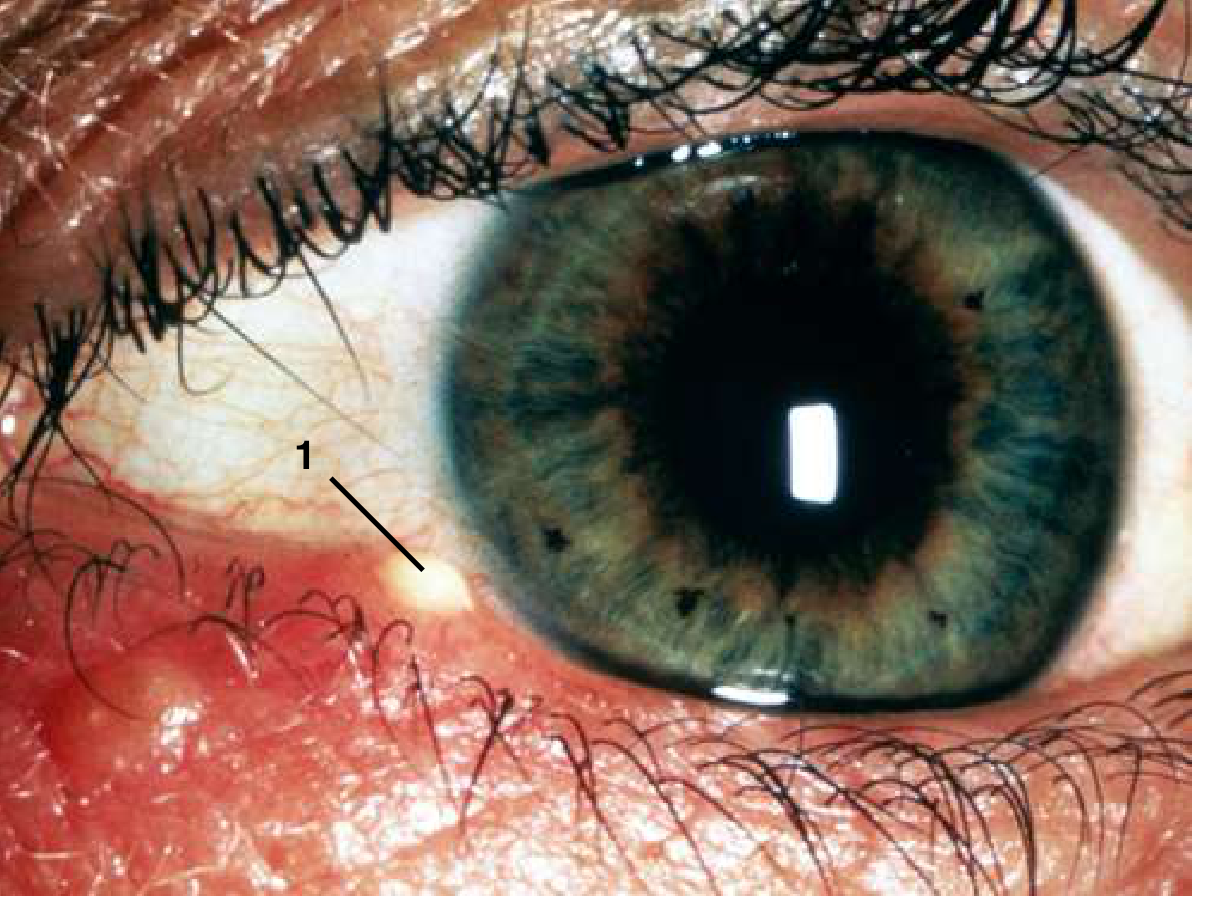
A hordeolum is an acute bacterial abscess of an eyelid gland, classified by anatomic location:
| Type | Gland Involved | Location |
|---|---|---|
| External hordeolum (stye) | Gland of Zeis (sebaceous) or Moll's gland; associated with lash follicle | Points anteriorly through the skin, usually with a lash at apex |
| Internal hordeolum | Meibomian gland | Points toward the palpebral conjunctiva (inner lid surface) |
The causative organism is almost always Staphylococcus aureus; it frequently co-exists with acute blepharitis.
Clinical Features
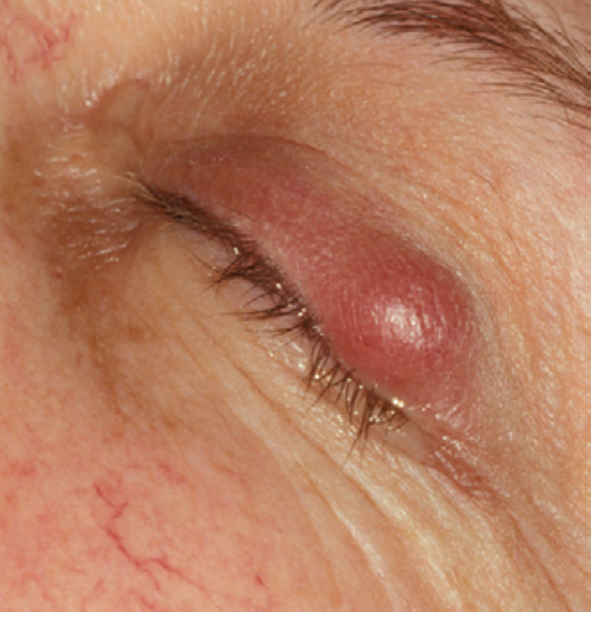
- Acute, tender, erythematous, fluctuant mass at or near the lid margin
- Associated eyelid cellulitis (localized erythema, edema, warmth of surrounding skin) is common
- Spontaneous drainage typically occurs at 5–7 days, often with symptom resolution
- Multiple lesions may be present; entire lid margin may be involved in severe cases
Hordeolum vs. Chalazion
| Feature | Hordeolum | Chalazion |
|---|---|---|
| Nature | Acute bacterial abscess | Chronic granulomatous inflammation (lipogranuloma) |
| Tenderness | Marked | Mild or none |
| Fluctuance | Present (pus) | May have soft center (not true pus) |
| Cellulitis | Common | Rare (mild erythema only) |
| Natural course | Acute, drains in 5–7 days | Chronic, waxes and wanes |
| Location | Lid margin (external) or deeper (internal) | Lid margin or a few mm away |
Key alert: A mass located nasal to the medial canthus suggests dacryocystitis, not hordeolum — refer urgently to ophthalmology (risk of dissection to cavernous sinus).
Differential Diagnosis
- Preseptal (periorbital) cellulitis — diffuse eyelid and periorbital erythema/edema
- Chalazion — chronic, non-infectious, lipogranuloma
- Dacryocystitis — medial canthal swelling, nasal to medial canthus
- Sebaceous carcinoma — suspect in older patients with recurrent/atypical lesions, madarosis, or chronic unilateral blepharitis
- Pyogenic granuloma — benign, deep-red pedunculated lesion often post-hordeolum or post-trauma
Workup
- History: previous eyelid lesions, surgery, trauma, acne rosacea
- External exam: palpate lid for nodule, assess for surrounding cellulitis
- Slit-lamp exam: evaluate meibomian gland orifices, check for madarosis/poliosis (would suggest malignancy)
Treatment
Conservative (first-line)
- Warm compresses ≥10 minutes, 4× daily with gentle massage — promotes spontaneous drainage
- Topical antibiotics: bacitracin, tobramycin, or erythromycin ointment b.i.d. for 1–2 weeks
- Oral antibiotics directed against Staphylococcus (e.g., dicloxacillin, doxycycline) if significant cellulitis is present or lesion fails to point
- Most hordeola resolve with this regimen within 5–7 days
Incision & Drainage (I&D)
Indications:
- Fails conservative management
- Significant pain
- Significant localized pus accumulation
- Associated or previous eyelid cellulitis
Contraindication: Near the lacrimal punctum (nasal to medial canthus) → refer to ophthalmology (risk of lacrimal drainage system damage)
Technique:
- Topical ophthalmic anesthetic drops (e.g., tetracaine) + local infiltration with 2% lidocaine with epinephrine (30-gauge, 3-mL syringe)
- Incise from whichever surface (anterior skin or posterior conjunctiva) provides best access to the pus collection using a no. 11 scalpel blade
- A tongue blade or metal elevator is placed behind the lid to protect the globe; a chalazion clamp may stabilize the lesion
- Express pus, apply direct pressure with gauze for hemostasis (5–10 minutes)
- If significant cellulitis: send pus for culture and sensitivity
- Do not suture skin in acute bacterial infection; consider systemic antibiotics for significant cellulitis
Post-procedure:
- Oral anti-staphylococcal antibiotic
- Daily follow-up until cellulitis resolves and pus is not reaccumulating
- Reassess at 2–3 weeks (swelling may persist for several weeks)
Complications
- Preseptal cellulitis — most common complication; treat as per cellulitis protocol
- Spread of infection — rare
- Lacrimal drainage system damage — if I&D performed near medial canthus
- Recurrence — associated with chronic blepharitis or acne rosacea; consider chronic low-dose doxycycline (20–50 mg/day) for recurrent cases
Key Points
- Hordeolum = acute staphylococcal abscess of an eyelid gland; chalazion = chronic lipogranuloma
- Most respond to warm compresses + topical antibiotics within a week
- I&D is reserved for failure, significant pain, or cellulitis
- Always exclude sebaceous carcinoma in recurrent or atypical cases (send specimens to pathology)
- Medial canthal lesions → refer, do not drain (dacryocystitis risk; cavernous sinus spread)
Sources: Wills Eye Manual 6th ed.; Goldman-Cecil Medicine; Pfenninger & Fowler's Procedures for Primary Care 3rd ed.; Kanski's Clinical Ophthalmology 10th ed.
This is a shared conversation. Sign in to Orris to start your own chat.