Management of Acute Cholelicycteticcholilethisasis
Reading File
Finding Sources
Searching PubMed
"acute cholecystitis" AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have excellent comprehensive content from multiple authoritative surgical and gastroenterology textbooks. I have enough to compose a thorough, well-structured response.
Management of Acute Calculous Cholecystitis
Acute calculous cholecystitis (ACC) — gallstone-induced gallbladder inflammation — results from cystic duct obstruction by a gallstone in >90% of cases, followed by distension, ischemia, bacterial overgrowth, and, if untreated, gangrene or perforation.
1. Diagnosis
Clinical Features
- RUQ or epigastric pain (constant, >6 hours), fever, nausea/vomiting
- Murphy's sign: inspiratory arrest on deep palpation of the RUQ (sonographic Murphy's sign is operator-dependent)
- Leukocytosis; mild elevations of ALP, bilirubin, and transaminases
- Profound jaundice is rare — if present, suspect cholangitis or Mirizzi syndrome
Imaging
| Modality | Sensitivity | Specificity | Role |
|---|---|---|---|
| RUQ Ultrasound (first choice) | 85–94% | 78–95% | Gallstones, wall thickening (>4 mm), pericholecystic fluid, sonographic Murphy's sign |
| HIDA scan | 96% | 90% | Non-filling of gallbladder = cystic duct obstruction; gold standard when US inconclusive |
| CT abdomen | High | High | Emphysematous cholecystitis, perforation, pericholecystic abscess, peritonitis |
| MRI/MRCP | High | High | Reserved for suspected choledocholithiasis or malignancy |
RUQ ultrasound is the diagnostic test of choice. CT is recommended when emphysematous cholecystitis or complications are suspected. — Sabiston Textbook of Surgery
2. Tokyo Guidelines 2018 (TG18) — Severity Grading
The TG18 framework is the most widely used system for risk-stratifying patients and guiding treatment:
| Grade | Severity | Criteria |
|---|---|---|
| Grade I (Mild) | No organ dysfunction; mild inflammation | Uncomplicated; manageable with standard care |
| Grade II (Moderate) | Marked local inflammation | WBC >18,000/mm³; symptom duration >72 h; palpable tender mass; marked pericholecystic inflammation on imaging; no organ dysfunction |
| Grade III (Severe) | Organ dysfunction | Cardiovascular (hypotension requiring vasopressors), neurological (decreased consciousness), respiratory (PaO₂/FiO₂ <300), renal (oliguria, Cr >2.0), hepatic (PT-INR >1.5), hematologic (platelet <100,000/mm³) |
The AAST EGS grading (Grades I–V) runs parallel to TG18, with Grade V denoting pericholecystic abscess, bilioenteric fistula, and peritonitis. — Sabiston Textbook of Surgery
3. Initial Resuscitation and Supportive Care
All patients require:
- IV fluid resuscitation — restore perfusion and electrolyte balance
- NPO (nothing by mouth)
- Parenteral analgesia (narcotics for pain control)
- IV antibiotics — bile cultures positive in >40% of patients
Antibiotic Selection
- Mild–moderate (Grade I–II): Cefoxitin (2nd-gen cephalosporin) or ampicillin-sulbactam
- Severe (Grade III) or broad-spectrum needed: Piperacillin-tazobactam or 3rd-generation cephalosporin + metronidazole
- Emphysematous/gangrenous cholecystitis: Must cover anaerobes (metronidazole or piperacillin-tazobactam)
- Organisms targeted: E. coli, Klebsiella, Enterobacter, Proteus (gram-negative enteric bacilli); Enterococcus, Streptococcus (gram-positive); anaerobes (~15% of isolates); Clostridium in emphysematous disease
If source control is achieved with surgery, postoperative antibiotics are NOT indicated for mild-to-moderate cholecystitis. Continue antibiotics postoperatively for severe infection, intraoperative gallbladder perforation, or gangrenous cholecystitis. — Sleisenger & Fordtran's GI and Liver Disease
4. Definitive Treatment: Cholecystectomy
Timing: Early vs. Delayed
Multiple RCTs have definitively resolved the old debate. Early laparoscopic cholecystectomy (within 72 hours of presentation) is the standard of care for surgically fit patients.
| Outcome | Early Cholecystectomy | Delayed (6–8 weeks) |
|---|---|---|
| Mortality | 0% | 2.0% |
| Total hospital stay | 9.6 days | 17.8 days |
| Failure requiring urgent surgery | N/A | 26% |
| Bile duct injuries | 0 | 0 |
Combined results from 7 randomized trials (n=742). — Sleisenger & Fordtran's GI and Liver Disease, p. 1263
Key insight: With delayed surgery, 26% of patients deteriorated and required urgent unplanned operation — the worst surgical scenario.
Surgical Approach
- Laparoscopic cholecystectomy is feasible in most cases and is the procedure of choice
- If severe inflammation obscures the hepatocystic triangle: laparoscopic subtotal fenestrating cholecystectomy or conversion to open
- Intraoperative cholangiography is especially valuable in acute cholecystitis to confirm ductal anatomy and detect CBD stones
- Routine placement of surgical drainage catheters after laparoscopic cholecystectomy is not warranted and may be harmful
Management Algorithm (Mulholland & Greenfield's Surgery, Algorithm 8.2)
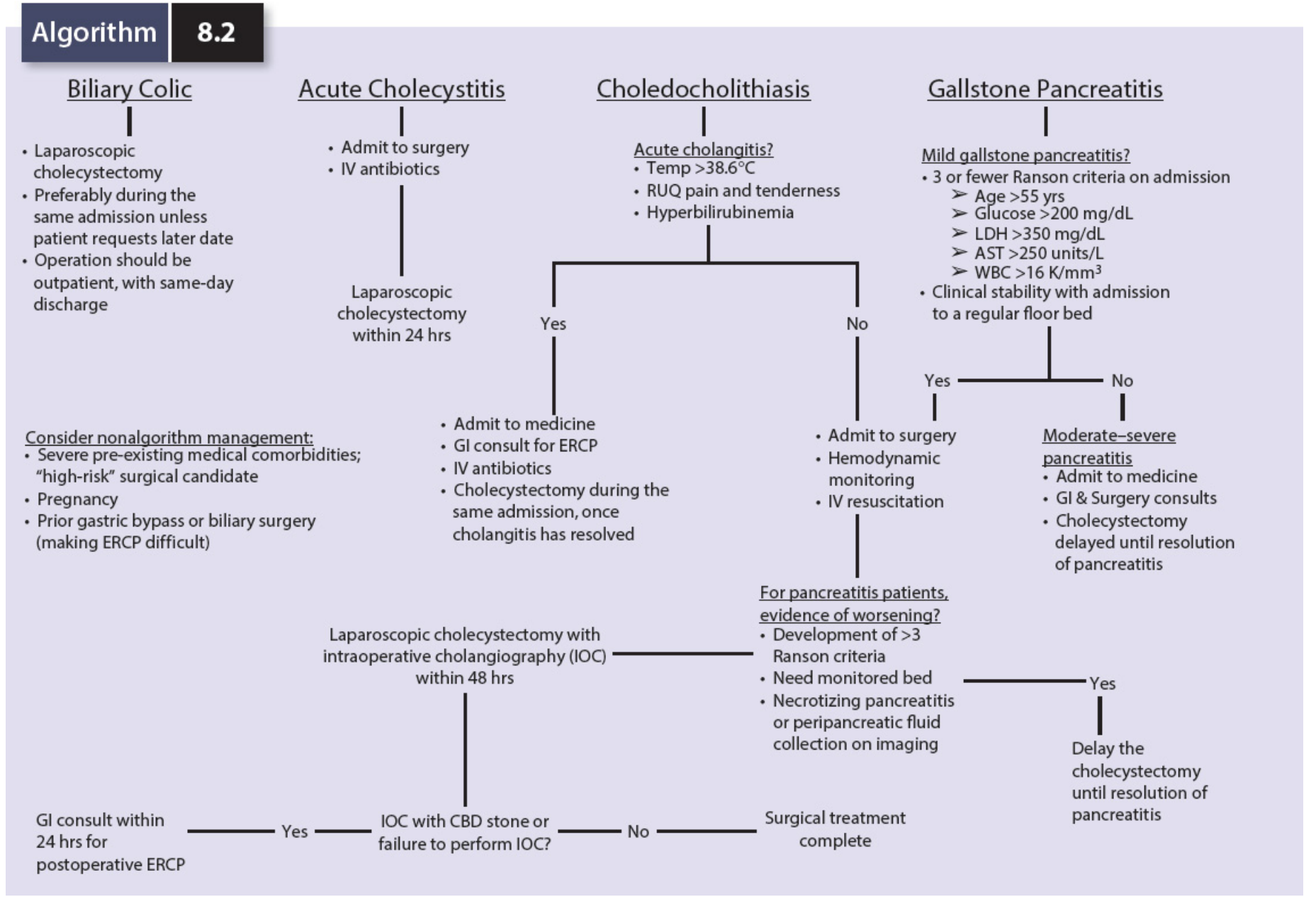
Algorithm 8.2: For acute cholecystitis — admit to surgery, start IV antibiotics, laparoscopic cholecystectomy within 24 hours (or within 48 hrs if concurrent cholangitis requiring ERCP first). From Mulholland & Greenfield's Surgery, 7e.
5. Non-Surgical Options for High-Risk Patients
When the patient is not a surgical candidate (severe comorbidities: cardiac, hepatic, pulmonary failure):
Percutaneous Cholecystostomy (PC)
- Gallbladder drainage performed under ultrasound or fluoroscopic guidance
- TG18 recommends PC for Grade II–III cholecystitis in high-surgical-risk patients failing antibiotics and supportive care
- Earlier TG versions specified: Grade II with symptoms >72 h failing antibiotics, OR any Grade III
- 30-day mortality after PC: 9–21% (reflecting the severity of underlying illness)
- Residual stones can be removed via the tube; however, ~50% of patients develop recurrent biliary symptoms
- After recovery, interval laparoscopic cholecystectomy should be performed if the patient's condition permits
Endoscopic Transmural Gallbladder Drainage
- EUS-guided endoluminal stent from gallbladder to duodenum (EUS-GBD)
- As effective as percutaneous drainage for decompression in non-surgical patients
- Caveat: If future surgery becomes possible, it requires additional repair of the duodenotomy site — so it is reserved for patients who will definitively remain non-surgical candidates
6. Special Populations
| Population | Key Consideration |
|---|---|
| Diabetic patients | Higher risk of sepsis, empyema, gangrene → perform cholecystectomy expeditiously |
| Elderly patients | Deceptively benign presentation; high rates of occult gangrene and empyema → early cholecystectomy warranted |
| Pregnancy | Laparoscopic cholecystectomy is safe and preferred over non-operative management (recent 2025 meta-analysis, PMID 40610639) |
| Gangrenous/emphysematous cholecystitis | Risk factors: male sex, DM, cardiovascular disease, WBC >15,000/mm³ → add anaerobic coverage; urgent surgery |
7. Complications to Recognize and Manage
| Complication | Features | Management |
|---|---|---|
| Gangrenous cholecystitis | Necrosis of gallbladder wall; high WBC, DM, male sex, CV disease | Urgent cholecystectomy + anaerobic antibiotics |
| Emphysematous cholecystitis | Gas in gallbladder wall on CT; Clostridium species | Urgent surgery; clostridial coverage |
| Perforation / pericholecystic abscess | Peritoneal signs, CT confirms | Urgent surgery or PC + antibiotics |
| Mirizzi syndrome | Stone in cystic duct/Hartmann's pouch compressing common hepatic duct → jaundice | MRCP; surgical biliary reconstruction |
| Empyema | Pus-filled gallbladder; spiking fevers, severe illness | Urgent cholecystectomy or PC drainage |
8. Summary Algorithm
Acute Calculous Cholecystitis Confirmed
↓
IV fluids + NPO + Analgesia + IV Antibiotics
↓
Assess Severity (TG18 Grade I / II / III)
+ Surgical Risk (ASA / comorbidities)
↓
┌─────────────────────────────────┐
│ Grade I–II, Low surgical risk │ → Early Laparoscopic Cholecystectomy
│ │ (within 72 hours, ideally 24–48 h)
└─────────────────────────────────┘
↓
┌─────────────────────────────────────────┐
│ Grade II–III, High surgical risk │ → Percutaneous Cholecystostomy
│ (organ failure, severe comorbidities) │ + Antibiotics
└─────────────────────────────────────────┘
↓ (after recovery)
Interval Laparoscopic Cholecystectomy
(if patient becomes operative candidate)
Key Sources:
- Sleisenger & Fordtran's GI and Liver Disease, Ch. 90, p. 1263
- Sabiston Textbook of Surgery, Ch. Biliary, pp. 1824–1831
- Mulholland & Greenfield's Surgery, 7e, pp. 461–462
- Current Surgical Therapy, 14e, pp. 510–511
- Tokyo Guidelines 2018 (TG18)
Recent Evidence Note: A 2025 systematic review (PMID 40610639) confirms operative management is preferred over non-operative treatment for acute cholecystitis in pregnancy. A 2024 meta-analysis (PMID 38758253) found CT has comparable diagnostic accuracy to ultrasound but US remains first-line due to cost, availability, and radiation avoidance.
This is a shared conversation. Sign in to Orris to start your own chat.