Hey tell me about chronic bronchitis from basics to clinical
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chronic bronchitis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive, rich information from multiple authoritative sources. Let me compile the full clinical response.
Chronic Bronchitis: From Basics to Clinical
1. Definition
Chronic bronchitis is defined clinically - not anatomically - as a persistent productive cough for at least 3 consecutive months in at least 2 consecutive years, in the absence of any other identifiable cause (e.g., bronchiectasis, TB, malignancy).
This is in direct contrast to emphysema, which is defined anatomically (alveolar wall destruction). A patient can have chronic bronchitis with or without airflow obstruction - when airflow obstruction co-exists, it falls under the COPD umbrella.
- Robbins & Kumar Basic Pathology
- Goldman-Cecil Medicine
2. Epidemiology & Risk Factors
-
Predominantly a disease of smokers - ~90% of affected patients have a significant smoking history, often 40+ pack-years
-
Affects adults, typically presenting in the 6th decade or later
-
Other exposures: biomass fuel combustion (poorly ventilated spaces), occupational dusts (grain, cotton, silica mines), sulfur dioxide, nitrogen dioxide air pollutants
-
In the US, COPD (the umbrella that includes CB with obstruction) costs approximately $50 billion annually in direct and indirect costs
-
Globally, COPD causes ~3.2 million deaths/year (3rd leading cause of death worldwide)
-
Up to 30% of the community smokes, but chronic bronchitis is only reported in ~5% of patients seeking medical care for cough
-
Goldman-Cecil Medicine
-
Murray & Nadel's Textbook of Respiratory Medicine
3. Pathogenesis
The central defect is mucus hypersecretion, driven by several interacting mechanisms:
3a. Mucus Hypersecretion
- Cigarette smoke and air pollutants trigger hypertrophy of mucous glands in the trachea and large bronchi
- Goblet cell hyperplasia in small airways (bronchi and bronchioles)
- The enlargement of submucosal glands and increase in goblet cells may represent a protective/adaptive response that becomes maladaptive
- Inflammatory mediators, particularly IL-13 from T cells and histamine, drive mucin expression
- Neutrophil elastase production is also increased by tobacco smoke exposure
3b. Acquired CFTR Dysfunction
- Smoking leads to acquired CFTR dysfunction, causing secretion of abnormal, dehydrated mucus - exacerbating severity (this is a key insight from Robbins Cotran, linking CB mechanistically to CF-like pathology)
3c. Inflammation
- Cellular damage from inhaled irritants elicits neutrophils, macrophages, and lymphocytes
- Note: eosinophils are NOT prominently seen (distinguishes from asthma)
- Long-standing airway inflammation + fibrosis in small airways leads to chronic obstruction
3d. Role of Infection
- Infection does not initiate chronic bronchitis
- However, it is critical in maintaining inflammation and precipitating acute exacerbations
- Common pathogens: Haemophilus influenzae, Moraxella catarrhalis, Streptococcus pneumoniae
3e. Airflow Obstruction Mechanism
-
Large airway changes (mucous gland hypertrophy) cause the sputum production
-
Airflow obstruction, however, results from small airway disease (chronic bronchiolitis): mucous plugging + inflammation + bronchiolar wall fibrosis in airways <2-3 mm diameter
-
Ciliary dysfunction from smoke prevents mucociliary clearance, perpetuating the cycle
-
Robbins & Kumar Basic Pathology
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
4. Morphology / Pathology
Gross Findings
- Mucosal lining of large airways is hyperemic, edematous, swollen
- Covered by a layer of mucinous or mucopurulent secretions
- Smaller bronchi and bronchioles may be filled with secretion casts
Microscopic Findings
The hallmark is enlargement of mucus-secreting submucosal glands:
| Feature | Detail |
|---|---|
| Reid Index | Ratio of mucous gland layer thickness to bronchial wall thickness (epithelium to cartilage). Normal = 0.4. Elevated in CB, correlating with severity and duration |
| Goblet cell metaplasia/hyperplasia | In small airways |
| Inflammatory infiltrate | Lymphocytes, macrophages, some neutrophils |
| Smooth muscle hypertrophy | Bronchiolar wall thickening |
| Peribronchial fibrosis | Leads to luminal narrowing |
| Squamous metaplasia/dysplasia | From mutagenic effects of tobacco smoke |
| Bronchiolitis obliterans | Severe cases - complete luminal obliteration by fibrosis |
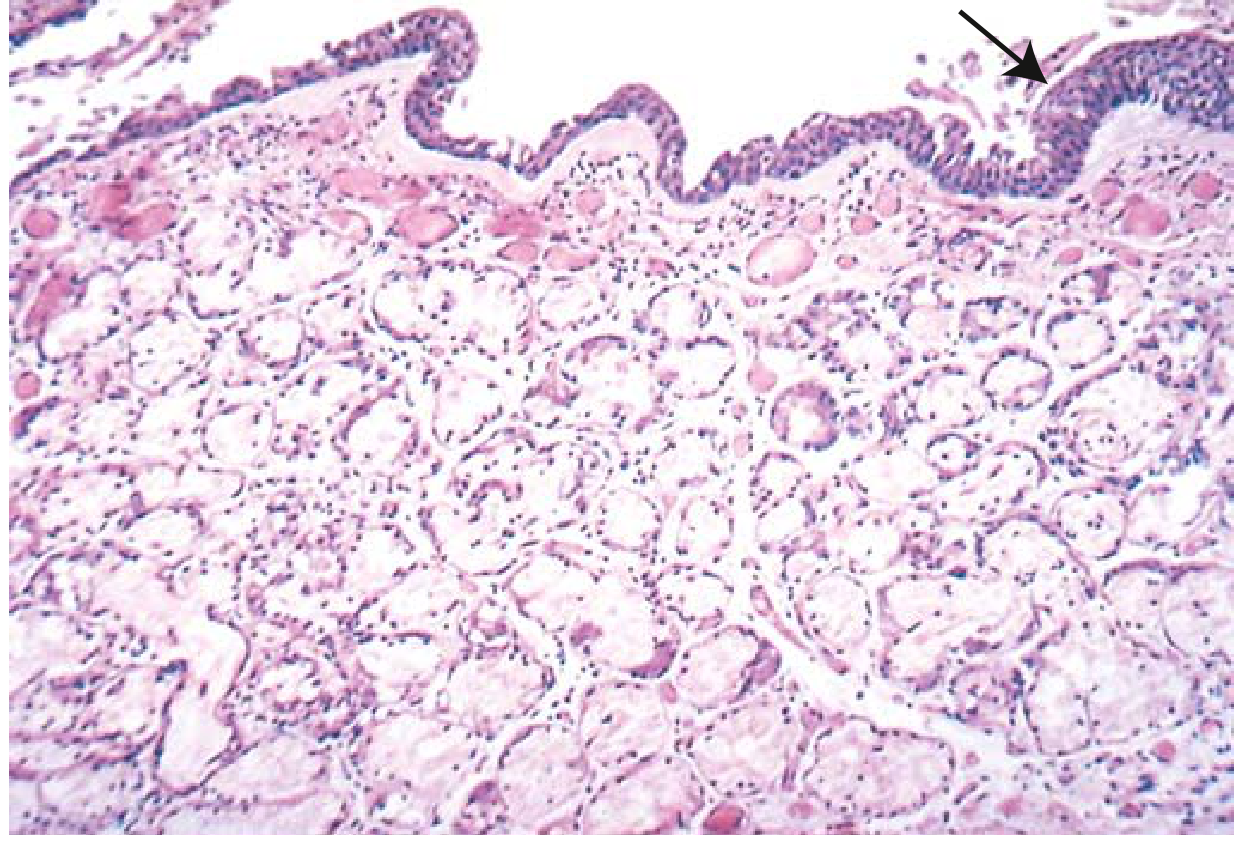
Here is the histology showing the markedly thickened mucous gland layer (approximately twice normal) with squamous metaplasia (arrow), from Robbins Basic Pathology:
- Robbins & Kumar Basic Pathology
- Robbins, Cotran & Kumar Pathologic Basis of Disease
5. Clinical Features
Classic Presentation: "Blue Bloater"
At one end of the COPD spectrum is the chronic bronchitis-dominant patient, classically called the "blue bloater":
| Feature | Chronic Bronchitis ("Blue Bloater") | Emphysema ("Pink Puffer") |
|---|---|---|
| Age at presentation | 40-45 years | 50-75 years |
| Cardinal symptom | Copious productive cough (early) | Severe dyspnea (early) |
| Dyspnea | Mild, late | Severe, early |
| Sputum | Copious | Scanty |
| Infections | Common | Occasional |
| Cor pulmonale | Common | Uncommon (end-stage) |
| Airway resistance | Increased | Normal/slightly increased |
| Elastic recoil | Normal | Low |
| Gas exchange | Hypoxemia + hypercapnia, cyanosis | Relatively preserved until late |
| Body habitus | Overweight/obese | Thin, weight loss |
| Chest X-ray | Prominent vessels, large heart | Hyperinflation, flattened diaphragm |
Most real patients fall somewhere between these two extremes.
Additional Clinical Findings
- Hemoptysis may occur, especially during exacerbations - always warrants evaluation for lung cancer
- Clubbing is NOT a feature of CB/COPD - if present, evaluate for lung cancer or pulmonary fibrosis
- Wheezing may be present (asthmatic bronchitis variant with airway hyperresponsiveness)
- Morning cough worsening, productive throughout the day
- Symptoms are worst in winter months
- Exacerbations are triggered by viral/bacterial URTIs, environmental pollutants
- Advanced disease: hypoxemia (cyanosis), hypercapnia (elevated serum bicarbonate as clue on labs), cor pulmonale, pulmonary hypertension
Complications
-
Pulmonary hypertension → cor pulmonale → right heart failure
-
Respiratory failure (acute on chronic)
-
Recurrent pneumonias
-
Obstructive sleep apnea (10-30% of COPD patients)
-
Atrial fibrillation and other arrhythmias
-
Depression (frequent comorbidity)
-
Polycythemia (secondary to chronic hypoxemia)
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
-
Goldman-Cecil Medicine
6. Investigations
Spirometry (Most Important)
- FEV1/FVC < 0.7 (post-bronchodilator) defines airflow obstruction/COPD
- FEV1 is reduced; FVC is normal or near-normal early on
- GOLD staging classifies severity by % predicted FEV1
Arterial Blood Gases
- Type 2 respiratory failure: hypoxemia + hypercapnia (PaO2 ↓, PaCO2 ↑)
- Compensatory metabolic alkalosis: elevated serum HCO3 is a clue that hypercarbia is chronic
- ABG required to confirm hypercarbia (pulse oximetry only shows SpO2)
Chest X-Ray
- Prominent bronchial markings ("dirty chest")
- Enlarged heart if cor pulmonale present
- Less useful for pure CB (no hyperinflation unlike emphysema)
HRCT Chest
- Airway wall thickening, mucus plugging
- Distinguishes CB from emphysema, bronchiectasis
- Bullae suggest emphysematous component
Sputum
- Mucoid (stable) or mucopurulent (exacerbation)
- Culture during exacerbations to guide antibiotic choice
ECG/Echo
- In advanced disease: right heart strain, pulmonary hypertension assessment
- Echocardiography may be limited by hyperinflation (retrosternal air)
7. Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Asthma | Young onset, atopy, reversible obstruction, eosinophilia, no smoking history (typically) |
| Bronchiectasis | Copious purulent sputum >30 mL/day, HRCT shows dilated non-tapering airways |
| Bronchiolitis obliterans | History of collagen vascular disease or lung transplant, no emphysema on CT |
| Lung cancer | Change in cough character + hemoptysis - must exclude with CXR ± CT |
| Heart failure | Dyspnea + orthopnea, elevated BNP, cardiomegaly |
| ACE inhibitor cough | Dry non-productive cough, no sputum, resolves on stopping drug |
8. Treatment
8a. Non-Pharmacological (Foundational)
- Smoking cessation - most effective intervention; cough typically reduces within 4-5 weeks of quitting
- Pulmonary rehabilitation
- Avoidance of occupational and environmental triggers
- Influenza and pneumococcal vaccinations
- Chest physiotherapy for secretion clearance
8b. Bronchodilators (Mainstay)
- Short-acting beta-2 agonists (SABA) - e.g., salbutamol/albuterol: relieves acute bronchospasm
- Short-acting muscarinic antagonists (SAMA) - e.g., ipratropium: reduces secretions + bronchodilation
- Long-acting beta-2 agonists (LABA) - e.g., salmeterol, formoterol
- Long-acting muscarinic antagonists (LAMA) - e.g., tiotropium: first-line maintenance for stable COPD
8c. Inhaled Corticosteroids (ICS)
- Added for patients with frequent exacerbations or eosinophil count >100-300 cells/µL
- Combined ICS + LABA suppresses airway inflammation
- Triple therapy: ICS + LABA + LAMA for severe cases
8d. Roflumilast (PDE4 inhibitor - oral)
- Specifically indicated for severe COPD with chronic bronchitis and frequent exacerbations
- GOLD guidelines recommend as add-on:
- In patients with exacerbations despite LABA/LAMA, if eosinophils <100 cells/µL
- In patients with CB + FEV1 <50% + ≥1 hospitalization on triple therapy
- Small but significant reduction in exacerbation rate
- Side effects: GI (diarrhea, nausea, weight loss), neuropsychiatric (depression, anxiety, suicidality) - monitor closely
- Contraindicated in Child-Pugh B/C liver disease
8e. Mucoactive Agents
- Guaifenesin (expectorant): increases airway water to facilitate mucus expulsion
- N-acetylcysteine (mucolytic): breaks disulfide bonds in mucin, reduces viscosity
- Hypertonic saline nebulization: osmotically draws water into airway lumen
- Beta-2 agonists (mukokinetic): enhance ciliary activity
- Anticholinergics (mucoregulators): reduce mucus secretion
8f. Long-Term Oxygen Therapy (LTOT)
- Indicated if resting PaO2 ≤55 mmHg or SpO2 ≤88% (or PaO2 56-59 with cor pulmonale/polycythemia)
-
15 hours/day shown to improve survival in hypoxic cor pulmonale complicating CB (landmark MRC Trial, 1981)
8g. Management of Exacerbations
- Antibiotics (amoxicillin, doxycycline, or macrolide for outpatient; broader coverage for inpatients)
- Short-course systemic corticosteroids (5-7 days prednisolone)
- Intensified bronchodilator therapy (nebulized SABA ± SAMA)
- Controlled oxygen therapy (target SpO2 88-92% to avoid hypercapnic drive suppression)
- Non-invasive ventilation (NIV/BiPAP) for acute hypercapnic respiratory failure (pH <7.35)
8h. Surgical / Interventional
-
Lung volume reduction surgery (selected emphysema-dominant patients)
-
Lung transplantation (end-stage, selected patients)
-
Murray & Nadel's Textbook of Respiratory Medicine
-
Goldman-Cecil Medicine
-
Fishman's Pulmonary Diseases and Disorders
-
Goodman & Gilman's Pharmacological Basis of Therapeutics
9. Prognosis & Natural History
- In a smoker, the presence of chronic bronchitis is predictive of progressive irreversible airflow obstruction leading to COPD
- Some patients retain a persistent productive cough without ever developing airflow obstruction - these have a better prognosis
- Patients with a dominant bronchitic component have more frequent exacerbations, more rapid disease progression, and poorer outcomes than those with emphysema alone
- Progressive disease leads to: pulmonary hypertension → cor pulmonale → right heart failure
- Death can result from:
- Acute respiratory failure (infection superimposed on COPD)
- Right heart failure (cor pulmonale)
- Pneumothorax (from emphysematous blebs)
- Lung cancer (due to shared risk factors + squamous metaplasia progression)
Summary at a Glance
| Domain | Key Point |
|---|---|
| Definition | Productive cough ≥3 months/year for ≥2 consecutive years |
| Pathology hallmark | Enlarged submucosal mucous glands; Reid index >0.4 |
| Cellular mechanism | IL-13, neutrophil elastase, acquired CFTR dysfunction, goblet cell hyperplasia |
| Key cell types | Neutrophils, macrophages, lymphocytes (NOT eosinophils) |
| Airflow obstruction | From small airway fibrosis (not the large airway gland hypertrophy) |
| Classic phenotype | "Blue bloater" - cyanotic, overweight, hypercapnic, cor pulmonale |
| Spirometry | FEV1/FVC <0.7 when obstruction is present |
| First-line treatment | Smoking cessation + LAMA ± LABA |
| Specific drug for CB exacerbations | Roflumilast (PDE4 inhibitor) |
| Infection | Maintains, does not initiate chronic bronchitis |
Sources: Robbins & Kumar Basic Pathology | Robbins, Cotran & Kumar Pathologic Basis of Disease | Goldman-Cecil Medicine | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases and Disorders | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.