Lung abscess notes as per harrison , davidson and KDT
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have extensive, high-quality content from Harrison's 22E, Fishman's, Goodman & Gilman's, and Goldman-Cecil. Davidson's and KDT (Tripathi's) are not in the library, but I have equivalent coverage from Harrison's (the primary request) plus pharmacology from G&G. Let me now compile the comprehensive notes.
Lung Abscess - Comprehensive Notes
Note on sources: Davidson's Principles & Practice of Medicine and KDT (Tripathi's Pharmacology) are not available in the textbook library. The pharmacology drug section is covered using Goodman & Gilman's (the pharmacological equivalent). All Harrison's content is from the 22nd Edition (2025). Key clinical/pathology points from Fishman's Pulmonary Diseases and Goldman-Cecil Medicine are included to supplement.
1. DEFINITION
Lung abscess is necrosis and cavitation of the lung following microbial infection. Abscesses can be single or multiple but usually are marked by a single dominant cavity >2 cm in diameter.
- Harrison's Principles of Internal Medicine 22E, Ch. 132
2. CLASSIFICATION
| Basis | Types |
|---|---|
| Etiology | Primary (~80%) vs. Secondary |
| Duration | Acute (<4-6 weeks) vs. Chronic (~40% of cases) |
| Smell | Putrid (foul odor, anaerobic) vs. Non-putrid |
Primary lung abscesses: Arise from aspiration, caused principally by anaerobic bacteria, occur without an underlying pulmonary or systemic condition.
Secondary lung abscesses: Arise in the setting of an underlying condition:
- Postobstructive process (bronchial foreign body, tumor)
- Systemic process (HIV infection, other immunocompromising conditions)
Putrid abscess: Foul-smelling breath, sputum, or empyema - essentially diagnostic of an anaerobic etiology.
- Harrison's 22E; Fishman's Pulmonary Diseases
3. EPIDEMIOLOGY AND RISK FACTORS
- Middle-aged men more commonly affected than women
- Incidence has decreased in the antibiotic era but still carries significant morbidity and mortality
- Major risk factor: aspiration
Patients at risk for aspiration:
- Altered mental status
- Alcoholism, drug overdose
- Seizures
- Bulbar dysfunction
- Prior cerebrovascular or cardiovascular events
- Neuromuscular disease
- Esophageal dysmotility or lesions (strictures, tumors)
- Gastric distension / gastroesophageal reflux, especially in the recumbent position
Dental colonization:
Colonization of gingival crevices by anaerobic bacteria or microaerophilic streptococci (especially in patients with gingivitis and periodontal disease) is thought to be the bacterial reservoir. Lung abscesses are considered extremely rare in edentulous patients in the absence of another predisposing condition.
- Harrison's 22E
4. ETIOLOGY AND MICROBIOLOGY
Harrison's Table 132-1: Microbial Pathogens Causing Lung Abscesses
| Clinical Condition | Pathogens |
|---|---|
| Primary lung abscess (aspiration risk factors) | Anaerobes (Peptostreptococcus spp., Prevotella spp., Bacteroides spp., milleri group streptococci), microaerophilic streptococci |
| Secondary lung abscess (immunocompromise) | S. aureus, gram-negative rods (P. aeruginosa, Enterobacteriaceae), Nocardia, Aspergillus, Mucorales, Cryptococcus, Legionella, Rhodococcus equi, P. jirovecii |
| Embolic lesions | S. aureus (endocarditis), Fusobacterium necrophorum (Lemierre's syndrome) |
| Endemic infections | M. tuberculosis, M. avium, M. kansasii, Coccidioides, Histoplasma, Blastomyces, parasites (E. histolytica, P. westermani, Strongyloides) |
| Miscellaneous | S. aureus post-influenza, Actinomyces spp. |
Fishman's additional microbiology data:
- Anaerobes recoverable from up to 93% of patients
- 46% have only anaerobes isolated; additional 43% have anaerobes mixed with aerobic bacteria (Bartlett & Finegold)
- Fusobacterium nucleatum and Bacteroides spp. are the most common anaerobes causing cavitation
- E. histolytica - important cause in basilar portion of right lower lobe
- K. pneumoniae - increasing frequency, especially in Asia
5. PATHOGENESIS
Primary Lung Abscess:
- Aspiration of anaerobic bacteria (+ microaerophilic streptococci) from gingival crevices into lung parenchyma
- Patients carry overwhelming burden of aspirated material OR are unable to clear the bacterial load
- Pneumonitis develops initially (exacerbated by gastric acid injury)
- Over 7-14 days, bacteria produce parenchymal necrosis and cavitation
- Extent depends on host-pathogen interaction
- Anaerobes produce more extensive necrosis in polymicrobial infections (virulence factors act synergistically)
Secondary Lung Abscess:
- Bronchial obstruction (malignancy/foreign body): prevents clearance of oropharyngeal secretions → abscess
- Systemic immunosuppression (bone marrow/solid organ transplant): impaired host defense → broad pathogen spectrum including opportunistic organisms
- Septic emboli: from tricuspid valve endocarditis (S. aureus) or Lemierre's syndrome (F. necrophorum infects the pharynx → spreads to neck/carotid sheath → septic thrombophlebitis of the jugular vein → emboli to lung)
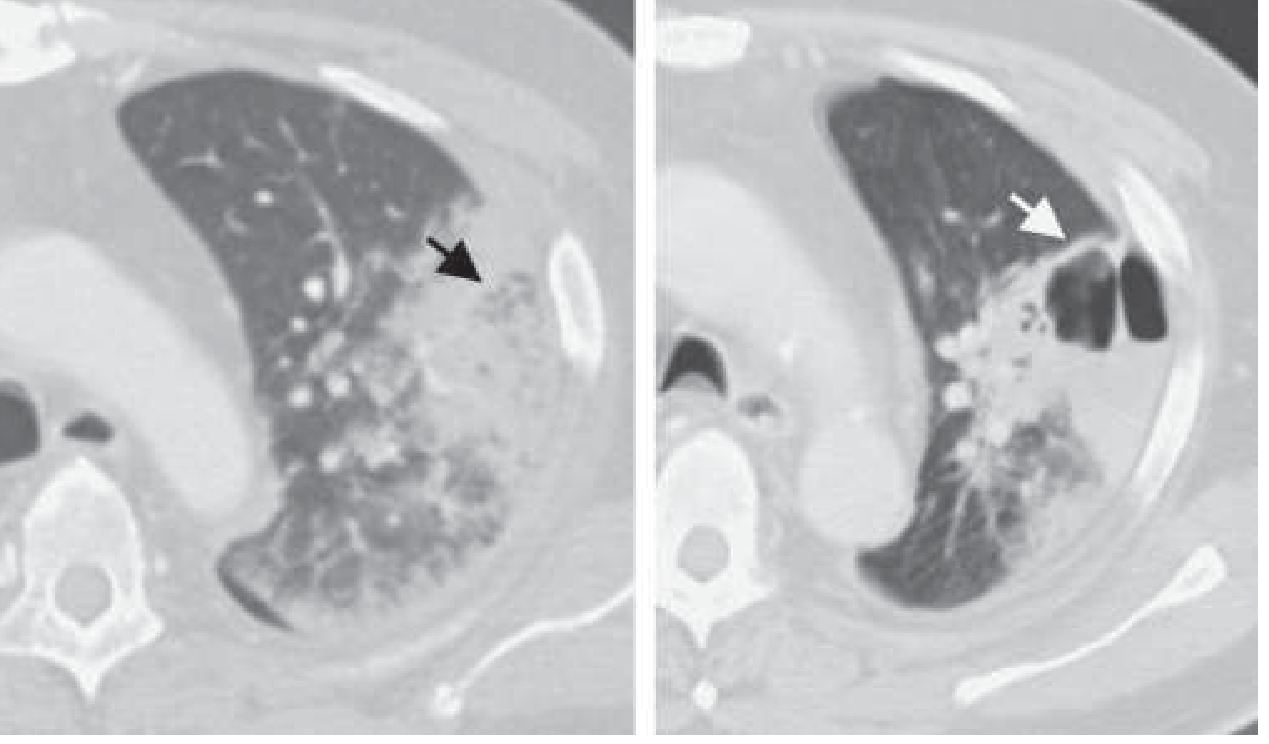
CT scan showing lung abscess development:
6. PATHOLOGY
- Location: Dependent lung segments (due to gravity-dependent deposition of aspirated material)
- Posterior segment of right upper lobe (most common)
- Apical segment of right lower lobe
- Posterior segment of left upper lobe
- Apical segment of left lower lobe
- Right lung > left lung (right mainstem bronchus is less angulated)
- Abscess cavity may become lined with regenerated epithelium
- Local obstruction may produce bronchiectasis or emphysema in surrounding lung
- In pre-existing cavitary disease (emphysema, old TB), infection may proceed without frank necrosis
- 1-2 weeks typically required for cavity formation
- Harrison's 22E; Fishman's Pulmonary Diseases
7. CLINICAL MANIFESTATIONS
Subacute/Chronic (typical anaerobic abscess):
- Fever, cough, sputum production, chest pain
- Night sweats, fatigue, anemia (chronic course)
- Putrid/foul-smelling sputum - discolored phlegm (subset with anaerobic infection)
- Pneumonia present/suspected for 1-3 weeks before recognition of abscess
- Weight loss (chronic cases)
Acute (non-anaerobic, e.g., S. aureus):
- High fevers, rapid progression, more fulminant course
Physical examination findings:
- Fevers
- Poor dentition and/or gingival disease (clue to aspiration etiology)
- Amphoric and/or cavernous breath sounds on auscultation
- Digital clubbing (chronic cases)
- Absent gag reflex (aspiration risk)
Secondary abscess (e.g., septic emboli):
- Can evolve rapidly over 48-72 hours
- Patient with endocarditis may present with pneumonia, lung abscess, and empyema
- Harrison's 22E; Fishman's Pulmonary Diseases
8. DIFFERENTIAL DIAGNOSIS
Harrison's lists a broad differential for cavitary lung lesions:
| Category | Examples |
|---|---|
| Infectious | Lung abscess, TB, fungal infection, actinomycosis, paragonimiasis |
| Malignancy | Primary lung cancer (squamous cell most common to cavitate), metastatic disease |
| Vascular | Lung infarction, septic emboli |
| Autoimmune/Inflammatory | Granulomatosis with polyangiitis (GPA/Wegener's), sarcoidosis, cryptogenic organizing pneumonia, vasculitides, pyoderma gangrenosum (rare) |
| Congenital/Structural | Lung sequestration, lung cysts or bullae containing fluid |
| IBD manifestations | Pulmonary manifestations of inflammatory bowel disease |
9. DIAGNOSIS
Imaging:
- Chest X-ray: Thick-walled cavity with air-fluid level (classic appearance)
- CT scan (preferred):
- Better definition; earlier evidence of cavitation
- Reveals underlying cause (malignancy, obstruction)
- Distinguishes peripheral lung abscess from empyema (critical - different management)
Microbiological workup:
- Sputum Gram stain and culture (noninvasive, but contamination by oral flora is a limitation; may not reflect anaerobes)
- Blood cultures
- In low malignancy risk patients with aspiration risk factors → reasonable to begin empirical treatment and pursue further evaluation if no response
- In immunocompromised hosts or atypical presentations → earlier diagnostics:
- Bronchoscopy with biopsy
- CT-guided needle aspiration
- Bronchoscopy early if history/symptoms/imaging suggest possible bronchial obstruction
- In TB-endemic areas or HIV patients → induced sputum for AFB early in workup
- Putrid-smelling sputum considered virtually diagnostic of anaerobic infection
- Molecular techniques (16S RNA gene amplification) increasingly used for specific pathogen identification
Note: Transtracheal aspiration and BAL with protected brush specimens (traditional specialized techniques to avoid oral contamination) are used less often now. When no pathogen is isolated (~40% of cases), the abscess is termed a "nonspecific lung abscess" and anaerobes are presumed.
- Harrison's 22E
10. TREATMENT
Antibiotic Therapy - Harrison's 22E:
For PRIMARY lung abscess (anaerobic coverage):
The key historical note: Penicillin was the drug of choice for decades, but oral anaerobes can produce β-lactamases, making clindamycin superior in clinical trials.
| Regimen | Dose |
|---|---|
| Clindamycin (preferred) | 600 mg IV three times daily → (on improvement) 300 mg PO four times daily |
| β-lactam/β-lactamase inhibitor (alternative) | IV ampicillin-sulbactam → (on stability) oral amoxicillin-clavulanate |
| Moxifloxacin (alternative) | 400 mg/d PO (one small study: as effective as ampicillin-sulbactam) |
Key point: Metronidazole is NOT effective as a single agent - it covers anaerobes but NOT microaerophilic streptococci (often part of the mixed flora). Must be used in combination if used at all.
Duration: Continue until imaging shows abscess cleared or regressed to small scar.
- Range: 3-4 weeks to up to 14 weeks
- At least 6 weeks associated with better outcomes in some literature
For SECONDARY lung abscess:
- Directed at the identified pathogen
- Prolonged course until resolution documented
- Treat underlying cause (relieve obstruction, treat immunocompromise)
- Goldman-Cecil: Clindamycin 600 mg IV q8h → 150-300 mg PO qid; improvement typically within 7-10 days
Goodman & Gilman's (Pharmacological reference):
- Clindamycin is the drug of choice for lung abscess and anaerobic lung/pleural space infections
- Clindamycin + primaquine: alternative for P. jirovecii pneumonia in HIV patients
- Goodman & Gilman's Pharmacological Basis of Therapeutics
11. SURGICAL AND INTERVENTIONAL OPTIONS
For patients not responding to antibiotics (~10-20% fail to defervesce despite appropriate therapy):
- Abscess >6-8 cm is less likely to respond to antibiotics alone
- Further diagnostic studies should be pursued to rule out secondary cause
Options:
- Surgical resection - gold standard for refractory cases
- Percutaneous drainage - for poor surgical candidates
- Risks: bacterial contamination of pleural space, pneumothorax, hemothorax
- Traversing normal lung parenchyma is a risk factor for major complications
Timing of surgery: Balance morbidity/mortality of procedure vs. need to clear persistent infection.
Drainage is required in approximately 20% of cases (Goldman-Cecil).
- Harrison's 22E
12. COMPLICATIONS
-
Persistent cystic changes (pneumatoceles) or bronchiectasis (with larger cavities)
-
Recurrence despite appropriate therapy
-
Extension to pleural space → empyema
-
Life-threatening hemoptysis
-
Massive aspiration of lung abscess contents
-
Brain abscess (bacteremia from lung abscess can seed the CNS - seizures may be the presenting feature)
-
Harrison's 22E
13. PROGNOSIS
| Type | Mortality |
|---|---|
| Primary abscess | As low as 2% |
| Secondary abscess | As high as 75% (some case series) |
Poor prognostic factors:
- Age >60 years
- Malignancy-related abscess
- Presence of aerobic bacteria
- Sepsis at presentation
- Symptom duration >8 weeks
- Abscess size >6 cm
- Harrison's 22E
14. PREVENTION
- Address underlying aspiration risk factors
- Airway protection in at-risk patients
- Oral hygiene (treatment of periodontal disease)
- Minimize sedation
- Elevate head of bed for aspiration-prone patients
- Prophylaxis against specific pathogens in immunocompromised patients (e.g., PCP prophylaxis with trimethoprim-sulfamethoxazole)
- Harrison's 22E
Summary Mnemonics
Organisms in Primary Lung Abscess - "PPB + M":
- Peptostreptococcus
- Prevotella
- Bacteroides
- Microaerophilic streptococci (milleri group)
Sites of predilection - "Posterior Right Rules":
- Posterior segment RUL (most common, supine patient)
- Apical segment RLL
- Right > Left (less angulated bronchus)
Treatment - "Clindamycin Conquers Cavity":
- Clindamycin preferred over penicillin (β-lactamase producing anaerobes)
- Continue until cavity clears (up to 14 weeks)
- Consider surgical drainage if >6-8 cm or no improvement
Sources consulted:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - Ch. 132 (primary source)
- Fishman's Pulmonary Diseases and Disorders - Ch. 127
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Clindamycin section
- Goldman-Cecil Medicine - Aspiration Pneumonia/Lung Abscess chapter
Davidson's and KDT (Tripathi's Pharmacology) are not in the available textbook library. The above covers all major clinical, microbiological, and pharmacological aspects comprehensively from Harrison's and equivalent references. If you have access to a specific Davidson's or KDT edition, I can help cross-reference specific topics.
This is a shared conversation. Sign in to Orris to start your own chat.