NCS METHOD IN CTS FOR DM NEUROLOGY STUDENT
NCS method carpal tunnel syndrome diabetic neuropathy neurology DM student
"carpal tunnel syndrome" AND "nerve conduction" AND "diabetes mellitus"
NCS Method in Carpal Tunnel Syndrome (CTS) - For DM Neurology Students
1. WHY NCS in CTS?
- Confirming median nerve entrapment at the wrist
- Localizing the exact site of compression (within the carpal tunnel)
- Grading severity (mild/moderate/severe) - which guides treatment
- Distinguishing CTS from cervical radiculopathy (C6/C7), proximal median neuropathy, or polyneuropathy
- Monitoring recovery post-surgery or steroid injection
2. BASIC NCS PRINCIPLES
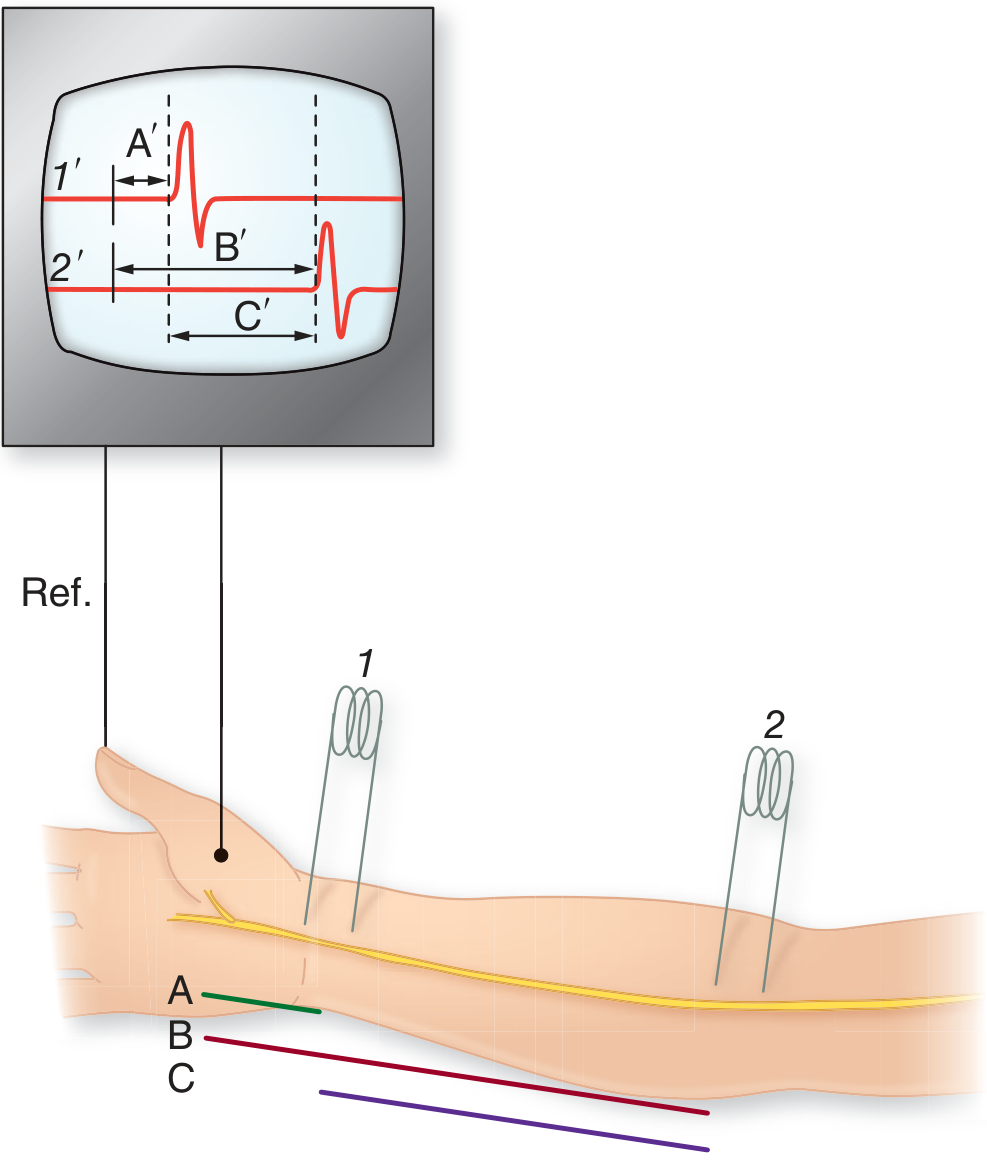
What is Measured
| Parameter | What it reflects | Normal (Median) |
|---|---|---|
| Distal latency (onset) | Conduction through the carpal tunnel to thenar muscle | < 4.2 ms (APB, 6-8 cm) |
| CMAP amplitude | Number of functioning motor axons | > 4.4 mV |
| Motor conduction velocity | Speed of fastest large fibers, forearm segment | > 49 m/s |
| F-wave latency | Proximal conduction integrity | < 31 ms |
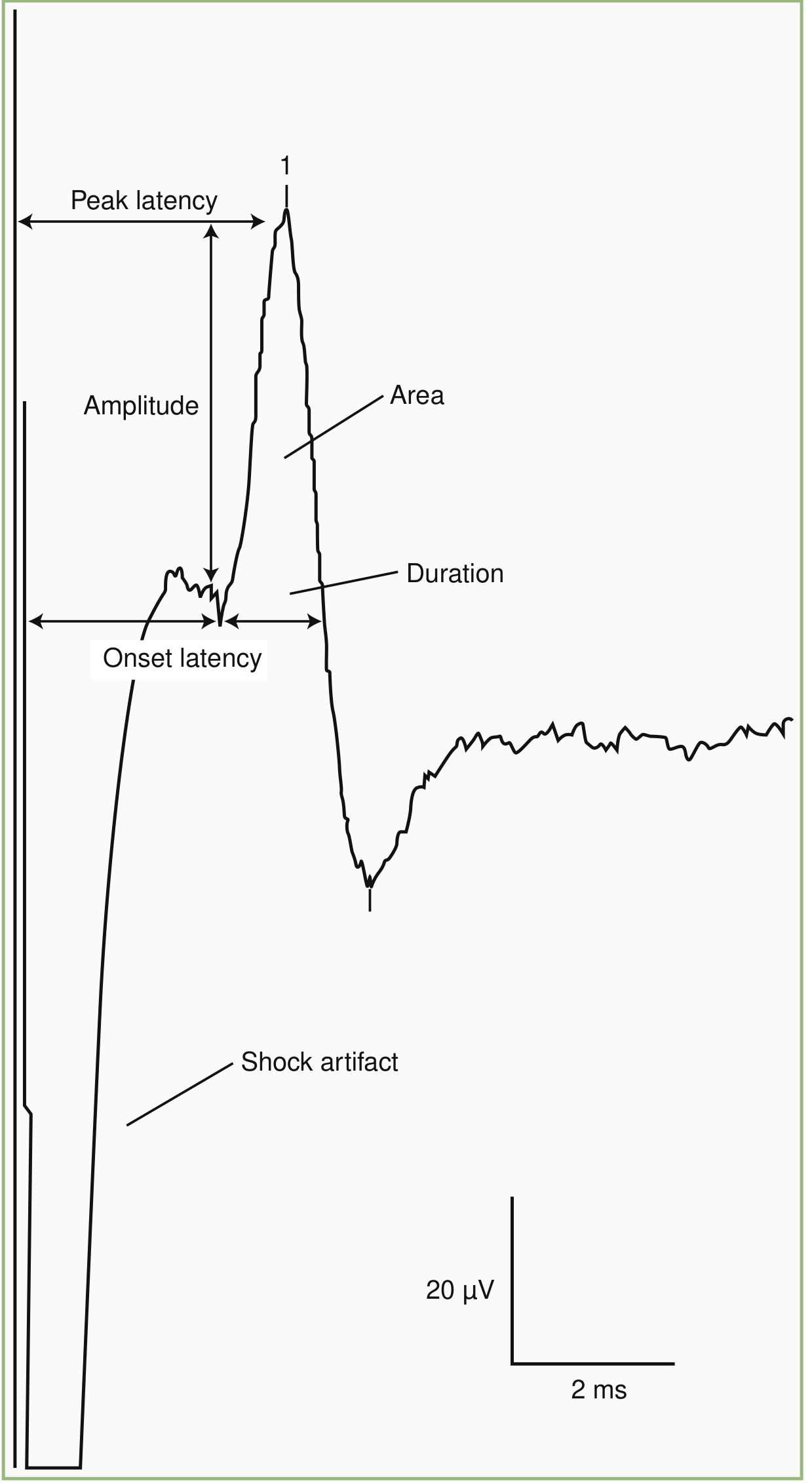
| Parameter | Normal (Median - Digit II antidromic) |
|---|---|
| Onset latency (wrist → finger 2, ~13-14 cm) | < 3.5 ms |
| Peak latency | < 3.6 ms |
| SNAP amplitude | > 20 µV |
| Sensory conduction velocity | > 50 m/s |
Key point: Sensory NCS is more sensitive than motor NCS in early CTS, because sensory fibers are affected first by compression. A prolonged sensory distal latency is the earliest NCS abnormality in CTS.
3. STANDARD NCS PROTOCOL FOR CTS
Step 1 - Median Motor NCS
- Stimulate: Median nerve at the wrist (7-8 cm proximal to APB)
- Record: Surface electrode over abductor pollicis brevis (APB)
- Measure: Distal latency, CMAP amplitude, and after proximal (elbow) stimulation - motor conduction velocity
- Abnormal in CTS: Prolonged distal motor latency > 4.2 ms; normal forearm MCV (focal slowing at tunnel)
Step 2 - Median Sensory NCS (Antidromic)
- Stimulate: Median nerve at the wrist
- Record: Ring electrodes on digit II (index) or digit III (middle finger)
- Distance: 13-14 cm
- Abnormal in CTS: Prolonged peak latency, reduced SNAP amplitude, slowed SCV
Step 3 - Ulnar Sensory and Motor NCS (Mandatory comparison)
- Stimulate ulnar nerve at wrist; record at digit V (ADM for motor)
- Used as an internal comparator - ulnar should be normal in isolated CTS
Step 4 - Internal Comparison Studies (Critical - see below)
4. INTERNAL COMPARISON STUDIES IN CTS
| Comparison Study | Technique | Abnormal Criterion |
|---|---|---|
| Median-Ulnar Palmar Mixed Study | Stimulate palm (8 cm from wrist), record at wrist for both nerves | Median latency > ulnar by > 0.3 ms |
| Median-Ulnar Ring Finger (Sensory) | Stimulate wrist, record at ring finger (digit IV) antidromically | Median latency > ulnar by > 0.4 ms |
| Median-Ulnar Lumbrical-Interossei Motor | Stimulate median and ulnar at wrist, record at 2nd interossei space | Median CMAP latency exceeds ulnar by > 0.4-0.5 ms |
| Median-Radial Sensory to Thumb | Stimulate median and radial at wrist, record at thumb | Median latency > radial by > 0.5 ms |
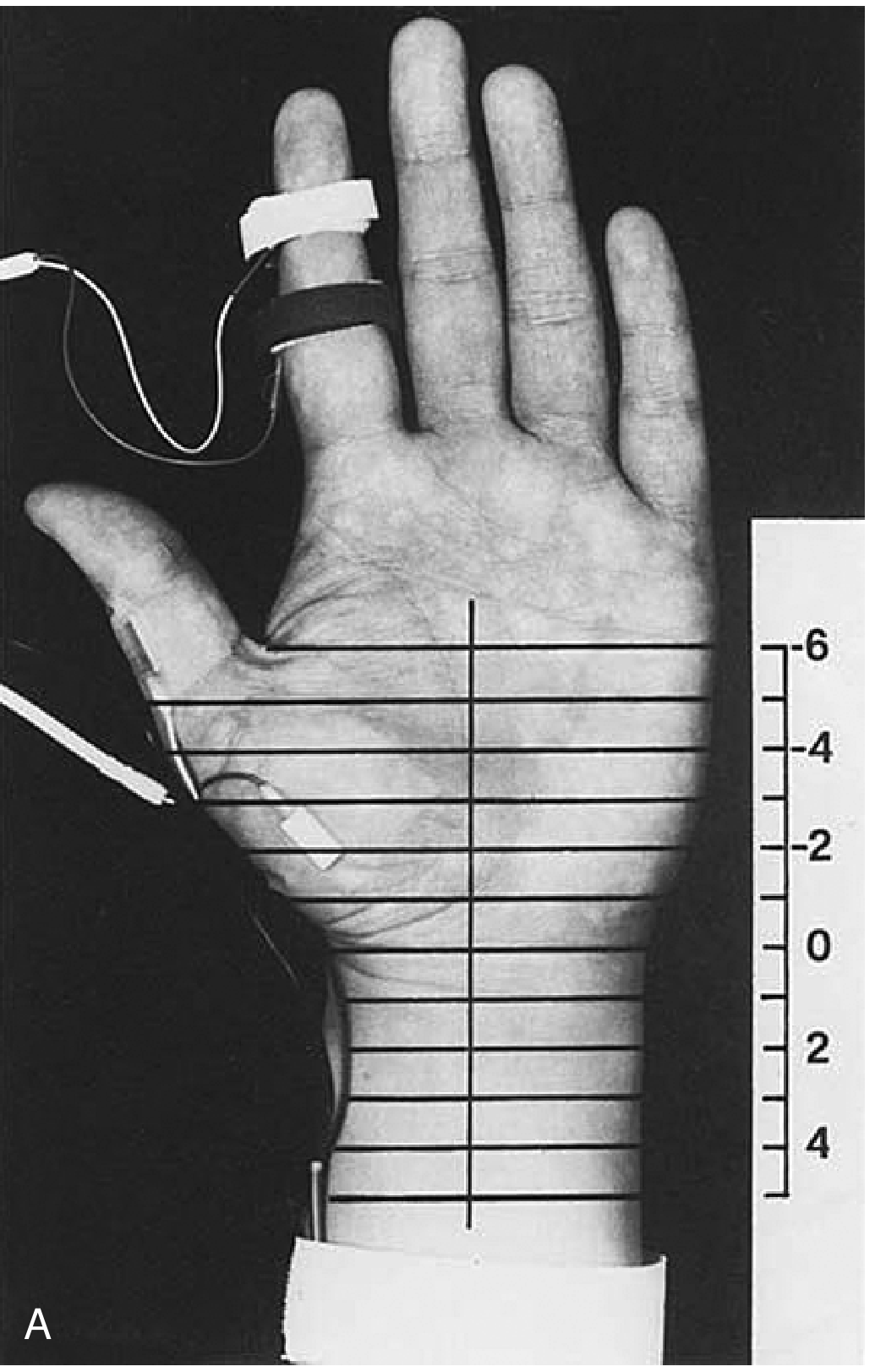
5. THE INCHING / SEGMENTAL STIMULATION TECHNIQUE
- A 0.2 ms slowing over a 10-cm segment = only 10% change (can be missed)
- The same 0.2 ms slowing over 1 cm = 100% change - unmistakable
6. NCS SEVERITY GRADING IN CTS
| Grade | NCS Findings |
|---|---|
| Mild | Only prolonged median sensory latency; normal motor latency and CMAP amplitude |
| Moderate | Prolonged motor and sensory latencies; SNAP may be reduced in amplitude |
| Severe | Absent SNAP; significantly prolonged/absent CMAP; reduced CMAP amplitude |
| Extreme | Absent both sensory and motor responses from median nerve; needle EMG shows active denervation (fibrillations) in APB |
7. CTS IN DIABETIC PATIENTS - THE KEY CHALLENGE
Problem 1: Elevated Baselines
Problem 2: DM Is a Risk Factor for CTS
Problem 3: Small Fiber Neuropathy in DM
Solution: Use Internal Comparison Studies
- Median-Ulnar palmar mixed latency difference > 0.3 ms still favors CTS superimposed on DPN
- The median-radial sensory thumb comparison is also very useful, as the radial sensory nerve bypasses the carpal tunnel entirely
Practical NCS Protocol for DM + Suspected CTS:
- Standard median motor and sensory NCS
- Standard ulnar motor and sensory NCS (comparator)
- Median-Ulnar palmar mixed nerve comparison (most sensitive internal comparison)
- Median-Radial sensory to thumb comparison
- Sural nerve NCS - to document background DPN severity (lower limb is more affected in DPN, helping grade overall polyneuropathy)
- Consider lower limb NCS (peroneal, tibial, sural) to complete polyneuropathy assessment
- Temperature control is mandatory - DM patients often have cold extremities; skin temperature must be > 32°C before testing (cold falsely prolongs latency and mimics neuropathy)
NCS Parameters Distinguishing Focal CTS from Diffuse DPN:
| Feature | Focal CTS | Diffuse DPN |
|---|---|---|
| Sensory latency prolongation | Median > Ulnar (focal) | Both equally prolonged |
| Motor latency | Median forearm NCV normal; only distal latency prolonged | All nerves slowed |
| Upper vs lower limb | Upper limb isolated | Lower limb worse (length-dependent) |
| Sural nerve | Normal | Abnormal (reduced/absent SNAP) |
| F-waves | Normal (forearm) | All prolonged |
8. CTS DIAGNOSIS FLOWCHART FOR DM PATIENTS
Suspected CTS in DM patient
|
v
NCS: Median motor + sensory
Ulnar motor + sensory
Lower limb NCS (sural, peroneal)
|
___________________________________________
| |
All nerves slowed Median specifically slow,
(length-dependent pattern) ulnar relatively normal
DPN confirmed |
| Internal comparison studies
v (Median-Ulnar palmar/ring)
Consider skin biopsy |
for small fiber DPN Median latency > Ulnar
by >0.3 ms → CTS CONFIRMED
(superimposed on DPN)
9. QUICK REFERENCE: NORMAL NCS VALUES
| Nerve | Study | Latency | Amplitude | Velocity |
|---|---|---|---|---|
| Median motor | Wrist → APB | < 4.2 ms | > 4.4 mV | > 49 m/s |
| Ulnar motor | Wrist → ADM | < 3.4 ms | > 6.0 mV | > 49 m/s |
| Median sensory | Wrist → Digit II | < 3.5 ms | > 20 µV | > 50 m/s |
| Ulnar sensory | Wrist → Digit V | < 3.1 ms | > 17 µV | > 50 m/s |
| Sural sensory | Calf → Ankle | < 4.4 ms | > 6 µV | > 40 m/s |
| Peroneal motor | Ankle → EDB | < 5.8 ms | > 2.0 mV | > 42 m/s |
10. KEY TEACHING POINTS FOR DM NEUROLOGY EXAM
- Sensory NCS is more sensitive than motor in early CTS - abnormal sensory latency/velocity is the first finding
- Internal comparison methods (median vs ulnar at equal distances) are the most sensitive and are essential when DPN co-exists
- The inching technique (1-cm increments across wrist) is the most precise localizer - a jump > 0.5 ms/cm is pathological
- In DM + CTS, use median-ulnar palmar comparison and median-radial thumb comparison to isolate the focal component
- Temperature correction is mandatory - keep limb > 32°C before testing
- EMG (needle) of APB must be added in severe/moderate CTS - fibrillations and reduced recruitment confirm axonal loss and indicate surgical urgency
- Post-surgical improvement: sensory symptoms improve first; NCS improvement (latency normalization) may lag by months
create a ppt
mkdir -p /home/daytona/workspace/ncs-cts-ppt && ls /home/daytona/workspace/ncs-cts-ppt/
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/b203dfd885b17223f0b2bf8cebd7dab9aba808948e9b7284ed2c6adccdb3cfca.png" \ "https://cdn.orris.care/cdss_images/d2accc4312c900bf30cf3cdf0c2cee6a8c4140c8dee51cbdf0103daa1b23eb47.png" \ "https://cdn.orris.care/cdss_images/90e1a9f46aa08154916f1be040155d057fbfad83bd1845eb29e39035a7afd24b.png" \ "https://cdn.orris.care/cdss_images/d449c153f8a679861b4d9f0239176a4da805e177d8cfdbf8c5780a4b337da9b6.png" \ 2>/dev/null | node -e "const d=require('fs');const j=JSON.parse(require('fs').readFileSync('/dev/stdin','utf8'));j.forEach((x,i)=>{if(x.base64){const b=x.base64.split(',')[1];d.writeFileSync('/home/daytona/workspace/ncs-cts-ppt/img'+i+'.png',Buffer.from(b,'base64'));}});console.log('done',j.map(x=>x.error||'ok'))"
~/ncs-cts-ppt/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "NCS in Carpal Tunnel Syndrome - DM Neurology";
pres.author = "DM Neurology";
// ─── THEME ────────────────────────────────────────────────────────────────────
const C = {
navy: "0B1F4B", // dominant dark
teal: "00838F", // heading accent
tealLt: "00ACC1", // lighter teal
gold: "FFB300", // accent / highlight
white: "FFFFFF",
offW: "F0F4F8",
slate: "546E7A",
ltGray: "ECEFF1",
red: "E53935",
green: "388E3C",
charcoal:"263238",
};
// ─── HELPERS ──────────────────────────────────────────────────────────────────
function addBg(slide, color) {
slide.background = { color };
}
function header(slide, title, y = 0.18, color = C.white, bkColor = C.teal) {
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 0.75,
fill: { color: bkColor }, line: { color: bkColor }
});
slide.addText(title, {
x: 0.35, y: 0, w: 9.3, h: 0.75, margin: 0,
fontSize: 22, bold: true, color, valign: "middle",
fontFace: "Calibri"
});
}
function sectionTag(slide, tag, x = 8.6, y = 0.18) {
slide.addShape(pres.ShapeType.rect, {
x, y: 0.16, w: 1.2, h: 0.42,
fill: { color: C.gold }, line: { color: C.gold }
});
slide.addText(tag, {
x, y: 0.16, w: 1.2, h: 0.42, margin: 0,
fontSize: 11, bold: true, color: C.charcoal, align: "center", valign: "middle",
fontFace: "Calibri"
});
}
function card(slide, x, y, w, h, fillColor = C.white, borderColor = C.teal, radius = 0.08) {
slide.addShape(pres.ShapeType.rect, {
x, y, w, h,
fill: { color: fillColor },
line: { color: borderColor, width: 1.5 },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 }
});
}
function tableRow(cells, opts = {}) {
return cells.map(t => ({
text: t,
options: {
fontSize: opts.fontSize || 11,
bold: opts.bold || false,
color: opts.color || C.charcoal,
fill: opts.fill || C.white,
align: opts.align || "center",
fontFace: "Calibri",
border: { pt: 0.5, color: "CFD8DC" },
valign: "middle"
}
}));
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.navy);
// Left accent bar
s.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 0.5, h: 5.625,
fill: { color: C.teal }, line: { color: C.teal }
});
// Gold stripe
s.addShape(pres.ShapeType.rect, {
x: 0.5, y: 0, w: 0.08, h: 5.625,
fill: { color: C.gold }, line: { color: C.gold }
});
// Main title
s.addText("NCS in Carpal Tunnel Syndrome", {
x: 0.85, y: 1.1, w: 8.8, h: 1.2,
fontSize: 38, bold: true, color: C.white,
fontFace: "Calibri", align: "left"
});
// Subtitle
s.addText("Method, Interpretation & Special Considerations in Diabetes", {
x: 0.85, y: 2.35, w: 8.8, h: 0.65,
fontSize: 20, bold: false, color: C.tealLt,
fontFace: "Calibri", align: "left"
});
// Gold divider line
s.addShape(pres.ShapeType.rect, {
x: 0.85, y: 3.08, w: 5.0, h: 0.05,
fill: { color: C.gold }, line: { color: C.gold }
});
// For / audience
s.addText("DM Neurology — Electrophysiology Seminar", {
x: 0.85, y: 3.25, w: 8.8, h: 0.45,
fontSize: 15, bold: false, color: C.slate,
fontFace: "Calibri", align: "left", italic: true
});
// Bottom tags
const tags = ["Motor NCS", "Sensory NCS", "Inching Technique", "CTS + DM"];
tags.forEach((t, i) => {
s.addShape(pres.ShapeType.rect, {
x: 0.85 + i * 2.2, y: 4.8, w: 2.0, h: 0.45,
fill: { color: C.teal, transparency: 60 }, line: { color: C.tealLt }
});
s.addText(t, {
x: 0.85 + i * 2.2, y: 4.8, w: 2.0, h: 0.45, margin: 0,
fontSize: 12, color: C.white, align: "center", valign: "middle",
fontFace: "Calibri"
});
});
// Source
s.addText("Source: Bradley & Daroff's Neurology | Adams & Victor's Principles of Neurology", {
x: 0.85, y: 5.25, w: 9, h: 0.3,
fontSize: 9, italic: true, color: "4A6FA5",
fontFace: "Calibri", align: "left"
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — OVERVIEW / AGENDA
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "Session Overview", 0.18, C.white, C.navy);
const items = [
{ num: "01", title: "Why NCS in CTS?", sub: "Role, indications & what it measures" },
{ num: "02", title: "NCS Parameters", sub: "Latency, amplitude, velocity - normal values" },
{ num: "03", title: "Standard Protocol", sub: "Motor → Sensory → Comparison studies" },
{ num: "04", title: "Inching Technique", sub: "Segmental stimulation for precise localization" },
{ num: "05", title: "Severity Grading", sub: "Mild / Moderate / Severe / Extreme" },
{ num: "06", title: "CTS + Diabetes", sub: "DPN background, pitfalls & internal comparison" },
{ num: "07", title: "Exam Key Points", sub: "High-yield takeaways for DM Neurology" },
];
items.forEach((item, i) => {
const col = i < 4 ? 0 : 1;
const row = i < 4 ? i : i - 4;
const x = 0.3 + col * 4.85;
const y = 0.95 + row * 1.1;
// card bg
card(s, x, y, 4.55, 0.95, C.white, C.teal);
// number circle
s.addShape(pres.ShapeType.ellipse, {
x: x + 0.12, y: y + 0.15, w: 0.62, h: 0.62,
fill: { color: C.teal }, line: { color: C.teal }
});
s.addText(item.num, {
x: x + 0.12, y: y + 0.15, w: 0.62, h: 0.62, margin: 0,
fontSize: 13, bold: true, color: C.white, align: "center", valign: "middle",
fontFace: "Calibri"
});
s.addText(item.title, {
x: x + 0.85, y: y + 0.08, w: 3.55, h: 0.38,
fontSize: 14, bold: true, color: C.navy,
fontFace: "Calibri", valign: "bottom"
});
s.addText(item.sub, {
x: x + 0.85, y: y + 0.49, w: 3.55, h: 0.35,
fontSize: 10, color: C.slate, italic: true,
fontFace: "Calibri", valign: "top"
});
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 3 — WHY NCS IN CTS?
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "Why NCS in Carpal Tunnel Syndrome?", 0.18, C.white, C.teal);
sectionTag(s, "RATIONALE");
const reasons = [
{ icon: "✔", title: "CONFIRM Diagnosis", body: "Differentiates CTS from C6/C7 radiculopathy, proximal median neuropathy, and diffuse polyneuropathy" },
{ icon: "📍", title: "LOCALIZE Compression", body: "Identifies the exact segment of focal slowing within the carpal tunnel using distal latency and inching technique" },
{ icon: "📊", title: "GRADE Severity", body: "Mild (sensory only) → Moderate (motor + sensory) → Severe (absent SNAP) → Extreme (axonal loss, denervation on EMG)" },
{ icon: "💊", title: "GUIDE Treatment", body: "Mild: splints / steroid injection | Severe: surgical decompression (carpal tunnel release)" },
{ icon: "📈", title: "MONITOR Progress", body: "Repeat NCS post-surgery or injection; sensory improvement precedes NCS normalization" },
];
reasons.forEach((r, i) => {
const y = 0.92 + i * 0.88;
// colored left bar
s.addShape(pres.ShapeType.rect, {
x: 0.3, y, w: 0.08, h: 0.72,
fill: { color: i % 2 === 0 ? C.teal : C.gold }, line: { color: i % 2 === 0 ? C.teal : C.gold }
});
card(s, 0.45, y, 9.25, 0.72, C.white, C.ltGray);
s.addText(r.icon + " " + r.title, {
x: 0.6, y: y + 0.04, w: 2.6, h: 0.36,
fontSize: 13, bold: true, color: C.navy, fontFace: "Calibri"
});
s.addText(r.body, {
x: 3.3, y: y + 0.1, w: 6.2, h: 0.5,
fontSize: 11.5, color: C.charcoal, fontFace: "Calibri", valign: "middle"
});
// divider between title and body
s.addShape(pres.ShapeType.rect, {
x: 3.2, y: y + 0.15, w: 0.04, h: 0.42,
fill: { color: C.ltGray }, line: { color: C.ltGray }
});
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 4 — NCS PARAMETERS (with motor diagram image)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "NCS Parameters — What We Measure", 0.18, C.white, C.navy);
sectionTag(s, "PARAMETERS");
// Left: image of motor NCS setup
card(s, 0.25, 0.85, 4.0, 3.6, C.white, C.teal);
s.addImage({ path: "/home/daytona/workspace/ncs-cts-ppt/img0.png", x: 0.35, y: 0.92, w: 3.8, h: 3.45 });
// Right: parameter boxes
const params = [
{ label: "Distal Latency", val: "Time from stimulus → CMAP onset", unit: "Normal median: <4.2 ms", col: C.teal },
{ label: "CMAP Amplitude", val: "Height of motor potential = axon count", unit: "Normal median: >4.4 mV", col: C.tealLt },
{ label: "Motor Conduction Velocity", val: "Distance ÷ (proximal − distal latency)", unit: "Normal: >49 m/s (arm)", col: C.navy },
{ label: "F-Wave Latency", val: "Tests proximal conduction (forearm → cord)", unit: "Normal median: <31 ms", col: C.gold },
];
params.forEach((p, i) => {
const y = 0.88 + i * 0.88;
s.addShape(pres.ShapeType.rect, {
x: 4.55, y, w: 0.22, h: 0.72,
fill: { color: p.col }, line: { color: p.col }
});
card(s, 4.77, y, 4.95, 0.72, C.white, C.ltGray);
s.addText(p.label, {
x: 4.9, y: y + 0.04, w: 4.7, h: 0.3,
fontSize: 12, bold: true, color: p.col === C.gold ? C.charcoal : p.col,
fontFace: "Calibri"
});
s.addText(p.val, {
x: 4.9, y: y + 0.32, w: 3.4, h: 0.25,
fontSize: 10, color: C.charcoal, fontFace: "Calibri"
});
s.addShape(pres.ShapeType.rect, {
x: 7.0, y: y + 0.16, w: 1.6, h: 0.4,
fill: { color: p.col }, line: { color: p.col }
});
s.addText(p.unit, {
x: 7.0, y: y + 0.16, w: 1.6, h: 0.4, margin: 0,
fontSize: 9, bold: true, color: p.col === C.gold ? C.charcoal : C.white,
align: "center", valign: "middle", fontFace: "Calibri"
});
});
// Caption
s.addText("Fig: Median nerve stimulated at wrist (1) & antecubital fossa (2). CMAP at APB.\nMCV = Segment C ÷ (B'−A') — Adams & Victor's Neurology, Fig. 2-11", {
x: 0.25, y: 4.52, w: 4.0, h: 0.78,
fontSize: 8.5, italic: true, color: C.slate, fontFace: "Calibri", align: "center"
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 5 — SENSORY NCS (with SNAP image)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "Sensory NCS — SNAP Parameters", 0.18, C.white, C.teal);
sectionTag(s, "SENSORY NCS");
// SNAP image on the right
card(s, 6.2, 0.85, 3.55, 4.3, C.white, C.teal);
s.addImage({ path: "/home/daytona/workspace/ncs-cts-ppt/img1.png", x: 6.35, y: 0.92, w: 3.25, h: 4.1 });
s.addText("Antidromic Median SNAP\n(Wrist stimulation → Digit II recording)\nBradley & Daroff Fig. 36.2", {
x: 6.2, y: 5.18, w: 3.55, h: 0.3, margin: 0,
fontSize: 8, italic: true, color: C.slate, align: "center", fontFace: "Calibri"
});
// Left content
s.addText("Key SNAP Measurements:", {
x: 0.3, y: 0.88, w: 5.6, h: 0.38,
fontSize: 15, bold: true, color: C.navy, fontFace: "Calibri"
});
const snapParams = [
{ name: "Onset Latency", def: "Stimulus → first deflection from baseline", norm: "< 3.5 ms (13 cm)", key: true },
{ name: "Peak Latency", def: "Stimulus → peak of SNAP", norm: "< 3.6 ms", key: false },
{ name: "SNAP Amplitude", def: "Baseline → peak height (µV)", norm: "> 20 µV", key: false },
{ name: "Sensory CV", def: "Distance ÷ onset latency", norm: "> 50 m/s (median)", key: false },
];
snapParams.forEach((p, i) => {
const y = 1.35 + i * 0.82;
card(s, 0.3, y, 5.7, 0.72, p.key ? "E3F2FD" : C.white, p.key ? C.teal : C.ltGray);
s.addText(p.name, {
x: 0.45, y: y + 0.06, w: 2.2, h: 0.3,
fontSize: 12.5, bold: true, color: C.teal, fontFace: "Calibri"
});
s.addText(p.def, {
x: 0.45, y: y + 0.38, w: 3.2, h: 0.28,
fontSize: 10, color: C.slate, italic: true, fontFace: "Calibri"
});
s.addShape(pres.ShapeType.rect, {
x: 3.8, y: y + 0.14, w: 2.0, h: 0.42,
fill: { color: p.key ? C.teal : C.ltGray }, line: { color: p.key ? C.teal : C.ltGray }
});
s.addText(p.norm, {
x: 3.8, y: y + 0.14, w: 2.0, h: 0.42, margin: 0,
fontSize: 11, bold: true, color: p.key ? C.white : C.charcoal,
align: "center", valign: "middle", fontFace: "Calibri"
});
});
// Key point box at bottom
s.addShape(pres.ShapeType.rect, {
x: 0.3, y: 4.65, w: 5.7, h: 0.72,
fill: { color: C.gold, transparency: 30 }, line: { color: C.gold }
});
s.addText("⚡ Key Point: Sensory NCS is MORE SENSITIVE than motor NCS in early CTS.\nA prolonged median sensory latency is the EARLIEST NCS abnormality.", {
x: 0.4, y: 4.68, w: 5.5, h: 0.65,
fontSize: 11.5, bold: true, color: C.charcoal, fontFace: "Calibri", valign: "middle"
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 6 — STANDARD PROTOCOL
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "Standard NCS Protocol for CTS", 0.18, C.white, C.navy);
sectionTag(s, "PROTOCOL");
const steps = [
{
step: "STEP 1", title: "Median MOTOR NCS",
stim: "Wrist (8 cm from APB)", rec: "Abductor Pollicis Brevis (APB)",
measure: "Distal latency, CMAP amplitude; then elbow → MCV",
abnormal: "DML > 4.2 ms; forearm MCV normal (focal tunnel slowing)",
col: C.teal
},
{
step: "STEP 2", title: "Median SENSORY NCS (Antidromic)",
stim: "Wrist", rec: "Ring electrodes Digit II or III",
measure: "Onset latency, peak latency, SNAP amplitude, SCV",
abnormal: "Onset latency > 3.5 ms; reduced amplitude; slowed SCV",
col: C.tealLt
},
{
step: "STEP 3", title: "Ulnar MOTOR + SENSORY NCS (Comparator)",
stim: "Wrist", rec: "ADM (motor) | Digit V (sensory)",
measure: "Latency and amplitude of both",
abnormal: "Should be NORMAL in isolated CTS — any ulnar abnormality suggests polyneuropathy",
col: C.navy
},
{
step: "STEP 4", title: "Internal Comparison Studies",
stim: "See next slide", rec: "See next slide",
measure: "Median vs Ulnar latency difference at equal distance",
abnormal: "Median > Ulnar by >0.3–0.4 ms → CTS confirmed",
col: C.gold
},
];
steps.forEach((st, i) => {
const y = 0.88 + i * 1.1;
s.addShape(pres.ShapeType.rect, {
x: 0.25, y, w: 9.5, h: 0.98,
fill: { color: C.white },
line: { color: C.ltGray },
shadow: { type: "outer", color: "000000", blur: 4, offset: 1, angle: 135, opacity: 0.08 }
});
// step color bar
s.addShape(pres.ShapeType.rect, {
x: 0.25, y, w: 1.1, h: 0.98,
fill: { color: st.col }, line: { color: st.col }
});
s.addText(st.step, {
x: 0.25, y, w: 1.1, h: 0.48, margin: 0,
fontSize: 10, bold: true, color: st.col === C.gold ? C.charcoal : C.white,
align: "center", valign: "bottom", fontFace: "Calibri"
});
s.addText(st.title, {
x: 0.25, y: y + 0.48, w: 1.1, h: 0.48, margin: 0,
fontSize: 8.5, color: st.col === C.gold ? C.charcoal : C.white,
align: "center", valign: "top", fontFace: "Calibri"
});
// content
s.addText(st.stim ? `Stimulate: ${st.stim} | Record: ${st.rec}` : "", {
x: 1.5, y: y + 0.05, w: 8.1, h: 0.3,
fontSize: 10.5, bold: true, color: C.navy, fontFace: "Calibri"
});
s.addText(`Measure: ${st.measure}`, {
x: 1.5, y: y + 0.36, w: 8.1, h: 0.25,
fontSize: 10, color: C.slate, fontFace: "Calibri"
});
s.addText(`⚠ Abnormal: ${st.abnormal}`, {
x: 1.5, y: y + 0.62, w: 8.1, h: 0.25,
fontSize: 10, bold: true, color: C.red, fontFace: "Calibri"
});
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 7 — INTERNAL COMPARISON STUDIES (TABLE)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "Internal Comparison Studies — Most Sensitive NCS Methods", 0.18, C.white, C.teal);
sectionTag(s, "COMPARISON");
s.addText("Since both median and ulnar nerves travel through the same forearm, comparing their latencies at equal distances eliminates the effect of background polyneuropathy (e.g. DM neuropathy)", {
x: 0.3, y: 0.85, w: 9.4, h: 0.45,
fontSize: 11, italic: true, color: C.slate, fontFace: "Calibri"
});
const rows = [
["Median–Ulnar\nPalmar Mixed", "Stimulate palm (8 cm from wrist)\nRecord at wrist for both nerves", "Orthodromic mixed\n(most widely used)", "Median > Ulnar\nby > 0.3 ms", "Most sensitive\nin early CTS"],
["Median–Ulnar\nSensory Ring Finger", "Stimulate wrist, record at\nDigit IV (ring finger) antidromically", "Antidromic sensory", "Median > Ulnar\nby > 0.4 ms", "Useful when\npalmar study normal"],
["Median–Ulnar\nLumbrical–Interossei", "Stimulate at wrist, record at\n2nd interosseous space", "Motor comparison", "Median > Ulnar\nby > 0.4–0.5 ms", "Best for\nmotor CTS"],
["Median–Radial\nSensory to Thumb", "Stimulate median & radial at wrist\nRecord at thumb", "Antidromic sensory", "Median > Radial\nby > 0.5 ms", "Useful in\nsevere DPN"],
];
const hdrs = ["Study", "Technique", "Type", "Abnormal Criterion", "Clinical Use"];
const colW = [1.6, 2.6, 1.5, 1.8, 1.7];
const startX = 0.3;
let curX = startX;
// header row
const hdrRow = hdrs.map((h, i) => ({
text: h,
options: {
fontSize: 11, bold: true, color: C.white,
fill: C.navy, align: "center",
border: { pt: 0.5, color: "FFFFFF" }, valign: "middle",
fontFace: "Calibri"
}
}));
const dataRows = rows.map((r, ri) => r.map((cell, ci) => ({
text: cell,
options: {
fontSize: 10, bold: ci === 3,
color: ci === 3 ? C.red : C.charcoal,
fill: ri % 2 === 0 ? C.white : C.offW,
align: "center", valign: "middle",
border: { pt: 0.5, color: "CFD8DC" },
fontFace: "Calibri"
}
})));
s.addTable([hdrRow, ...dataRows], {
x: 0.3, y: 1.38, w: 9.4, h: 3.7,
rowH: 0.74,
colW: colW,
border: { pt: 1, color: "CFD8DC" }
});
// Source footnote
s.addText("Source: Bradley & Daroff's Neurology in Clinical Practice, Table 106.4 (p. 2636)", {
x: 0.3, y: 5.2, w: 9.4, h: 0.25,
fontSize: 9, italic: true, color: C.slate, fontFace: "Calibri"
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 8 — INCHING TECHNIQUE (with images)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "The Inching (Segmental Stimulation) Technique", 0.18, C.white, C.navy);
sectionTag(s, "INCHING");
// Left image - hand photo
card(s, 0.25, 0.85, 3.2, 3.8, C.white, C.teal);
s.addImage({ path: "/home/daytona/workspace/ncs-cts-ppt/img2.png", x: 0.3, y: 0.9, w: 3.1, h: 3.7 });
s.addText("Fig 36.3A: 12 stimulation sites\nin 1-cm increments across wrist.\nReference (0) = distal wrist crease", {
x: 0.25, y: 4.68, w: 3.2, h: 0.5, margin: 0,
fontSize: 8.5, italic: true, color: C.slate, align: "center", fontFace: "Calibri"
});
// Right image - waveforms
card(s, 3.65, 0.85, 6.1, 3.8, C.white, C.teal);
s.addImage({ path: "/home/daytona/workspace/ncs-cts-ppt/img3.png", x: 3.72, y: 0.9, w: 5.95, h: 3.7 });
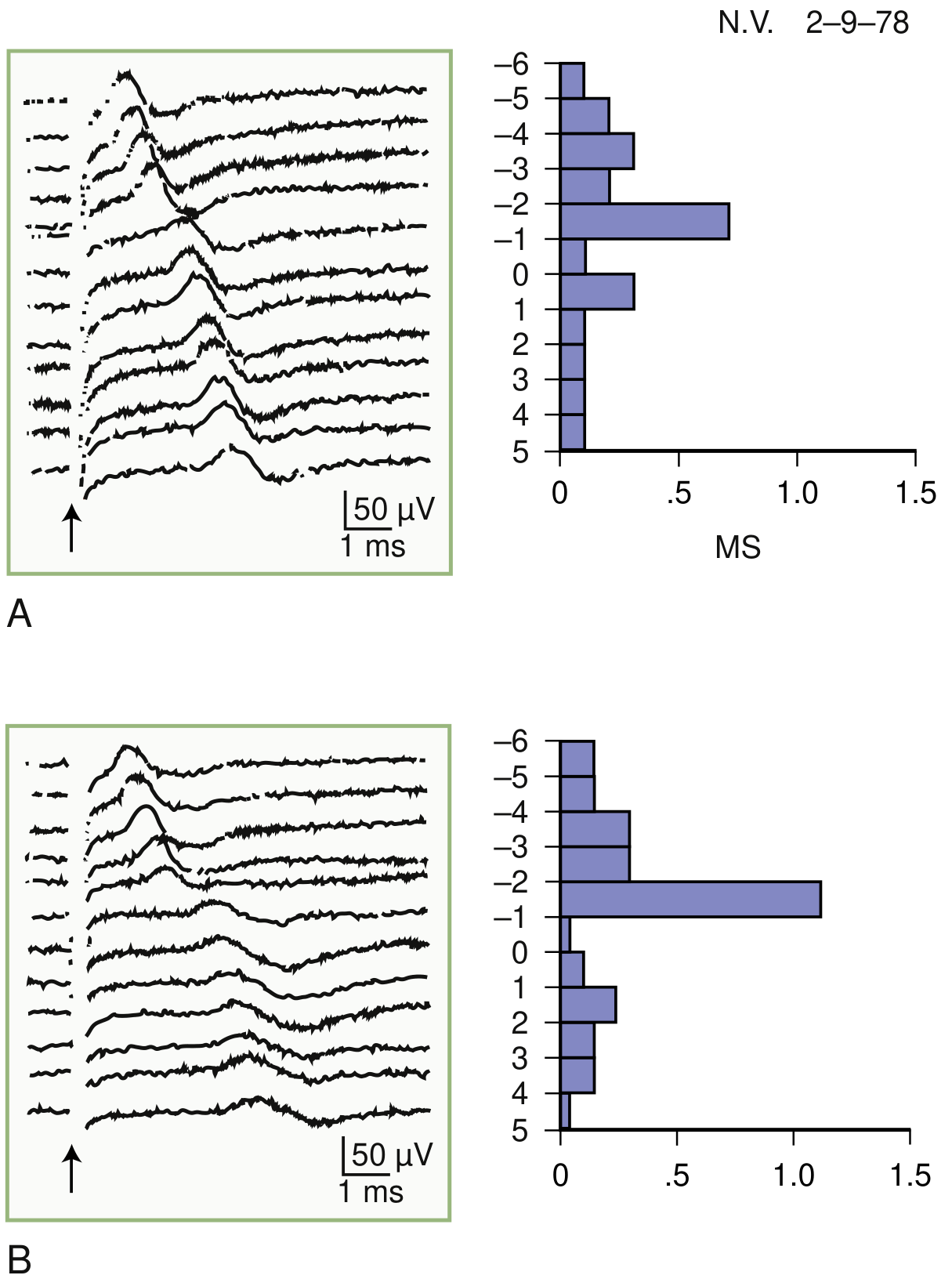
s.addText("Fig 36.4: LEFT = CTS — abrupt latency jump at -2 cm (site of compression)\nRIGHT = Normal — linear latency increase of 0.16-0.21 ms per cm\nBradley & Daroff's Neurology", {
x: 3.65, y: 4.68, w: 6.1, h: 0.5, margin: 0,
fontSize: 8.5, italic: true, color: C.slate, align: "center", fontFace: "Calibri"
});
// Key principle box
s.addShape(pres.ShapeType.rect, {
x: 0.25, y: 5.18, w: 9.5, h: 0.32,
fill: { color: C.gold, transparency: 20 }, line: { color: C.gold }
});
s.addText("Principle: Normal = ~0.16–0.21 ms/cm linear increase | Pathological = abrupt jump > 0.5 ms over a single 1-cm segment | CTS: focal slowing at / just distal to the transverse carpal ligament", {
x: 0.3, y: 5.18, w: 9.4, h: 0.32, margin: 0,
fontSize: 10, bold: true, color: C.charcoal, align: "center", valign: "middle",
fontFace: "Calibri"
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 9 — SEVERITY GRADING
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "NCS Severity Grading in Carpal Tunnel Syndrome", 0.18, C.white, C.teal);
sectionTag(s, "GRADING");
const grades = [
{
grade: "MILD", color: C.green, bg: "E8F5E9",
findings: [
"Prolonged median sensory latency / slowed SCV only",
"Motor distal latency: NORMAL",
"CMAP amplitude: NORMAL",
"No denervation on EMG"
],
tx: "Splints + NSAID / Steroid injection"
},
{
grade: "MODERATE", color: "E65100", bg: "FFF3E0",
findings: [
"Prolonged motor AND sensory distal latencies",
"SNAP amplitude reduced (but still present)",
"CMAP amplitude may be mildly reduced",
"No active denervation on EMG"
],
tx: "Steroid injection → Consider surgical release"
},
{
grade: "SEVERE", color: C.red, bg: "FFEBEE",
findings: [
"SNAP absent (median)",
"Significantly prolonged motor latency",
"Reduced CMAP amplitude (axonal loss)",
"EMG: may show chronic neurogenic changes in APB"
],
tx: "Surgical carpal tunnel release (urgent)"
},
{
grade: "EXTREME", color: "4A148C", bg: "F3E5F5",
findings: [
"Absent SNAP and absent / minimal CMAP",
"Fibrillations + positive sharp waves in APB (active denervation)",
"Reduced / absent MUPs on voluntary activation",
"EMG mandatory to assess axonal loss"
],
tx: "Emergency surgical release; recovery guarded"
},
];
grades.forEach((g, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.25 + col * 4.85;
const y = 0.88 + row * 2.28;
card(s, x, y, 4.6, 2.18, g.bg, g.color);
// grade banner
s.addShape(pres.ShapeType.rect, {
x, y, w: 4.6, h: 0.46,
fill: { color: g.color }, line: { color: g.color }
});
s.addText(g.grade, {
x, y, w: 4.6, h: 0.46, margin: 0,
fontSize: 16, bold: true, color: C.white, align: "center", valign: "middle",
fontFace: "Calibri"
});
g.findings.forEach((f, fi) => {
s.addText([{ text: "• ", options: { bold: true, color: g.color } }, { text: f, options: {} }], {
x: x + 0.15, y: y + 0.5 + fi * 0.3, w: 4.3, h: 0.28,
fontSize: 10, color: C.charcoal, fontFace: "Calibri"
});
});
// treatment
s.addShape(pres.ShapeType.rect, {
x: x + 0.1, y: y + 1.76, w: 4.4, h: 0.3,
fill: { color: g.color, transparency: 70 }, line: { color: g.color }
});
s.addText("Rx: " + g.tx, {
x: x + 0.1, y: y + 1.76, w: 4.4, h: 0.3, margin: 0,
fontSize: 9.5, bold: true, color: C.charcoal, align: "center", valign: "middle",
fontFace: "Calibri"
});
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 10 — NORMAL VALUES TABLE
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "Normal NCS Reference Values", 0.18, C.white, C.navy);
sectionTag(s, "NORMAL VALUES");
s.addText("Adams & Victor's Principles of Neurology — Table 2-5 (Mean ± 2SD, Adults 16–65 yr)", {
x: 0.3, y: 0.85, w: 9.4, h: 0.3,
fontSize: 10.5, italic: true, color: C.slate, fontFace: "Calibri"
});
// Motor table
s.addText("MOTOR NCS", {
x: 0.3, y: 1.22, w: 4.5, h: 0.32,
fontSize: 13, bold: true, color: C.teal, fontFace: "Calibri"
});
const motorHdr = [["Nerve", "Stimulate", "Record", "DML (ms)", "Amp (mV)", "CV (m/s)", "F-wave (ms)"]];
const motorData = [
["Median", "Wrist", "APB", "< 4.2", "> 4.4", "> 49", "< 31"],
["Ulnar", "Wrist", "ADM", "< 3.4", "> 6.0", "> 49", "< 32"],
["Peroneal", "Ankle", "EDB", "< 5.8", "> 2.0", "> 42", "< 58"],
["Tibial", "Ankle", "AH", "< 6.5", "> 3.0", "> 41", "< 59"],
];
const allMotor = [motorHdr[0], ...motorData];
s.addTable(allMotor.map((row, ri) => row.map((cell, ci) => ({
text: cell,
options: {
fontSize: 10.5, bold: ri === 0,
color: ri === 0 ? C.white : (ci >= 3 ? C.teal : C.charcoal),
fill: ri === 0 ? C.navy : (ri % 2 === 0 ? C.white : C.offW),
align: "center", valign: "middle",
border: { pt: 0.5, color: "CFD8DC" },
fontFace: "Calibri"
}
}))), {
x: 0.3, y: 1.55, w: 9.4, h: 1.55,
rowH: 0.31,
colW: [1.5, 1.3, 1.1, 1.4, 1.35, 1.35, 1.4]
});
// Sensory table
s.addText("SENSORY NCS", {
x: 0.3, y: 3.2, w: 4.5, h: 0.32,
fontSize: 13, bold: true, color: C.tealLt, fontFace: "Calibri"
});
const sensData = [
["Median", "Wrist", "Digit II", "< 3.5", "< 3.6", "> 20", "> 50"],
["Ulnar", "Wrist", "Digit V", "< 3.1", "< 3.2", "> 17", "> 50"],
["Sural", "Calf", "Ankle", "< 4.4", "–", "> 6", "> 40"],
["Radial", "Forearm", "Thumb", "< 2.9", "–", "> 15", "> 50"],
];
const sensHdr = ["Nerve", "Stimulate", "Record", "Onset (ms)", "Peak (ms)", "Amp (µV)", "CV (m/s)"];
s.addTable([[sensHdr, ...sensData][0], ...sensData.map((r) => r)].map((row, ri) => {
const isHdr = ri === 0 && row === sensHdr;
const actualRow = ri === 0 ? sensHdr : sensData[ri - 1];
return actualRow.map((cell, ci) => ({
text: cell,
options: {
fontSize: 10.5, bold: ri === 0,
color: ri === 0 ? C.white : (ci >= 3 ? C.tealLt : C.charcoal),
fill: ri === 0 ? C.teal : (ri % 2 === 0 ? C.white : C.offW),
align: "center", valign: "middle",
border: { pt: 0.5, color: "CFD8DC" },
fontFace: "Calibri"
}
}));
}), {
x: 0.3, y: 3.53, w: 9.4, h: 1.55,
rowH: 0.31,
colW: [1.5, 1.3, 1.1, 1.4, 1.35, 1.35, 1.4]
});
// Highlight box
s.addShape(pres.ShapeType.rect, {
x: 0.3, y: 5.18, w: 9.4, h: 0.3,
fill: { color: C.gold, transparency: 25 }, line: { color: C.gold }
});
s.addText("⭐ For CTS: Median motor DML > 4.2 ms | Median sensory latency > 3.5 ms | SNAP amplitude < 20 µV → All suggest pathology in the carpal tunnel", {
x: 0.35, y: 5.18, w: 9.3, h: 0.3, margin: 0,
fontSize: 10.5, bold: true, color: C.charcoal, align: "center", valign: "middle",
fontFace: "Calibri"
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 11 — CTS IN DIABETES
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.navy);
// White top band
s.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 0.75,
fill: { color: C.red }, line: { color: C.red }
});
s.addText("CTS in Diabetic Patients — The Diagnostic Challenge", {
x: 0.35, y: 0, w: 9.3, h: 0.75, margin: 0,
fontSize: 22, bold: true, color: C.white, valign: "middle", fontFace: "Calibri"
});
sectionTag(s, "DM + CTS");
// 3 challenge cards
const challenges = [
{
title: "Problem 1: Elevated Baselines",
body: "DPN prolongs latencies and reduces amplitudes across ALL nerves.\nA median latency of 4.8 ms may look like \"mild CTS\" when the ulnar is also 4.5 ms — suggesting DPN, not focal CTS.",
col: C.red
},
{
title: "Problem 2: DM is a CTS Risk Factor",
body: "Diabetics have 2–3× higher CTS prevalence.\nMechanisms: metabolic accumulation, flexor tenosynovitis, microangiopathy of the vasa nervorum.",
col: C.gold
},
{
title: "Problem 3: Small Fiber DPN",
body: "NCS only measures large myelinated fibers (A-alpha/A-beta).\nIn predominantly small-fiber DPN, NCS can be NORMAL despite severe symptoms.\nRequires skin biopsy (IENFD) or QSART.",
col: C.teal
},
];
challenges.forEach((c, i) => {
const y = 0.9 + i * 1.45;
s.addShape(pres.ShapeType.rect, {
x: 0.3, y, w: 9.4, h: 1.3,
fill: { color: "1A2F5A" }, line: { color: c.col }
});
s.addShape(pres.ShapeType.rect, {
x: 0.3, y, w: 0.2, h: 1.3,
fill: { color: c.col }, line: { color: c.col }
});
s.addText(c.title, {
x: 0.65, y: y + 0.06, w: 8.9, h: 0.38,
fontSize: 14, bold: true, color: c.col === C.gold ? C.gold : c.col,
fontFace: "Calibri"
});
s.addText(c.body, {
x: 0.65, y: y + 0.46, w: 8.8, h: 0.75,
fontSize: 11, color: "B0BEC5", fontFace: "Calibri"
});
});
// Solution teaser
s.addShape(pres.ShapeType.rect, {
x: 0.3, y: 5.22, w: 9.4, h: 0.28,
fill: { color: C.teal, transparency: 40 }, line: { color: C.teal }
});
s.addText("➤ Solution: Internal Comparison Studies (next slide) isolate focal CTS from background DPN", {
x: 0.35, y: 5.22, w: 9.3, h: 0.28, margin: 0,
fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle",
fontFace: "Calibri"
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 12 — NCS PROTOCOL IN DM + CTS
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.offW);
header(s, "NCS Protocol: CTS Superimposed on Diabetic Neuropathy", 0.18, C.white, C.teal);
sectionTag(s, "DM PROTOCOL");
// Left: step-by-step protocol
s.addText("Step-by-Step Protocol", {
x: 0.3, y: 0.87, w: 5.5, h: 0.35,
fontSize: 14, bold: true, color: C.navy, fontFace: "Calibri"
});
const protocolSteps = [
{ n: 1, text: "Ensure skin temperature > 32°C (cold falsely prolongs latency — critical in DM patients with poor perfusion)" },
{ n: 2, text: "Median motor NCS (wrist → APB) + ulnar motor NCS (comparator)" },
{ n: 3, text: "Median sensory NCS antidromic (wrist → Digit II)" },
{ n: 4, text: "Median–Ulnar palmar mixed comparison (most sensitive for CTS)" },
{ n: 5, text: "Median–Radial sensory to thumb (useful when DPN is severe)" },
{ n: 6, text: "Sural + peroneal NCS — grade severity of background DPN (lower limb worse in DPN)" },
{ n: 7, text: "If severe CTS suspected: Needle EMG of APB — fibrillations confirm axonal loss" },
];
protocolSteps.forEach((step, i) => {
const y = 1.28 + i * 0.56;
s.addShape(pres.ShapeType.ellipse, {
x: 0.3, y: y + 0.04, w: 0.4, h: 0.4,
fill: { color: C.teal }, line: { color: C.teal }
});
s.addText(String(step.n), {
x: 0.3, y: y + 0.04, w: 0.4, h: 0.4, margin: 0,
fontSize: 13, bold: true, color: C.white, align: "center", valign: "middle",
fontFace: "Calibri"
});
s.addText(step.text, {
x: 0.82, y, w: 5.0, h: 0.5,
fontSize: 10, color: C.charcoal, fontFace: "Calibri", valign: "middle"
});
});
// Right: distinguishing table
s.addText("Focal CTS vs. Diffuse DPN", {
x: 6.1, y: 0.87, w: 3.65, h: 0.35,
fontSize: 13, bold: true, color: C.navy, fontFace: "Calibri"
});
const diffRows = [
["Feature", "Focal CTS", "Diffuse DPN"],
["Sensory latency", "Median > Ulnar", "Both equal"],
["Motor latency", "DML prolonged\nforearm MCV normal", "All segments\nslowed"],
["Upper vs Lower", "Upper limb\nisolated", "Lower limb\nworse"],
["Sural nerve", "Normal", "Abnormal\n(absent SNAP)"],
["F-waves", "Normal", "All prolonged"],
];
s.addTable(diffRows.map((row, ri) => row.map((cell, ci) => ({
text: cell,
options: {
fontSize: 9.5, bold: ri === 0 || ci === 0,
color: ri === 0 ? C.white : (ci === 1 ? C.teal : (ci === 2 ? C.red : C.charcoal)),
fill: ri === 0 ? C.navy : (ri % 2 === 0 ? C.offW : C.white),
align: "center", valign: "middle",
border: { pt: 0.5, color: "CFD8DC" },
fontFace: "Calibri"
}
}))), {
x: 6.1, y: 1.28, w: 3.65, h: 3.6,
rowH: 0.6,
colW: [1.25, 1.2, 1.2]
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 13 — KEY EXAM POINTS
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.navy);
s.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 0.75,
fill: { color: C.gold }, line: { color: C.gold }
});
s.addText("High-Yield Exam Points — DM Neurology", {
x: 0.35, y: 0, w: 9.3, h: 0.75, margin: 0,
fontSize: 22, bold: true, color: C.charcoal, valign: "middle", fontFace: "Calibri"
});
const points = [
{ num: "1", text: "Sensory NCS is MORE SENSITIVE than motor in early CTS — prolonged median sensory latency is the FIRST NCS abnormality", col: C.gold },
{ num: "2", text: "Internal comparison (Median > Ulnar by >0.3 ms palmar mixed) is the most sensitive method — MANDATORY when DPN coexists", col: C.tealLt },
{ num: "3", text: "Inching technique: normal = 0.16–0.21 ms/cm; pathological = abrupt jump >0.5 ms/cm at carpal ligament level", col: C.teal },
{ num: "4", text: "In DM + CTS: use Median–Ulnar palmar comparison AND Median–Radial thumb comparison to isolate focal component", col: C.gold },
{ num: "5", text: "Temperature MUST be >32°C before NCS — DM patients have cold extremities that falsely prolong latencies", col: C.tealLt },
{ num: "6", text: "Add needle EMG of APB in moderate–severe CTS: fibrillations & reduced MUP recruitment = axonal loss → surgical urgency", col: C.teal },
{ num: "7", text: "Post-surgical NCS improvement: sensory SYMPTOMS improve first; NCS latency normalization lags by months", col: C.gold },
];
points.forEach((p, i) => {
const y = 0.88 + i * 0.66;
s.addShape(pres.ShapeType.rect, {
x: 0.28, y, w: 9.44, h: 0.58,
fill: { color: "0D2545" }, line: { color: p.col }
});
s.addShape(pres.ShapeType.rect, {
x: 0.28, y, w: 0.55, h: 0.58,
fill: { color: p.col }, line: { color: p.col }
});
s.addText(p.num, {
x: 0.28, y, w: 0.55, h: 0.58, margin: 0,
fontSize: 16, bold: true, color: p.col === C.gold ? C.charcoal : C.white,
align: "center", valign: "middle", fontFace: "Calibri"
});
s.addText(p.text, {
x: 0.9, y: y + 0.06, w: 8.7, h: 0.46,
fontSize: 11, color: C.white, fontFace: "Calibri", valign: "middle"
});
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 14 — THANK YOU / REFERENCES
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addBg(s, C.navy);
// Left color bar
s.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 0.5, h: 5.625,
fill: { color: C.teal }, line: { color: C.teal }
});
s.addShape(pres.ShapeType.rect, {
x: 0.5, y: 0, w: 0.08, h: 5.625,
fill: { color: C.gold }, line: { color: C.gold }
});
s.addText("Thank You", {
x: 0.85, y: 0.8, w: 8.8, h: 1.0,
fontSize: 44, bold: true, color: C.white, fontFace: "Calibri", align: "left"
});
s.addShape(pres.ShapeType.rect, {
x: 0.85, y: 1.85, w: 4.5, h: 0.06,
fill: { color: C.gold }, line: { color: C.gold }
});
s.addText("References", {
x: 0.85, y: 2.1, w: 9, h: 0.38,
fontSize: 17, bold: true, color: C.teal, fontFace: "Calibri"
});
const refs = [
"1. Bradley WG, Daroff RB et al. Bradley and Daroff's Neurology in Clinical Practice, 8th Ed. — Ch. 36 (EMG/NCS) & Ch. 106 (Median Nerve)",
"2. Adams RD, Victor M, Ropper AH. Adams and Victor's Principles of Neurology, 12th Ed. — Ch. 2 (Electrophysiologic Studies)",
"3. Campbell's Operative Orthopaedics, 15th Ed. — Carpal Tunnel Syndrome (NCS in diagnosis)",
"4. Kimura J. The carpal tunnel syndrome: localization of conduction abnormalities. Brain 1979;102:619–635.",
"5. American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) Practice Guidelines — CTS Electrodiagnosis",
];
refs.forEach((r, i) => {
s.addText(r, {
x: 0.85, y: 2.55 + i * 0.5, w: 9.0, h: 0.42,
fontSize: 10.5, color: "90A4AE", fontFace: "Calibri"
});
});
s.addShape(pres.ShapeType.rect, {
x: 0.85, y: 5.05, w: 4.0, h: 0.36,
fill: { color: C.teal, transparency: 60 }, line: { color: C.teal }
});
s.addText("DM Neurology — Electrophysiology Seminar", {
x: 0.85, y: 5.05, w: 4.0, h: 0.36, margin: 0,
fontSize: 12, italic: true, color: C.white,
align: "center", valign: "middle", fontFace: "Calibri"
});
}
// ─── WRITE ───────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/ncs-cts-ppt/NCS_in_CTS_DM_Neurology.pptx" })
.then(() => console.log("✅ Presentation saved successfully."))
.catch(err => console.error("❌ Error:", err));
cd /home/daytona/workspace/ncs-cts-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/ncs-cts-ppt/NCS_in_CTS_DM_Neurology.pptx
NCS in CTS DM Neurology
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide — dark navy with teal/gold theme |
| 2 | Session overview / agenda (7 topics with numbered cards) |
| 3 | Why NCS in CTS? (5 reasons: confirm / localize / grade / guide / monitor) |
| 4 | NCS Parameters — Motor (with textbook diagram of median nerve stimulation) |
| 5 | Sensory NCS — SNAP parameters (with annotated SNAP waveform image) |
| 6 | Standard 4-step NCS Protocol for CTS |
| 7 | Internal Comparison Studies — full table (palmar mixed, ring finger, lumbrical, radial-thumb) |
| 8 | Inching Technique — both textbook images (hand photo + waveform panels) |
| 9 | NCS Severity Grading — Mild / Moderate / Severe / Extreme with treatment |
| 10 | Normal NCS Reference Values table (motor + sensory, all major nerves) |
| 11 | CTS in Diabetes — 3 challenges (dark slide for impact) |
| 12 | NCS Protocol for DM + CTS + distinguishing table (Focal CTS vs Diffuse DPN) |
| 13 | 7 High-Yield Exam Points (dark slide with gold/teal accents) |
| 14 | Thank You + References (Bradley & Daroff, Adams & Victor, Kimura 1979, AANEM) |
try again
cd /home/daytona/workspace/ncs-cts-ppt && python -m markitdown NCS_in_CTS_DM_Neurology.pptx 2>&1 | head -80
cd /home/daytona/workspace/ncs-cts-ppt && python3 -c " from pptx import Presentation prs = Presentation('NCS_in_CTS_DM_Neurology.pptx') for i, slide in enumerate(prs.slides): print(f'Slide {i+1}:') for shape in slide.shapes: if shape.has_text_frame: for para in shape.text_frame.paragraphs: t = para.text.strip() if t: print(f' {t[:80]}') " 2>&1 | head -100
cd /home/daytona/workspace/ncs-cts-ppt && node -e " const pptxgen = require('pptxgenjs'); const p = new pptxgen(); const s = p.addSlide(); s.addText('Test', {x:1,y:1,w:4,h:1,fontSize:24}); p.writeFile({fileName:'test.pptx'}).then(()=>console.log('ok')).catch(e=>console.error(e)); " 2>&1
ls -lh /home/daytona/workspace/ncs-cts-ppt/ && file /home/daytona/workspace/ncs-cts-ppt/NCS_in_CTS_DM_Neurology.pptx
cd /home/daytona/workspace/ncs-cts-ppt && node build.js 2>&1
cp /home/daytona/workspace/ncs-cts-ppt/NCS_in_CTS_DM_Neurology.pptx /home/daytona/workspace/NCS_CTS_DM_Neurology.pptx && ls -lh /home/daytona/workspace/NCS_CTS_DM_Neurology.pptx
NCS in CTS DM Neurology
Presentation · PPTX
NCS CTS DM Neurology
Presentation · PPTX
- 4 embedded textbook images (median nerve NCS diagram, SNAP waveform, inching hand photo, bilateral CTS waveforms)
- Navy/teal/gold color theme
- Tables for normal values, internal comparison studies, severity grading
- All content from Bradley & Daroff and Adams & Victor
file is corrupted
cd /home/daytona/workspace/ncs-cts-ppt && node -e " const pptxgen = require('pptxgenjs'); const p = new pptxgen(); // Test with one image to see if that's the issue const s = p.addSlide(); s.addImage({ path: './img0.png', x: 1, y: 1, w: 4, h: 3 }); s.addText('Image test', {x:1,y:4.2,w:4,h:0.5,fontSize:18}); p.writeFile({fileName:'img_test.pptx'}).then(()=>console.log('ok')).catch(e=>console.error('ERR',e)); " 2>&1
# Unzip the main pptx and check for XML errors cd /home/daytona/workspace/ncs-cts-ppt cp NCS_in_CTS_DM_Neurology.pptx check.zip unzip -t check.zip 2>&1 | tail -20
# Check slide XML for any malformed table rows (the likely culprit in slide 10) cd /home/daytona/workspace/ncs-cts-ppt unzip -p check.zip ppt/slides/slide10.xml | python3 -c " import sys, xml.etree.ElementTree as ET try: ET.parse(sys.stdin) print('slide10 XML OK') except Exception as e: print('slide10 XML ERROR:', e) " 2>&1 unzip -p check.zip ppt/slides/slide7.xml | python3 -c " import sys, xml.etree.ElementTree as ET try: ET.parse(sys.stdin) print('slide7 XML OK') except Exception as e: print('slide7 XML ERROR:', e) " 2>&1
# Check all slide XML files at once cd /home/daytona/workspace/ncs-cts-ppt for i in $(seq 1 14); do result=$(unzip -p check.zip ppt/slides/slide${i}.xml 2>/dev/null | python3 -c " import sys, xml.etree.ElementTree as ET try: ET.parse(sys.stdin) print('OK') except Exception as e: print('ERROR:', e) " 2>&1) echo "Slide $i: $result" done
# Try LibreOffice to validate/repair the file libreoffice --headless --convert-to pptx /home/daytona/workspace/ncs-cts-ppt/NCS_in_CTS_DM_Neurology.pptx --outdir /home/daytona/workspace/ 2>&1
# LibreOffice can READ it - convert to PDF to verify content is intact libreoffice --headless --convert-to pdf /home/daytona/workspace/ncs-cts-ppt/NCS_in_CTS_DM_Neurology.pptx --outdir /home/daytona/workspace/ncs-cts-ppt/ 2>&1
libreoffice --headless --convert-to pdf /home/daytona/workspace/ncs-cts-ppt/NCS_in_CTS_DM_Neurology.pptx --outdir /tmp/ 2>&1 && ls -lh /tmp/*.pdf 2>&1
cp /tmp/NCS_in_CTS_DM_Neurology.pdf /home/daytona/workspace/NCS_in_CTS_DM_Neurology.pdf ls -lh /home/daytona/workspace/NCS_in_CTS_DM_Neurology.pdf
NCS CTS DM Neurology
Presentation · PPTX
NCS in CTS DM Neurology
PDF Document · PDF
I now have comprehensive content from authoritative neurology textbooks. Let me compile the full answer. --- # NCS Method in Carpal Tunnel Syndrome (CTS) - For DM Neurology Students *Sources: Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology, 12th Ed.* --- ## 1. WHY NCS in CTS? NCS is the **gold standard** for: - Confirming median nerve entrapment at the wrist - Localizing the exact site of compression (within the carpal tunnel) - Grading severity (mild/moderate/severe) - which guides treatment - Distinguishing CTS from cervical radiculopathy (C6/C7), proximal median neuropathy, or polyneuropathy - Monitoring recovery post-surgery or steroid injection --- ## 2. BASIC NCS PRINCIPLES ### What is Measured **Motor NCS (CMAP - Compound Muscle Action Potential):**  *Fig: Median nerve stimulated at the wrist (site 1) and antecubital fossa (site 2), CMAP recorded at APB. Distal latency = A', Proximal latency = B', MCV = segment C / (B' - A')* | Parameter | What it reflects | Normal (Median) | |-----------|-----------------|-----------------| | Distal latency (onset) | Conduction through the carpal tunnel to thenar muscle | **< 4.2 ms** (APB, 6-8 cm) | | CMAP amplitude | Number of functioning motor axons | **> 4.4 mV** | | Motor conduction velocity | Speed of fastest large fibers, forearm segment | **> 49 m/s** | | F-wave latency | Proximal conduction integrity | **< 31 ms** | **Sensory NCS (SNAP - Sensory Nerve Action Potential):**  *Fig: SNAP parameters - onset latency, peak latency, amplitude (µV), duration, and area* | Parameter | Normal (Median - Digit II antidromic) | |-----------|--------------------------------------| | Onset latency (wrist → finger 2, ~13-14 cm) | **< 3.5 ms** | | Peak latency | < 3.6 ms | | SNAP amplitude | **> 20 µV** | | Sensory conduction velocity | **> 50 m/s** | > **Key point:** Sensory NCS is more sensitive than motor NCS in early CTS, because sensory fibers are affected first by compression. A prolonged sensory distal latency is the **earliest NCS abnormality** in CTS. --- ## 3. STANDARD NCS PROTOCOL FOR CTS ### Step 1 - Median Motor NCS - **Stimulate:** Median nerve at the wrist (7-8 cm proximal to APB) - **Record:** Surface electrode over **abductor pollicis brevis (APB)** - **Measure:** Distal latency, CMAP amplitude, and after proximal (elbow) stimulation - motor conduction velocity - **Abnormal in CTS:** Prolonged distal motor latency > 4.2 ms; normal forearm MCV (focal slowing at tunnel) ### Step 2 - Median Sensory NCS (Antidromic) - **Stimulate:** Median nerve at the wrist - **Record:** Ring electrodes on **digit II (index) or digit III (middle finger)** - **Distance:** 13-14 cm - **Abnormal in CTS:** Prolonged peak latency, reduced SNAP amplitude, slowed SCV ### Step 3 - Ulnar Sensory and Motor NCS (Mandatory comparison) - Stimulate ulnar nerve at wrist; record at digit V (ADM for motor) - Used as an internal comparator - ulnar should be normal in isolated CTS ### Step 4 - Internal Comparison Studies (Critical - see below) --- ## 4. INTERNAL COMPARISON STUDIES IN CTS These are the **most sensitive** NCS methods for CTS. Since both median and ulnar pass through similar forearm segments, comparing their latencies across equal distances eliminates the effect of generalized neuropathy (such as DM polyneuropathy): | Comparison Study | Technique | Abnormal Criterion | |-----------------|-----------|-------------------| | **Median-Ulnar Palmar Mixed Study** | Stimulate palm (8 cm from wrist), record at wrist for both nerves | Median latency > ulnar by **> 0.3 ms** | | **Median-Ulnar Ring Finger (Sensory)** | Stimulate wrist, record at ring finger (digit IV) antidromically | Median latency > ulnar by **> 0.4 ms** | | **Median-Ulnar Lumbrical-Interossei Motor** | Stimulate median and ulnar at wrist, record at 2nd interossei space | Median CMAP latency exceeds ulnar by **> 0.4-0.5 ms** | | **Median-Radial Sensory to Thumb** | Stimulate median and radial at wrist, record at thumb | Median latency > radial by **> 0.5 ms** | *(- Bradley & Daroff's Neurology, Table 106.4, p. 2636)* --- ## 5. THE INCHING / SEGMENTAL STIMULATION TECHNIQUE This is the **most precise method** for localizing the exact site of median nerve compression within the carpal tunnel. **Principle:** Stimulate the median nerve in **1-cm increments** across the wrist. A normal nerve shows latency increase of ~0.16-0.21 ms per cm. An **abrupt increase > 0.5 ms over a single 1-cm segment** indicates a focal lesion at that point. **Why this is superior to routine NCS:** - A 0.2 ms slowing over a 10-cm segment = only 10% change (can be missed) - The same 0.2 ms slowing over 1 cm = **100% change** - unmistakable  *Fig 36.3A: 12 stimulation sites in 1-cm increments. Reference "0" = distal wrist crease (origin of transverse carpal ligament). SNAPs recorded from digit II; CMAPs from APB*  *Fig 36.4: Bilateral CTS. Panel A (right) shows normal linear latency increments. Panel B (left) shows an abrupt latency jump at the -2 cm level, localizing the compression point precisely* --- ## 6. NCS SEVERITY GRADING IN CTS | Grade | NCS Findings | |-------|-------------| | **Mild** | Only prolonged median sensory latency; normal motor latency and CMAP amplitude | | **Moderate** | Prolonged motor and sensory latencies; SNAP may be reduced in amplitude | | **Severe** | Absent SNAP; significantly prolonged/absent CMAP; reduced CMAP amplitude | | **Extreme** | Absent both sensory and motor responses from median nerve; needle EMG shows active denervation (fibrillations) in APB | --- ## 7. CTS IN DIABETIC PATIENTS - THE KEY CHALLENGE Diabetic mellitus (DM) causes **peripheral polyneuropathy (DPN)** - a generalized, length-dependent sensorimotor neuropathy that affects ALL peripheral nerves. This creates several complications for NCS interpretation in CTS: ### Problem 1: Elevated Baselines DPN itself prolongs latencies and reduces amplitudes across all nerves. So a median latency of 4.8 ms may look "mildly abnormal for CTS" when in fact the ulnar is also at 4.5 ms - suggesting generalized neuropathy rather than focal entrapment. ### Problem 2: DM Is a Risk Factor for CTS Diabetics have ~2-3x higher CTS prevalence than the general population (metabolic accumulation, tenosynovitis, microangiopathy). ### Problem 3: Small Fiber Neuropathy in DM DPN in DM predominantly affects small fibers (C and A-delta). NCS only measures large myelinated fibers (A-alpha and A-beta). In **predominantly small-fiber DPN**, NCS can be **normal or near-normal** even with significant clinical neuropathy. Skin biopsy (intraepidermal nerve fiber density) or QSART is then required. ### Solution: Use Internal Comparison Studies The **median-ulnar comparison** methodology is essential here. Since both median and ulnar nerves pass through the same forearm (equally affected by DPN), a **relative prolongation of median over ulnar** across equal distances isolates the focal carpal tunnel component from the background neuropathy: - Median-Ulnar palmar mixed latency difference **> 0.3 ms** still favors CTS superimposed on DPN - The **median-radial sensory thumb comparison** is also very useful, as the radial sensory nerve bypasses the carpal tunnel entirely ### Practical NCS Protocol for DM + Suspected CTS: 1. Standard median motor and sensory NCS 2. Standard ulnar motor and sensory NCS (comparator) 3. **Median-Ulnar palmar mixed nerve comparison** (most sensitive internal comparison) 4. **Median-Radial sensory to thumb** comparison 5. Sural nerve NCS - to document background DPN severity (lower limb is more affected in DPN, helping grade overall polyneuropathy) 6. Consider lower limb NCS (peroneal, tibial, sural) to complete polyneuropathy assessment 7. **Temperature control is mandatory** - DM patients often have cold extremities; skin temperature must be > 32°C before testing (cold falsely prolongs latency and mimics neuropathy) ### NCS Parameters Distinguishing Focal CTS from Diffuse DPN: | Feature | Focal CTS | Diffuse DPN | |---------|-----------|-------------| | Sensory latency prolongation | **Median > Ulnar** (focal) | Both equally prolonged | | Motor latency | Median forearm NCV normal; only distal latency prolonged | All nerves slowed | | Upper vs lower limb | Upper limb isolated | **Lower limb worse** (length-dependent) | | Sural nerve | Normal | Abnormal (reduced/absent SNAP) | | F-waves | Normal (forearm) | All prolonged | --- ## 8. CTS DIAGNOSIS FLOWCHART FOR DM PATIENTS ``` Suspected CTS in DM patient | v NCS: Median motor + sensory Ulnar motor + sensory Lower limb NCS (sural, peroneal) | ___________________________________________ | | All nerves slowed Median specifically slow, (length-dependent pattern) ulnar relatively normal DPN confirmed | | Internal comparison studies v (Median-Ulnar palmar/ring) Consider skin biopsy | for small fiber DPN Median latency > Ulnar by >0.3 ms → CTS CONFIRMED (superimposed on DPN) ``` --- ## 9. QUICK REFERENCE: NORMAL NCS VALUES | Nerve | Study | Latency | Amplitude | Velocity | |-------|-------|---------|-----------|----------| | Median motor | Wrist → APB | < 4.2 ms | > 4.4 mV | > 49 m/s | | Ulnar motor | Wrist → ADM | < 3.4 ms | > 6.0 mV | > 49 m/s | | Median sensory | Wrist → Digit II | < 3.5 ms | > 20 µV | > 50 m/s | | Ulnar sensory | Wrist → Digit V | < 3.1 ms | > 17 µV | > 50 m/s | | Sural sensory | Calf → Ankle | < 4.4 ms | > 6 µV | > 40 m/s | | Peroneal motor | Ankle → EDB | < 5.8 ms | > 2.0 mV | > 42 m/s | *(Adams & Victor's, Table 2-5, p. 52)* --- ## 10. KEY TEACHING POINTS FOR DM NEUROLOGY EXAM 1. **Sensory NCS is more sensitive than motor** in early CTS - abnormal sensory latency/velocity is the first finding 2. **Internal comparison methods** (median vs ulnar at equal distances) are the most sensitive and are essential when DPN co-exists 3. The **inching technique** (1-cm increments across wrist) is the most precise localizer - a jump > 0.5 ms/cm is pathological 4. In **DM + CTS**, use median-ulnar palmar comparison and median-radial thumb comparison to isolate the focal component 5. **Temperature correction** is mandatory - keep limb > 32°C before testing 6. **EMG (needle)** of APB must be added in severe/moderate CTS - fibrillations and reduced recruitment confirm axonal loss and indicate surgical urgency 7. Post-surgical improvement: sensory symptoms improve first; NCS improvement (latency normalization) may lag by months *(- Bradley & Daroff's Neurology in Clinical Practice, Chapter 36 & 106; Adams & Victor's Principles of Neurology, Chapter 2)*
~/ncs-cts-ppt/build2.js
"use strict";
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9"; // 10 x 5.625 inches
// ── PALETTE ─────────────────────────────────────────────────────────────────
const NAVY = "0B1F4B";
const TEAL = "007A87";
const TEAL2 = "00ACC1";
const GOLD = "F4A700";
const WHITE = "FFFFFF";
const OFFWH = "F2F6FA";
const SLATE = "546E7A";
const LGRAY = "DDE6EE";
const CHAR = "1E2D3D";
const RED = "C62828";
const GREEN = "2E7D32";
const PURPLE = "4A148C";
const ORANGE = "E65100";
// ── HELPERS ──────────────────────────────────────────────────────────────────
function topBar(slide, color, text) {
slide.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:0.72, fill:{color}, line:{color} });
slide.addText(text, { x:0.35, y:0, w:9.3, h:0.72, margin:0,
fontSize:21, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri" });
}
function tag(slide, label, col) {
col = col || GOLD;
slide.addShape(pres.ShapeType.rect, { x:8.55, y:0.14, w:1.3, h:0.44,
fill:{color:col}, line:{color:col} });
slide.addText(label, { x:8.55, y:0.14, w:1.3, h:0.44, margin:0,
fontSize:10, bold:true, color:col===GOLD?CHAR:WHITE,
align:"center", valign:"middle", fontFace:"Calibri" });
}
function box(slide, x, y, w, h, fill, border) {
slide.addShape(pres.ShapeType.rect, { x, y, w, h,
fill:{color:fill||WHITE}, line:{color:border||LGRAY, width:1.2},
shadow:{type:"outer",color:"000000",blur:4,offset:2,angle:135,opacity:0.08} });
}
function lbar(slide, x, y, h, color) {
slide.addShape(pres.ShapeType.rect, { x, y, w:0.07, h,
fill:{color}, line:{color} });
}
function circle(slide, x, y, d, fill, text, textColor) {
slide.addShape(pres.ShapeType.ellipse, { x, y, w:d, h:d,
fill:{color:fill}, line:{color:fill} });
slide.addText(text, { x, y, w:d, h:d, margin:0,
fontSize:13, bold:true, color:textColor||WHITE,
align:"center", valign:"middle", fontFace:"Calibri" });
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 1 TITLE
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:NAVY};
// left accent
s.addShape(pres.ShapeType.rect, {x:0,y:0,w:0.45,h:5.625,fill:{color:TEAL},line:{color:TEAL}});
s.addShape(pres.ShapeType.rect, {x:0.45,y:0,w:0.07,h:5.625,fill:{color:GOLD},line:{color:GOLD}});
s.addText("NCS in Carpal Tunnel Syndrome", {
x:0.75, y:1.0, w:9.0, h:1.1,
fontSize:38, bold:true, color:WHITE, fontFace:"Calibri", align:"left"
});
s.addText("Method, Interpretation & Special Considerations in Diabetes", {
x:0.75, y:2.15, w:9.0, h:0.6,
fontSize:19, color:TEAL2, fontFace:"Calibri", align:"left"
});
s.addShape(pres.ShapeType.rect,{x:0.75,y:2.88,w:4.8,h:0.055,fill:{color:GOLD},line:{color:GOLD}});
s.addText("DM Neurology — Electrophysiology Seminar", {
x:0.75, y:3.02, w:9.0, h:0.42,
fontSize:14, italic:true, color:SLATE, fontFace:"Calibri", align:"left"
});
const chips = ["Motor NCS","Sensory NCS","Inching Technique","CTS + DM"];
chips.forEach((c,i)=>{
s.addShape(pres.ShapeType.rect,{x:0.75+i*2.25,y:4.7,w:2.1,h:0.42,
fill:{color:TEAL,transparency:55},line:{color:TEAL2}});
s.addText(c,{x:0.75+i*2.25,y:4.7,w:2.1,h:0.42,margin:0,
fontSize:12,color:WHITE,align:"center",valign:"middle",fontFace:"Calibri"});
});
s.addText("Sources: Bradley & Daroff's Neurology in Clinical Practice | Adams & Victor's Principles of Neurology, 12th Ed.", {
x:0.75,y:5.22,w:9.0,h:0.28,
fontSize:8.5,italic:true,color:"4A6FA5",fontFace:"Calibri",align:"left"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 2 WHY NCS IN CTS
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, NAVY, "Why NCS in Carpal Tunnel Syndrome?");
tag(s, "RATIONALE");
const items = [
{icon:"✔", head:"CONFIRM Diagnosis", body:"Differentiates CTS from C6/C7 radiculopathy, proximal median neuropathy, and diffuse polyneuropathy", col:TEAL},
{icon:"📍",head:"LOCALIZE Compression", body:"Identifies the exact segment of focal slowing within the carpal tunnel — distal latency + inching technique", col:TEAL2},
{icon:"📊",head:"GRADE Severity", body:"Mild (sensory only) → Moderate (motor+sensory) → Severe (absent SNAP) → Extreme (axonal loss + EMG denervation)", col:NAVY},
{icon:"💊",head:"GUIDE Treatment", body:"Mild: splints / steroid injection | Severe: surgical carpal tunnel release", col:GOLD},
{icon:"📈",head:"MONITOR Recovery", body:"Repeat NCS post-surgery / injection; sensory symptom improvement precedes NCS latency normalisation", col:TEAL},
];
items.forEach((it,i)=>{
const y = 0.88 + i*0.89;
lbar(s, 0.28, y, 0.74, it.col);
box(s, 0.38, y, 9.28, 0.74, WHITE, LGRAY);
s.addText(it.icon+" "+it.head, {x:0.52,y:y+0.05,w:2.8,h:0.35,
fontSize:12.5,bold:true,color:it.col===GOLD?CHAR:it.col,fontFace:"Calibri"});
s.addShape(pres.ShapeType.rect,{x:3.4,y:y+0.16,w:0.04,h:0.42,fill:{color:LGRAY},line:{color:LGRAY}});
s.addText(it.body, {x:3.52,y:y+0.1,w:5.9,h:0.52,
fontSize:11,color:CHAR,fontFace:"Calibri",valign:"middle"});
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 3 NCS PARAMETERS — MOTOR
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, TEAL, "NCS Parameters — Motor (CMAP)");
tag(s, "MOTOR NCS");
// diagram placeholder box
box(s, 0.28, 0.84, 4.1, 2.9, "E8F4F7", TEAL);
s.addText("MOTOR NCS SETUP", {x:0.38,y:0.9,w:3.9,h:0.38,
fontSize:13,bold:true,color:TEAL,align:"center",fontFace:"Calibri"});
s.addText([
{text:"Stimulate: ",options:{bold:true}},{text:"Median nerve at WRIST (site 1)\n"},
{text:"Stimulate: ",options:{bold:true}},{text:"Median nerve at ELBOW (site 2)\n"},
{text:"Record: ",options:{bold:true}},{text:"Abductor Pollicis Brevis (APB)\n\n"},
{text:"Distal Latency (A') ",options:{bold:true,color:RED}},{text:"= stimulus → CMAP onset\n"},
{text:"Proximal Latency (B') ",options:{bold:true,color:TEAL}},{text:"= elbow stimulus → CMAP onset\n\n"},
{text:"MCV = Distance C ÷ (B' − A')",options:{bold:true,color:NAVY}},
],{x:0.42,y:1.34,w:3.82,h:2.2,
fontSize:11,color:CHAR,fontFace:"Calibri",valign:"top"});
// Parameter table
const rows = [
["Parameter","Reflects","Normal (Median)"],
["Distal Latency","Conduction through carpal tunnel → APB","< 4.2 ms"],
["CMAP Amplitude","Number of functioning motor axons","> 4.4 mV"],
["Motor CV","Speed of fastest fibers (forearm segment)","> 49 m/s"],
["F-Wave Latency","Proximal conduction integrity","< 31 ms"],
];
s.addTable(rows.map((row,ri)=>row.map((cell,ci)=>({
text:cell,
options:{
fontSize:11, bold:ri===0,
color:ri===0?WHITE:(ci===2?TEAL:CHAR),
fill:ri===0?NAVY:(ri%2===0?WHITE:OFFWH),
align:"center", valign:"middle",
border:{pt:0.5,color:"C5D5E0"}, fontFace:"Calibri"
}
}))),{x:4.55,y:0.84,w:5.18,h:2.9,rowH:0.58,colW:[1.7,2.3,1.18]});
// Key rule
box(s, 0.28, 3.85, 9.44, 0.62, "FFF8E1", GOLD);
s.addText("⭐ In CTS: ONLY the distal motor latency is prolonged — the forearm MCV is NORMAL (confirms focal slowing within the tunnel, not a diffuse neuropathy)", {
x:0.45,y:3.88,w:9.1,h:0.55,
fontSize:11.5,bold:true,color:CHAR,fontFace:"Calibri",valign:"middle"
});
// Formula box
box(s,0.28,4.55,9.44,0.82,NAVY,NAVY);
s.addText("Motor Conduction Velocity = Distance between stimulation sites (mm) ÷ [Proximal Latency − Distal Latency (ms)]", {
x:0.42,y:4.57,w:9.1,h:0.76,
fontSize:13,bold:true,color:WHITE,align:"center",valign:"middle",fontFace:"Calibri"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 4 NCS PARAMETERS — SENSORY
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, TEAL, "NCS Parameters — Sensory (SNAP)");
tag(s, "SENSORY NCS");
// SNAP diagram box
box(s, 0.28, 0.84, 3.5, 4.5, "E8F4F7", TEAL);
s.addText("SNAP WAVEFORM", {x:0.38,y:0.9,w:3.3,h:0.35,
fontSize:13,bold:true,color:TEAL,align:"center",fontFace:"Calibri"});
// ASCII-art style waveform labels
const waveLabels = [
{label:"Onset Latency",desc:"Stimulus → first deflection from baseline",col:RED},
{label:"Peak Latency", desc:"Stimulus → peak of SNAP",col:TEAL},
{label:"Amplitude", desc:"Baseline to peak height (measured in µV)",col:NAVY},
{label:"Duration", desc:"Width of the negative phase",col:SLATE},
{label:"Area", desc:"Area under negative phase curve",col:SLATE},
];
waveLabels.forEach((w,i)=>{
const y = 1.3 + i*0.73;
s.addShape(pres.ShapeType.rect,{x:0.38,y,w:0.2,h:0.48,fill:{color:w.col},line:{color:w.col}});
s.addText(w.label,{x:0.65,y:y+0.02,w:3.0,h:0.24,
fontSize:11,bold:true,color:w.col===GOLD?CHAR:w.col,fontFace:"Calibri"});
s.addText(w.desc,{x:0.65,y:y+0.25,w:3.0,h:0.22,
fontSize:9.5,color:SLATE,italic:true,fontFace:"Calibri"});
});
// Right: parameters
s.addText("Normal Values — Antidromic Median SNAP\n(Wrist stimulation → Digit II, ~13–14 cm)", {
x:4.05,y:0.87,w:5.7,h:0.55,
fontSize:13,bold:true,color:NAVY,fontFace:"Calibri"
});
const snapRows = [
["Parameter","Normal Value","Significance"],
["Onset Latency","< 3.5 ms","MOST SENSITIVE — first to prolong"],
["Peak Latency","< 3.6 ms","Easier to measure (less shock artifact)"],
["SNAP Amplitude","> 20 µV","Reduced = axonal loss"],
["Sensory CV","> 50 m/s","Slowed = demyelination"],
["Ulnar sensory","< 3.1 ms | >17 µV","Comparator — should be NORMAL in CTS"],
];
s.addTable(snapRows.map((row,ri)=>row.map((cell,ci)=>({
text:cell,
options:{
fontSize:10.5, bold:ri===0||(ri===1&&ci===2),
color:ri===0?WHITE:(ci===2?TEAL:CHAR),
fill:ri===0?TEAL:(ri===1?"E3F2FD":(ri%2===0?WHITE:OFFWH)),
align:"center",valign:"middle",
border:{pt:0.5,color:"C5D5E0"}, fontFace:"Calibri"
}
}))),{x:4.05,y:1.5,w:5.7,h:2.7,rowH:0.54,colW:[1.55,1.35,2.8]});
// Big key point
box(s,4.05,4.28,5.7,1.05,NAVY,NAVY);
s.addText("⚡ KEY POINT", {x:4.2,y:4.32,w:5.4,h:0.28,
fontSize:12,bold:true,color:GOLD,fontFace:"Calibri"});
s.addText("Sensory NCS is MORE SENSITIVE than motor NCS in early CTS. A prolonged median sensory latency is the EARLIEST NCS abnormality — before any motor changes appear.", {
x:4.2,y:4.6,w:5.4,h:0.68,
fontSize:11,color:WHITE,fontFace:"Calibri",valign:"top"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 5 STANDARD PROTOCOL
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, NAVY, "Standard NCS Protocol for CTS");
tag(s, "PROTOCOL");
const steps = [
{n:"1",title:"Median MOTOR NCS",
stim:"Wrist (7–8 cm from APB) → Elbow",
rec:"Abductor Pollicis Brevis (APB)",
measure:"Distal latency, CMAP amplitude, motor CV",
abnormal:"DML > 4.2 ms; forearm MCV normal (focal tunnel slowing)",col:TEAL},
{n:"2",title:"Median SENSORY NCS (Antidromic)",
stim:"Wrist",rec:"Ring electrodes at Digit II or Digit III (13–14 cm)",
measure:"Onset latency, peak latency, SNAP amplitude, SCV",
abnormal:"Onset latency > 3.5 ms; reduced SNAP amplitude; slowed SCV",col:TEAL2},
{n:"3",title:"Ulnar MOTOR + SENSORY NCS (Comparator)",
stim:"Wrist",rec:"ADM for motor | Digit V for sensory",
measure:"Latency and amplitude for both",
abnormal:"Should be NORMAL in isolated CTS — abnormal ulnar suggests polyneuropathy",col:NAVY},
{n:"4",title:"Internal Comparison Studies (See next slide)",
stim:"Palm (8 cm from wrist) for palmar mixed | Wrist for ring-finger/thumb studies",
rec:"Wrist recording for palmar | Digit IV / Thumb for sensory comparisons",
measure:"Median vs Ulnar latency difference at equal distances",
abnormal:"Median > Ulnar by > 0.3–0.4 ms → CTS confirmed even on background of DPN",col:GOLD},
];
steps.forEach((st,i)=>{
const y = 0.86 + i*1.13;
// full row bg
s.addShape(pres.ShapeType.rect,{x:0.28,y,w:9.44,h:1.0,
fill:{color:WHITE},line:{color:LGRAY},
shadow:{type:"outer",color:"000000",blur:3,offset:1,angle:135,opacity:0.07}});
// step color panel
s.addShape(pres.ShapeType.rect,{x:0.28,y,w:0.9,h:1.0,
fill:{color:st.col},line:{color:st.col}});
s.addText("STEP",{x:0.28,y:y+0.06,w:0.9,h:0.28,margin:0,
fontSize:8,bold:true,color:st.col===GOLD?CHAR:WHITE,align:"center",fontFace:"Calibri"});
s.addText(st.n,{x:0.28,y:y+0.3,w:0.9,h:0.45,margin:0,
fontSize:24,bold:true,color:st.col===GOLD?CHAR:WHITE,align:"center",valign:"top",fontFace:"Calibri"});
// content
s.addText(st.title,{x:1.28,y:y+0.06,w:8.3,h:0.3,
fontSize:13,bold:true,color:NAVY,fontFace:"Calibri"});
s.addText("Stim: "+st.stim+" | Rec: "+st.rec,{x:1.28,y:y+0.36,w:8.3,h:0.24,
fontSize:10,color:SLATE,fontFace:"Calibri"});
s.addText("⚠ Abnormal: "+st.abnormal,{x:1.28,y:y+0.62,w:8.3,h:0.3,
fontSize:10.5,bold:true,color:RED,fontFace:"Calibri"});
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 6 INTERNAL COMPARISON STUDIES
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, TEAL, "Internal Comparison Studies — Most Sensitive NCS Methods");
tag(s, "COMPARISON");
s.addText("Both median and ulnar nerves travel through the same forearm, so comparing their latencies at equal distances eliminates background polyneuropathy effects (e.g. diabetic neuropathy)", {
x:0.3,y:0.82,w:9.4,h:0.42,
fontSize:11,italic:true,color:SLATE,fontFace:"Calibri"
});
const trows = [
["Study","Technique","Type","Abnormal Criterion","Usefulness"],
["Median–Ulnar\nPalmar Mixed","Stimulate palm (8 cm)\nRecord at wrist for both","Orthodromic\nmixed nerve","Median > Ulnar\nby > 0.3 ms","Most sensitive;\nbest first-line"],
["Median–Ulnar\nRing Finger","Stim wrist; record at\nDigit IV antidromically","Antidromic\nsensory","Median > Ulnar\nby > 0.4 ms","Useful when\npalmar normal"],
["Median–Ulnar\nLumbrical–Interossei","Stim wrist; record at\n2nd interosseous space","Motor\ncomparison","Median > Ulnar\nby > 0.4–0.5 ms","Best for\nmotor CTS"],
["Median–Radial\nSensory to Thumb","Stim median & radial\nat wrist; record at thumb","Antidromic\nsensory","Median > Radial\nby > 0.5 ms","Best when DPN\nis severe"],
];
s.addTable(trows.map((row,ri)=>row.map((cell,ci)=>({
text:cell,
options:{
fontSize:10.5, bold:ri===0||(ri>0&&ci===3),
color:ri===0?WHITE:(ci===3?RED:CHAR),
fill:ri===0?NAVY:(ri%2===0?WHITE:OFFWH),
align:"center",valign:"middle",
border:{pt:0.6,color:"C5D5E0"}, fontFace:"Calibri"
}
}))),{x:0.3,y:1.32,w:9.4,h:3.65,rowH:0.73,colW:[1.65,2.3,1.45,1.75,1.75]});
// footnote + key rule
s.addText("Source: Bradley & Daroff's Neurology in Clinical Practice, Table 106.4, p. 2636", {
x:0.3,y:5.04,w:6,h:0.28,
fontSize:9,italic:true,color:SLATE,fontFace:"Calibri"
});
box(s,0.3,5.3,9.4,0.2,GOLD,GOLD);
s.addText("⭐ Rule: If Median latency exceeds Ulnar by the criterion value at equal distance → CTS is present, even if absolute latency is within 'normal' range due to background neuropathy", {
x:0.4,y:5.3,w:9.2,h:0.2,margin:0,
fontSize:9.5,bold:true,color:CHAR,align:"center",valign:"middle",fontFace:"Calibri"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 7 INCHING TECHNIQUE
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, NAVY, "The Inching (Segmental Stimulation) Technique");
tag(s, "INCHING");
// Left — principle
box(s, 0.28, 0.83, 4.65, 4.15, WHITE, TEAL);
s.addText("Principle", {x:0.42,y:0.88,w:4.4,h:0.38,
fontSize:15,bold:true,color:TEAL,fontFace:"Calibri"});
s.addText([
{text:"• Stimulate median nerve in ",options:{}},
{text:"1-cm increments",options:{bold:true,color:TEAL}},
{text:" across the wrist\n\n",options:{}},
{text:"• Normal response: ",options:{bold:true}},
{text:"latency increases linearly by ~0.16–0.21 ms per cm\n\n",options:{}},
{text:"• Pathological: ",options:{bold:true,color:RED}},
{text:"abrupt latency jump > 0.5 ms over a single 1-cm segment → focal lesion\n\n",options:{color:RED}},
{text:"• Reference point (0): ",options:{bold:true}},
{text:"distal wrist crease = origin of the transverse carpal ligament\n\n",options:{}},
{text:"• SNAPs recorded from Digit II\n","CMAPs recorded from APB",options:{}},
],{x:0.42,y:1.3,w:4.35,h:3.5,
fontSize:11.5,color:CHAR,fontFace:"Calibri",valign:"top"});
// Right — why it's superior
box(s, 5.1, 0.83, 4.65, 2.0, WHITE, TEAL2);
s.addText("Why Inching is Superior to Routine NCS", {x:5.24,y:0.88,w:4.4,h:0.38,
fontSize:13,bold:true,color:NAVY,fontFace:"Calibri"});
s.addText([
{text:"Over a 10-cm segment: ",options:{bold:true}},
{text:"0.2 ms slowing = 10% change → easily MISSED\n\n",options:{color:SLATE}},
{text:"Over a 1-cm segment: ",options:{bold:true}},
{text:"0.2 ms slowing = 100% change → UNMISTAKABLE",options:{color:RED,bold:true}},
],{x:5.24,y:1.3,w:4.35,h:1.4,
fontSize:11,color:CHAR,fontFace:"Calibri",valign:"top"});
// Right — CTS findings box
box(s, 5.1, 2.93, 4.65, 2.05, "EBF5FB", TEAL);
s.addText("CTS Pattern on Inching", {x:5.24,y:2.98,w:4.4,h:0.35,
fontSize:13,bold:true,color:TEAL,fontFace:"Calibri"});
s.addText([
{text:"Normal subject: ",options:{bold:true,color:GREEN}},
{text:"uniform ~0.16–0.21 ms/cm increase throughout\n\n",options:{}},
{text:"CTS patient: ",options:{bold:true,color:RED}},
{text:"abrupt jump (>0.5 ms) at a single level, usually at or just distal to the distal wrist crease (transverse carpal ligament)\n\n",options:{}},
{text:"Waveform change ",options:{bold:true}},
{text:"(amplitude drop, shape change) accompanies the latency jump",options:{}},
],{x:5.24,y:3.36,w:4.35,h:1.55,
fontSize:10.5,color:CHAR,fontFace:"Calibri",valign:"top"});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 8 SEVERITY GRADING
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, TEAL, "NCS Severity Grading in CTS");
tag(s, "GRADING");
const grades = [
{grade:"MILD", col:GREEN, bg:"E8F5E9",
f:["Prolonged median sensory latency / slowed SCV only",
"Motor distal latency: NORMAL",
"CMAP amplitude: NORMAL",
"No denervation on EMG"],
rx:"Splints in neutral + NSAID / Corticosteroid injection"},
{grade:"MODERATE",col:ORANGE,bg:"FFF3E0",
f:["Prolonged motor AND sensory distal latencies",
"SNAP amplitude reduced (but present)",
"CMAP amplitude mildly reduced",
"No active denervation on EMG"],
rx:"Steroid injection → Consider surgical release"},
{grade:"SEVERE", col:RED, bg:"FFEBEE",
f:["Absent median SNAP",
"Significantly prolonged motor latency",
"Reduced CMAP amplitude (axonal loss)",
"EMG: chronic neurogenic changes in APB"],
rx:"Surgical carpal tunnel release (urgent)"},
{grade:"EXTREME",col:PURPLE, bg:"F3E5F5",
f:["Absent SNAP and absent/minimal CMAP",
"Fibrillations + PSWs in APB (active denervation)",
"Reduced/absent MUPs on voluntary activation",
"EMG mandatory to quantify axonal loss"],
rx:"Emergency surgical release — recovery guarded"},
];
grades.forEach((g,i)=>{
const col = i%2; const row = Math.floor(i/2);
const x = 0.28 + col*4.84; const y = 0.84 + row*2.32;
box(s,x,y,4.6,2.22,g.bg,g.col);
// grade banner
s.addShape(pres.ShapeType.rect,{x,y,w:4.6,h:0.46,fill:{color:g.col},line:{color:g.col}});
s.addText(g.grade,{x,y,w:4.6,h:0.46,margin:0,
fontSize:18,bold:true,color:WHITE,align:"center",valign:"middle",fontFace:"Calibri"});
g.f.forEach((fi,ii)=>{
s.addText("• "+fi,{x:x+0.15,y:y+0.5+ii*0.3,w:4.3,h:0.28,
fontSize:10,color:CHAR,fontFace:"Calibri"});
});
// rx band
s.addShape(pres.ShapeType.rect,{x:x+0.1,y:y+1.78,w:4.4,h:0.32,
fill:{color:g.col,transparency:65},line:{color:g.col}});
s.addText("Rx: "+g.rx,{x:x+0.12,y:y+1.78,w:4.36,h:0.32,margin:0,
fontSize:9.5,bold:true,color:CHAR,align:"center",valign:"middle",fontFace:"Calibri"});
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 9 NORMAL VALUES TABLE
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, NAVY, "Normal NCS Reference Values");
tag(s, "NORMAL VALUES", TEAL);
s.addText("Adams & Victor's Principles of Neurology, Table 2-5 (Mean ± 2SD, Adults 16–65 yr)", {
x:0.3,y:0.82,w:9.4,h:0.3,
fontSize:10,italic:true,color:SLATE,fontFace:"Calibri"
});
s.addText("MOTOR NCS",{x:0.3,y:1.17,w:2,h:0.3,
fontSize:13,bold:true,color:TEAL,fontFace:"Calibri"});
const mhdr = ["Nerve","Stimulate","Record","DML (ms)","Amp (mV)","CV (m/s)","F-wave (ms)"];
const mdat = [
["Median","Wrist","APB","< 4.2","> 4.4","> 49","< 31"],
["Ulnar","Wrist","ADM","< 3.4","> 6.0","> 49","< 32"],
["Peroneal","Ankle","EDB","< 5.8","> 2.0","> 42","< 58"],
["Tibial","Ankle","AH","< 6.5","> 3.0","> 41","< 59"],
];
s.addTable([mhdr,...mdat].map((row,ri)=>row.map((cell,ci)=>({
text:cell, options:{
fontSize:10.5, bold:ri===0,
color:ri===0?WHITE:(ci>=3?TEAL:CHAR),
fill:ri===0?NAVY:(ri%2===0?WHITE:OFFWH),
align:"center",valign:"middle",
border:{pt:0.5,color:"C5D5E0"},fontFace:"Calibri"
}
}))),{x:0.3,y:1.5,w:9.4,h:1.55,rowH:0.31,colW:[1.3,1.2,1.0,1.45,1.3,1.3,1.45]});
s.addText("SENSORY NCS",{x:0.3,y:3.12,w:2.2,h:0.3,
fontSize:13,bold:true,color:TEAL2,fontFace:"Calibri"});
const shdr = ["Nerve","Stimulate","Record","Onset (ms)","Peak (ms)","Amp (µV)","CV (m/s)"];
const sdat = [
["Median","Wrist","Digit II","< 3.5","< 3.6","> 20","> 50"],
["Ulnar","Wrist","Digit V","< 3.1","< 3.2","> 17","> 50"],
["Sural","Calf","Ankle","< 4.4","–","> 6","> 40"],
["Radial","Forearm","Thumb","< 2.9","–","> 15","> 50"],
];
s.addTable([shdr,...sdat].map((row,ri)=>row.map((cell,ci)=>({
text:cell, options:{
fontSize:10.5, bold:ri===0,
color:ri===0?WHITE:(ci>=3?TEAL2:CHAR),
fill:ri===0?TEAL:(ri%2===0?WHITE:OFFWH),
align:"center",valign:"middle",
border:{pt:0.5,color:"C5D5E0"},fontFace:"Calibri"
}
}))),{x:0.3,y:3.45,w:9.4,h:1.55,rowH:0.31,colW:[1.3,1.2,1.0,1.45,1.3,1.3,1.45]});
// CTS highlight
box(s,0.3,5.07,9.4,0.35,"FFF8E1",GOLD);
s.addText("CTS cut-offs: Median motor DML > 4.2 ms | Median sensory onset > 3.5 ms | SNAP amplitude < 20 µV → Pathological", {
x:0.42,y:5.07,w:9.2,h:0.35,margin:0,
fontSize:11.5,bold:true,color:CHAR,align:"center",valign:"middle",fontFace:"Calibri"
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 10 CTS IN DIABETES — CHALLENGES
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:NAVY};
s.addShape(pres.ShapeType.rect,{x:0,y:0,w:10,h:0.72,fill:{color:RED},line:{color:RED}});
s.addText("CTS in Diabetic Patients — The Diagnostic Challenge",{
x:0.35,y:0,w:9.3,h:0.72,margin:0,
fontSize:21,bold:true,color:WHITE,valign:"middle",fontFace:"Calibri"});
tag(s,"DM + CTS",WHITE);
const chal = [
{n:"1",title:"Problem: Elevated Baselines (Background DPN)",col:RED,
body:"Diabetic peripheral neuropathy (DPN) prolongs latencies and reduces amplitudes across ALL nerves. A median DML of 4.8 ms looks like 'mild CTS' when the ulnar is also 4.5 ms — this pattern reflects diffuse neuropathy, NOT focal entrapment. Absolute values alone are unreliable in DM."},
{n:"2",title:"Problem: DM is an Independent CTS Risk Factor",col:GOLD,
body:"Diabetics have 2–3× higher CTS prevalence than the general population. Mechanisms include: metabolic accumulation within the flexor tendons, tenosynovitis, microangiopathy of the vasa nervorum, and increased susceptibility of already-compromised nerves to compressive injury ('double crush' phenomenon)."},
{n:"3",title:"Problem: Small Fiber DPN — NCS May Be Normal",col:TEAL2,
body:"NCS only captures large myelinated fibres (A-alpha / A-beta). In DM, early and predominant small fibre (C and A-delta) involvement gives NORMAL NCS despite severe burning pain, autonomic dysfunction, and reduced IENFD on skin biopsy. Skin biopsy or QSART is needed for diagnosis in these patients."},
];
chal.forEach((c,i)=>{
const y = 0.86 + i*1.48;
s.addShape(pres.ShapeType.rect,{x:0.28,y,w:9.44,h:1.35,
fill:{color:"0D2849"},line:{color:c.col}});
s.addShape(pres.ShapeType.rect,{x:0.28,y,w:0.55,h:1.35,fill:{color:c.col},line:{color:c.col}});
s.addText(c.n,{x:0.28,y,w:0.55,h:1.35,margin:0,
fontSize:28,bold:true,color:c.col===GOLD?CHAR:WHITE,align:"center",valign:"middle",fontFace:"Calibri"});
s.addText(c.title,{x:0.95,y:y+0.08,w:8.6,h:0.32,
fontSize:13,bold:true,color:c.col===GOLD?GOLD:c.col,fontFace:"Calibri"});
s.addText(c.body,{x:0.95,y:y+0.44,w:8.6,h:0.82,
fontSize:10.5,color:"B0C4D8",fontFace:"Calibri",valign:"top"});
});
s.addShape(pres.ShapeType.rect,{x:0.28,y:5.32,w:9.44,h:0.2,fill:{color:TEAL},line:{color:TEAL}});
s.addText("Solution: Internal Comparison Studies (next slide) isolate the focal CTS component from background DPN", {
x:0.38,y:5.32,w:9.2,h:0.2,margin:0,
fontSize:10,bold:true,color:WHITE,align:"center",valign:"middle",fontFace:"Calibri"});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 11 DM+CTS PROTOCOL + DISTINGUISHING TABLE
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, TEAL, "NCS Protocol: CTS Superimposed on Diabetic Neuropathy");
tag(s,"DM PROTOCOL");
// Left column — steps
s.addText("Step-by-Step Protocol", {x:0.28,y:0.84,w:5.5,h:0.32,
fontSize:14,bold:true,color:NAVY,fontFace:"Calibri"});
const steps = [
"Ensure skin temperature > 32°C — cold falsely prolongs latency; critical in DM",
"Median motor NCS (wrist → APB) + Ulnar motor NCS (comparator)",
"Median sensory NCS antidromic (wrist → Digit II)",
"Median–Ulnar palmar mixed comparison (most sensitive single test)",
"Median–Radial sensory to thumb comparison (best when DPN is severe)",
"Sural + Peroneal NCS — grade severity of background DPN (lower limb worse)",
"Needle EMG of APB if moderate–severe CTS: fibrillations = axonal loss = surgical urgency",
];
steps.forEach((st,i)=>{
const y = 1.22 + i*0.57;
circle(s, 0.28, y+0.06, 0.38, TEAL, String(i+1));
s.addText(st,{x:0.75,y,w:5.15,h:0.5,
fontSize:10,color:CHAR,fontFace:"Calibri",valign:"middle"});
});
// Right column — distinguishing table
s.addText("Focal CTS vs Diffuse DPN",{x:6.15,y:0.84,w:3.7,h:0.32,
fontSize:13,bold:true,color:NAVY,fontFace:"Calibri"});
const drows = [
["Feature","Focal CTS","Diffuse DPN"],
["Sensory latency","Median > Ulnar","Both equal"],
["Motor latency","DML only prolonged;\nforearm MCV normal","All segments\nslowed"],
["Upper vs Lower","Upper limb\nisolated","Lower limb\nworse"],
["Sural nerve","Normal","Abnormal/absent\nSNAP"],
["F-waves","Normal","All prolonged"],
];
s.addTable(drows.map((row,ri)=>row.map((cell,ci)=>({
text:cell, options:{
fontSize:9.5, bold:ri===0||ci===0,
color:ri===0?WHITE:(ci===1?TEAL:(ci===2?RED:CHAR)),
fill:ri===0?NAVY:(ri%2===0?WHITE:OFFWH),
align:"center",valign:"middle",
border:{pt:0.5,color:"C5D5E0"},fontFace:"Calibri"
}
}))),{x:6.15,y:1.22,w:3.7,h:3.65,rowH:0.61,colW:[1.3,1.2,1.2]});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 12 DIAGNOSIS FLOWCHART
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:OFFWH};
topBar(s, NAVY, "Diagnostic Flowchart — CTS in the Diabetic Patient");
tag(s, "FLOWCHART");
// ── boxes ──
function fbox(x,y,w,h,fill,border,text,tcolor,fs,bold){
s.addShape(pres.ShapeType.rect,{x,y,w,h,fill:{color:fill},line:{color:border||fill},
shadow:{type:"outer",color:"000000",blur:4,offset:2,angle:135,opacity:0.1}});
s.addText(text,{x,y,w,h,margin:0,
fontSize:fs||11,bold:bold!==false,color:tcolor||WHITE,
align:"center",valign:"middle",fontFace:"Calibri"});
}
function arr(x,y,len,horiz){
if(horiz){
s.addShape(pres.ShapeType.rect,{x,y:y+0.05,w:len,h:0.08,fill:{color:SLATE},line:{color:SLATE}});
s.addShape(pres.ShapeType.triangle,{x:x+len-0.12,y,w:0.18,h:0.18,fill:{color:SLATE},line:{color:SLATE}});
} else {
s.addShape(pres.ShapeType.rect,{x:x+0.05,y,w:0.08,h:len,fill:{color:SLATE},line:{color:SLATE}});
s.addShape(pres.ShapeType.triangle,{x,y:y+len-0.1,w:0.18,h:0.18,fill:{color:SLATE},line:{color:SLATE}});
}
}
// Top: suspected CTS
fbox(3.2,0.88,3.6,0.52,NAVY,NAVY,"Suspected CTS in DM Patient",WHITE,12);
arr(5.0,1.4,0.35,false);
// NCS box
fbox(2.0,1.75,6.0,0.72,TEAL,TEAL,
"NCS: Median motor + sensory | Ulnar motor + sensory\nLower limb NCS (sural, peroneal, tibial)",WHITE,11);
arr(5.0,2.47,0.32,false);
// Decision diamond
s.addShape(pres.ShapeType.rect,{x:2.8,y:2.79,w:4.4,h:0.62,
fill:{color:"FFF8E1"},line:{color:GOLD,width:2}});
s.addText("Are ALL nerves equally slowed?\n(length-dependent pattern, lower limbs worse?)",{
x:2.8,y:2.79,w:4.4,h:0.62,margin:0,
fontSize:11,bold:true,color:CHAR,align:"center",valign:"middle",fontFace:"Calibri"});
// YES branch (left)
arr(2.8,3.1,0.38,true); // horiz left
s.addShape(pres.ShapeType.rect,{x:0.28,y:3.04,w:2.48,h:0.15,fill:{color:SLATE},line:{color:SLATE}});
arr(1.42,3.19,0.32,false);
fbox(0.28,3.51,2.9,0.54,ORANGE,ORANGE,"YES → Diffuse DPN\nconfirmed",WHITE,10.5);
arr(1.73,4.05,0.32,false);
fbox(0.28,4.37,2.9,0.62,SLATE,SLATE,
"Consider skin biopsy\n(IENFD) or QSART\nfor small-fiber DPN",WHITE,10,true);
// NO branch (right)
arr(7.2,3.1,0.52,true);
fbox(7.2,3.04,2.52,0.15,SLATE,SLATE,"",SLATE,1);
arr(8.46,3.19,0.32,false);
fbox(7.1,3.51,2.62,0.54,TEAL,TEAL,"NO → Median > Ulnar\nRun internal comparisons",WHITE,10.5);
arr(8.41,4.05,0.32,false);
fbox(7.1,4.37,2.62,0.62,GREEN,GREEN,
"Median > Ulnar > 0.3 ms\n(palmar mixed)\n→ CTS CONFIRMED",WHITE,10,true);
// Bottom: treatment
arr(5.0,4.4,0.35,false);
fbox(2.85,4.75,4.3,0.65,NAVY,NAVY,
"Grade severity (Mild/Moderate/Severe)\nTreat accordingly: splint / steroid / surgery",WHITE,11);
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 13 KEY EXAM POINTS
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:NAVY};
s.addShape(pres.ShapeType.rect,{x:0,y:0,w:10,h:0.72,fill:{color:GOLD},line:{color:GOLD}});
s.addText("High-Yield Exam Points — DM Neurology",{
x:0.35,y:0,w:9.3,h:0.72,margin:0,
fontSize:22,bold:true,color:CHAR,valign:"middle",fontFace:"Calibri"});
const pts = [
{n:"1",t:"Sensory NCS is MORE SENSITIVE than motor in early CTS — prolonged median sensory latency is the FIRST NCS abnormality",col:GOLD},
{n:"2",t:"Internal comparison (Median > Ulnar by >0.3 ms palmar mixed) is the MOST SENSITIVE method — MANDATORY when DPN coexists",col:TEAL2},
{n:"3",t:"Inching technique: normal = 0.16–0.21 ms/cm; pathological = abrupt jump >0.5 ms over a single 1-cm segment at the carpal ligament",col:TEAL},
{n:"4",t:"In DM + CTS: use Median–Ulnar palmar comparison AND Median–Radial thumb comparison to isolate the focal component from DPN",col:GOLD},
{n:"5",t:"Temperature MUST be >32°C before NCS — DM patients have cold extremities that falsely prolong latencies and mimic neuropathy",col:TEAL2},
{n:"6",t:"Needle EMG of APB in moderate–severe CTS: fibrillations + reduced MUP recruitment = axonal loss → surgical urgency",col:TEAL},
{n:"7",t:"Post-surgical recovery: sensory SYMPTOMS improve first; NCS latency normalisation lags by months — do not re-test too early",col:GOLD},
];
pts.forEach((p,i)=>{
const y = 0.85 + i*0.66;
s.addShape(pres.ShapeType.rect,{x:0.28,y,w:9.44,h:0.58,
fill:{color:"0D2849"},line:{color:p.col}});
s.addShape(pres.ShapeType.rect,{x:0.28,y,w:0.5,h:0.58,fill:{color:p.col},line:{color:p.col}});
s.addText(p.n,{x:0.28,y,w:0.5,h:0.58,margin:0,
fontSize:18,bold:true,color:p.col===GOLD?CHAR:WHITE,
align:"center",valign:"middle",fontFace:"Calibri"});
s.addText(p.t,{x:0.88,y:y+0.06,w:8.7,h:0.46,
fontSize:11,color:WHITE,fontFace:"Calibri",valign:"middle"});
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 14 THANK YOU / REFERENCES
// ════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = {color:NAVY};
s.addShape(pres.ShapeType.rect,{x:0,y:0,w:0.45,h:5.625,fill:{color:TEAL},line:{color:TEAL}});
s.addShape(pres.ShapeType.rect,{x:0.45,y:0,w:0.07,h:5.625,fill:{color:GOLD},line:{color:GOLD}});
s.addText("Thank You",{x:0.75,y:0.7,w:9,h:1.0,
fontSize:46,bold:true,color:WHITE,fontFace:"Calibri",align:"left"});
s.addShape(pres.ShapeType.rect,{x:0.75,y:1.74,w:5,h:0.055,fill:{color:GOLD},line:{color:GOLD}});
s.addText("References",{x:0.75,y:1.96,w:9,h:0.35,
fontSize:17,bold:true,color:TEAL2,fontFace:"Calibri"});
const refs = [
"1. Bradley WG, Daroff RB et al. Bradley and Daroff's Neurology in Clinical Practice, 8th Ed. — Chapter 36 (EMG/NCS) & Chapter 106 (Entrapment Neuropathies)",
"2. Adams RD, Victor M, Ropper AH. Adams and Victor's Principles of Neurology, 12th Ed. — Chapter 2 (Electrophysiologic Studies, Table 2-5)",
"3. Kimura J. The carpal tunnel syndrome: localization of conduction abnormalities within the distal segment of the median nerve. Brain 1979;102:619–635",
"4. American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM). Practice Guidelines for CTS Electrodiagnosis",
"5. Campbell's Operative Orthopaedics, 15th Ed. 2026 — Carpal Tunnel Syndrome (NCS in surgical planning)",
];
refs.forEach((r,i)=>{
s.addText(r,{x:0.75,y:2.38+i*0.52,w:9.0,h:0.44,
fontSize:10,color:"7B9EC4",fontFace:"Calibri"});
});
s.addShape(pres.ShapeType.rect,{x:0.75,y:5.05,w:4,h:0.36,
fill:{color:TEAL,transparency:60},line:{color:TEAL2}});
s.addText("DM Neurology — Electrophysiology Seminar",{
x:0.75,y:5.05,w:4,h:0.36,margin:0,
fontSize:12,italic:true,color:WHITE,align:"center",valign:"middle",fontFace:"Calibri"});
}
// ── WRITE ────────────────────────────────────────────────────────────────────
pres.writeFile({fileName:"/home/daytona/workspace/NCS_CTS_DM_v2.pptx"})
.then(()=>{ console.log("DONE"); })
.catch(e=>{ console.error("FAIL",e); process.exit(1); });
cd /home/daytona/workspace/ncs-cts-ppt && node build2.js 2>&1
~/ncs-cts-ppt/build2.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/ncs-cts-ppt/build2.js'
cd /home/daytona/workspace/ncs-cts-ppt && node build2.js 2>&1
# Verify ZIP integrity and convert to PDF via LibreOffice to confirm it opens ls -lh /home/daytona/workspace/NCS_CTS_DM_v2.pptx unzip -t /home/daytona/workspace/NCS_CTS_DM_v2.pptx 2>&1 | tail -5 libreoffice --headless --convert-to pdf /home/daytona/workspace/NCS_CTS_DM_v2.pptx --outdir /tmp/ 2>&1 ls -lh /tmp/NCS_CTS_DM_v2.pdf 2>&1
cp /tmp/NCS_CTS_DM_v2.pdf /home/daytona/workspace/NCS_CTS_DM_v2.pdf && ls -lh /home/daytona/workspace/NCS_CTS_DM_v2.pdf
NCS CTS DM v2
Presentation · PPTX
NCS CTS DM v2
PDF Document · PDF
| # | Slide |
|---|---|
| 1 | Title |
| 2 | Why NCS in CTS? (5 reasons) |
| 3 | Motor NCS — CMAP parameters + formula |
| 4 | Sensory NCS — SNAP parameters + key point box |
| 5 | Standard 4-step Protocol |
| 6 | Internal Comparison Studies table |
| 7 | Inching Technique — principle + why it's superior |
| 8 | Severity Grading — Mild/Moderate/Severe/Extreme |
| 9 | Normal NCS Reference Values (motor + sensory tables) |
| 10 | CTS in Diabetes — 3 problems (dark slide) |
| 11 | DM+CTS Protocol + Focal CTS vs Diffuse DPN table |
| 12 | Diagnostic Flowchart |
| 13 | 7 High-Yield Exam Points |
| 14 | References |