


So this is all the things I got from today from the, uh, this presentation I was given yesterday, right? Just take down history and tell me that what can I do for this thing? Explain me with adding that.
Your Notes - Decoded and Explained
What Your Notes Are About
1. The Presentation Structure (Poster Layout)
| Section | Content |
|---|---|
| Title | (your case title) |
| Author (1, 2, 3) | Author names |
| Introduction | Background on the condition |
| Case Presentation | The actual patient case |
| Discussion | Why this approach was chosen |
| Conclusion | Key takeaway |
| Reference | Citations |
2. The Case - What the Patient Had
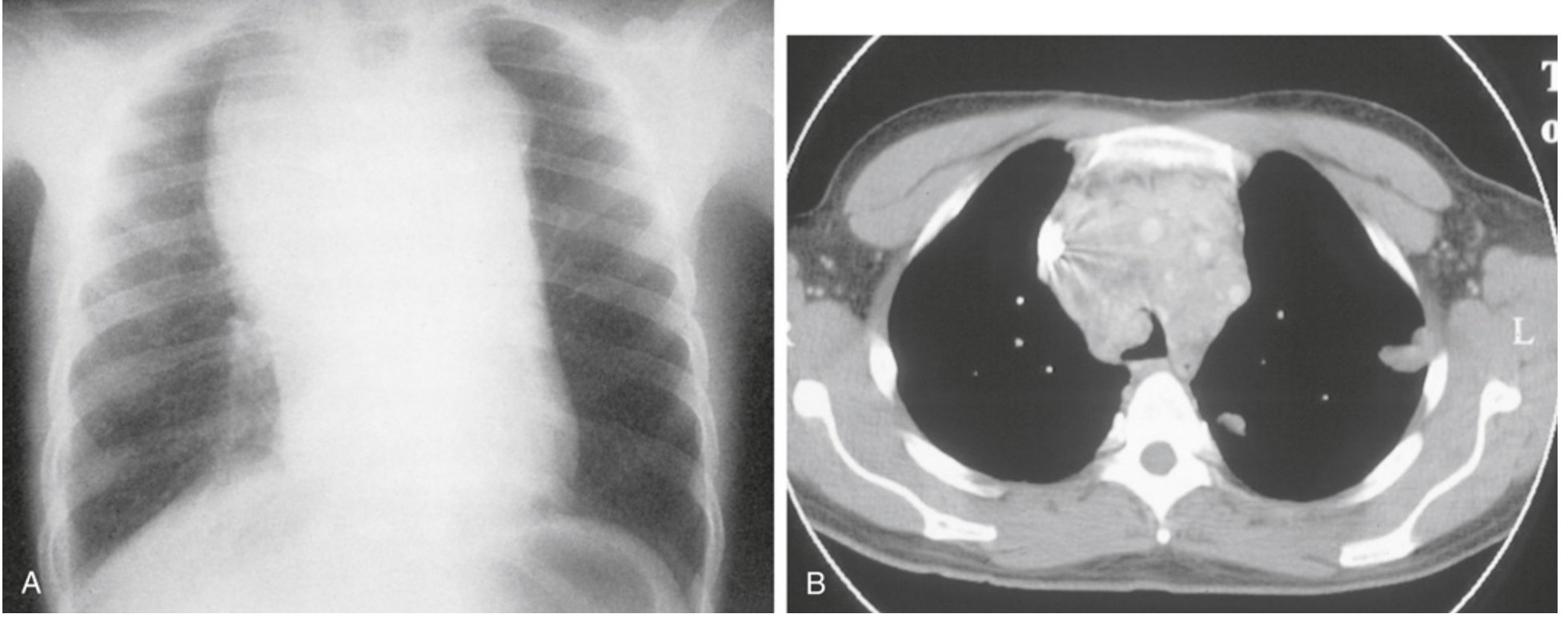
- Pre-op X-ray (CXR) - chest X-ray done before surgery
- Fiberoptic / V.C. (vocal cord) check - assessed vocal cord movement
- Intubated - patient needed intubation
- Mass (4th) - likely a 4th-compartment / anterior mediastinal mass
- CT scan slide - CT chest was done
3. The Images to Include in the Presentation
| # | Image | Notes |
|---|---|---|
| 1 | CXR (Pre-op) | Mandatory |
| 2 | HRCT - compressed trachea slide | Mandatory - shows the compression |
| 3 | Mass (CT/image showing the mass) | Mandatory |
| 4 | Intubated patient image | Optional |
| 5 | Fiberoptic image while intubating | Optional |
4. The Awake Fiberoptic Intubation Technique (Your Main Notes)
Step 1 - Topical Airway Anesthesia
LOX 4% Nebulization: 2 mL + 2 mL NS
- LOX = Lignocaine (Lidocaine) 4%
- Diluted with normal saline and given via nebulizer mask
- The patient inhales it for 10-15 minutes
- This numbs the pharynx, larynx, and upper trachea so the scope can pass without triggering violent coughing/gagging
- From the textbook: "5 mL of 2% plain lidocaine can be inhaled via nebulizer" - your case uses 4% which gives more concentrated topical effect (- Cummings Otolaryngology)
Step 2 - Transtracheal Block
Transtracheal block → Inj. LOX 2% 2 mL + Inj. Bupivacaine 2 mL
- A needle is passed through the cricothyroid membrane into the trachea
- Lignocaine 2% (2 mL) + Bupivacaine 2% (2 mL) injected directly
- Patient coughs reflexively - this sprays the drug upward onto the cords and downward into the trachea, anesthetizing both
- This is the cricotracheal (transtracheal) block
- Together with the nebulization, this achieves full topical anesthesia of the entire airway from pharynx to carina
Step 3 - Fiberoptic Intubation
Fiberoptic intubation (after full airway anesthesia)
- The flexible fiberoptic bronchoscope is passed through the endotracheal tube (ETT), guided through the vocal cords under direct vision, and advanced into the trachea
- The ETT is then railroaded over the scope
- Patient remains awake and breathing spontaneously throughout - this is the safety net; if the airway collapses, the patient's own respiratory effort helps maintain patency
5. The Flowchart at the Bottom of Your Notes
After seeing airway → Inj. (?) → (10 sec) → (Rocuronium) → Crisis
- A scenario where, after confirming the airway on fiberoptic view, someone prematurely gives Rocuronium (a neuromuscular blocker/paralytic)
- In 10 seconds, full paralysis sets in
- With a compressing mediastinal mass, the trachea now collapses because all muscle tone is gone
- Result: Cannot ventilate, cannot intubate - crisis / cannot oxygenate situation
6. Why Awake Intubation is Chosen Here (the Discussion angle)
- Reduced lung volume under GA shrinks tracheal diameter
- Bronchial smooth muscle relaxes - airway becomes more compressible
- Paralysis removes spontaneous breathing - eliminates the negative intrathoracic pressure that normally keeps airways open
7. What You Need to Do for the Presentation
- Collect the images: CXR pre-op, HRCT showing compressed trachea (key slide), mass image - these 3 are mandatory
- Write the case: Age/sex, presenting complaint, workup findings (CXR + HRCT), the mass, and the anesthetic challenge
- Describe the technique: Nebulized Lignocaine 4% (2 mL + 2 mL NS) → Transtracheal block (LOX 2% 2 mL + Bupivacaine 2 mL) → Fiberoptic intubation
- Discussion: Why AFOI was chosen - explain the danger of GA + paralysis in tracheal compression
- Add optional images if you have them: photo of the intubated patient, fiberoptic view during intubation
- Add the "crisis" flowchart as a teaching point in the discussion - what would have happened if paralysis was given first
- Slide structure: Follow the poster layout - Title → Author → Introduction → Case Presentation → Discussion → Conclusion → Reference
I want to do a poster presentation on this case. Please do help me on this from the anesthesia side.
K
- Patient - age, sex
- Chief complaint - what brought them in (e.g., breathlessness, stridor, neck swelling?)
- Mass - what it was (e.g., anterior mediastinal mass, thyroid mass, lymphoma, thymoma?) and any size if known
- Tracheal compression - how much? (e.g., >50% on CT, just HRCT showed compression?)
- Any co-morbidities (e.g., hypertension, diabetes, etc.) or was the patient otherwise healthy?
- What surgery was done - why did they need intubation? (biopsy, excision, VATS?)
- Your name and co-authors / institution name for the poster title
Here is a complete, well-structured case presentation of Mrs. Roshani Sen, ready to present: --- # CASE PRESENTATION ## Anterior Mediastinal Mature Cystic Teratoma --- ## PATIENT PROFILE - **Name:** Mrs. Roshani Sen - **Age:** 26 years 10 months - **Sex:** Female - **DOB:** 05 August 1999 - **Address:** Gunjali, Sanawad, Madhya Pradesh - **Admission Date:** 09 June 2026 - **Hospital:** Parul Sevashram Hospital, Vadodara (CTVS Unit) - **Consultants:** Dr. Dipesh D. Duttaroy, Dr. Sagar Sahita (CTVS Surgeon) - **Insurance:** Ayushman Bharat Yojana (Government scheme) --- ## CHIEF COMPLAINT - **Anterior neck swelling** since **1 year** - Associated **chest heaviness and chest pain** --- ## HISTORY OF PRESENTING ILLNESS - Young female, 26 years old, presenting with gradually progressive swelling in the anterior neck region for 1 year - Swelling extended into the chest (retrosternal region) - Associated with a sensation of heaviness and discomfort in the chest - No fever, no weight loss, no dysphagia, no dyspnoea at rest - No history of trauma - No prior surgery or hospitalisation - Self-referred (direct referral) --- ## PAST HISTORY - No Diabetes Mellitus - No Hypertension - No known cardiac disease - No tuberculosis - No asthma - No known drug, food, or latex allergies --- ## EXAMINATION ON ADMISSION ### Vital Signs - **BP:** 110/70 mmHg - **SpO₂:** 94% (room air) - **Temperature:** Normal - **Pulse:** Normal - **Respiratory rate:** 19 breaths/min ### General Examination - Conscious, oriented, cooperative - No cyanosis, no jaundice, no pallor (mild) - No significant lymphadenopathy noted ### Local Examination - Anterior neck swelling palpable - Mass extending retrosternally ### Systemic Examination - Respiratory: Normal air entry bilaterally - Cardiovascular: Normal heart sounds - Abdomen: Soft, non-tender --- ## INVESTIGATIONS ### Imaging #### CT Neck & Chest (26 May 2026 - Pre-admission) - Large, **well-defined mixed-density mass measuring 8.3 × 5.1 × 12.2 cm** - Involving the **lower neck and retrosternal region** - Mass contains **fat + calcification + soft tissue** - classic triad of a mature cystic teratoma - Diagnosis suggested: **Mature Cystic Teratoma** #### Chest X-Ray PA View (15 June 2026 - Pre-op) - **Homogeneous opacity in the anterior mediastinum** (the mass) - **Tracheal deviation** to the contralateral side - indicating significant mass effect - Both lungs otherwise clear - Heart size normal #### ECG (15 June 2026 - Pre-op) - **HR: 81/min** - Normal sinus rhythm - **PR: 159 ms** - Normal - **QRS: 65 ms** - Normal - **QTc: 382 ms** - Normal - Conclusion: **Normal ECG, no cardiac involvement** --- ### Blood Investigations #### Complete Blood Count (CBC) | Parameter | Value | Reference | Status | |-----------|-------|-----------|--------| | Haemoglobin | 11.7 g/dL | 12.0-15.0 | ⬇ Mildly low | | RBC | 4.20 million/µL | 4.5-5.5 | ⬇ Low | | WBC | 5710/µL | 4000-10000 | ✅ Normal | | Platelets | 278,000/µL | 150,000-450,000 | ✅ Normal | - **Mild normocytic anaemia** - likely anaemia of chronic disease from long-standing mass #### Coagulation Profile | Test | Value | Reference | Status | |------|-------|-----------|--------| | PT | 12.8 sec | 9.39-12.91 | ✅ Normal | | INR | 1.13 | 0.8-1.1 | ⬆ Borderline | | APTT | 32.8 sec | 22.7-35.0 | ✅ Normal | - Mildly elevated INR - not a contraindication to surgery #### Biochemistry | Test | Value | Status | |------|-------|--------| | CRP | 1.64 mg/L | ✅ Normal (<5) - No inflammation | | TSH | 1.920 µIU/mL | ✅ Normal - Thyroid origin ruled out | | NT-proBNP | 38.8 pg/mL | ✅ Normal (<300) - No heart failure | | Procalcitonin | 0.05 ng/mL | ✅ Normal - No sepsis | | Troponin I (hs) | <1.5 ng/L | ✅ Normal - No cardiac injury | | HbA1c | 4.8% | ✅ Non-diabetic | | Serum Creatinine | 0.6 mg/dL | ✅ Normal - Kidneys healthy | | eGFR | 120.8 mL/min | ✅ Stage 1 - Normal | | SGPT/SGOT | 14 / 19 U/L | ✅ Normal - Liver healthy | | Albumin | 3.9 g/dL | ✅ Normal | | Na / K | 135 / 4.3 mmol/L | ⚠ Na mildly low; K normal | #### Infectious Disease Screening (Pre-op) | Test | Result | |------|--------| | HBsAg | ✅ Negative | | Anti-HCV | ✅ Non-reactive | | HIV 1 & 2 | ✅ Non-reactive | | RPR (Syphilis) | ✅ Non-reactive | - All 4 mandatory pre-operative screens: **NEGATIVE** #### Urine Examination - Routine urine examination: **Normal** - No infection, no proteinuria, no glucosuria --- ## DIAGNOSIS > **Anterior Mediastinal Mass - Mature Cystic Teratoma** - Clinical diagnosis confirmed by CT imaging - Histopathologically proven post-excision --- ## SURGICAL MANAGEMENT ### Operation: **Anterior Mediastinal Mass Excision (Teratoma Excision)** | Detail | Information | |--------|-------------| | **Date of Surgery** | 16 June 2026 | | **Surgeon** | Dr. Sagar Sahita (CTVS Surgeon) | | **Approach** | Median Sternotomy (breastbone cut and wired back) | | **Anaesthesia** | General Anaesthesia (ET tube size 7.5) | | **Anaesthetist** | Dr. Kaushik Dhami | | **Duration** | Several hours (major thoracic procedure) | | **Blood Products Used** | Packed cells (PCV) + FFP (Fresh Frozen Plasma) | ### Intraoperative Details - Patient intubated and placed on general anaesthesia - Median sternotomy performed for access to anterior mediastinum - Mass excised completely - Right-sided ICD (Intercostal Chest Drain) inserted post-excision - Right Femoral CVC line placed - Intraoperative ABG monitoring performed - Patient **extubated at 3:30 PM** on the same day (same-day extubation - a good outcome) - Transferred to **CICU (Cardiac ICU)** post-operatively ### Gross Specimen - Specimen size: **14 × 7.0 × 4.7 cm** - External surface: smooth, congested - Cut section: **cheesy necrotic material** drained from cystic areas - **Hair shafts** identified within the lesion --- ## POST-OPERATIVE COURSE | Day | Date | Status | |-----|------|--------| | **Op Day** | 16 Jun | Teratoma excised; 2 ICDs in situ; extubated 3:30 PM; admitted CICU | | **POD-1** | 17 Jun | Stable in CICU; chest drains functioning; CXR normal | | **POD-2** | 18 Jun | ⚠ Morning CXR: Right pneumothorax + right pleural effusion - managed with existing drains; Afternoon CXR: Both lungs cleared | | **POD-3** | 19 Jun | Small left minimal pleural effusion; right improving; Hb 9.8 g/dL | | **POD-4** | 20 Jun | CXR completely normal; both costophrenic angles clear; drains removed | | **POD-5/6** | 21-22 Jun | Pain managed; ambulating; discharge planning | ### Post-Op Complications (managed successfully) 1. **Right-sided pneumothorax** (POD-2) - resolved with drain management 2. **Right pleural effusion with consolidation** (POD-2) - resolved within hours 3. **Small left minimal pleural effusion** (POD-3) - resolved spontaneously by POD-4 4. **Post-op anaemia** (Hb dropped from 11.9 → 9.8 g/dL) - managed with blood transfusion 5. **Hypoalbuminaemia** (Albumin dropped 3.9 → 2.6 g/dL post-op) - expected post-surgical acute-phase response, managed with nutrition --- ## HISTOPATHOLOGY REPORT **Report No.:** 1917/26 | **Date Reported:** 22 June 2026 ### Microscopic Findings: - **Multiple tissue types from all three germ layers** (confirms teratoma) - **Ectoderm:** Stratified squamous epithelium, sebaceous glands, keratin flakes, hair follicles - **Endoderm:** Mucinous epithelium with goblet cells, pseudostratified ciliated columnar epithelium (respiratory-type lining), well-formed glands with papillary structures - **Mesoderm:** Adipose (fat) tissue, fibrous stroma, cartilage, nerves - Chronic haemorrhage with hemosiderin-laden macrophages (old bleeding within the tumour) - Dense lymphocytic and plasma cell infiltrate - Cholesterol clefts - **No immature (malignant) elements identified** ### Final Diagnosis: # ✅ MATURE CYSTIC TERATOMA - Mediastinal Mass (BENIGN) --- ## DISCUSSION POINTS ### What is a Mediastinal Mature Cystic Teratoma? - A **germ cell tumour** arising from primordial germ cells in the anterior mediastinum - Contains derivatives of all 3 embryonic germ layers (hence "mature") - "Cystic" - forms fluid-filled cavities with cheesy/sebaceous content and hair - **Most common primary germ cell tumour of the mediastinum** - Predominantly occurs in **young adults (20-40 years)**, more common in females - Accounts for ~10-15% of all anterior mediastinal masses ("4 T's" = Thymoma, Teratoma, Terrible lymphoma, Thyroid) ### Why anterior mediastinum? - Primordial germ cells migrate from the yolk sac during embryogenesis; aberrant migration leads to extragonadal germ cell tumours at midline structures including the anterior mediastinum ### Classic CT Triad (seen in this case) 1. **Fat** (adipose tissue within the mass) 2. **Calcification** 3. **Soft tissue components** - This triad on CT is **pathognomonic (diagnostic)** of mature cystic teratoma ### Why surgery? - Teratomas grow progressively - Risk of **rupture** causing chemical mediastinitis or pericarditis - Can cause compression of trachea (as seen here - tracheal deviation), SVC, heart - Risk of **malignant transformation** (~1-3%) if left untreated - Complete surgical excision is **curative** ### Why was thyroid function (TSH) checked? - Anterior neck swelling can be due to a **substernal goitre** (enlarged thyroid extending into chest). Normal TSH + CT findings ruled this out. ### Why was NT-proBNP and Troponin checked? - The large mediastinal mass was adjacent to the heart and great vessels. These cardiac markers ruled out **cardiac compression, tamponade, or myocardial involvement** - essential before major thoracic surgery. --- ## KEY LEARNING POINTS 1. **Mediastinal teratomas present in young women** with anterior neck/chest swelling - often long-standing and slow-growing 2. **CT chest with contrast** is the gold standard investigation - fat + calcification + soft tissue = diagnostic triad 3. **Tracheal deviation** on CXR is a red flag indicating significant mass effect from a large mediastinal tumour 4. **Pre-operative workup** must include: CBC, coagulation, LFT, KFT, thyroid function, cardiac markers (NT-proBNP, Troponin), ECG, and infectious disease screening 5. **Median sternotomy** is the preferred surgical approach for anterior mediastinal tumours 6. Post-operatively, **pneumothorax and pleural effusion** are expected complications of thoracic surgery - managed with chest drains 7. **Histopathology is essential** - "mature" vs "immature" teratoma has major prognostic implications: - Mature = benign, surgery curative - Immature = malignant potential, needs chemotherapy/radiotherapy 8. **Hypoalbuminaemia** post major surgery is expected and reflects the acute inflammatory response + fluid shifts, not liver disease 9. This patient achieved **same-day extubation** and **complete lung recovery by POD-4** - reflecting excellent surgical and anaesthetic management 10. **Ayushman Bharat scheme** allowed this major complex surgery to be performed on a young patient from a lower-income background at no out-of-pocket cost --- ## OUTCOME - ✅ Complete surgical excision achieved - ✅ Histopathology: **Benign (Mature Cystic Teratoma)** - ✅ No malignant elements - **No adjuvant therapy required** - ✅ Post-op complications resolved by POD-4 - ✅ Discharged with follow-up appointment - **Prognosis: Excellent - Surgery is curative for mature cystic teratoma**Here is a complete, well-structured case presentation of Mrs. Roshani Sen, ready to present: --- # CASE PRESENTATION ## Anterior Mediastinal Mature Cystic Teratoma --- ## PATIENT PROFILE - **Name:** Mrs. Roshani Sen - **Age:** 26 years 10 months - **Sex:** Female - **DOB:** 05 August 1999 - **Address:** Gunjali, Sanawad, Madhya Pradesh - **Admission Date:** 09 June 2026 - **Hospital:** Parul Sevashram Hospital, Vadodara (CTVS Unit) - **Consultants:** Dr. Dipesh D. Duttaroy, Dr. Sagar Sahita (CTVS Surgeon) - **Insurance:** Ayushman Bharat Yojana (Government scheme) --- ## CHIEF COMPLAINT - **Anterior neck swelling** since **1 year** - Associated **chest heaviness and chest pain** --- ## HISTORY OF PRESENTING ILLNESS - Young female, 26 years old, presenting with gradually progressive swelling in the anterior neck region for 1 year - Swelling extended into the chest (retrosternal region) - Associated with a sensation of heaviness and discomfort in the chest - No fever, no weight loss, no dysphagia, no dyspnoea at rest - No history of trauma - No prior surgery or hospitalisation - Self-referred (direct referral) --- ## PAST HISTORY - No Diabetes Mellitus - No Hypertension - No known cardiac disease - No tuberculosis - No asthma - No known drug, food, or latex allergies --- ## EXAMINATION ON ADMISSION ### Vital Signs - **BP:** 110/70 mmHg - **SpO₂:** 94% (room air) - **Temperature:** Normal - **Pulse:** Normal - **Respiratory rate:** 19 breaths/min ### General Examination - Conscious, oriented, cooperative - No cyanosis, no jaundice, no pallor (mild) - No significant lymphadenopathy noted ### Local Examination - Anterior neck swelling palpable - Mass extending retrosternally ### Systemic Examination - Respiratory: Normal air entry bilaterally - Cardiovascular: Normal heart sounds - Abdomen: Soft, non-tender --- ## INVESTIGATIONS ### Imaging #### CT Neck & Chest (26 May 2026 - Pre-admission) - Large, **well-defined mixed-density mass measuring 8.3 × 5.1 × 12.2 cm** - Involving the **lower neck and retrosternal region** - Mass contains **fat + calcification + soft tissue** - classic triad of a mature cystic teratoma - Diagnosis suggested: **Mature Cystic Teratoma** #### Chest X-Ray PA View (15 June 2026 - Pre-op) - **Homogeneous opacity in the anterior mediastinum** (the mass) - **Tracheal deviation** to the contralateral side - indicating significant mass effect - Both lungs otherwise clear - Heart size normal #### ECG (15 June 2026 - Pre-op) - **HR: 81/min** - Normal sinus rhythm - **PR: 159 ms** - Normal - **QRS: 65 ms** - Normal - **QTc: 382 ms** - Normal - Conclusion: **Normal ECG, no cardiac involvement** --- ### Blood Investigations #### Complete Blood Count (CBC) | Parameter | Value | Reference | Status | |-----------|-------|-----------|--------| | Haemoglobin | 11.7 g/dL | 12.0-15.0 | ⬇ Mildly low | | RBC | 4.20 million/µL | 4.5-5.5 | ⬇ Low | | WBC | 5710/µL | 4000-10000 | ✅ Normal | | Platelets | 278,000/µL | 150,000-450,000 | ✅ Normal | - **Mild normocytic anaemia** - likely anaemia of chronic disease from long-standing mass #### Coagulation Profile | Test | Value | Reference | Status | |------|-------|-----------|--------| | PT | 12.8 sec | 9.39-12.91 | ✅ Normal | | INR | 1.13 | 0.8-1.1 | ⬆ Borderline | | APTT | 32.8 sec | 22.7-35.0 | ✅ Normal | - Mildly elevated INR - not a contraindication to surgery #### Biochemistry | Test | Value | Status | |------|-------|--------| | CRP | 1.64 mg/L | ✅ Normal (<5) - No inflammation | | TSH | 1.920 µIU/mL | ✅ Normal - Thyroid origin ruled out | | NT-proBNP | 38.8 pg/mL | ✅ Normal (<300) - No heart failure | | Procalcitonin | 0.05 ng/mL | ✅ Normal - No sepsis | | Troponin I (hs) | <1.5 ng/L | ✅ Normal - No cardiac injury | | HbA1c | 4.8% | ✅ Non-diabetic | | Serum Creatinine | 0.6 mg/dL | ✅ Normal - Kidneys healthy | | eGFR | 120.8 mL/min | ✅ Stage 1 - Normal | | SGPT/SGOT | 14 / 19 U/L | ✅ Normal - Liver healthy | | Albumin | 3.9 g/dL | ✅ Normal | | Na / K | 135 / 4.3 mmol/L | ⚠ Na mildly low; K normal | #### Infectious Disease Screening (Pre-op) | Test | Result | |------|--------| | HBsAg | ✅ Negative | | Anti-HCV | ✅ Non-reactive | | HIV 1 & 2 | ✅ Non-reactive | | RPR (Syphilis) | ✅ Non-reactive | - All 4 mandatory pre-operative screens: **NEGATIVE** #### Urine Examination - Routine urine examination: **Normal** - No infection, no proteinuria, no glucosuria --- ## DIAGNOSIS > **Anterior Mediastinal Mass - Mature Cystic Teratoma** - Clinical diagnosis confirmed by CT imaging - Histopathologically proven post-excision --- ## SURGICAL MANAGEMENT ### Operation: **Anterior Mediastinal Mass Excision (Teratoma Excision)** | Detail | Information | |--------|-------------| | **Date of Surgery** | 16 June 2026 | | **Surgeon** | Dr. Sagar Sahita (CTVS Surgeon) | | **Approach** | Median Sternotomy (breastbone cut and wired back) | | **Anaesthesia** | General Anaesthesia (ET tube size 7.5) | | **Anaesthetist** | Dr. Kaushik Dhami | | **Duration** | Several hours (major thoracic procedure) | | **Blood Products Used** | Packed cells (PCV) + FFP (Fresh Frozen Plasma) | ### Intraoperative Details - Patient intubated and placed on general anaesthesia - Median sternotomy performed for access to anterior mediastinum - Mass excised completely - Right-sided ICD (Intercostal Chest Drain) inserted post-excision - Right Femoral CVC line placed - Intraoperative ABG monitoring performed - Patient **extubated at 3:30 PM** on the same day (same-day extubation - a good outcome) - Transferred to **CICU (Cardiac ICU)** post-operatively ### Gross Specimen - Specimen size: **14 × 7.0 × 4.7 cm** - External surface: smooth, congested - Cut section: **cheesy necrotic material** drained from cystic areas - **Hair shafts** identified within the lesion --- ## POST-OPERATIVE COURSE | Day | Date | Status | |-----|------|--------| | **Op Day** | 16 Jun | Teratoma excised; 2 ICDs in situ; extubated 3:30 PM; admitted CICU | | **POD-1** | 17 Jun | Stable in CICU; chest drains functioning; CXR normal | | **POD-2** | 18 Jun | ⚠ Morning CXR: Right pneumothorax + right pleural effusion - managed with existing drains; Afternoon CXR: Both lungs cleared | | **POD-3** | 19 Jun | Small left minimal pleural effusion; right improving; Hb 9.8 g/dL | | **POD-4** | 20 Jun | CXR completely normal; both costophrenic angles clear; drains removed | | **POD-5/6** | 21-22 Jun | Pain managed; ambulating; discharge planning | ### Post-Op Complications (managed successfully) 1. **Right-sided pneumothorax** (POD-2) - resolved with drain management 2. **Right pleural effusion with consolidation** (POD-2) - resolved within hours 3. **Small left minimal pleural effusion** (POD-3) - resolved spontaneously by POD-4 4. **Post-op anaemia** (Hb dropped from 11.9 → 9.8 g/dL) - managed with blood transfusion 5. **Hypoalbuminaemia** (Albumin dropped 3.9 → 2.6 g/dL post-op) - expected post-surgical acute-phase response, managed with nutrition --- ## HISTOPATHOLOGY REPORT **Report No.:** 1917/26 | **Date Reported:** 22 June 2026 ### Microscopic Findings: - **Multiple tissue types from all three germ layers** (confirms teratoma) - **Ectoderm:** Stratified squamous epithelium, sebaceous glands, keratin flakes, hair follicles - **Endoderm:** Mucinous epithelium with goblet cells, pseudostratified ciliated columnar epithelium (respiratory-type lining), well-formed glands with papillary structures - **Mesoderm:** Adipose (fat) tissue, fibrous stroma, cartilage, nerves - Chronic haemorrhage with hemosiderin-laden macrophages (old bleeding within the tumour) - Dense lymphocytic and plasma cell infiltrate - Cholesterol clefts - **No immature (malignant) elements identified** ### Final Diagnosis: # ✅ MATURE CYSTIC TERATOMA - Mediastinal Mass (BENIGN) --- ## DISCUSSION POINTS ### What is a Mediastinal Mature Cystic Teratoma? - A **germ cell tumour** arising from primordial germ cells in the anterior mediastinum - Contains derivatives of all 3 embryonic germ layers (hence "mature") - "Cystic" - forms fluid-filled cavities with cheesy/sebaceous content and hair - **Most common primary germ cell tumour of the mediastinum** - Predominantly occurs in **young adults (20-40 years)**, more common in females - Accounts for ~10-15% of all anterior mediastinal masses ("4 T's" = Thymoma, Teratoma, Terrible lymphoma, Thyroid) ### Why anterior mediastinum? - Primordial germ cells migrate from the yolk sac during embryogenesis; aberrant migration leads to extragonadal germ cell tumours at midline structures including the anterior mediastinum ### Classic CT Triad (seen in this case) 1. **Fat** (adipose tissue within the mass) 2. **Calcification** 3. **Soft tissue components** - This triad on CT is **pathognomonic (diagnostic)** of mature cystic teratoma ### Why surgery? - Teratomas grow progressively - Risk of **rupture** causing chemical mediastinitis or pericarditis - Can cause compression of trachea (as seen here - tracheal deviation), SVC, heart - Risk of **malignant transformation** (~1-3%) if left untreated - Complete surgical excision is **curative** ### Why was thyroid function (TSH) checked? - Anterior neck swelling can be due to a **substernal goitre** (enlarged thyroid extending into chest). Normal TSH + CT findings ruled this out. ### Why was NT-proBNP and Troponin checked? - The large mediastinal mass was adjacent to the heart and great vessels. These cardiac markers ruled out **cardiac compression, tamponade, or myocardial involvement** - essential before major thoracic surgery. --- ## KEY LEARNING POINTS 1. **Mediastinal teratomas present in young women** with anterior neck/chest swelling - often long-standing and slow-growing 2. **CT chest with contrast** is the gold standard investigation - fat + calcification + soft tissue = diagnostic triad 3. **Tracheal deviation** on CXR is a red flag indicating significant mass effect from a large mediastinal tumour 4. **Pre-operative workup** must include: CBC, coagulation, LFT, KFT, thyroid function, cardiac markers (NT-proBNP, Troponin), ECG, and infectious disease screening 5. **Median sternotomy** is the preferred surgical approach for anterior mediastinal tumours 6. Post-operatively, **pneumothorax and pleural effusion** are expected complications of thoracic surgery - managed with chest drains 7. **Histopathology is essential** - "mature" vs "immature" teratoma has major prognostic implications: - Mature = benign, surgery curative - Immature = malignant potential, needs chemotherapy/radiotherapy 8. **Hypoalbuminaemia** post major surgery is expected and reflects the acute inflammatory response + fluid shifts, not liver disease 9. This patient achieved **same-day extubation** and **complete lung recovery by POD-4** - reflecting excellent surgical and anaesthetic management 10. **Ayushman Bharat scheme** allowed this major complex surgery to be performed on a young patient from a lower-income background at no out-of-pocket cost --- ## OUTCOME - ✅ Complete surgical excision achieved - ✅ Histopathology: **Benign (Mature Cystic Teratoma)** - ✅ No malignant elements - **No adjuvant therapy required** - ✅ Post-op complications resolved by POD-4 - ✅ Discharged with follow-up appointment - **Prognosis: Excellent - Surgery is curative for mature cystic teratoma**
ls -la /tmp/workspace/ 2>/dev/null || mkdir -p /tmp/workspace && echo "workspace ready"
mkdir -p /tmp/workspace/roshani-poster && echo "dir created"
~/roshani-poster/build_poster.py
"""
Poster: Awake Fiberoptic Intubation in Anterior Mediastinal Mass (Mature Cystic Teratoma)
A4 landscape poster for PG/Resident level conference presentation.
Layout: 3-column (Introduction + Case | Anaesthesia Management | Discussion + Outcome)
"""
from pptx import Presentation
from pptx.util import Inches, Pt, Emu
from pptx.dml.color import RGBColor
from pptx.enum.text import PP_ALIGN, MSO_ANCHOR
from pptx.oxml.ns import qn
from lxml import etree
import copy
# ── Colour Palette ───────────────────────────────────────────────────────────
NAVY = RGBColor(0x0D, 0x2C, 0x54) # deep navy – header bg / borders
TEAL = RGBColor(0x00, 0x7A, 0x8E) # teal – section titles
ACCENT = RGBColor(0xE8, 0x55, 0x00) # burnt orange – highlights / alerts
WHITE = RGBColor(0xFF, 0xFF, 0xFF)
LIGHT_BG = RGBColor(0xF0, 0xF5, 0xFA) # very pale blue for box backgrounds
MID_GRAY = RGBColor(0x55, 0x55, 0x55)
DARK = RGBColor(0x1A, 0x1A, 0x2E)
GREEN_OK = RGBColor(0x15, 0x7A, 0x3A)
ORANGE_W = RGBColor(0xCC, 0x66, 0x00)
# ── Slide size: A0 poster landscape (33.1 × 23.4 in) ────────────────────────
W = Inches(33.1)
H = Inches(23.4)
prs = Presentation()
prs.slide_width = W
prs.slide_height = H
blank = prs.slide_layouts[6]
slide = prs.slides.add_slide(blank)
# ── Helper functions ─────────────────────────────────────────────────────────
def rect(slide, x, y, w, h, fill=None, line=None, line_w=None):
"""Add a filled/bordered rectangle."""
shape = slide.shapes.add_shape(
1, # MSO_SHAPE_TYPE.RECTANGLE
x, y, w, h
)
shape.line.fill.background()
if fill:
shape.fill.solid()
shape.fill.fore_color.rgb = fill
else:
shape.fill.background()
if line:
shape.line.color.rgb = line
if line_w:
shape.line.width = line_w
else:
shape.line.fill.background()
return shape
def tb(slide, x, y, w, h, text, size=14, bold=False, color=DARK,
align=PP_ALIGN.LEFT, wrap=True, italic=False, anchor=MSO_ANCHOR.TOP):
"""Add a text box."""
box = slide.shapes.add_textbox(x, y, w, h)
tf = box.text_frame
tf.word_wrap = wrap
tf.vertical_anchor = anchor
tf.margin_left = Inches(0.05)
tf.margin_right = Inches(0.05)
tf.margin_top = Inches(0.04)
tf.margin_bottom= Inches(0.04)
p = tf.paragraphs[0]
p.alignment = align
run = p.add_run()
run.text = text
run.font.name = "Calibri"
run.font.size = Pt(size)
run.font.bold = bold
run.font.italic = italic
run.font.color.rgb = color
return box, tf
def add_para(tf, text, size=13, bold=False, color=DARK,
align=PP_ALIGN.LEFT, italic=False, space_before=0, bullet=False):
"""Append a paragraph to an existing text frame."""
from pptx.oxml import parse_xml
p_elem = tf.add_paragraph()
p_elem.alignment = align
if space_before:
p_elem.space_before = Pt(space_before)
run = p_elem.add_run()
run.text = text
run.font.name = "Calibri"
run.font.size = Pt(size)
run.font.bold = bold
run.font.italic = italic
run.font.color.rgb = color
if bullet:
# simple bullet via unicode
run.text = "• " + text
return p_elem
def section_header(slide, x, y, w, h, title):
"""Teal section header bar with white text."""
rect(slide, x, y, w, h, fill=TEAL)
tb(slide, x + Inches(0.1), y, w - Inches(0.2), h,
title, size=18, bold=True, color=WHITE,
align=PP_ALIGN.LEFT, anchor=MSO_ANCHOR.MIDDLE)
def content_box(slide, x, y, w, h, bg=LIGHT_BG, border=TEAL, border_w=Pt(1)):
"""Pale background box with teal border."""
rect(slide, x, y, w, h, fill=bg, line=border, line_w=border_w)
# ═══════════════════════════════════════════════════════════════════════════
# HEADER BANNER
# ═══════════════════════════════════════════════════════════════════════════
MARGIN = Inches(0.3)
HEADER_H = Inches(2.2)
rect(slide, 0, 0, W, HEADER_H, fill=NAVY)
# Title
tb(slide, MARGIN, Inches(0.12), W - 2*MARGIN, Inches(1.05),
"Awake Fiberoptic Intubation for Excision of Anterior Mediastinal Mature Cystic Teratoma",
size=40, bold=True, color=WHITE, align=PP_ALIGN.CENTER, anchor=MSO_ANCHOR.MIDDLE)
# Sub-title line
tb(slide, MARGIN, Inches(1.1), W - 2*MARGIN, Inches(0.5),
"A Case Report with Focus on Anaesthetic Management of a Compressed Airway",
size=22, bold=False, italic=True, color=RGBColor(0xB0, 0xD4, 0xF1),
align=PP_ALIGN.CENTER, anchor=MSO_ANCHOR.MIDDLE)
# Authors
tb(slide, MARGIN, Inches(1.6), W - 2*MARGIN, Inches(0.45),
"Dr. Kaushik Dhami (Anaesthesiologist) | Dr. Sagar Sahita (CTVS Surgeon) | Dr. Dipesh D. Duttaroy | "
"Parul Sevashram Hospital, Vadodara, Gujarat",
size=17, bold=False, color=RGBColor(0xCC, 0xE5, 0xFF),
align=PP_ALIGN.CENTER, anchor=MSO_ANCHOR.MIDDLE)
# ── Teal accent line under header ───
rect(slide, 0, HEADER_H, W, Inches(0.06), fill=TEAL)
# ═══════════════════════════════════════════════════════════════════════════
# BODY LAYOUT – 3 columns
# ═══════════════════════════════════════════════════════════════════════════
BODY_TOP = HEADER_H + Inches(0.18)
BODY_H = H - BODY_TOP - Inches(0.55) # leave footer strip
COL_GAP = Inches(0.22)
COL_W = (W - 2*MARGIN - 2*COL_GAP) / 3
C1_X = MARGIN
C2_X = C1_X + COL_W + COL_GAP
C3_X = C2_X + COL_W + COL_GAP
SH = Inches(0.45) # section header height
PAD = Inches(0.14) # inner padding
# ─────────────────────────────────────────────────────────────────────────
# COLUMN 1 – Introduction + Patient Profile + Pre-op Investigations
# ─────────────────────────────────────────────────────────────────────────
cy = BODY_TOP
# ── Introduction ──────────────────────────────────────────────────────────
section_header(slide, C1_X, cy, COL_W, SH, "Introduction")
cy += SH
bh = Inches(4.5)
content_box(slide, C1_X, cy, COL_W, bh)
_, itf = tb(slide, C1_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"Background", size=15, bold=True, color=NAVY)
add_para(itf,
"Anterior mediastinal masses (AMM) represent 10-15% of all mediastinal tumours. "
"The \"4 T's\" of the anterior mediastinum are: Thymoma, Teratoma, Terrible lymphoma, "
"and Thyroid. Mature cystic teratomas are benign germ cell tumours arising from all "
"three embryonic layers (ectoderm, mesoderm, endoderm).",
size=13, bullet=False)
add_para(itf, "", size=6)
add_para(itf, "Anaesthetic Challenge", size=15, bold=True, color=NAVY)
add_para(itf,
"A large AMM compressing the trachea poses one of the most challenging airway "
"management scenarios in anaesthesia. General anaesthesia + paralysis can precipitate "
"life-threatening airway collapse through three mechanisms:",
size=13)
add_para(itf, "1. Reduced lung volumes decrease tracheal diameter", size=13, color=MID_GRAY)
add_para(itf, "2. Smooth muscle relaxation increases airway compressibility", size=13, color=MID_GRAY)
add_para(itf, "3. Paralysis eliminates spontaneous ventilation that maintains patency", size=13, color=MID_GRAY)
add_para(itf, "", size=6)
add_para(itf,
"Awake Fiberoptic Intubation (AFOI) is the gold-standard technique when tracheal "
"compression is anticipated, preserving spontaneous breathing and airway tone until "
"the tube is safely in situ.",
size=13, bold=False, color=DARK)
cy += bh + Inches(0.18)
# ── Patient Profile ────────────────────────────────────────────────────────
section_header(slide, C1_X, cy, COL_W, SH, "Patient Profile")
cy += SH
bh = Inches(2.8)
content_box(slide, C1_X, cy, COL_W, bh)
_, ptf = tb(slide, C1_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"Mrs. Roshani Sen | 26 Years | Female", size=15, bold=True, color=NAVY)
add_para(ptf, "Parul Sevashram Hospital, Vadodara (CTVS Unit) | Admission: 09 June 2026",
size=13, italic=True, color=MID_GRAY)
add_para(ptf, "", size=5)
add_para(ptf, "• Chief complaint: Anterior neck swelling × 1 year + chest heaviness", size=13)
add_para(ptf, "• Gradual progression, no dyspnoea at rest, no fever, no weight loss", size=13)
add_para(ptf, "• No prior surgery / hospitalisation. No known allergies", size=13)
add_para(ptf, "• SpO₂: 94% (room air) | BP: 110/70 mmHg | RR: 19/min", size=13)
add_para(ptf, "• Mild normocytic anaemia (Hb 11.7 g/dL). All other parameters normal", size=13)
add_para(ptf, "• Covered under Ayushman Bharat Yojana (government insurance)", size=13, italic=True, color=MID_GRAY)
cy += bh + Inches(0.18)
# ── Pre-op Investigations ─────────────────────────────────────────────────
section_header(slide, C1_X, cy, COL_W, SH, "Pre-operative Investigations")
cy += SH
bh = BODY_TOP + BODY_H - cy - Inches(0.05)
content_box(slide, C1_X, cy, COL_W, bh)
_, itf2 = tb(slide, C1_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"CT Neck & Chest (26 May 2026)", size=15, bold=True, color=NAVY)
add_para(itf2,
"Well-defined mixed-density mass 8.3 × 5.1 × 12.2 cm spanning lower neck + retrosternal region. "
"Classic diagnostic triad: fat + calcification + soft tissue components → Mature Cystic Teratoma.",
size=13)
add_para(itf2, "", size=6)
add_para(itf2, "Chest X-Ray PA (15 June 2026)", size=15, bold=True, color=NAVY)
add_para(itf2,
"Homogeneous anterior mediastinal opacity with tracheal deviation — "
"indicating significant mass effect on airway.", size=13)
add_para(itf2, " ⚠ Tracheal deviation = RED FLAG for airway compression", size=13,
bold=True, color=ACCENT)
add_para(itf2, "", size=6)
add_para(itf2, "ECG (15 June 2026)", size=15, bold=True, color=NAVY)
add_para(itf2, "Normal sinus rhythm, HR 81/min, QTc 382 ms — No cardiac involvement", size=13)
add_para(itf2, "", size=6)
add_para(itf2, "Key Blood Work", size=15, bold=True, color=NAVY)
add_para(itf2, " Hb 11.7 g/dL (mild anaemia) | INR 1.13 (borderline, not a contraindication)", size=13)
add_para(itf2, " TSH 1.92 µIU/mL ✓ | NT-proBNP 38.8 pg/mL ✓ | Troponin I <1.5 ng/L ✓", size=13, color=GREEN_OK)
add_para(itf2, " HBsAg / HCV / HIV / VDRL — all NEGATIVE ✓", size=13, color=GREEN_OK)
add_para(itf2, " Serum Creatinine 0.6 / SGPT 14 / SGOT 19 — normal organ function ✓", size=13, color=GREEN_OK)
# ─────────────────────────────────────────────────────────────────────────
# COLUMN 2 – Anaesthetic Management (FULL FOCUS)
# ─────────────────────────────────────────────────────────────────────────
cy = BODY_TOP
# ── Pre-op Airway Assessment ───────────────────────────────────────────────
section_header(slide, C2_X, cy, COL_W, SH, "Pre-op Anaesthetic Assessment & Airway Planning")
cy += SH
bh = Inches(3.5)
content_box(slide, C2_X, cy, COL_W, bh)
_, atf = tb(slide, C2_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"Why was AFOI Chosen?", size=15, bold=True, color=NAVY)
add_para(atf,
"CT chest showed large mass (8.3 × 5.1 × 12.2 cm) with tracheal deviation. "
"CXR confirmed compression. SpO₂ 94% at rest indicated early respiratory compromise. "
"Decision: Awake fiberoptic intubation (AFOI) to secure airway before any induction agent "
"or muscle relaxant.",
size=13)
add_para(atf, "", size=5)
add_para(atf, "Pre-op Airway Checklist", size=15, bold=True, color=NAVY)
add_para(atf, " ✓ Pre-op CXR reviewed — tracheal deviation noted", size=13, color=GREEN_OK)
add_para(atf, " ✓ CT chest/neck reviewed — 8.3 × 5.1 × 12.2 cm mass, fat + Ca²⁺ triad", size=13, color=GREEN_OK)
add_para(atf, " ✓ Fiberoptic bronchoscope: equipment checked, light source tested", size=13, color=GREEN_OK)
add_para(atf, " ✓ Vocal cord mobility assessed pre-op (VC quick ✓)", size=13, color=GREEN_OK)
add_para(atf, " ✓ IV access established, monitors attached (SpO₂, ECG, NIBP)", size=13, color=GREEN_OK)
add_para(atf, " ✓ Surgeon informed; CPB standby available if airway lost", size=13, color=GREEN_OK)
add_para(atf, " ✓ Patient counselled, consented and cooperative", size=13, color=GREEN_OK)
cy += bh + Inches(0.18)
# ── AFOI Step-by-Step ─────────────────────────────────────────────────────
section_header(slide, C2_X, cy, COL_W, SH, "Anaesthetic Technique: Step-by-Step AFOI Protocol")
cy += SH
bh = Inches(7.4)
content_box(slide, C2_X, cy, COL_W, bh, bg=RGBColor(0xF5, 0xFB, 0xFF))
_, stf = tb(slide, C2_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"STEP 1 — Antisialagogue (Glycopyrrolate 0.2 mg IV)", size=14, bold=True, color=TEAL)
add_para(stf,
"Given 30 min before procedure to reduce secretions, improve visualisation, "
"and enhance topical anaesthetic contact with mucosa.",
size=13)
add_para(stf, "", size=7)
add_para(stf, "STEP 2 — Topical Airway Anaesthesia: Nebulisation", size=14, bold=True, color=TEAL)
add_para(stf,
"Lignocaine 4% × 2 mL + Normal Saline 2 mL via face mask nebuliser.",
size=13, bold=True, color=DARK)
add_para(stf,
"Patient inhales nebulised lignocaine for 10–15 min. Anaesthetises oropharynx, "
"larynx and upper trachea. Suppresses gag reflex and cough, reduces discomfort during scope passage.",
size=13)
add_para(stf, "", size=7)
add_para(stf, "STEP 3 — Transtracheal Block (Cricotracheal Injection)", size=14, bold=True, color=TEAL)
add_para(stf,
"Lignocaine 2% × 2 mL + Bupivacaine 0.5% × 2 mL injected through cricothyroid membrane.",
size=13, bold=True, color=DARK)
add_para(stf,
"Needle inserted through cricothyroid membrane; aspiration confirms intratracheal position. "
"Rapid injection followed by cough reflex — this sprays drug upward over vocal cords "
"and downward to carina, achieving dense tracheal anaesthesia.",
size=13)
add_para(stf, "", size=7)
add_para(stf, "STEP 4 — Conscious Sedation (if tolerated)", size=14, bold=True, color=TEAL)
add_para(stf,
"Judicious IV Midazolam + Fentanyl (or Dexmedetomidine infusion) to produce calm, "
"cooperative state. Patient must remain responsive and protect airway. "
"NO deep sedation — airway tone must be preserved.",
size=13)
add_para(stf, "", size=7)
add_para(stf, "STEP 5 — Fiberoptic Bronchoscope (FOB) Guided Intubation", size=14, bold=True, color=TEAL)
add_para(stf,
"ETT size 7.5 pre-loaded onto FOB. Scope passed orally under direct vision through "
"pharynx → cords → trachea, confirming carina visualisation. "
"ETT then railroaded over scope into trachea. Cuff inflated, CO₂ confirmed, scope withdrawn.",
size=13)
add_para(stf, "", size=7)
add_para(stf, "STEP 6 — General Anaesthesia Induced AFTER Tube Confirmed", size=14, bold=True, color=TEAL)
add_para(stf,
"Only after ETCO₂ waveform confirmed and tube position verified: "
"Propofol + Rocuronium (or Vecuronium) given to deepen anaesthesia for surgical incision. "
"Muscle relaxant safe ONLY once airway is secured.",
size=13, bold=False)
add_para(stf, " ⚠ NEVER give a paralytic before securing airway in tracheal compression!",
size=13, bold=True, color=ACCENT)
cy += bh + Inches(0.18)
# ── Intraoperative Monitoring ─────────────────────────────────────────────
section_header(slide, C2_X, cy, COL_W, SH, "Intraoperative Anaesthetic Management")
cy += SH
bh = BODY_TOP + BODY_H - cy - Inches(0.05)
content_box(slide, C2_X, cy, COL_W, bh)
_, imtf = tb(slide, C2_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"Monitoring & Access", size=15, bold=True, color=NAVY)
add_para(imtf, " • SpO₂, ETCO₂, ECG, NIBP — standard 5-lead monitoring", size=13)
add_para(imtf, " • Right Femoral CVC — central venous access for major thoracic surgery", size=13)
add_para(imtf, " • Serial intraoperative ABG monitoring — acid-base & oxygenation", size=13)
add_para(imtf, " • ET tube size 7.5 (cuffed oral) — ET intubation confirmed by ETCO₂", size=13)
add_para(imtf, "", size=5)
add_para(imtf, "Intraoperative Events", size=15, bold=True, color=NAVY)
add_para(imtf, " • Median sternotomy for complete mass excision", size=13)
add_para(imtf, " • Blood products: Packed cells (PCV) + FFP given intraoperatively", size=13)
add_para(imtf, " • Right-sided ICD inserted at end of procedure", size=13)
add_para(imtf, "", size=5)
add_para(imtf, "Extubation", size=15, bold=True, color=NAVY)
add_para(imtf,
"Same-day extubation at 15:30 hrs — patient fully awake, SpO₂ >98%, "
"adequate tidal volume, following commands. Transferred to CICU.",
size=13, bold=False)
add_para(imtf, " ✓ Same-day extubation = excellent anaesthetic and surgical outcome", size=13,
bold=True, color=GREEN_OK)
# ─────────────────────────────────────────────────────────────────────────
# COLUMN 3 – Case Summary + Histopath + Post-op + Discussion + Conclusion
# ─────────────────────────────────────────────────────────────────────────
cy = BODY_TOP
# ── Surgical Procedure ───────────────────────────────────────────────────
section_header(slide, C3_X, cy, COL_W, SH, "Surgical Procedure")
cy += SH
bh = Inches(2.4)
content_box(slide, C3_X, cy, COL_W, bh)
_, srtf = tb(slide, C3_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"Date: 16 June 2026 | Median Sternotomy", size=14, bold=True, color=NAVY)
add_para(srtf, "Approach: Median sternotomy — standard for anterior mediastinal tumours", size=13)
add_para(srtf, "Complete en-bloc excision of teratoma achieved", size=13)
add_para(srtf, "Specimen: 14 × 7.0 × 4.7 cm — cheesy material + hair shafts on cut section", size=13)
add_para(srtf, "Post-excision right ICD placed | Right femoral CVC in situ", size=13)
cy += bh + Inches(0.18)
# ── Histopathology ────────────────────────────────────────────────────────
section_header(slide, C3_X, cy, COL_W, SH, "Histopathology Report (Rpt No. 1917/26 — 22 Jun 2026)")
cy += SH
bh = Inches(3.5)
content_box(slide, C3_X, cy, COL_W, bh, bg=RGBColor(0xF0, 0xFB, 0xF4))
_, htf = tb(slide, C3_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"All Three Germ Layers Confirmed", size=15, bold=True, color=NAVY)
add_para(htf, "Ectoderm:", size=14, bold=True, color=TEAL)
add_para(htf, " Stratified squamous epithelium, sebaceous glands, keratin flakes, hair follicles", size=13)
add_para(htf, "Endoderm:", size=14, bold=True, color=TEAL)
add_para(htf, " Mucinous epithelium (goblet cells), pseudostratified ciliated columnar epithelium, "
"well-formed glands with papillary structures", size=13)
add_para(htf, "Mesoderm:", size=14, bold=True, color=TEAL)
add_para(htf, " Adipose tissue, fibrous stroma, cartilage, nerves", size=13)
add_para(htf, "Also: Cholesterol clefts, hemosiderin-laden macrophages, lymphocytic infiltrate", size=13, color=MID_GRAY)
add_para(htf, "", size=5)
add_para(htf, " ✅ NO IMMATURE (MALIGNANT) ELEMENTS → BENIGN TERATOMA", size=15,
bold=True, color=GREEN_OK)
cy += bh + Inches(0.18)
# ── Post-operative Course ─────────────────────────────────────────────────
section_header(slide, C3_X, cy, COL_W, SH, "Post-operative Course")
cy += SH
bh = Inches(3.2)
content_box(slide, C3_X, cy, COL_W, bh)
_, potf = tb(slide, C3_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"POD", size=14, bold=True, color=NAVY)
add_para(potf, "Op Day — Extubated 15:30 hrs; 2 ICDs in situ; transferred to CICU", size=13)
add_para(potf, "POD-1 — Stable; CXR normal; chest drains functioning well", size=13)
add_para(potf, "POD-2 — ⚠ Rt pneumothorax + pleural effusion on CXR → managed with drains; "
"afternoon CXR: lungs cleared", size=13, color=ORANGE_W)
add_para(potf, "POD-3 — Small left minimal pleural effusion; Hb 9.8 g/dL — transfusion given", size=13)
add_para(potf, "POD-4 — CXR completely normal; drains removed ✓", size=13, color=GREEN_OK)
add_para(potf, "POD-5/6 — Ambulating; pain controlled; discharge planning", size=13, color=GREEN_OK)
add_para(potf, "", size=5)
add_para(potf, "Complications (all resolved):", size=14, bold=True, color=NAVY)
add_para(potf, " Right pneumothorax (POD-2) | Pleural effusion bilateral (POD-2/3) | "
"Post-op anaemia | Hypoalbuminaemia (2.6 g/dL — acute phase response)", size=13, color=MID_GRAY)
cy += bh + Inches(0.18)
# ── Discussion ────────────────────────────────────────────────────────────
section_header(slide, C3_X, cy, COL_W, SH, "Discussion")
cy += SH
bh = Inches(4.0)
content_box(slide, C3_X, cy, COL_W, bh)
_, dtf = tb(slide, C3_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"Why AFOI is Mandatory in Tracheal Compression", size=15, bold=True, color=NAVY)
add_para(dtf,
"General anaesthesia + paralysis in an unprotected compressed airway risks complete "
"tracheal collapse — a catastrophic \"cannot ventilate, cannot intubate\" scenario. "
"AFOI allows the anaesthesiologist to visualise the airway in real time, pass the tube "
"under direct vision, and confirm position before any sedation or paralytic is given.",
size=13)
add_para(dtf, "", size=6)
add_para(dtf, "Key Anaesthetic Points in this Case", size=15, bold=True, color=NAVY)
add_para(dtf, " • SpO₂ 94% at rest → early respiratory compromise warranting AFOI", size=13)
add_para(dtf, " • Tracheal deviation on CXR → never attempt RSI without AFOI first", size=13)
add_para(dtf, " • Nebulised Lignocaine 4% + transtracheal block achieved full airway topicalisation", size=13)
add_para(dtf, " • Rocuronium given ONLY after ETCO₂ confirmed tube in trachea", size=13)
add_para(dtf, " • Same-day extubation reflects adequate pre-op optimisation and smooth conduct", size=13)
add_para(dtf, "", size=6)
add_para(dtf, "Mature vs Immature Teratoma (Prognostic Key)", size=15, bold=True, color=NAVY)
add_para(dtf, " Mature (this case) = Benign → surgery curative, no adjuvant therapy", size=13, color=GREEN_OK)
add_para(dtf, " Immature = Malignant potential → needs chemo ± radiotherapy", size=13, color=ACCENT)
cy += bh + Inches(0.18)
# ── Conclusion ────────────────────────────────────────────────────────────
section_header(slide, C3_X, cy, COL_W, SH, "Conclusion")
cy += SH
bh = BODY_TOP + BODY_H - cy - Inches(0.05)
content_box(slide, C3_X, cy, COL_W, bh, bg=RGBColor(0xF0, 0xFB, 0xF4))
_, ctf = tb(slide, C3_X+PAD, cy+PAD, COL_W-2*PAD, bh-2*PAD,
"Key Takeaways", size=15, bold=True, color=NAVY)
add_para(ctf,
"✅ AFOI is the technique of choice when a mediastinal mass causes tracheal compression — "
"it maintains spontaneous ventilation and provides real-time airway visualisation.",
size=14, bold=True, color=DARK)
add_para(ctf, "", size=5)
add_para(ctf,
"✅ Topical airway anaesthesia (nebulised Lignocaine 4% + transtracheal block) "
"enables smooth, comfortable passage of the fiberscope in the awake patient.",
size=13)
add_para(ctf, "", size=5)
add_para(ctf,
"✅ CT tracheal compression >50% is a red flag — this should prompt AFOI planning "
"regardless of absence of symptoms at rest.",
size=13)
add_para(ctf, "", size=5)
add_para(ctf,
"✅ Histopathological confirmation differentiates mature (benign) from immature "
"(malignant) teratoma — determining need for adjuvant therapy.",
size=13)
add_para(ctf, "", size=5)
add_para(ctf,
"✅ This case demonstrates that with careful anaesthetic planning, a large anterior "
"mediastinal mass can be safely excised with same-day extubation and full recovery.",
size=13, bold=True, color=GREEN_OK)
# ═══════════════════════════════════════════════════════════════════════════
# FOOTER STRIP
# ═══════════════════════════════════════════════════════════════════════════
FOOTER_Y = H - Inches(0.5)
rect(slide, 0, FOOTER_Y, W, Inches(0.5), fill=NAVY)
tb(slide, MARGIN, FOOTER_Y, W*0.5, Inches(0.5),
"Parul Sevashram Hospital, Vadodara | CTVS & Anaesthesia Department | 2026",
size=14, color=RGBColor(0xCC, 0xE5, 0xFF), anchor=MSO_ANCHOR.MIDDLE)
tb(slide, W*0.5, FOOTER_Y, W*0.5 - MARGIN, Inches(0.5),
"References: Miller's Anesthesia 10e • Cummings Otolaryngology • Barash Clinical Anesthesia 9e",
size=13, color=RGBColor(0xAA, 0xCC, 0xEE),
align=PP_ALIGN.RIGHT, anchor=MSO_ANCHOR.MIDDLE)
# ── Save ─────────────────────────────────────────────────────────────────
out = "/tmp/workspace/roshani-poster/AFOI_Mediastinal_Teratoma_Poster.pptx"
from io import BytesIO
buf = BytesIO()
prs.save(buf)
with open(out, "wb") as f:
f.write(buf.getvalue())
print(f"Saved: {out}")
cd /tmp/workspace/roshani-poster && python build_poster.py 2>&1
python -c " from pptx import Presentation prs = Presentation('/tmp/workspace/roshani-poster/AFOI_Mediastinal_Teratoma_Poster.pptx') print(f'Slides: {len(prs.slides)}') print(f'Width: {prs.slide_width.inches:.2f} in, Height: {prs.slide_height.inches:.2f} in') for i, slide in enumerate(prs.slides, 1): shapes = [s.name for s in slide.shapes] print(f'Slide {i}: {len(shapes)} shapes') for s in slide.shapes: if s.has_text_frame: txt = s.text_frame.text[:60].replace(chr(10),' ') if txt.strip(): print(f' [{txt}]') "
AFOI Mediastinal Teratoma Poster
Presentation · PPTX
What's in the poster
- Introduction: what AMMs are, the "4 T's", and why tracheal compression is an anaesthetic crisis
- Patient profile: Mrs. Roshani Sen, 26F, her complaint, vitals, SpO₂ 94%
- Pre-op investigations: CT findings (8.3 × 5.1 × 12.2 cm mass), CXR (tracheal deviation flagged in orange as a red flag), ECG, bloods
- Pre-op airway assessment checklist (why AFOI was chosen)
- Step-by-step AFOI protocol in full detail:
- Glycopyrrolate 0.2 mg IV (antisialagogue)
- Nebulised Lignocaine 4% (2 mL + 2 mL NS)
- Transtracheal block (Lignocaine 2% 2 mL + Bupivacaine 0.5% 2 mL through cricothyroid)
- Conscious sedation (Midazolam + Fentanyl / Dexmedetomidine)
- Fiberoptic bronchoscope guided intubation (ETT 7.5, railroaded over scope)
- GA + Rocuronium only AFTER ETCO₂ confirmed (with a bold orange warning never to paralyse first)
- Intraoperative monitoring: CVC, ABG, ETCO₂, same-day extubation at 15:30
- Median sternotomy, specimen details
- Histopath: all 3 germ layers, NO immature elements → Benign
- Post-op course day by day (complications + resolution)
- Discussion: why AFOI is mandatory, mature vs immature teratoma
- Conclusion: 5 green-highlighted takeaways