Mac types
Asking for Preferences
Could you clarify what you mean by "Mac types"? For example:
- Macrophage types (immunology/biology)?
- MAC (Mycobacterium avium complex) types?
- MAC protocol types in networking (Media Access Control)?
- Something completely different?
Let me know and I'll give you a thorough answer!
Minimum alveolar concentration
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a thorough overview of Minimum Alveolar Concentration (MAC):
Definition
MAC is the alveolar concentration of an inhaled anesthetic (expressed as volume % at 1 atmosphere) that prevents movement in response to a standardized noxious stimulus (e.g., surgical skin incision) in 50% of patients.
- It is analogous to the ED50 for IV drugs and the EC50 (plasma concentration for 50% effect).
- It directly mirrors brain partial pressure of the anesthetic, making it a reliable index of anesthetic depth.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 294
MAC Values of Common Inhaled Anesthetics
| Agent | MAC (%) |
|---|---|
| Nitrous oxide (N₂O) | 105% (requires hyperbaric conditions for 1 MAC) |
| Halothane | 0.75% |
| Isoflurane | 1.2% |
| Sevoflurane | 2.0% |
| Desflurane | 6.0% |
Values are for 30-55 year-old subjects at sea level. Lower MAC = more potent agent.
Key MAC Multiples
| Multiple | Clinical Meaning |
|---|---|
| 0.3-0.4 MAC | MAC-awake: patient wakes up (when volatile agent is the only anesthetic) |
| 0.4-0.5 MAC | Loss of consciousness / loss of recall |
| 1.0 MAC | Prevents movement in 50% of patients (ED50) |
| 1.2-1.3 MAC | Prevents movement in ~95% of patients (clinical dosing target) |
| 1.5 MAC | MAC-BAR: blunts adrenergic (stress) responses to noxious stimuli |
- MAC values are roughly additive - 0.5 MAC isoflurane + 0.5 MAC N₂O = 1.0 MAC effect for immobility.
- Additivity does not extend to all effects: cardiovascular depression is NOT equivalent at the same MAC across agents (e.g., halothane depresses the myocardium more than N₂O at 0.5 MAC).
- Barash Clinical Anesthesia, 9e, p. 1407
Factors That INCREASE MAC
- Increased CNS neurotransmitter levels: MAOIs, acute amphetamine, cocaine, ephedrine, levodopa
- Hyperthermia (temperature >42°C)
- Chronic ethanol abuse
- Hypernatremia
- Young age
- Red hair (MC1R gene variant - ~19% higher MAC)
Factors That DECREASE MAC
- Increasing age (~6% decrease per decade, linear from age 1 onward)
- Hypothermia
- Pregnancy (MAC decreased by ~1/3 at 8 weeks' gestation; normalizes by 72 hours postpartum)
- Metabolic acidosis
- Hypoxia (PaO₂ < 40 mmHg)
- Induced hypotension (MAP < 40-50 mmHg)
- Severe anemia (Hct < 10%)
- Hypercarbia (PaCO₂ > 95 mmHg - via CSF pH reduction)
- Drugs that decrease MAC: opioids, benzodiazepines, barbiturates, ketamine, local anesthetics (except cocaine), verapamil, lithium, alpha-2 agonists (clonidine, dexmedetomidine), methyldopa
- Acute alcohol intoxication
- Hyponatremia, hypercalcemia
Factors That Do NOT Alter MAC
- Duration of anesthetic administration
- Sex/gender
- Type of surgical stimulation
- Thyroid function (hyper or hypo)
- Hypo- or hypercarbia (within normal range)
- Metabolic alkalosis, hyperkalemia, magnesium levels
Barash Clinical Anesthesia, 9e, p. 1408-1409
Clinical Significance
- Potency comparison: Lower MAC = higher potency (e.g., halothane at 0.75% is more potent than desflurane at 6%).
- Meyer-Overton correlation: Anesthetic potency correlates with lipid solubility - the fat:water partition coefficient. More lipid-soluble agents have lower MAC.
- Spinal cord, not brain, mediates immobility: MAC is not altered by spinal cord transection, suggesting the motor suppression occurs at the spinal cord level - not the cortex.
- Median value limitation: MAC is a population median (ED50). It has limited use for individual patients, especially during rapidly changing alveolar concentrations (induction/emergence).
Miller's Anesthesia, 10e, p. 1807-1809
Cmro ,cbfand mac
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of the relationship between CMRO₂ (cerebral metabolic rate of oxygen), CBF (cerebral blood flow), and MAC for volatile anesthetics:
The Core Relationship
All volatile anesthetics have two opposing effects on the cerebral vasculature:
- Direct vasodilation - increases CBF
- Metabolic depression (↓ CMRO₂) - coupled decrease in CBF (vasoconstriction)
The net effect on CBF at any given dose is the balance of these two influences. This creates a characteristic pattern: CMRO₂ falls first and more steeply, while CBF changes are more complex and dose-dependent.
CBF and CMRO₂ vs. MAC - What the Data Shows
The graph below (from Miller's Anesthesia, 10e) illustrates this beautifully:
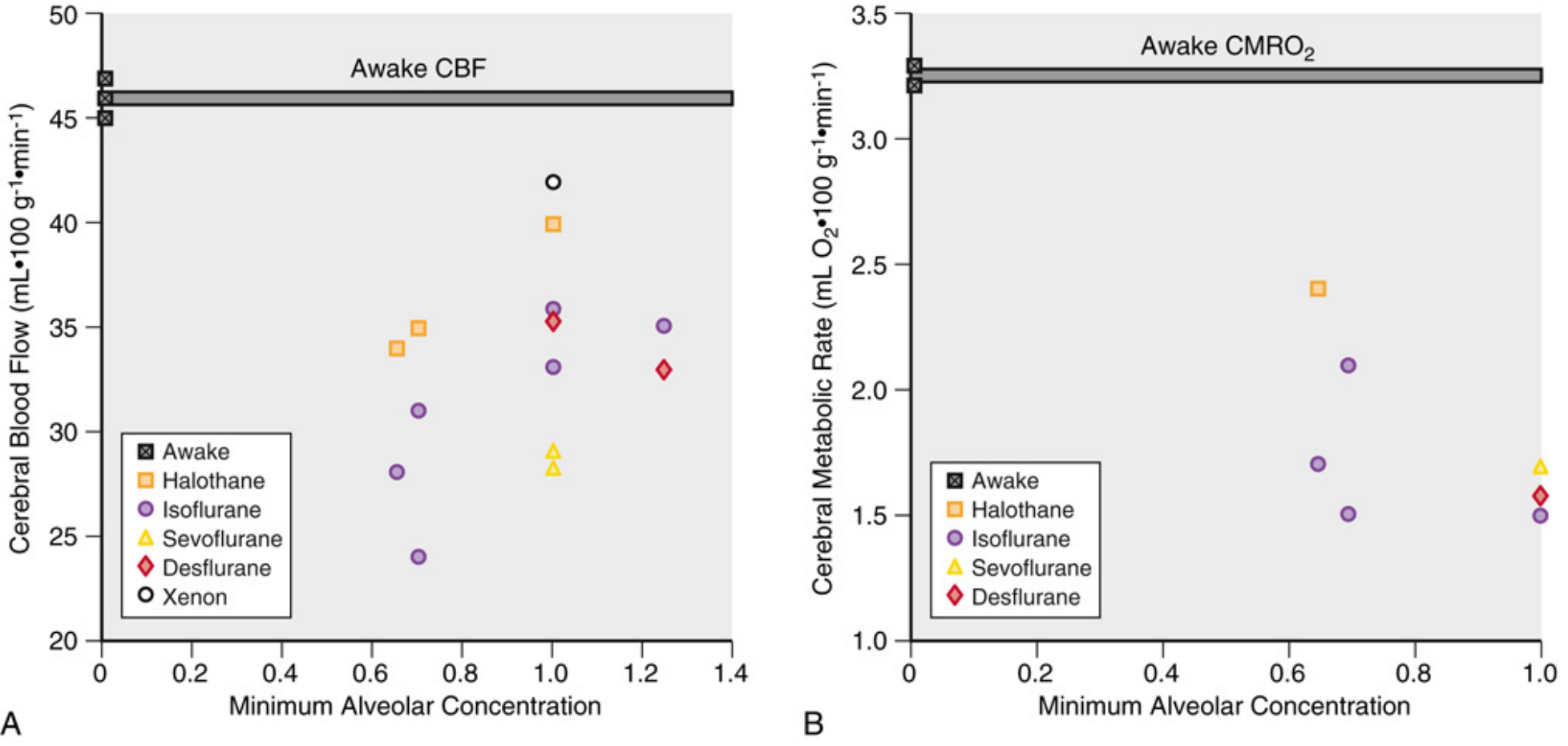
Panel A (CBF): Awake CBF ~46 mL/100g/min. Most agents decrease CBF below awake values at 0.5-1 MAC (especially sevoflurane and isoflurane), while halothane increases CBF even at moderate doses.
Panel B (CMRO₂): All agents progressively reduce CMRO₂ from the awake value (~3.3 mL O₂/100g/min) in a dose-dependent fashion.
Agent-by-Agent Summary at 1.0-1.1 MAC
| Agent | CBF change vs. awake | CMRO₂ change |
|---|---|---|
| Halothane | ↑ ~191% (massive vasodilation) | ↓ ~10% (minimal CMR suppression) |
| Enflurane | ↑ (significant increase) | ↓ ~15% |
| Isoflurane | ↑ ~19% (modest) | ↓ ~45% |
| Sevoflurane | ↓ ~38-50% | ↓ ~39-50% |
| Desflurane | ↓ ~22% | ↓ ~22-35% |
| Xenon | Near-awake values | Near-awake values |
Order of cerebral vasodilating potency: Halothane >> Enflurane > Desflurane ≈ Isoflurane > Sevoflurane
The Uncoupling Concept - "Luxury Perfusion"
- Normally, CBF tightly tracks CMRO₂ (flow-metabolism coupling).
- Volatile anesthetics do NOT truly uncouple CBF from CMRO₂ - a coupled response still exists - but they shift the ratio upward.
- At doses > 1 MAC: CMRO₂ suppression plateaus, while CBF continues to rise due to direct vasodilation.
- Result: CBF/CMRO₂ ratio increases with higher MAC - called "luxury perfusion".
- Higher MAC = greater luxury perfusion.
Miller's Anesthesia, 10e, p. 1007
Effect on Cerebral Autoregulation
- Volatile anesthetics impair autoregulation in a dose-dependent manner.
- At high doses, CBF becomes pressure-passive (follows MAP directly).
- Sevoflurane best preserves autoregulation - intact up to ~1 MAC; at 1.5 MAC, dynamic autoregulation is better preserved with sevoflurane than isoflurane.
- Isoflurane and desflurane reduce autoregulation in a dose-dependent manner.
Barash Clinical Anesthesia, 9e, p. 1415
CMRO₂ Dose-Response Details
- CMRO₂ reduction is dose-dependent and shows some nonlinearity:
- A sharp initial drop in CMRO₂ occurs with the onset of anesthesia (EEG pattern change).
- Thereafter, it declines more gradually.
- Maximum CMRO₂ suppression coincides with EEG burst suppression, which occurs at ~1.5-2 MAC for isoflurane/sevoflurane/desflurane.
- Beyond EEG suppression, no further CMRO₂ reduction occurs - the floor has been reached.
- Halothane is an exception: requires >4 MAC for EEG suppression, and at very high doses may interfere with oxidative phosphorylation.
- At 1 MAC: isoflurane ↓ CMRO₂ ~45%, sevoflurane ~38%, desflurane ~22%, halothane only ~10%.
Miller's Anesthesia, 10e, p. 1014-1015
Clinical Takeaways
| Concern | Implication |
|---|---|
| Raised ICP | Halothane is worst (massive CBF↑ → ICP↑); sevoflurane and isoflurane safest at ≤1 MAC |
| Neuroprotection | Isoflurane/sevoflurane reduce CMRO₂ substantially → possible metabolic protection |
| Neurosurgery | Keep volatile dose ≤1 MAC; combine with hyperventilation (↓PaCO₂ → vasoconstriction) to counteract vasodilation |
| Autoregulation preservation | Sevoflurane preferred at ≤1 MAC |
- Miller's Anesthesia, 10e, p. 1005-1016
- Barash Clinical Anesthesia, 9e, p. 1414-1415
Modalities of cerebral protection
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive summary of the modalities of cerebral protection drawn from the anesthesia literature:
Pathophysiologic Basis
Cerebral ischemia triggers a cascade: oxygen-glucose deprivation → ATP depletion → membrane depolarization → excitatory amino acid (glutamate) release → calcium influx → free radical production → neuronal death. Cerebral protection strategies target one or more points in this cascade.
1. Hypothermia
The most reliable and time-tested modality.
Mechanisms of protection:
| Effect | Detail |
|---|---|
| Favorable O₂ supply/demand balance | Reduces CMRO₂ ~7% per 1°C decrease |
| ↓ Excitatory amino acid release | Delays glutamate-mediated excitotoxicity |
| ↓ Blood-brain barrier permeability | Reduces vasogenic edema |
| ↓ Inflammatory response | Suppresses PMN leukocyte adhesion in damaged tissue |
| Delayed free radical production | Reduces oxidative injury |
Clinical applications:
- Deep hypothermia (15-18°C) with circulatory arrest: standard for complex aortic arch surgery - unequivocal protection
- Mild hypothermia (32-36°C, "targeted temperature management"): used after cardiac arrest; early trials showed benefit, but TTM1 (33°C vs 36°C) and TTM2 (hypothermia vs normothermia) did NOT demonstrate superiority of lower temperature - current practice emphasizes strict prevention of hyperthermia at minimum
- Neonatal hypoxic-ischemic encephalopathy: whole-body cooling to 33.5°C for 72 hours - remains beneficial
Hyperthermia is actively harmful:
- Even a 2°C temperature increase decreases cerebral ischemia tolerance
- Worsens excitotoxin release, free radical production, intracellular acidosis, BBB permeability
- Fever and hyperthermia worsen prognosis in stroke
Miller's Anesthesia, 10e, p. 7562-7564
2. Barbiturates
Mechanism: CMR suppression (↓ CMRO₂), CBF redistribution, free radical scavenging
- Protective in focal ischemia in animals and one human study
- Maximal CMRO₂ reduction achieved at EEG burst suppression
- Same protective benefit demonstrated at 1/3 of the burst-suppression dose - raises the question of non-metabolic mechanisms
- Barbiturates are NOT equivalent: methohexital and thiopental reduce infarct volume, but pentobarbital does not in direct animal comparisons
- IHAST Trial: thiopental to EEG suppression during aneurysm clipping did NOT improve short or long-term outcomes
- After cardiac arrest: barbiturates are ineffective
- Current status: Use is reasonable for temporary vessel occlusion (e.g., aneurysm surgery), but evidence does not support routine use for brain protection in focal ischemia
- Risks: cardiovascular depression, delayed emergence
Miller's Anesthesia, 10e, p. 1058-1060
3. Volatile Anesthetic Agents
Mechanism: CMR suppression + possible ischemic preconditioning
- Isoflurane: neuroprotective in models of hemispheric, focal, and near-complete ischemia; reduces CMRO₂ ~45% at 1 MAC
- Sevoflurane: similar CMR-suppressing profile to isoflurane; reduces CMRO₂ ~38% at 1 MAC
- Protection is not sustained in models of severe ischemia - only durable with mild insults
- Anesthetic preconditioning: brief sublethal exposure to volatile agents activates endogenous protective pathways (analogous to ischemic preconditioning) - promising concept
- Order of cerebral vasodilatory risk: Halothane >> Enflurane > Isoflurane ≈ Desflurane > Sevoflurane (relevant when ICP is a concern)
Miller's Anesthesia, 10e, p. 1060-1061
4. Propofol
Mechanism: GABA-A agonism, CMR suppression, antioxidant properties (free radical scavenging due to phenolic structure)
- EEG suppression achievable at clinical doses
- Used anecdotally during aneurysm surgery and carotid endarterectomy
- In animal models: infarction significantly reduced with propofol vs. awake controls
- Direct comparison with pentobarbital: similar degree of injury reduction
- Protection not sustained with severe ischemia; durable protection only with mild insults
- Considered a viable alternative to barbiturates for CMR suppression
Miller's Anesthesia, 10e, p. 1062-1063
5. Etomidate
- Also produces GABA-A agonism and maximal CMR suppression equivalent to barbiturates
- Proposed for aneurysm surgery
- However, in focal ischemia models, injury volume was NOT reduced vs. halothane controls - in fact, injury was significantly larger
- In patients with temporary intracranial vessel occlusion: greater tissue hypoxia and acidosis than desflurane
- Not recommended for cerebral protection
Miller's Anesthesia, 10e, p. 1063
6. Xenon
Mechanism: Non-competitive NMDA receptor blockade (blocks excitotoxic pathway)
- Neuroprotection demonstrated: against O₂-glucose deprivation (in vitro), focal ischemia (mice), and CPB-induced cognitive dysfunction (rats)
- Anesthetic preconditioning: prior xenon exposure reduces brain vulnerability to subsequent ischemic injury
- Combined with hypothermia or isoflurane: significantly reduces neuronal injury in neonatal hypoxia-ischemia models
- Protective effect visible up to 30 days post-injury
- Does not cause developmental apoptosis (unlike ketamine/volatile agents in neonates)
- Clinical limitation: no proven long-term neuroprotection in adult humans yet; outcome studies pending
Miller's Anesthesia, 10e, p. 1062
7. Physiological Optimization (Universal Measures)
These are the most consistently supported strategies regardless of etiology:
| Parameter | Target | Rationale |
|---|---|---|
| PaCO₂ | Normocapnia | Hypocapnia → vasoconstriction (may worsen ischemia); hypercapnia → vasodilation → ↑ ICP |
| MAP | Normotension | Maintain CPP; avoid hypotension |
| Temperature | Strict normothermia | Prevent even mild hyperthermia |
| Glucose | Normoglycemia | Hyperglycemia worsens ischemic injury (lactic acidosis); hypoglycemia equally harmful |
| Seizure control | Treat promptly | Seizures dramatically increase CMRO₂ |
| ICP management | ↓ ICP | Via mannitol, head elevation, CSF drainage, hyperventilation (short-term only) |
8. Pharmacologic Agents (Limited Clinical Proof)
| Agent | Mechanism | Status |
|---|---|---|
| Calcium channel blockers (nimodipine) | Reduces vasospasm after SAH | Proven benefit in SAH; not in general neuroprotection |
| NMDA antagonists (ketamine, MK-801) | Block excitotoxic pathway | Effective in animals; failed in human trials |
| Corticosteroids | Reduce vasogenic edema | Proven for peritumoral edema; not for ischemic stroke |
| Mannitol | Reduces cerebral edema via osmotherapy | Useful for ICP reduction; not a direct neuroprotectant |
| Argon | Noble gas with NMDA activity | Promising in experimental models; not yet in humans |
Summary Table
| Modality | Evidence in Humans | Clinical Use |
|---|---|---|
| Deep hypothermia (circulatory arrest) | Strong | Cardiac/aortic surgery |
| Targeted temperature management | Moderate (avoid hyperthermia) | Post-cardiac arrest |
| Volatile anesthetics | Experimental + indirect | Routine anesthesia, preconditioning |
| Barbiturates | Weak (IHAST negative) | Selective use in temporary occlusion |
| Propofol | Animal/anecdotal | Alternative to barbiturates |
| Nimodipine | Proven in SAH vasospasm | SAH only |
| Physiological optimization | Strong consensus | All settings |
| NMDA antagonists | Failed clinical trials | Research only |
| Xenon/Argon | Preclinical | Investigational |
Miller's Anesthesia, 10e, p. 1054-1063; Barash Clinical Anesthesia, 9e; Harrison's Principles 22e
This is a shared conversation. Sign in to Orris to start your own chat.