Fibrous dysplasia in mandible
Reading File
Finding Sources
Searching PubMed
"fibrous dysplasia" AND mandible
Searching the Web
fibrous dysplasia mandible clinical features pathology treatment 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to write a thorough answer. Let me compile everything.
Fibrous Dysplasia of the Mandible
Definition and Overview
Fibrous dysplasia (FD) is a benign, chronic, slowly progressive bone disorder in which normal bone is replaced by fibrous connective tissue containing irregularly arranged spicules of woven bone. In the jaw, the mandible is classified as a membranous bone, and FD may occur there in either a localized (monostotic) or diffuse (polyostotic) form. The mandible is actually less commonly involved than the maxilla in craniofacial FD - maxillary FD is often associated with other craniofacial involvement, whereas mandibular lesions tend to be truly monostotic.
- Cummings Otolaryngology, p. 996; S Das Manual on Clinical Surgery, p. 342
Etiopathogenesis
FD results from a somatic gain-of-function mutation in the GNAS1 gene (chromosome 20q13.2-3), which encodes the alpha subunit of the stimulatory G-protein (Gsα). This mutation occurs during fetal development, and its timing determines the extent of disease:
- Mutation during very early embryogenesis → McCune-Albright syndrome (polyostotic FD + cafe-au-lait spots + endocrinopathies)
- Mutation in an osteoblast precursor late in skeletal formation → monostotic FD
The activating mutation causes constitutive Gsα activation, raising intracellular cAMP levels, which alters the Wnt pathway and downstream signaling, promoting cellular proliferation and inhibiting osteoblast differentiation. The result is replacement of normal bone by immature mesenchymal osteoblastic precursor cells that lay down woven bone without proper maturation.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1102; Robbins & Kumar Basic Pathology, p. 7
Clinical Forms
| Form | Description |
|---|---|
| Monostotic | Single bone involved; 70-85% of all FD cases; mandibular FD is typically this type |
| Polyostotic | Multiple bones; craniofacial region + femur most common; continues into adulthood |
| McCune-Albright syndrome | Polyostotic FD + cafe-au-lait pigmentation + endocrinopathies (precocious puberty, hyperthyroidism, GH excess) |
| Mazabraud syndrome | Polyostotic FD + intramuscular myxomas (in same anatomic region) |
Clinical Features in the Mandible
- Age of onset: First two decades of life; commonly diagnosed before age 20
- Sex: Affects men and women ages 25-35 at diagnosis (some sources); no strong sex predilection in jaw cases
- Presentation: Painless, slowly progressive unilateral swelling of the mandible
- Bony deformity causing facial asymmetry - "cherubism" refers specifically to bilateral FD of mandible and maxilla
- Pathologic fracture (uncommon in the jaw compared to long bones)
- Dental effects: Malocclusion, tooth displacement, altered eruption pattern
- Paresthesia: Inferior alveolar nerve can be compressed in larger lesions
- Growth pattern: Monostotic lesions often stabilize at skeletal maturity (puberty); surgery is therefore delayed in growing children when possible
- Serum alkaline phosphatase may be elevated (30% of polyostotic cases); calcium and phosphorus are usually normal
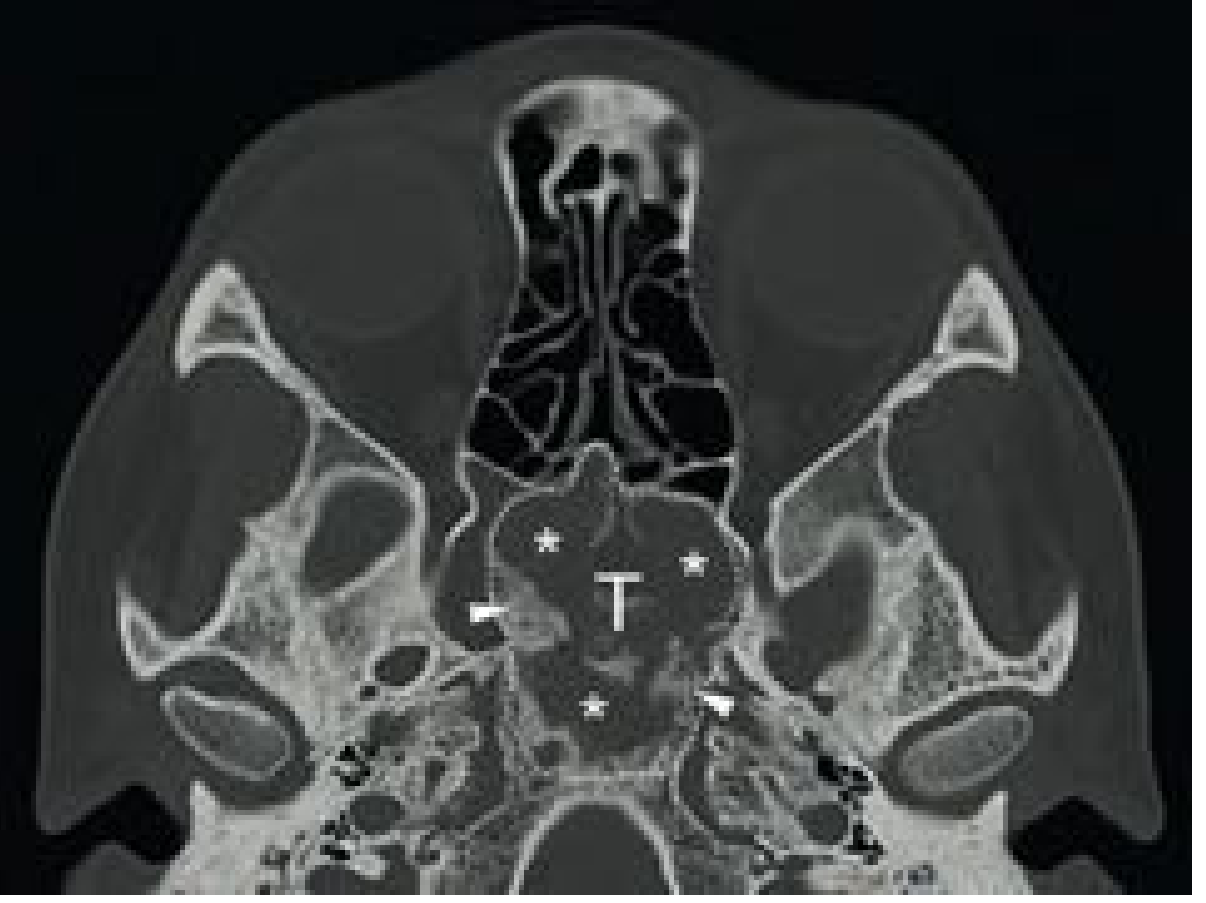
Radiology
Plain radiograph / CT findings:
The CT appearance varies with degree of mineralization and goes through distinct phases:
| Phase | Appearance |
|---|---|
| Early (high fibrous content) | Radiolucent / lytic |
| Intermediate | Ground-glass opacity (most characteristic) |
| Late (heavy mineralization) | Dense/sclerotic areas |
- The classic "ground-glass" appearance on CT reflects the variable mineralization of fibrous tissue replacing normal bone
- Endosteal scalloping of the inner cortex with a smooth non-reactive periosteal surface
- Lesions have diffuse, ill-defined margins (no sclerotic rim - unlike ossifying fibroma, which has an eggshell peripheral rim)
- Cortex is thinned and expanded but periosteal reaction is typically absent
- On MRI: T1 - hypointense; T2 - variable; may show non-homogeneous gadolinium enhancement
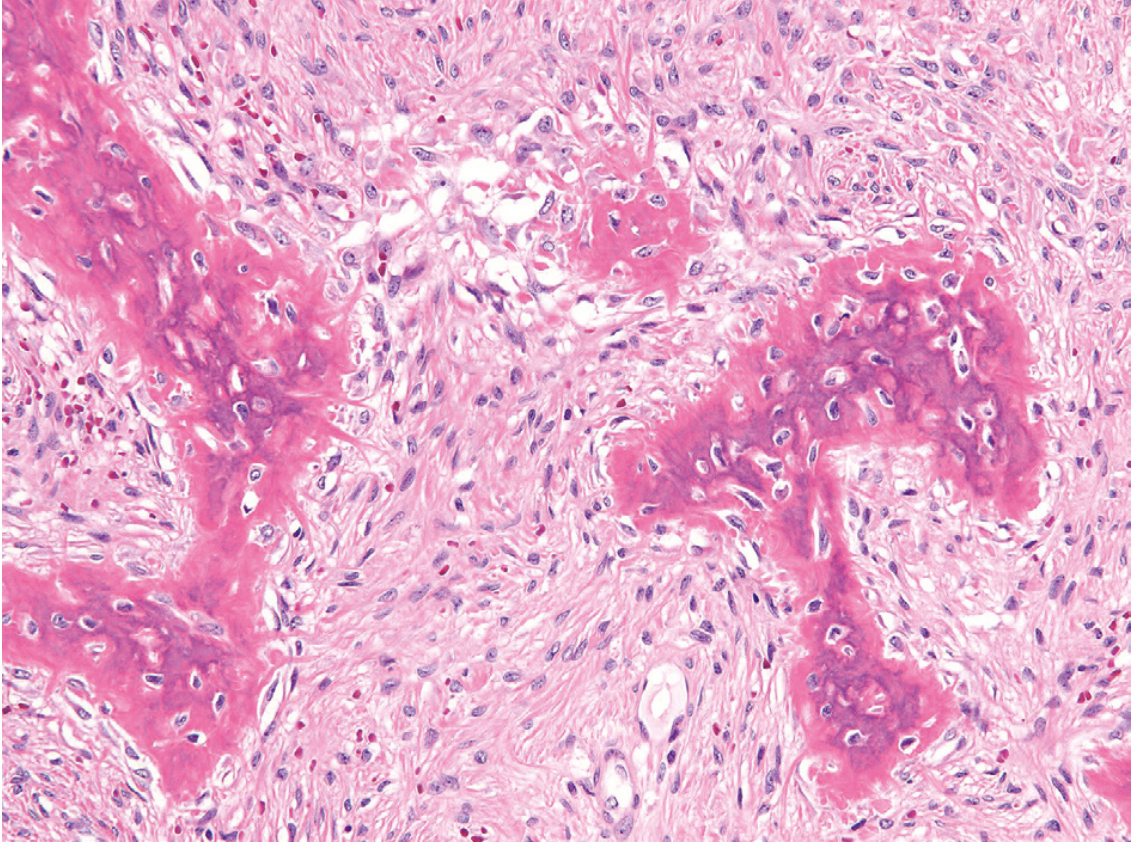
Histopathology
The microscopic hallmark is curvilinear "Chinese letter" trabeculae of woven bone embedded in a fibrous stroma, with the following features:
- Irregular, haphazardly arranged spicules of woven bone (confirmed under polarized light)
- Absent or minimal osteoblastic rimming around the trabeculae (key difference from ossifying fibroma)
- Moderately cellular fibroblastic stroma with loose collagen arranged in a whorled pattern
- No capsule (unlike ossifying fibroma)
- Secondary changes: cystic degeneration, hemorrhage, foamy macrophages
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Ossifying fibroma | Well-defined lesion with eggshell peripheral rim on CT; true neoplasm; osteoblastic rimming on histology; high recurrence after excision |
| Paget's disease | Older patient; "cotton wool" pattern; elevated ALP/urine hydroxyproline; autosomal dominant |
| Osteosarcoma | Rapid growth, pain, periosteal reaction ("sunburst"), soft tissue invasion |
| Aneurysmal bone cyst | Expansile, fluid-fluid levels on MRI; hemorrhagic aspirate |
| Central cemento-osseous dysplasia | Peroapical distribution; associated with teeth |
| Cherubism | Bilateral mandible/maxilla; autosomal dominant; bilateral symmetric "cherub" appearance |
Treatment
Management strategy is guided by age, lesion size, growth rate, and symptoms:
Conservative (preferred in children and quiescent disease):
- Asymptomatic lesions are observed with periodic clinical and radiologic follow-up
- Monostotic lesions often stabilize after skeletal maturity - surgery deferred in young patients
- Bisphosphonates (pamidronate): Inhibit osteoclastic activity; used for extensive lesions with significant pain or disfigurement
Surgical:
- Indicated for: progressive deformity causing facial asymmetry, pathologic fracture, nerve compression (inferior alveolar nerve), significant functional impairment
- Surgical recontouring / osteoplasty is the standard approach for mandibular FD causing deformity
- Important caveat: recurrence risk ~25% after recontouring; more likely to recur if surgery is done before skeletal maturity
- For jaw lesions, piezosurgery (ultrasonic bone cutting) has been used to preserve the inferior alveolar nerve
- Curettage is used for symptomatic monostotic lesions, though recurrence is common
Contraindicated:
- Radiotherapy is contraindicated - risks impaired facial skeleton growth in young patients and increases the risk of malignant transformation
Complications
- Malignant transformation: Rare (<1%), occurring in polyostotic > monostotic form; typically to osteosarcoma, usually decades after initial diagnosis. Incidence estimated at 0.4-1% overall.
- Pathologic fracture (less common in jaw than long bones)
- Nerve compression (inferior alveolar nerve → paresthesia)
- Dental malocclusion and displacement
Key Distinguishing Features - Fibrous Dysplasia vs. Ossifying Fibroma
| Feature | Fibrous Dysplasia | Ossifying Fibroma |
|---|---|---|
| Nature | Developmental/genetic anomaly | True benign neoplasm |
| Capsule | Absent | Present |
| Osteoblastic rimming | Absent/minimal | Present |
| CT margins | Ill-defined | Well-defined eggshell rim |
| Recurrence | Stabilizes at maturity | High recurrence rate (>40%) |
| Treatment | Conservative/recontouring | Wide radical resection |
- Cummings Otolaryngology, p. 996
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (p. 1102-1103); Robbins & Kumar Basic Pathology; Cummings Otolaryngology Head and Neck Surgery (p. 996-997, 2917); Scott-Brown's Otorhinolaryngology Vol 2 (p. 301); S Das Manual on Clinical Surgery (p. 342)
This is a shared conversation. Sign in to Orris to start your own chat.