Classification of laryngeal tumors
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to provide a comprehensive classification of laryngeal tumors. Here is the full answer:
Classification of Laryngeal Tumors
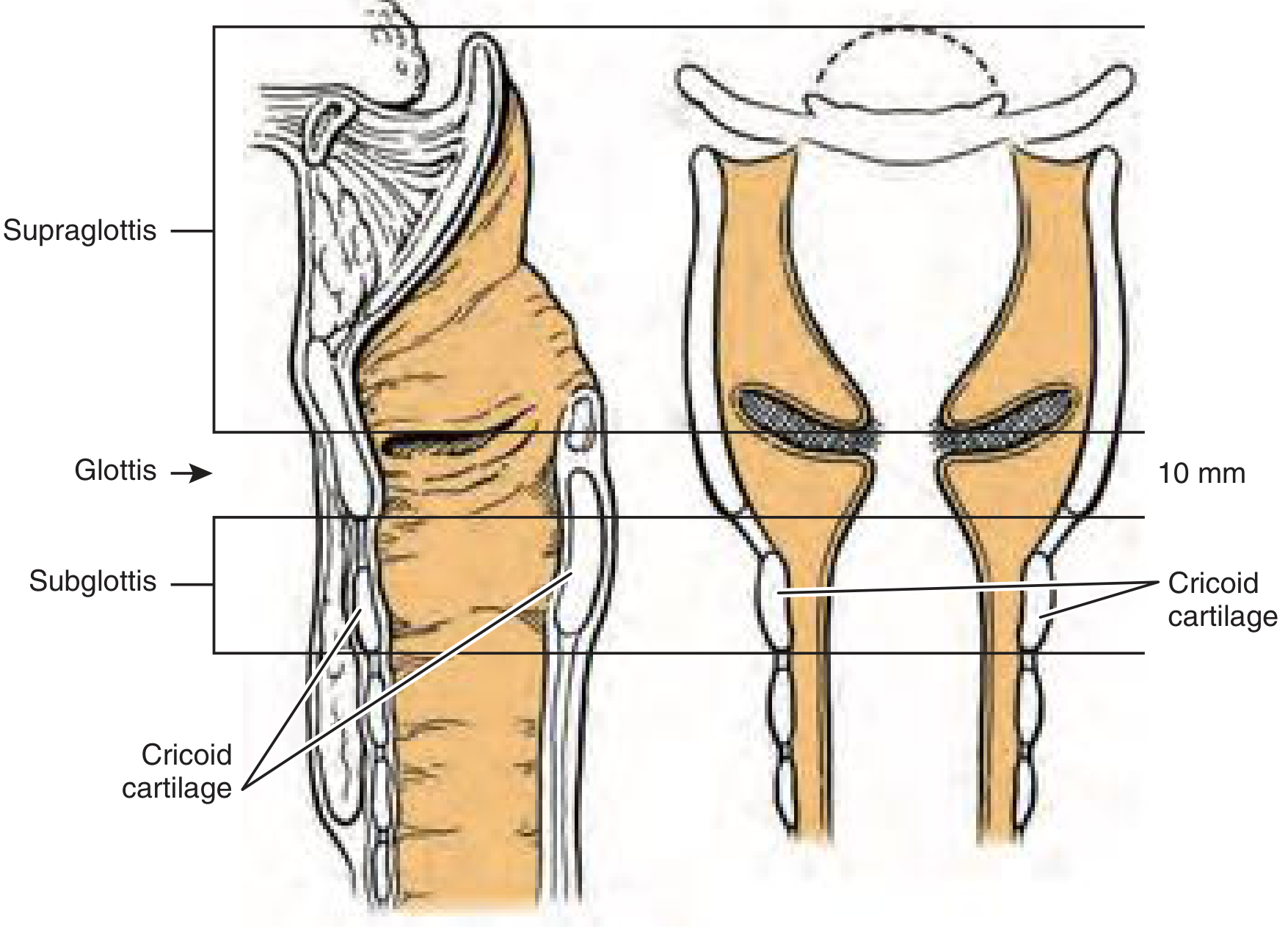
Fig. 105.1 - Classification of laryngeal lesions by anatomic site (Cummings Otolaryngology)
I. ANATOMICAL SITE CLASSIFICATION
The larynx is divided into three anatomically and embryologically distinct regions. This division guides tumor behavior, lymphatic drainage patterns, and staging:
1. Supraglottis (40% of laryngeal cancers)
Includes:
- Suprahyoid and infrahyoid epiglottis (both lingual and laryngeal surfaces)
- Aryepiglottic folds (laryngeal surfaces)
- Arytenoids
- False vocal cords (vestibular folds)
Embryologic origin: buccopharyngeal primordium (3rd and 4th branchial arches). Lymphatic drainage goes bilaterally to Level II and III deep cervical nodes - hence higher risk of bilateral nodal metastasis.
2. Glottis (59% of laryngeal cancers)
Includes:
- True vocal cords (superior and inferior surfaces)
- Anterior commissure
- Posterior commissure
- Zone extending 1 cm below the inferior margin of the true cords
Embryologic origin: tracheobronchial primordium (6th branchial arch). Sparse lymphatics at the glottis level = lower risk of nodal metastasis, which explains why glottic cancers present earlier and have better prognosis.
3. Subglottis (1% of laryngeal cancers)
- Region from 1 cm below the inferior true cord to the inferior margin of the cricoid cartilage
- Drains to Level VI (prelaryngeal/pretracheal) and Level IV nodes
- Very rare primary site; often represents inferior extension of glottic tumors
II. CLASSIFICATION BY HISTOPATHOLOGY / TUMOR TYPE
A. Non-neoplastic Lesions (Differential Diagnoses)
- Mucus retention cyst / laryngocele / saccular cyst
- Vocal fold polyp / vocal process granuloma
- Keratosis / amyloidosis
- Heterotopic thyroid tissue
- Infectious: tuberculosis, candidiasis, histoplasmosis
- Inflammatory: Wegener granulomatosis, relapsing polychondritis, foreign body granuloma
B. Premalignant / Precursor Lesions
The 2017 WHO classification adopted a two-tier system (based on the amended Ljubljana classification):
| Tier | Category | Risk |
|---|---|---|
| Low-grade | Low-grade dysplasia | Low malignant potential |
| High-grade | High-grade dysplasia + Carcinoma in situ (CIS) | High-risk premalignant lesion |
For treatment purposes, a three-tier system may be used: low-grade dysplasia / high-grade dysplasia / CIS. CIS is reserved for cases with severe architectural disorder, severe atypia, and increased mitoses.
Clinically these appear as:
- Leukoplakia (white patches)
- Erythroplakia (red patches) - higher malignant potential
- Erythroleukoplakia (mixed)
The Ljubljana taxonomy (also known as the EHLL - Epithelial Hyperplastic Laryngeal Lesions classification) is the closest to an internationally accepted classification for precursor lesions.
C. Benign Neoplasms
- Papilloma (squamous) - most common benign laryngeal tumor; caused by HPV types 6 and 11; 3-7% risk of malignant degeneration to SCC
- Pleomorphic adenoma
- Oncocytic papillary cystadenoma
- Lipoma
- Neurofibroma
- Leiomyoma
- Paraganglioma (benign)
- Chondroma
- Giant cell tumor (benign)
D. Primary Laryngeal Malignancies
1. Epithelial Malignancies (85-95% of all laryngeal malignancies)
Squamous Cell Carcinoma (SCC) variants:
- Conventional SCC - most common
- Verrucous SCC - well-differentiated, exophytic, locally aggressive, rarely metastasizes
- Spindle cell carcinoma (sarcomatoid SCC)
- Acantholytic (adenoid) SCC
- Papillary SCC
- Lymphoepithelial carcinoma
- Clear cell carcinoma
- Basaloid SCC
- Giant cell carcinoma
- Adenosquamous carcinoma
2. Malignant Salivary Gland Tumors
- Adenocarcinoma (NOS)
- Acinic cell carcinoma
- Mucoepidermoid carcinoma
- Adenoid cystic carcinoma
- Carcinoma ex pleomorphic adenoma
- Epithelial-myoepithelial cell carcinoma
- Salivary duct carcinoma
3. Neuroendocrine Carcinomas
| Grade | Type |
|---|---|
| Well-differentiated | Carcinoid tumor (typical carcinoid) |
| Moderately differentiated | Atypical carcinoid tumor |
| Poorly differentiated | Large-cell NEC |
| Poorly differentiated | Small-cell NEC (most aggressive) |
| Malignant paraganglioma |
4. Malignant Soft Tissue Tumors (Sarcomas)
- Fibrosarcoma
- Malignant fibrous histiocytoma (undifferentiated pleomorphic sarcoma)
- Liposarcoma
- Leiomyosarcoma
- Rhabdomyosarcoma
- Angiosarcoma
- Kaposi sarcoma
- Malignant hemangiopericytoma
- Malignant nerve sheath tumor
- Synovial sarcoma
- Ewing sarcoma
- Alveolar soft part sarcoma
5. Malignant Bone/Cartilage Tumors
- Chondrosarcoma (most common laryngeal cartilage malignancy)
- Osteosarcoma
6. Hematolymphoid Tumors
- Lymphoma
- Extramedullary plasmacytoma
E. Secondary (Metastatic) Laryngeal Malignancies
Contiguous spread from:
- Hypopharynx, oropharynx, thyroid
Distant hematogenous spread from:
- Kidney (most common), skin (melanoma), breast, lung, prostate, gastrointestinal tract
III. AJCC/TNM STAGING (8th Edition) - Epithelial Malignancies Only
Note: Non-epithelial tumors (lymphoid, soft tissue, cartilage, bone) are not staged by this system; they use their own relevant TNM schemes.
Primary Tumor (T) - By Subsite
Supraglottis
| Stage | Criteria |
|---|---|
| Tis | Carcinoma in situ |
| T1 | Limited to ONE subsite of supraglottis; normal vocal cord mobility |
| T2 | Invades mucosa of >1 adjacent subsite of supraglottis or glottis or region outside (base of tongue, vallecula, medial piriform sinus); NO fixation |
| T3 | Limited to larynx with vocal cord FIXATION and/or invades: postcricoid area, preepiglottic space, paraglottic space, inner cortex of thyroid cartilage |
| T4a | Moderately advanced: invades through outer cortex of thyroid cartilage and/or tissues beyond larynx (trachea, strap muscles, thyroid, esophagus) |
| T4b | Very advanced: invades prevertebral space, encases carotid artery, or invades mediastinal structures |
Glottis
| Stage | Criteria |
|---|---|
| T1 | Limited to vocal cord(s); NORMAL mobility; may involve anterior/posterior commissure |
| T1a | Limited to ONE vocal cord |
| T1b | Involves BOTH vocal cords |
| T2 | Extends to supraglottis and/or subglottis and/or IMPAIRED vocal cord mobility |
| T3 | Limited to larynx; vocal cord FIXATION and/or invasion of paraglottic space and/or inner cortex of thyroid cartilage |
| T4a | Invades through outer cortex of thyroid cartilage and/or beyond larynx (trachea, cricoid, soft tissues of neck) |
| T4b | Invades prevertebral space, encases carotid, or invades mediastinal structures |
Note: Many authors subdivide T2 glottic as T2a (normal mobility) and T2b (impaired mobility) because T2b has inferior local control with RT - this subdivision is NOT in the official AJCC system.
Subglottis
| Stage | Criteria |
|---|---|
| T1 | Limited to subglottis |
| T2 | Extends to vocal cord(s) with normal or impaired mobility |
| T3 | Limited to larynx with vocal cord fixation |
| T4a | Moderately advanced: invades cricoid or thyroid cartilage and/or extends beyond larynx |
| T4b | Very advanced: invades prevertebral space, encases carotid, invades mediastinum |
Regional Lymph Nodes (N) - Clinical
| Stage | Criteria |
|---|---|
| N0 | No regional lymph node metastasis |
| N1 | Single ipsilateral node ≤3 cm, ENE(-) |
| N2a | Single ipsilateral node >3 cm but ≤6 cm, ENE(-) |
| N2b | Multiple ipsilateral nodes, none >6 cm, ENE(-) |
| N2c | Bilateral or contralateral nodes, none >6 cm, ENE(-) |
| N3a | Any node >6 cm, ENE(-) |
| N3b | Any node with ENE(+) |
(ENE = extranodal extension)
Distant Metastasis (M)
- M0: No distant metastasis
- M1: Distant metastasis present
Overall Stage Grouping
| Stage | T | N | M |
|---|---|---|---|
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III | T3 | N0 | M0 |
| III | T1, T2, T3 | N1 | M0 |
| IVa | T4a | N0, N1, N2 | M0 |
| IVa | T1-T4a | N2 | M0 |
| IVb | T4b | Any N | M0 |
| IVb | Any T | N3 | M0 |
| IVc | Any T | Any N | M1 |
IV. CLINICAL STAGING CATEGORIES (Operative / Treatment Planning)
Cummings Otolaryngology uses this pragmatic system for surgical decision-making:
| Category | Description |
|---|---|
| Very Early | Exophytic growth, minimal lamina propria invasion; ideal for photoablation |
| Early | Broadly corresponds to T1b/T2a glottic and T1 supraglottic; suitable for open VPL or supraglottic laryngectomy |
| Intermediate | T2-T3 range lesions |
| Advanced | T3-T4a range; may require total laryngectomy or organ-preservation CRT |
| Very Advanced | T4b; unresectable disease |
Key Epidemiological Points
- Laryngeal cancer is the 2nd most common malignancy of the upper aerodigestive tract
- Represents 1-5% of all malignancies; ~13,150 new cases/year in the USA
- M:F ratio 4:1
- SCC: 85-95% of all laryngeal malignancies
- Distribution: glottis 59%, supraglottis 40%, subglottis 1%
- Major risk factors: smoking (10-20x increased risk), alcohol, prior head and neck SCC, HPV (types 6/11 in RRP; types 16/18 weakly implicated), asbestos, diesel fumes, gastroesophageal reflux
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Box 105.1, Table 105.1, Table 106.2 (pp. 1980-1985)
- K.J. Lee's Essential Otolaryngology, Table 44-1 (p. 815)
- Bailey and Love's Short Practice of Surgery, 28th ed., Chapter 52
This is a shared conversation. Sign in to Orris to start your own chat.