Explain me different types of ST ELEVATION EGG AND ST DEPRESSION ECG WITH IMAGEs of the disease
Reading File
Finding Sources
Finding Sources
Searching the Web
types of ST elevation ECG patterns STEMI pericarditis early repolarization images diagrams
Reading File
Finding Sources
Searching the Web
types ST depression ECG patterns NSTEMI ischemia digoxin LVH hypokalemia images
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive content and images. Let me compile the full, detailed answer.
ST Elevation and ST Depression ECG: Types, Patterns & Images
The ST segment represents the period between ventricular depolarization (end of QRS) and repolarization (T wave). Deviation above or below the isoelectric baseline - measured at the J point - is one of the most diagnostically important findings in emergency medicine.
PART 1: ST ELEVATION (STE)
Normal STE: up to 1 mm in limb leads and up to 2 mm in precordial leads V1-V3 in men, 1.5 mm in women. Any elevation beyond these thresholds in two contiguous leads is pathological until proven otherwise.
1. ST-Elevation Myocardial Infarction (STEMI)
The most dangerous cause of STE. Caused by complete occlusion of a coronary artery, producing full-thickness (transmural) ischemia. The STE in STEMI is typically convex (dome-shaped or tombstone) - the hallmark that distinguishes it from other benign causes.
Key ECG Features:
- Convex or tombstone-shaped STE in the territory of the affected artery
- Reciprocal ST depression in mirror-image leads
- Hyperacute (tall, peaked) T waves in the earliest phase
- Evolution to Q waves (pathological) as necrosis sets in
- T wave inversion developing over hours to days
Territorial patterns:
| Territory | Leads with STE | Culprit Vessel |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Inferior | II, III, aVF | RCA or LCx |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | Reciprocal STD in V1-V3 (STE in V7-V9) | RCA/LCx |
| Right ventricle | RV1-RV4 (right-sided leads) | Proximal RCA |
Right Ventricular Infarction ECG (from ROSEN's Emergency Medicine):
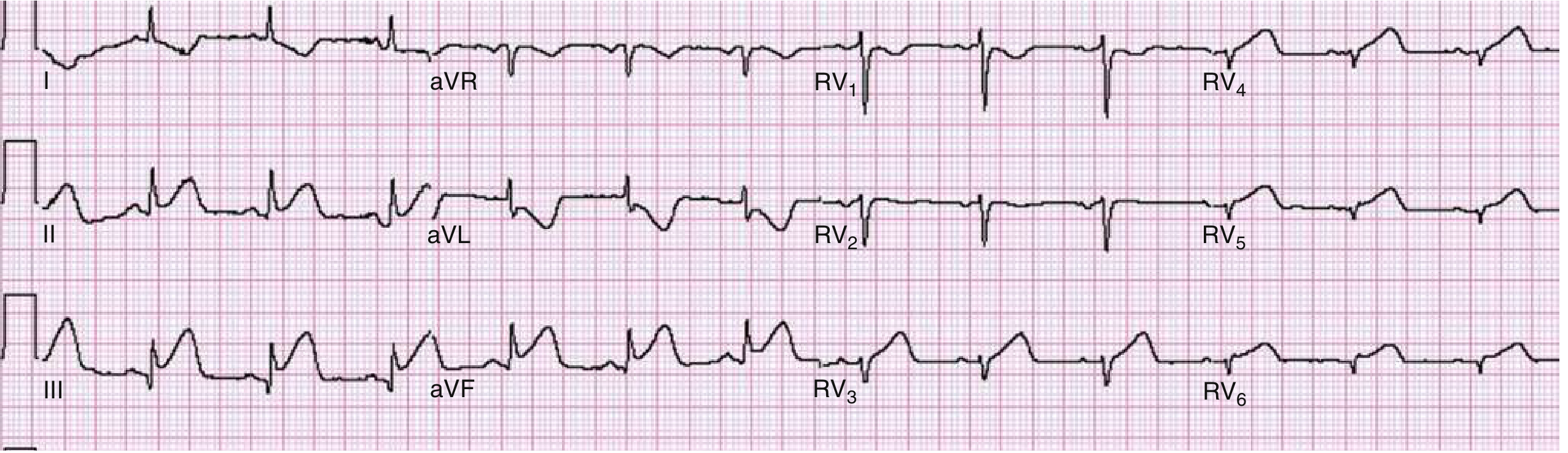
Right ventricular infarction demonstrated with right-sided precordial leads. ST elevation is noted in RV3 to RV6, consistent with RV infarction. Reciprocal ST depression is seen in leads I and aVL.
2. Benign Early Repolarization (BER)
A normal ECG variant seen commonly in young, healthy individuals (especially men <40 years and athletes). Does NOT imply ACS, but must be distinguished from STEMI.
Key ECG Features:
- Concave (smiley-face) upward ST elevation - the classic distinguishing feature
- Notched J point ("fish-hook" pattern) at the end of the QRS
- Maximal STE in V2-V5, usually <3.5 mm at the J point and <2 mm in the ST segment itself
- Large, symmetric concordant T waves
- Diffuse distribution, temporally stable
- Absent reciprocal changes
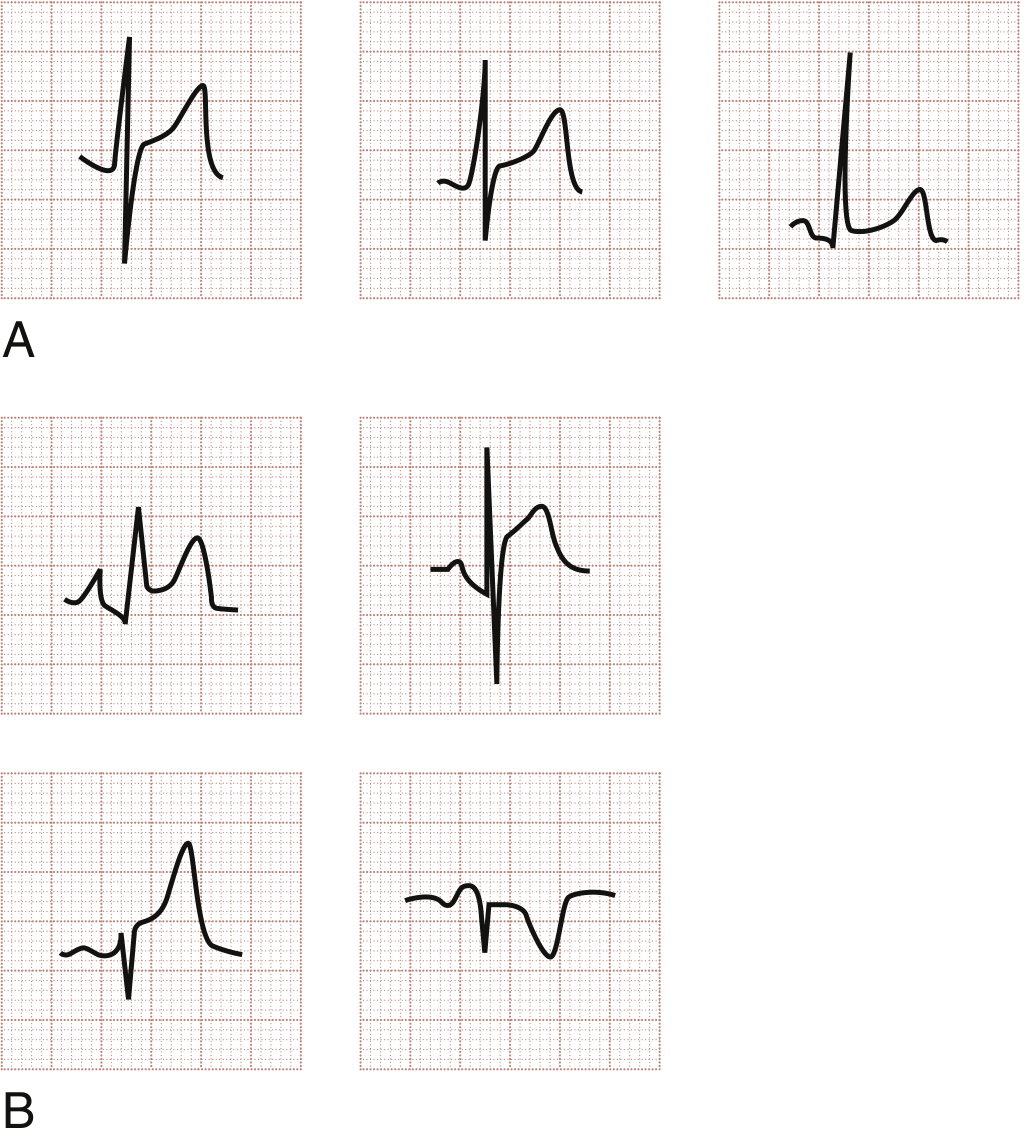
Panel A: Benign early repolarization (BER) - concave STE with notched J point in three morphologic variants. Panel B: Acute pericarditis patterns - concave STE with PR depression (upper panels), STE without PR changes (lower left), and reciprocal PR elevation in aVR (lower right).
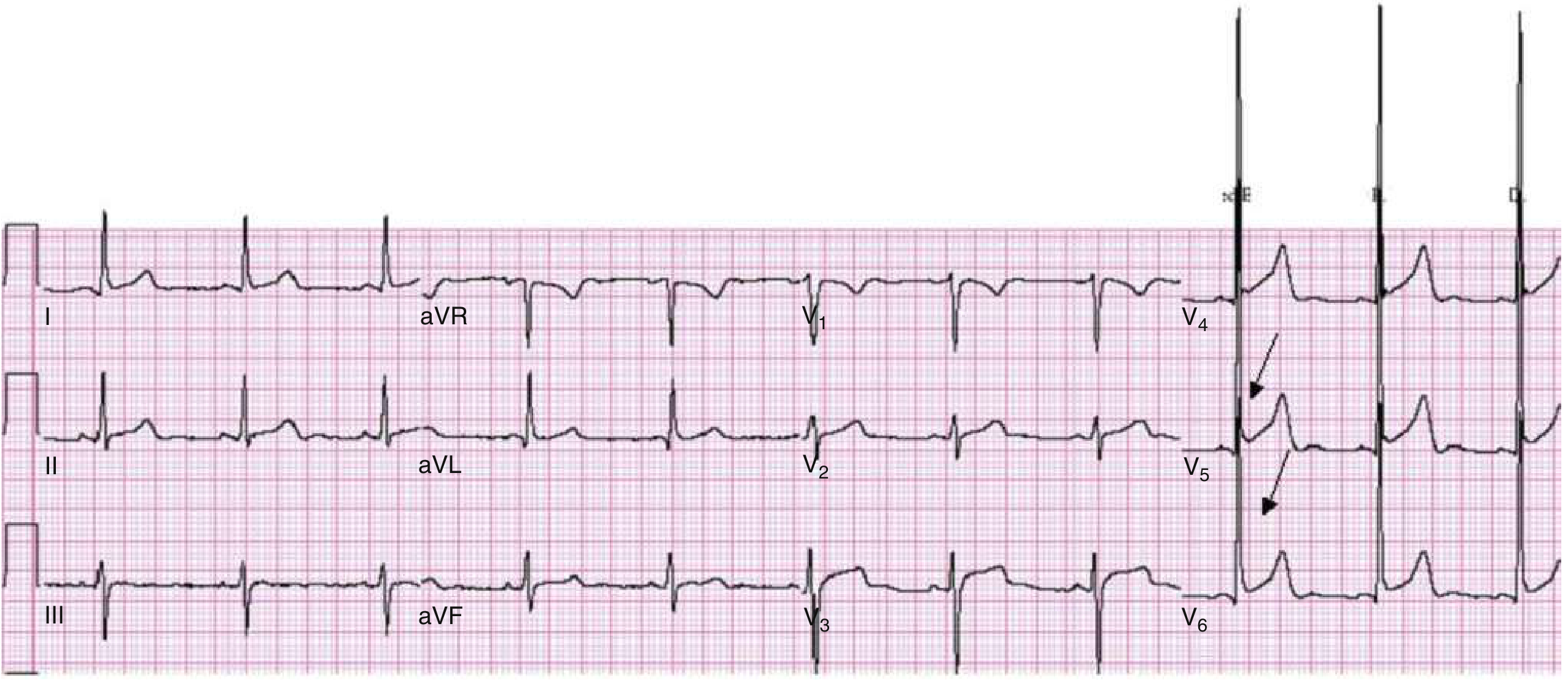
BER: Upwardly concave ST segment elevation best seen in V4-V6. Large T waves in the same leads. Subtle J-point irregularity (arrows) in V5-V6. ECG was unchanged from tracing 18 months prior.
3. Acute Pericarditis
Inflammation of the pericardium (technically myopericarditis, since the pericardium itself is electrically silent; changes reflect epicardial irritation). Typically presents in stages over days to weeks.
Key ECG Features:
- Diffuse concave STE - seen in nearly all leads except aVR (and sometimes V1)
- PR segment depression - sensitive and specific clue; best seen in lead II and V6; reciprocal PR elevation in aVR
- STE usually <5 mm
- No reciprocal ST depression (except in aVR)
- No pathological Q waves
- Four evolving stages: STE → ST normalization → T wave inversion → ECG normalization
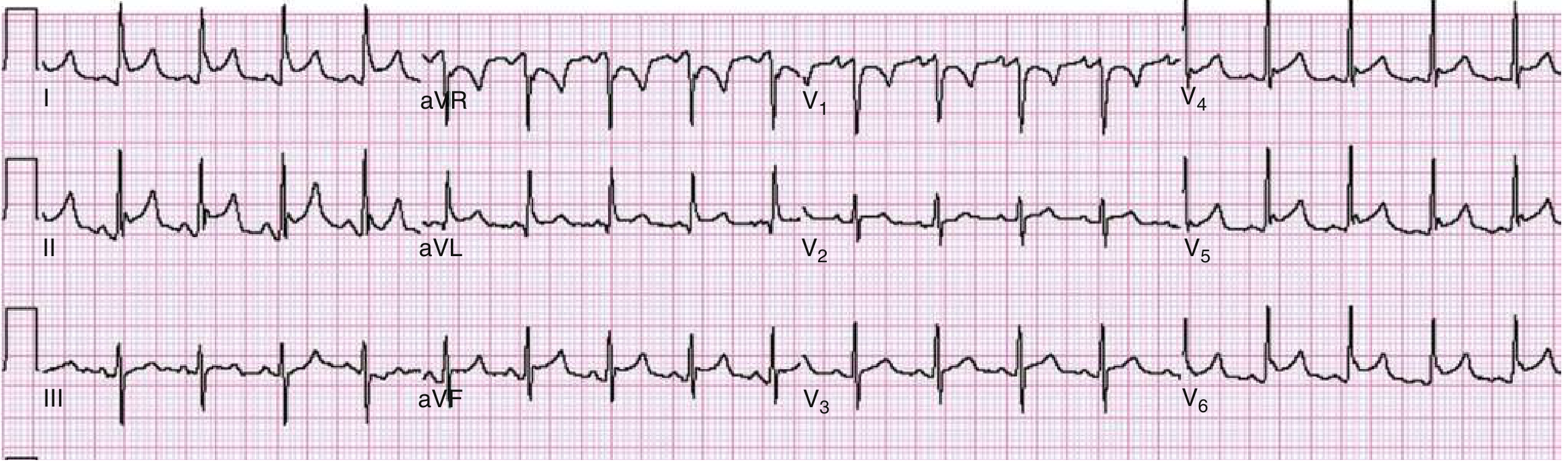
Pericarditis: Sinus tachycardia, diffuse concave upward STE, PR segment depression best seen in lead II, and PR elevation in aVR - all classic signs.
Key distinction from STEMI: Pericarditis shows diffuse STE in almost all leads; STEMI is territorial (limited to leads reflecting one vascular territory). Convex morphology strongly favors STEMI.
4. Left Ventricular Aneurysm (LVA)
A chronic complication of prior MI where a focal segment of myocardium paradoxically bulges outward during systole. The STE represents persistent chronic injury current, not acute infarction.
Key ECG Features:
- STE in the leads corresponding to the aneurysm territory (usually anterior: V1-V4)
- Well-developed, completed Q waves in the same leads
- T/QRS amplitude ratio <0.36 in all leads (helps distinguish from STEMI; STEMI ratio >0.36)
- No reciprocal changes in contralateral leads
- Temporally stable (unchanged from previous ECGs)
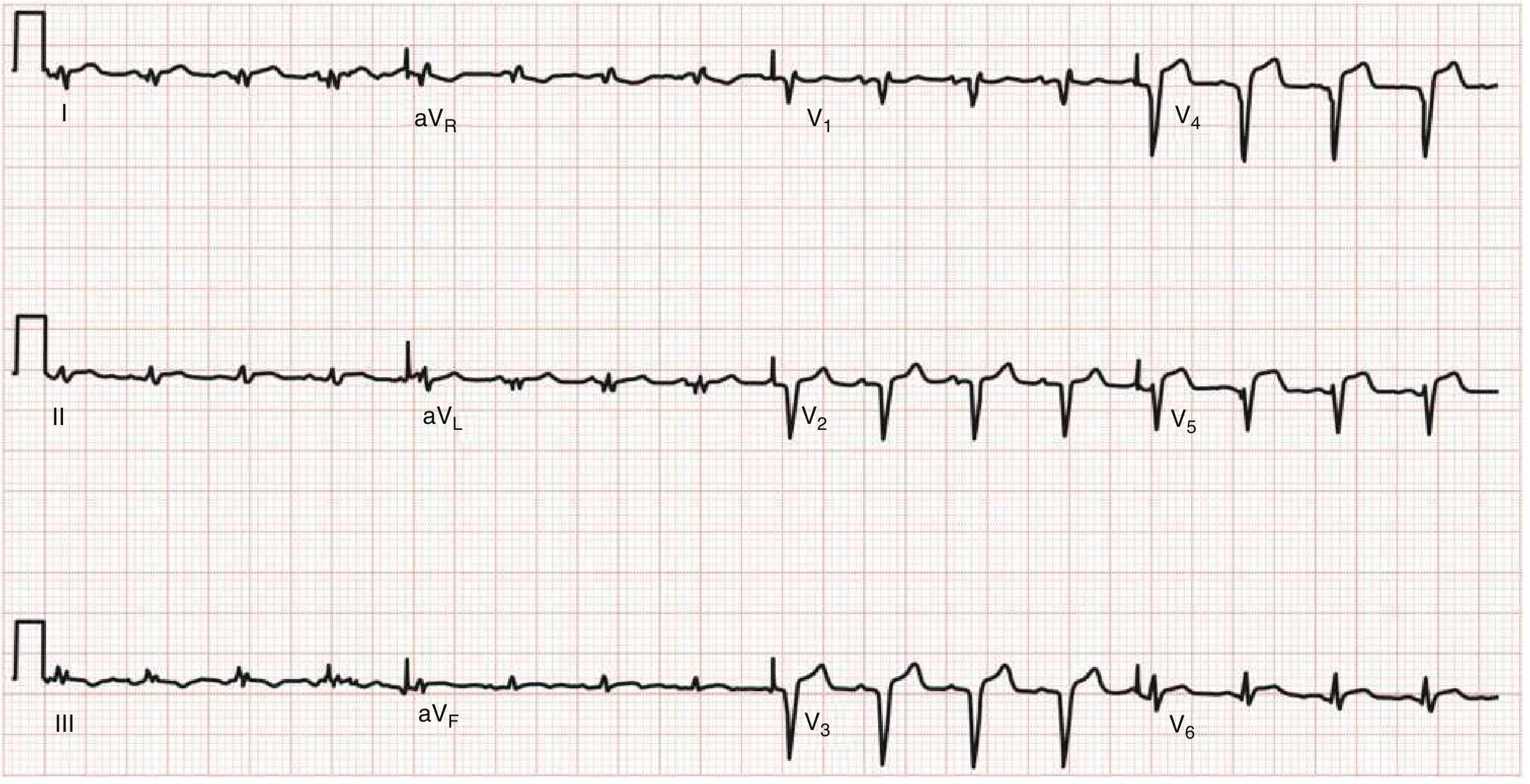
LV Aneurysm: 12-lead ECG with completed Q waves in V2-V5 and STE in the anterior leads, without reciprocal changes in contralateral leads.
5. Left Bundle Branch Block (LBBB) with STE
LBBB creates pseudo-STE via the "rule of appropriate discordance." The ST and T wave vectors are opposite to the major QRS direction.
Normal LBBB pattern (not representing MI):
- STE and tall T waves in V1-V3 (right precordial leads) - due to discordance
- ST depression with T wave inversion in V5, V6, I, aVL - also due to discordance
Sgarbossa Criteria - ECG evidence of MI in LBBB:
- STE ≥1 mm concordant with QRS complex (score 5) - most specific
- ST depression ≥1 mm in V1, V2, or V3 (score 3)
- STE ≥5 mm discordant with QRS complex (score 2)
- Score ≥3 = 90% specificity for AMI
- Modified Sgarbossa: ST/S wave ratio >0.25 replaces criterion 3 (increased sensitivity)
6. Other Causes of STE
| Cause | Key Feature |
|---|---|
| Brugada syndrome | Coved (type 1) or saddleback (type 2/3) STE in V1-V2; risk of VF |
| Vasospastic (Prinzmetal) angina | Transient STE during spasm; resolves spontaneously |
| Hyperkalemia | Peaked T waves + wide QRS + STE in V1-V2 (sine wave pattern) |
| Pulmonary embolism | STE in right-sided leads, S1Q3T3 pattern |
| LV hypertrophy (strain) | STE in V1-V2, discordant to QRS (secondary changes) |
| Hypothermia | Osborn (J) wave causing apparent STE |
| Takotsubo cardiomyopathy | Anterior STE mimicking STEMI, no obstructive CAD |
PART 2: ST DEPRESSION (STD)
STD is measured at the J point (or 40-80 ms after it). Any depression >0.5 mm in two or more contiguous leads is considered significant in the right clinical context.
1. Myocardial Ischemia / NSTEMI
The primary ischemic finding in non-ST-elevation acute coronary syndromes (NSTE-ACS). Reflects subendocardial ischemia (the subendocardium is most vulnerable to ischemia because it is farthest from coronary supply and has the highest oxygen demand).
Key ECG Features:
- Horizontal STD: flat ST segment, most specific for ischemia
- Downsloping STD: ST segment slopes downward from J point, also highly suggestive
- Transition from ST segment to T wave is more abrupt than normal
- May be accompanied by T wave inversion (flat or inverted T waves)
- Dynamic changes over time (worsening during chest pain, improving with nitrates or rest) strongly support ischemia
- Absence of STE does NOT mean better outcome - STD in V1-V4 may herald posterior STEMI (true posterior infarction)
NSTEMI ECG characteristics per ROSEN's: "Electrocardiographic manifestations of NSTEMI include ST segment depression and T wave inversion, which may be deep and symmetrical; nonspecific ST segment or T wave abnormalities may also be seen."
Patients with STD on initial ECG have an in-hospital mortality ~15-16%, comparable to STEMI patients.
STD morphologies:
| Type | Description | Clinical Significance |
|---|---|---|
| Horizontal STD | ST remains flat, parallel to baseline | Most specific for ischemia |
| Downsloping STD | ST slopes downward away from J point | Highly suggestive of ischemia |
| Upsloping STD | ST slopes upward toward T wave | Less specific; may be normal variant or tachycardia-related |
2. STEMI Reciprocal Changes
In STEMI, the leads facing the opposite wall show reciprocal ST depression - a mirror image of the STE in the primary territory. This is a secondary finding but an important clue to confirm STEMI territory and occlusion vessel.
Examples:
- Inferior STEMI (II, III, aVF) → Reciprocal STD in I, aVL
- Anterior STEMI (V1-V4) → Reciprocal STD in II, III, aVF (less common)
- Posterior STEMI → Maximal STD in V1-V3 is the PRIMARY finding (no STE on standard 12-lead); confirmed by STE in posterior leads V7-V9
3. Wellens Syndrome
A pre-infarction pattern indicating critical proximal LAD stenosis, seen between episodes of chest pain (pain-free state). Carries high risk of large anterior MI if not revascularized.
Two patterns:
- Type A (biphasic T waves): Positive-to-negative biphasic T waves in V2-V3 - often missed
- Type B (deep symmetric T wave inversion): Deeply and symmetrically inverted T waves in V2-V3 - the more recognized pattern
Key features: isoelectric or minimally elevated ST (<1 mm), NO Q waves, normal or slightly elevated troponin, history of chest pain resolving before ECG was taken.
4. Left Ventricular Hypertrophy (LVH) Strain Pattern
Chronic pressure/volume overload of the LV causes secondary repolarization changes - a "strain" pattern in lateral leads.
Key ECG Features:
- STD with asymmetric T wave inversion in lateral leads (I, aVL, V5-V6)
- ST and T wave vectors are discordant to the major QRS direction (secondary changes)
- Associated with voltage criteria for LVH (Sokolow-Lyon: SV1 + RV5/V6 >35 mm)
- The STD is smooth and gradual (as opposed to abrupt in ischemia)
5. Digoxin Effect
Digoxin produces a characteristic ECG pattern (not necessarily toxicity) at therapeutic levels.
Key ECG Features:
- Scooped or "reverse tick" (sagging) STD - the pathognomonic pattern
- Most prominent in lateral leads (V5-V6, I, aVL)
- Shortened QT interval
- Flattened or inverted T waves
- At toxic levels: brady-arrhythmias, PAT with block, bidirectional VT, AV blocks
6. Hypokalemia
Low serum potassium prolongs repolarization and alters ST-T morphology.
Key ECG Features:
- ST depression (often mild)
- T wave flattening or inversion
- Prominent U waves (key finding - U wave amplitude > T wave amplitude)
- Prolonged QU interval (appears as QT prolongation)
- Risk of torsades de pointes
7. Other Causes of STD
| Cause | Key Feature |
|---|---|
| RBBB (right bundle branch block) | Secondary STD in right precordial leads (V1-V2) - discordant to QRS |
| Tachycardia (rate-related) | Upsloping STD at fast rates, resolves with rate control |
| Pulmonary embolism | STD in inferior/anterior leads, T wave inversion in V1-V4 |
| Posterior STEMI | Maximal horizontal STD V1-V3 (the mirror of posterior wall STE) |
| Hypertrophic cardiomyopathy | Giant negative T waves + deep STD in midprecordial leads |
| Subarachnoid hemorrhage | Widespread deep T wave inversion and STD ("neurogenic" pattern) |
| WPW syndrome | Secondary repolarization abnormalities due to delta wave |
Quick Reference: STE vs STD Morphology
| Feature | Ischemic STE (STEMI) | Benign/Non-ischemic STE | Ischemic STD | Non-ischemic STD |
|---|---|---|---|---|
| Morphology | Convex/tombstone | Concave | Horizontal/downsloping | Upsloping or scooped |
| Distribution | Territorial | Diffuse | Contiguous leads | Lateral leads |
| PR segment | Normal | Depressed (pericarditis) | Normal | Normal |
| Reciprocal changes | Yes (contralateral STD) | No | May be present | No |
| Dynamic change | Yes (evolves over hours) | Stable | Yes (with symptoms) | Stable |
| Q waves | Develops | Absent | Absent | Absent |
Source: ROSEN's Emergency Medicine - Concepts and Clinical Practice, "Electrocardiographic Differential Diagnosis of ST Segment Elevation," Chapter 64; GOLDMAN-CECIL Medicine; Harrison's Principles of Internal Medicine 22E.
This is a shared conversation. Sign in to Orris to start your own chat.